
Abstract
Background
Medical students often lack sufficient nutrition education, leading to confidence gaps and an inability to address this healthcare aspect. Culinary Medicine (CM) courses offer an innovative solution.
Methods
We tested the first French-speaking CM courses among 2 groups of second-third year medical students, compared to a control group (CG). The objectives were to assess if an optional CM course could enhance their confidence in both nutritional knowledge and providing nutritional advice, and improve their food agency (CAFPAS: Cooking and Food Provisioning Action Scale). The analysis examines changes in scores by comparing post-session to pre-session questionnaire measurements.
Results
Of the 22 CM students and 6 in CG, predominantly aged 20-25 years, Caucasian, and female, the majority (CG = 100%, CM = 86.4%) reported <5 hours of nutrition education. Almost all expressed dissatisfaction with nutrition education provided in medicine, both quantitatively and qualitatively. CM students reported significantly increased confidence in their knowledge and ability to advise about nutrition during the sessions. We also observed improvements in their CAFPAS scores, which measure food agency, while the control group exhibited no change in confidence or CAFPAS scores.
Conclusion
The findings highlight CM as practical strategy for integrating nutrition education into medical curricula, offering insights for enhancing future physicians’ knowledge.
Keywords
“Students unanimously acknowledge that nutrition plays a crucial role in maintaining good health, the development of chronic diseases, and their management.”
Introduction
Globally, inadequate diet quality contributes to premature death. 1 Recent evidence highlighted the persistently poor diet quality in the Canadian population, showing minimal improvement in recent years. 2 Despite the profound impact of food in human life, medical students lack sufficient training and academic support in this field. A systematic review revealed a global deficiency in nutritional education for medical students, resulting in a lack of confidence in their knowledge and an inadequate preparation to provide effective nutritional guidance. 3 However, the role of nutrition in health is well recognized, both as protective risk factor and treatment for chronic diseases.4-6 The global crises of obesity and type 2 diabetes posed significant threats to the health and economies of nations worldwide.7-9 In a landscape where chronic diseases prevailed, envisioning global patient healthcare by physicians became challenging without sufficient education and a substantial interest in nutrition. For instance, guidelines for managing patients with stable ischemic heart disease emphasized the importance of addressing unhealthy behaviors and promoting lifestyle changes, including maintaining a healthy weight and adopting a healthy diet. 10 Do physicians, both in training and in practice, received adequate education in nutrition to implement these recommendations? Without addressing the deficiency in nutritional education within the medical field, it is conceivable to effectively prevent or manage societal chronic diseases?
For many years, the scientific community has voiced concerns about the inadequate training of physicians in nutrition. In 1961, the American Medical Association (AMA) Council on Foods and Nutrition highlighted the “inadequate recognition, support, and attention” given to nutrition in U.S. medical schools. 11 What is astonishing is that the recognition of the significance of food in medicine is linked to the foundational principles established by Hippocrates of Cos (fifth century BC), the father of Western medicine. 12 The Hippocratic Corpus distinctly recognized a separation between food and medicines. Food was regarded as a substance that undergoes assimilation and transformation into the body’s material, a distinction not applied to medicine. Food was not considered as medicine, 12 but the misquotation and misinterpretation of “Food as Medicine” 13 persists. More deeply, in Corpus work “On Ancient Medicine,” cooking appears to play a significant role in the Hippocratic medicine. 14 The first of two dietary imperatives in Hippocratic medicine emphasizes “the necessity to adapt healthy people’s food to human nature,” implying the importance of cooking it. 12
In the context of widespread prevalence of chronic diseases in our societies, the medical prospect of delivering comprehensive global patient care without proper education and a pronounced interest in nutrition appears to be a challenge. 15 According to Barnard, 16 “Nutritional ignorance is no longer defensible” in medicine and the medical community should stand to benefit from current nutritional knowledge for both patient well-being and its own. Physicians have the opportunity to positively influence patient behaviors, but without sufficient education in nutrition, they face challenges in acquiring confidences and skills to provide global care. 3 This nutritional deficiency could lead to a diminished recognition of its importance and associated challenges. It is also a leadership perspective as physicians who maintaining healthy lifestyle habits are perceived as more credible and motivating by their patients and supervised residents, in contrast to those neglecting their health.17,18
Culinary Medicine (CM), popular in many American medical schools, has emerged as a means to enhance physicians’ nutritional knowledge while making the learning experience engaging and practical.19,20 The educational approach of CM is based on medical and nutritional evidence but uses culinary art as an intervention tool.20-22 It aims to develop individuals’ skills and abilities to make healthy and sustainable food choices. It recognizes that adopting a healthy diet and relationship with food requires upstream skills, such as culinary, organoleptic knowledge and skills, as well as multisensory experiences. This aligns with Albert Einstein’s famous quote: “Knowledge is Experience. Everything else is Just Information.” Therefore, CM embodies this philosophy by prioritizing experiential learning through hands-on activities, such as cooking skills, tasting, and food exploration, rather than solely focusing on nutritional knowledge.
In the initial phase of this educational research project, we gathered insights from junior and senior external students in the Doctor of Medicine program at Université Laval. A total of 115 external students participated in the survey from September 23, 2021 to February 26, 2022. Our results support previous research, 3 indicating that medical students recognize the importance of nutritional education but note significant gaps in their training. Nearly 90% of these students report receiving less than 10 hours of nutrition education throughout their medical studies, and 78% express dissatisfaction with the quantity, while 67% are dissatisfied regarding the quality of this education (data not shown).
The central aim of this educational initiative was to test a CM elective course designed for medical students. To our knowledge, the Faculty of Medicine at Université Laval (FMED-UL) stands as the first French-speaking university worldwide to offer CM training. The primary goal of this project is to initially address the existing gap in nutrition training within the current medical curriculum and assess the impact of this dynamic and collaborative pedagogy on medical students. The specific research objectives aim to enhance medical students’ knowledge and interest in nutrition and cooking, increase their confidence in providing nutritional advice, and improve their food agency (self-efficacy and ability to take action).
Methods
Participants
The only selection criterion was to be a pre-clerkship student in Laval University’s Medicine program (first -third year). On April 5 and November 29, 2022, the office of undergraduate medical education at Laval University invited interested medical students to enroll into the elective CM course. As the number of interested students exceeded the maximum capacity of 12 places in each session, 12 students were selected through a random drawing. The students enrolled in the CM course in fall 2022 session (from September 6 to December 16) and winter 2023 session (from January 10 to April 21) represents the experimental CM group. Medical students of the same level, but not enrolled in the course, were also invited by email from the office of undergraduate medical education to participate in the study and served as the control group (CG, fall 2022 session only).
Culinary Medicine (CM) Course at Laval University
Many CM courses worldwide offered in medical schools consist of 2 to 3 hours of weekly training, with online components for theoretical aspects of nutrition and health, and hands-on components for practical skills. The CM course at Laval University has 3 distinct components.
The
The
Questionnaires
The questionnaires were completed online via the Research Electronic Data Capture (REDCap) system 23 through the Clinical Research Platform (CRP) of the CHU de Québec. An invitation containing the web link to the online questionnaires was sent by email to CM and CG participants during each recruitment period. A reminder to complete the paper questionnaire and online questionnaires was sent to participants by email for each recruitment period. Socioeconomic questions were included to gather identification and descriptive information about the students, focusing on sociodemographic factors and specific lifestyle habits. Before completing the questionnaires, students were required to read and provide their agreement to the information and consent form. The Research Ethics Committee of the CHU de Québec-Université Laval reviewed and approved the project on October 4, 2021 (Project Number: 2022-6066, SIRUL 131748).
Opinions and Perceptions of Nutrition in the Context of Medical Education
Students were surveyed using self-administered questionnaires to assess their opinions and perceptions of nutrition in the context of medical education. These sections of our questionnaires aim to collect students’ opinions about the nutrition education received during their undergraduate medical studies, their perceived importance of nutrition in medical teaching and practice, as well as the adequacy of nutrition training in medicine and students’ confidence in their nutrition knowledge and skills. We used questions derived from previously validated studies to assess students’ perceptions and attitudes regarding nutrition and the provision of nutritional care.24-27 For the responses, we used a 7-point Likert scale (Strongly disagree, disagree, somewhat disagree, neither agree nor disagree, somewhat agree, agree, strongly agree). For clarity in reading the results, we grouped the responses into 3 categories (Disagree, neither agree nor disagree, agree). To appreciate changes in opinions and perceptions between the beginning and end of the session, the scores from the 7-point Likert scale were also transformed into quantitative form.
Food Agency: The Cooking and Food Provisioning Action Scale (CAFPAS)
The Cooking and Food Provisioning Action Scale (CAFPAS) is a validated measurement28,29 based on the theoretical framework of “food agency.”28,30 The conceptual model of food agency helps understand individual abilities to acquire and prepare food in specific environments, contexts, and constraints. The CAFPAS includes 28 items grouped into 3 subscales (self-efficacy (items 1-13), attitude (items 14-23), structure (items 24-28)). We used a simpler calculation for the CAFPAS score than that of the authors. For each subscale, we employed the means of raw scores ranging from 1 to 7, and subsequently computed the means of these subscale means for the total score.
Meaning of Food and Eating Behavior Questionnaires (MFLQ)
The behavior of food consumers is a complex phenomenon determined by a multitude of factors that go beyond hunger or nutrition and often include personal, cultural, and religious values and ideals. People attribute different meaning to food which could predict their eating behavior. In their work, Arbit et al (2017) 31 identified 5 major meanings of food for people: moral, sacred, health, social, aesthetics. The MFLQ includes 22 items grouped into these 5 domains.
Eating Pleasure Questionnaire (EPQ)
The pleasure of eating is multidimensional. In their systematic review, Bédard et al 32 identified 89 sub-dimensions about eating pleasure, which they grouped into 22 key dimensions. They developed and validated the Eating Pleasure Questionnaire (EPQ) among Quebecers, 33 which includes 53 items grouped under a seven-factor structure: 1- health/ideological food choice motives, 2- sensory experiences and individual preferences, 3- social experiences, 4- mindful eating, 5- emotional/situational eating and reward, 6- food preparation process, 7- new experiences.
Statistical Analysis
The project’s objective was to quantify changes in participants’ responses to questionnaires from the beginning to the end of each session. The analyses primarily involve individual pre-post measures, that is, changes in scores on various questionnaires. Comparative analyses were conducted between CM and CG groups to highlight the evolution of changes. Specifically, the intervention’s effect was measured for each response variable using a repeated measures model with group effects (CG, CM), time (pre- and post-intervention), and group-by-time interaction. More specifically, a generalized linear model with an identity link and normal distribution was used, with generalized estimating equations to account for correlation over time. Only individuals who responded at both measurement times were retained for the analyses. Various comparisons of interest were made using contrasts: changes between pre- and post-intervention measurements for each of the 3 groups, followed by comparisons of pre-post changes between groups. All analyses were performed in SAS 9.4.
Results
A maximum of 12 students were admitted and exposed to the CM course during the fall 2022 session, and another 12 students were admitted during the winter 2023 session. All students in each session completed all the CM courses. However, only 11 students completed both the initial and final session questionnaires in both 2022 and 2023. This resulted in a total of 22 students being available for analysis in CM group. A total of 8 students from the CG completed the first questionnaire, but only 6 students completed both questionnaires.
Baseline Characteristics and Perceptions of Students From the Control Group (CG) and Culinary Medicine (CM) Course.
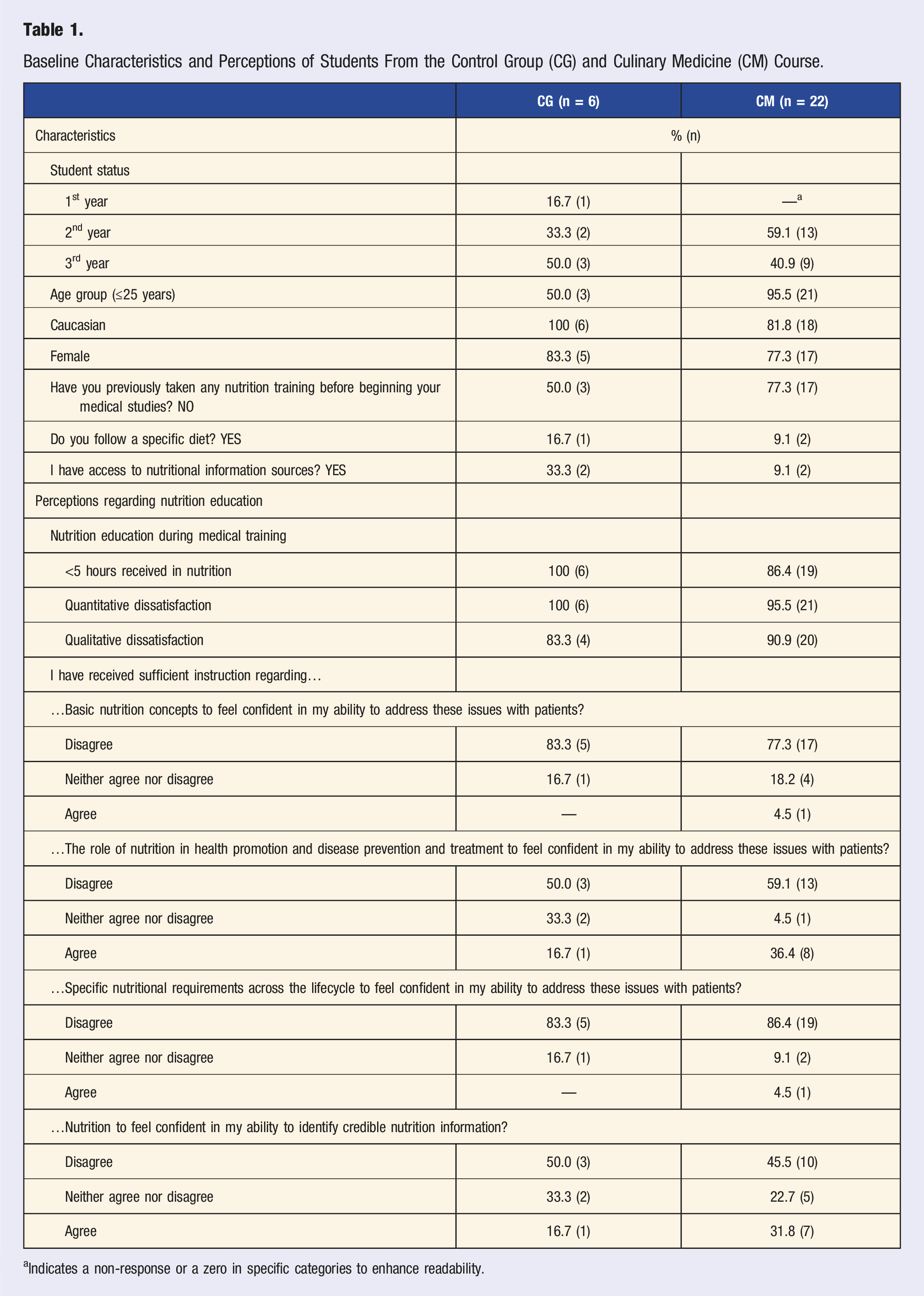
aIndicates a non-response or a zero in specific categories to enhance readability.
Perceptions of Participants Regarding Nutrition Education in Medicine
A large majority of participants (CM = 86.4%, CG = 100%) reported having received less than 5 hours of nutrition education during their medical training, including lectures, tutorials, workshops, and online learning (Table 1). Almost all participants expressed dissatisfaction with the nutrition education provided in medicine. When we asked, “What are the obstacles to improving nutrition education in the medical program?” the main obstacles reported were “lack of time” and “lack of awareness.” The majority (CM = 77.3%, CG = 83.3%) disagreed with the idea that the nutrition knowledge acquired during their training was sufficient to feel confident in their abilities to address these issues with patients for “Basic nutrition concepts” (Table 1). The majority (CM = 86.4%, CG = 83.3%) expressed disagreement regarding the sufficiency of knowledge acquired about “Specific nutritional requirements across the lifecycle.” Only 45.5% in CM and 50% in CG agreed on the fact that they received sufficient instruction regarding “nutrition to feel confident in my ability to identify credible nutrition information?”
Attitudes and Perceptions of Participants Regarding Nutrition in Medicine
Attitudes and Perceptions a Regarding Nutrition in Medicine, Scores and Changes of Students From the Control Group (CG) and Culinary Medicine (CM) Course.
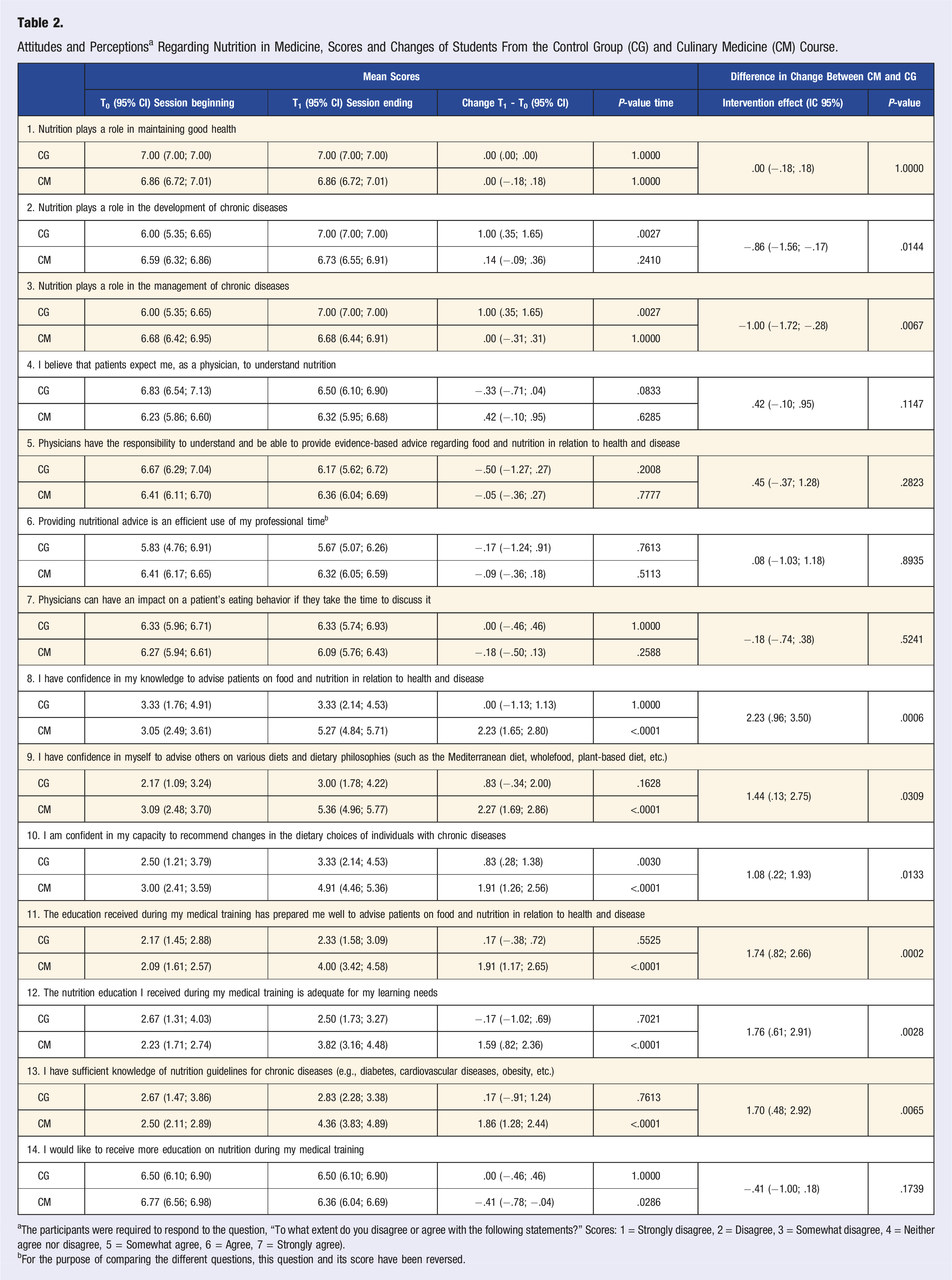
aThe participants were required to respond to the question, “To what extent do you disagree or agree with the following statements?” Scores: 1 = Strongly disagree, 2 = Disagree, 3 = Somewhat disagree, 4 = Neither agree nor disagree, 5 = Somewhat agree, 6 = Agree, 7 = Strongly agree).
bFor the purpose of comparing the different questions, this question and its score have been reversed.
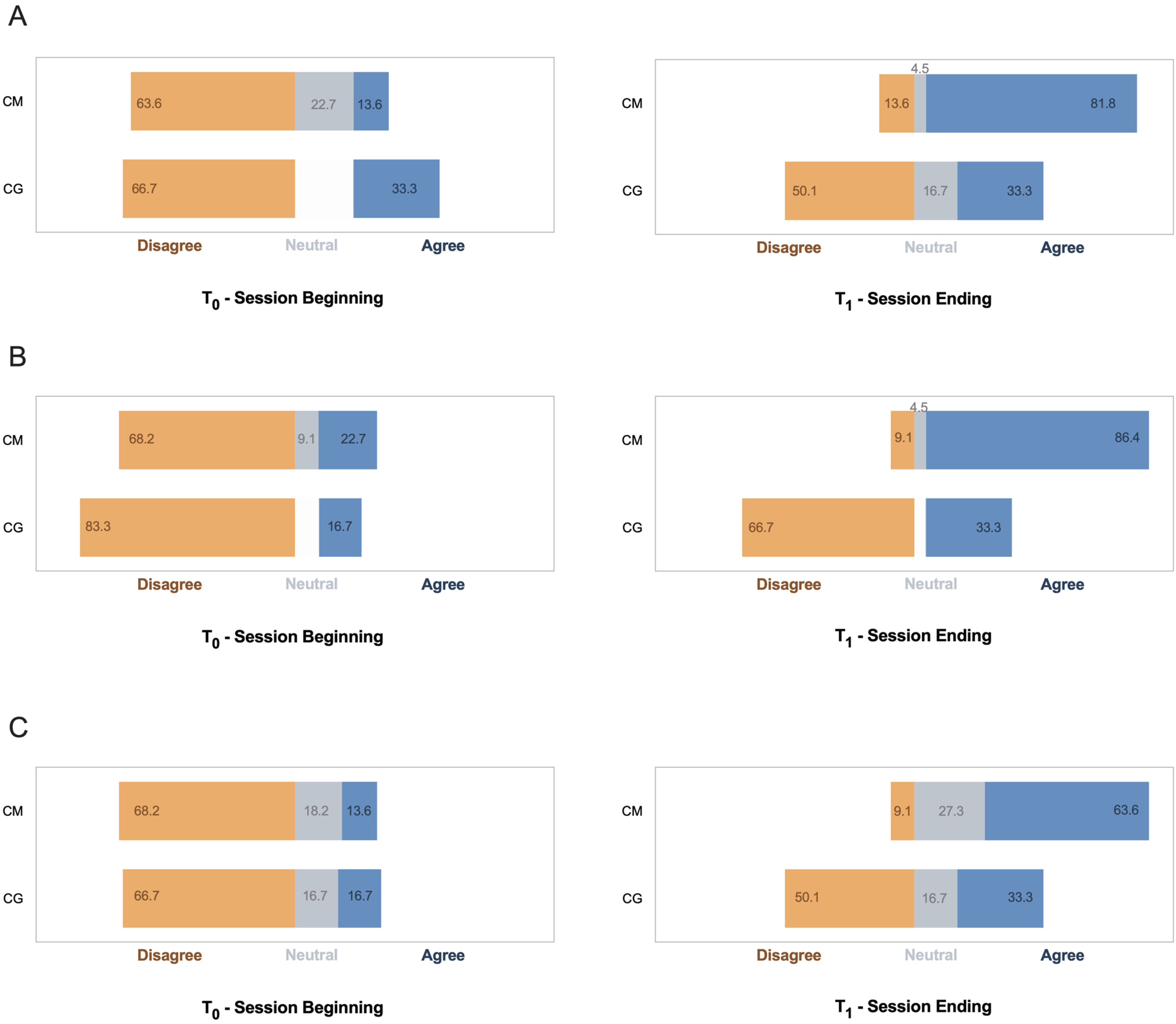
Confidence levels in the Culinary Medicine (CM) and control group (CG) before and after the session. (a) I have confidence in my knowledge to advise patients on food and nutrition in relation to health and disease? (b) I have confidence in myself to advise others on various diets and dietary philosophies (such as the Mediterranean diet, wholefood, plant-based diet, etc.)? (c) I am confident in my capacity to recommend changes in the dietary choices of individuals with chronic diseases?
At the beginning of the session, the majority of students in both groups disagreed with the statements “The education received during my medical training has prepared me well to advise patients on food and nutrition in relation to health and disease” and “The nutrition education I received during my medical training is adequate for my learning needs.” A noteworthy improvement in their attitudes was observed at the end of the session for students in the CM courses, whereas no such improvement was noted in the CG (Table 2). All students, regardless of the group, concurred on the need for more education on nutrition during their medical training.
Food Agency: the Cooking and Food Provisioning Action Scale (CAFPAS)
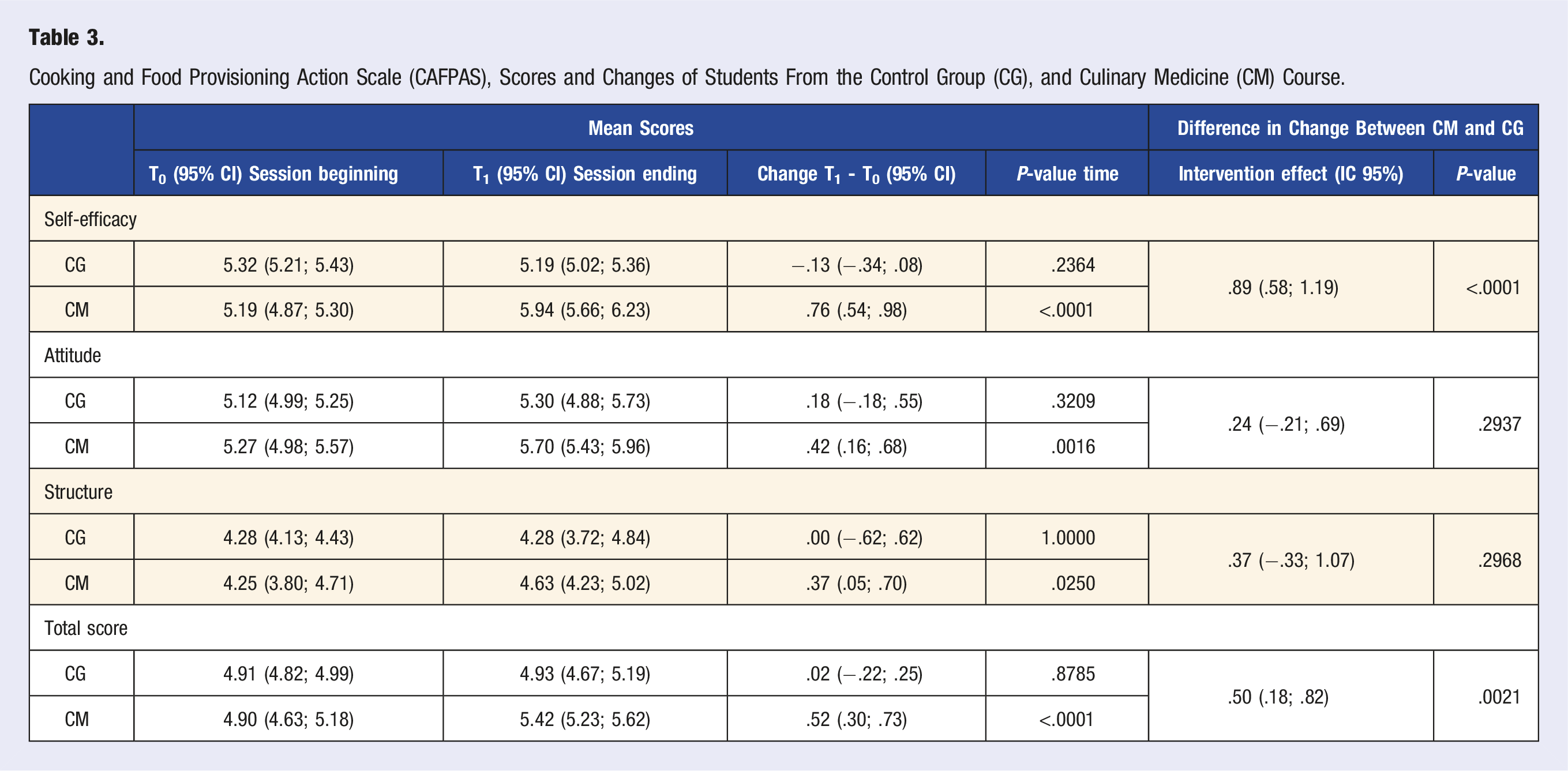
Cooking and Food Provisioning Action Scale (CAFPAS), Scores and Changes of Students From the Control Group (CG), and Culinary Medicine (CM) Course.
Meaning of Food and Eating Behavior Questionnaires (MFLQ) and Eating Pleasure Questionnaire (EPQ)
No statistically significant difference in the change between CM and CG was observed concerning scores on the MFLQ (Supplemental Material Table S4) and EPQ (Supplemental Material Table S5). However, an improvement in the MFLQ scores of all the subscales was noted for the CM group. The subscale on “Sacred” depicted the lowest score among all groups. No statistically significant change was observed in the EPQ for both CM and CG.
Discussion
Among medical students in their 2-3rd year in medicine school at Laval University, our observations highlight the fact that the majority students perceive the amount of nutrition education as insufficient, and this dissatisfaction is also reflected in the quality of the education received. A large majority indicate that they received less than 5 hours of nutrition education during their medicine school. The majority believe that their undergraduate program should allocate more time to nutrition education. Students unanimously acknowledge that nutrition plays a crucial role in maintaining good health, the development of chronic diseases, and their management. They are aware that patients expect them to have a substantial understanding of dietary concepts as physicians. They also share the conviction that physicians have the responsibility to comprehend nutrition and provide evidence-based dietary advice. They consider this as an efficient use of their professional time and believe that they can influence patients’ eating behavior if they dedicate time to discuss it. CM students demonstrated an important and statistically significant shift in attitude over the course, while the CG exhibited no change. Statistically significant improvements in CAFPAS were observed in the CM group, while no such changes were noted in the CG.
In our study, we used 4 questions about perceptions regarding nutrition education (Table 1) from a validated questionnaire used in a study among 9 medical schools in Canada between January and July 2008. 25 This survey targeted students with at least 8 months of medical education (mostly second/third year, 21-28 years old, 65% female). Compared to these Canadian students, ours (CM & CG) reported significantly lower confidence in addressing nutrition topics with patients. For example, only 3.6% felt prepared for “basic nutrition concepts” compared to 70% in the Canadian survey (similar trends observed for other perceptions). This difference might be due to number of years in the medical program (our students were mostly in their second year, Canadians in their third or fourth year) or program variations. Notably, both studies found overwhelming student agreement on needing more nutrition education in medicine, mirroring a 2009 CMAJ article titled “Canadian medical students want more nutrition instruction.” 34
At the beginning of the session, a high proportion of students expressed low confidence in their ability to advise patients on food and nutrition in relation to health and disease, to advise others on various diets and dietary philosophies, and to recommend changes in the dietary choices of individuals with chronic diseases (Table 2, Figure 1). Similar observations have been noted previously among medical students. A systematic review of 24 studies (2012-2018) on nutrition education for medical students found insufficient integration of nutrition curricula, regardless of region, setting, or year of study. 3 This lack of training, despite nutrition’s role in healthy living, impacts students’ skills and confidence in providing nutritional care. 3
The situation appears to be similar among medical students and trainee doctors in United Kingdom (n = 853). 27 The survey results indicated that 99% of respondents believe that nutrition plays a significant role in maintaining good health and most of them agree with the physician’s role in nutritional care and expressed a desire for more education on the subject. Regarding the statement “my medical school has prepared me (or is preparing me) to advise patients on food and nutrition in relation to health and disease,” only 12% agree or strongly agree with this statement. In our study, only 1 student over 28 (3.6%) agreed with this statement at the beginning of the session (Q11, Table S3 in Supplemental material). Among students in the CM course, we noted a remarkable and statistically significant shift in attitude over the course, especially increase in confidence (Table 3, Q8 to Q10) and perception that the nutrition education received is adequate and better prepares them to advise patients (Table 3, Q11 to Q13), while these confidences and perceptions remain similar across the session in the CG.
Newman et al 35 recently conducted a scoping review of the literature (articles published between January 1, 2012, and October 15, 2021) on CM programs for medical students. Twelve included studies revealed diverse CM program formats, encompassing factors like student level, participant numbers, course duration/structure, and instructor backgrounds. The diversity is also observed in the outcome evaluations. Some studies noted an improvement of confidence in counseling or discussing nutrition with patient and better understanding of nutrition,36-44 cooking abilities and food preparation,37,42,44,45 and healthy diet changes (more fruits, vegetables, homemade meals, and less meat).39,40,42-44 One of the major limitations noted is the absence of control groups in the analyses.
One of the oldest and most widespread CM programs is the CHOP program (Cooking for Health Optimization with Patients) at the Goldring Center for Culinary Medicine (Tulane University, New Orleans, Louisiana).39,40 This study has the largest number of participants and includes a control group. According to their results, participants in the CHOP program were 82% more likely to adhere to the Mediterranean diet than those receiving traditional nutritional education (Odds Ratio (OR) = 1.82; P < .001). 46 Compared to controls, CHOP program participants are more likely to meet daily recommendations for fruits (OR = 1.33; P = .019) and vegetables (OR = 2.06; P < .001), more frequently agree that nutrition advice should be a routine component of clinical care (OR = 2.43; P < .001), and that physician advice can improve patients’ dietary habits (OR = 1.62; P < .001). Both CHOP and Laval University’s CM programs aim to improve dietary behaviors in healthcare professionals, utilizing online modules, teamwork, cooking, and case studies. However, they differ in focus, approach, and length. CHOP is a shorter program (32 hours delivered in 8 4-hour modules) centered on the Mediterranean diet and a nutrients-based approach. In contrast, Laval University’s program is longer (55 hours over 15 weeks), emphasizing hands-on cooking classes (32 hours) and adopting a broader nutritional education approach (23 hours) not solely based on nutrients (see Supplemental Table S1).
Evidence suggests that an increase in culinary skills and knowledge of food provisioning would improve food choices, diet quality, and health outcomes.28,29 This body of literature also suggests that improving dietary outcomes goes beyond education about nutritional information. Recent data from surveys conducted with national samples of adults and parents in the U.S. (n = 2856) show that higher food agency (CAFPAS score) is associated with a higher frequency of preparing all meals, more frequent meal preparation from scratch, and less frequent preparation with packaged ingredients. 30 Higher food agency is also associated with increased consumption of fruits and vegetables and reduced intake of fries and sugary beverages.
Food agency was not assessed in any of the CM studies cited in the scoping review by Newman et al 35 To our knowledge, the CAFPAS (a food agency scale) has never been used in a CM intervention or with a group of medical students. Our analyses show that total scores on the CAFPAS scale and all subscales significantly improve in the CM, while the CG shows no significant change. The “structure (items 24-28)” subscale evaluates notably the “structural (social) barriers” related to time management for meal planning and preparation. This is an important aspect as it shows that culinary skills and dietary behaviors do not occur in a vacuum, and the ability to put them into practice in daily life, in other words, to be an active agent (agency concept), depends on other contextual factors such as available time for cooking, work schedules, and responsibilities. For medical students, who have a very busy academic schedule, this requires significant awareness and prioritization of an activity to allocate more time to it, which is hardly easy for them. The only statistically significant difference observed in the change between CM and CG is related to “self-efficacy” items, which drove the overall significant difference in scores.
In our initial objectives regarding CM course, we planned to measure students’ dietary intake at the beginning and end of the session using a targeted food intake journal. Unfortunately, few students completed and returned their food journals. This observation suggests that obtaining feedback on certain questionnaires from students, especially during a busy session, is challenging, especially for most dietary questionnaires, which are tedious and time-consuming. Therefore, it would be necessary to consider alternative methods (e.g., very short questionnaire) or periods to gather valuable information on students’ dietary intake changes during the session.
No statistically significant differences were found in the change between CM and CG regarding MFLQ and EPQ scores (Table S4 and S5 in Supplemental material). However, the CM depicts a statistically significant improvement in the 5 domains of MFLQ. Except for “Social” subscale, no statistically significant improvement is observed in CG. No statistically significant improvement was noted for EPQ subscales and total scores. The MFLQ 31 assess the various aspects of meaning individuals derive from their connection with food whereas the EPQ 33 assess eating pleasure dimensions. Our observations suggest 2 possibilities: either the intervention has no effect on EPQ values, or this questionnaire is not very sensitive or adequate for measuring changes resulting from interventions. However, the study design did not aim to address changes the pleasure of eating but rather focused on developing attitudes and perception regarding nutrition, food agency, as well as a healthy relationship with food. Other questionnaires than the EPQ may be better suited for the purpose of addressing a healthy relationship with food. However, we observed that the “Sacred” subscale of the MFLQ consistently registers a score significantly lower than all other categories by a substantial margin. As the sacred nature of food is deeply rooted in most religions and doctrines, where food carries meanings, taboos, or prohibitions, 47 thus creating a set of immutable beliefs, this observation among medical students might suggest a finding that appears favorable to dietary changes.
In line with the conclusions of the recent scoping review on CM, 35 it is important to consider the weaknesses of studies on CM to enhance knowledge and evidence regarding its role in the nutritional education of physicians and healthcare professionals. The absence of comparison groups and the use of validated assessments are significant limitations in the studies in this field, which is not the case in our study. We recognize the limited size of our CG, but obtaining control participants in studies of this nature poses a challenge. All measures included in our studies are self-reported and may be subject to reporting, social desirability, and recall biases. It is important to clarify that our samples are not intended to be representative of medical students. Nevertheless, the consistency of our observations with those of other surveys conducted among medical students in Canada and worldwide reinforce our findings, providing reassurance in terms of data reliability. In the realm of this emerging CM discipline, neuropedagogy 48 remains unexplored. The integration of neuropedagogy could provide avenues for a lasting improvement in individual learning and behavior related to CM.
Conclusion
Our findings suggest that medical students acknowledge the significance of nutrition education but identify gaps in their training, expressing reluctance to discuss nutrition with patients and recognizing their limitations in this domain. Students unanimously expressed a desire for more nutrition education during their medical training. Our study reveals the positive impact of the CM course, indicating a substantial shift in students’ attitude and confidence in nutrition, progressing from a low level initially to a very high level by the end of the session. Our CM course also underscores the potential for a significant improvement in food agency. The conclusions drawn from the CM course highlight the feasibility of addressing both theoretical and practical aspects of nutrition while employing an active pedagogical approach, providing valuable insights for medical schools and education authorities aiming to enhance the nutrition education of future physicians.
Supplemental Material
Supplemental Material - Improvement in Nutritional Knowledge Confidence and Food-Agency: Outcomes of the First French-Speaking Culinary Medicine Courses Among Medical Students
Supplemental Material for Improvement in Nutritional Knowledge Confidence and Food Agency: Outcomes of the First French-Speaking Culinary Medicine Courses Among Medical Students by Sylvie Dodin, Catherine Bégin, and Michel Lucas in American Journal of Lifestyle Medicine
Footnotes
Author Contributions
Conceptualization: SD, ML; Methodology: SD, ML; Statistical analysis: ML; Writing—original draft preparation: SD, CB, ML; Writing—review and editing: SD, CB, ML; Supervision: ML; Project administration: SD, ML. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the “Fonds Gilles Cormier. Programme d’innovation pédagogique des sciences de la santé. Faculté de médecine, Université Laval” and the “Fonds d’approche intégrée en santé des femmes. Faculté de médecine, Université Laval.”
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.