
Abstract
Occupational therapists (OT) are trained in interventions related to health and well-being, facilitating individuals in achieving occupational balance. This scoping review explored the current methods of disseminating Lifestyle Medicine (LM) knowledge in post-secondary health education and assessed the potential integration of LM principles into OT education. The review covered publications related to LM implementation in post-secondary health professions curricula. Six databases were searched. The authors conducted initial blind reviews of titles and abstracts, followed by a similar screening of full-text articles. Included full-text articles were obtained from university databases with the assistance of systematic review software. Among the 304 abstracts reviewed, 60 full-text articles were assessed, with 16 included in this scoping review. However, none of the programs in the literature were OT programs. The results show that the six pillars of lifestyle medicine were not equally emphasized in the reviewed programs, with social connection being the least addressed. However, OT education places importance on social connections, and the other pillars align well with the 2018 standards set by Accreditation Council of OT Education (ACOTE) and the parameters outlined in OT Practice Framework 4th Edition (OTFP-4). This alignment can be valuable for OT programs in meeting their accreditation requirements.
“The models currently taught in occupational therapy education encourage students to consider social connection within a client’s context.”
Introduction
Every day, there is an opportunity to make a decision that will positively impact one’s health and quality of life. What if every healthcare provider had the education, the resources, and the evidence to practice preventive medicine and support positive lifestyle decisions? With the American College of Lifestyle Medicine, health providers, such as occupational therapists can access the evidence, training, and resources that support people, communities, and populations in making decisions that positively impact their health for years to come. Occupational therapy professionals use meaningful engagement in roles, routines, and every day occupations to support their clients in health maintenance and health promotion, aligning with the goal of positive lifestyle decisions and action within the American College of Lifestyle Medicine. 1
Occupational therapy practitioners are educated on, trained in, and utilize interventions that address health and wellness, and support individuals in their journey towards a meaningful participation in their environments including the physical, cultural, institutional, social, and socioeconomic. Occupational therapists use engagement in valued occupations such as self-care, rest, work, and education as a means or intervention to manage health and view the occupation of health management as an ends or outcome when considering overall health and well-being. Imbalance among occupations or lack of access to an occupation can disrupt wellness. 2 In occupational therapy education, theoretical frameworks3–6 are used to help students and clinicians explore comprehensive approaches to wellness that support people, communities, and populations. Some models support the goal of health and well-being through the whole person in their appropriate context. 4
Occupational therapists could have a pivotal role in advancing preventive health and overall well-being. They possess a keen understanding of the intricate relationship between the environment, culture, and an individual’s life experiences. They provide tangible, hands-on interventions to empower individuals, communities, and entire populations in their pursuit of positive lifestyle changes.2,6 While there is work to do to expand the role occupational therapists have in the promotion of health and well-being, the profession is committed to health promotion, as demonstrated by the American Occupational Therapy Association (AOTA) statement on “Occupational Therapy in the Promotion of Health and Well-Being.” In this statement AOTA defines critical roles for occupational therapists in health promotion and prevention, such as promoting healthy occupations and lifestyles for everyone and incorporating occupation in health promotion strategies. Some examples of prevention interventions approaches utilized by occupational therapists include education and training on eating habits and physical activity. 2
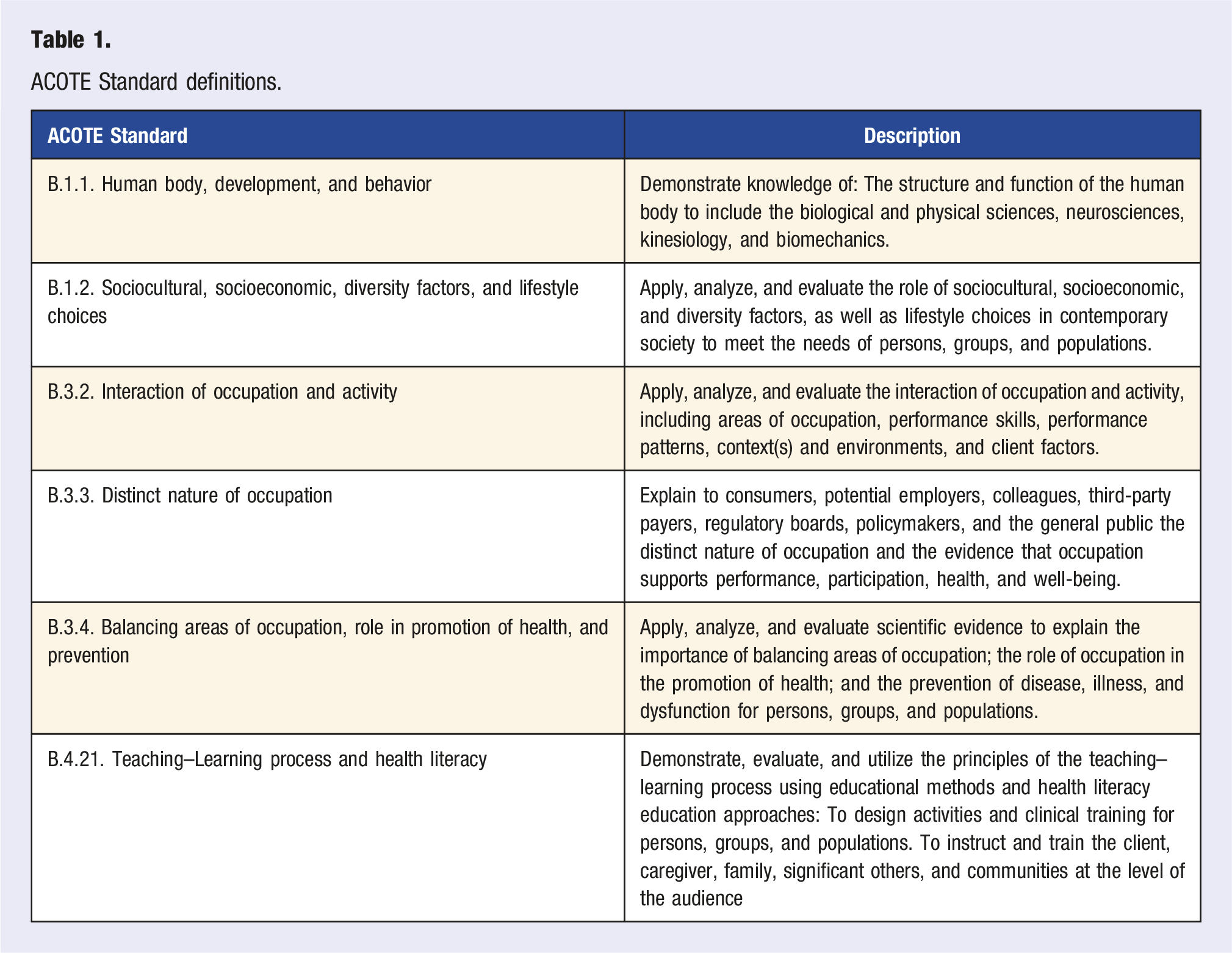
ACOTE Standard definitions.
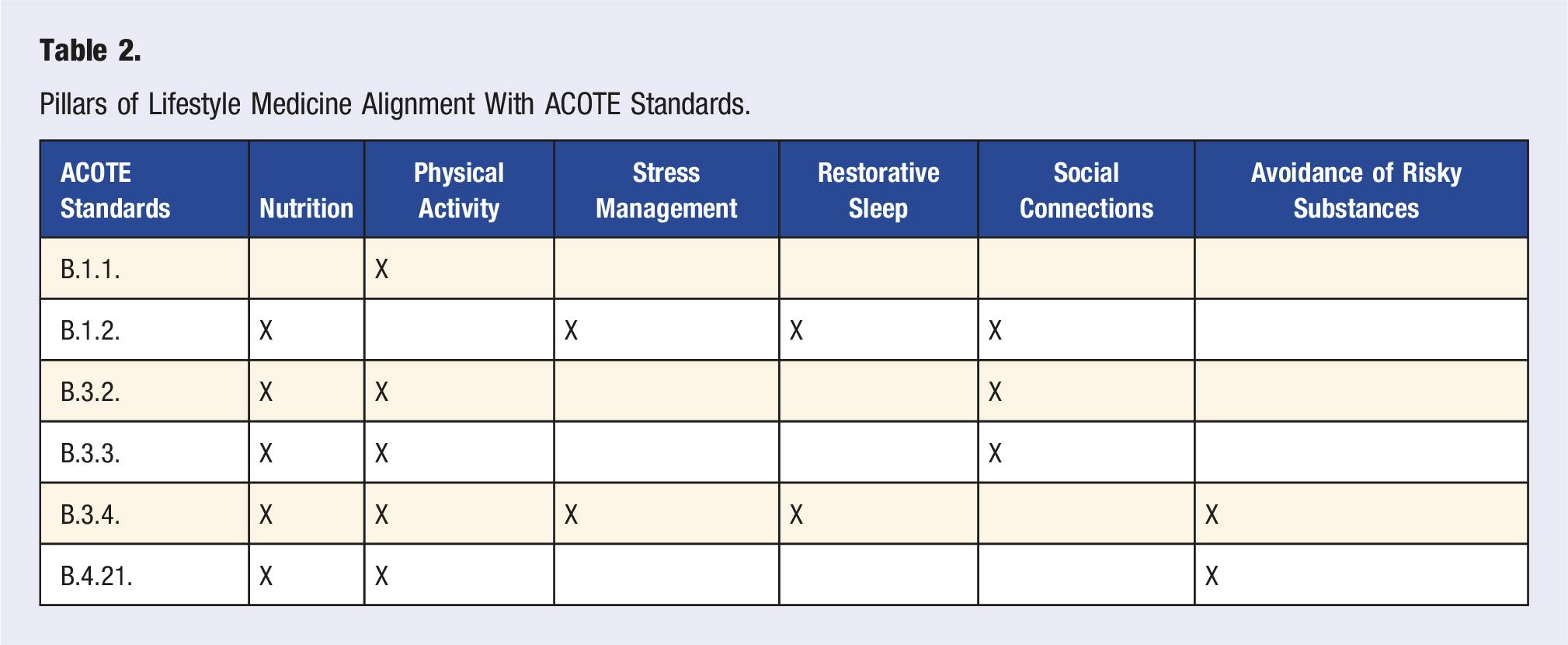
Pillars of Lifestyle Medicine Alignment With ACOTE Standards.
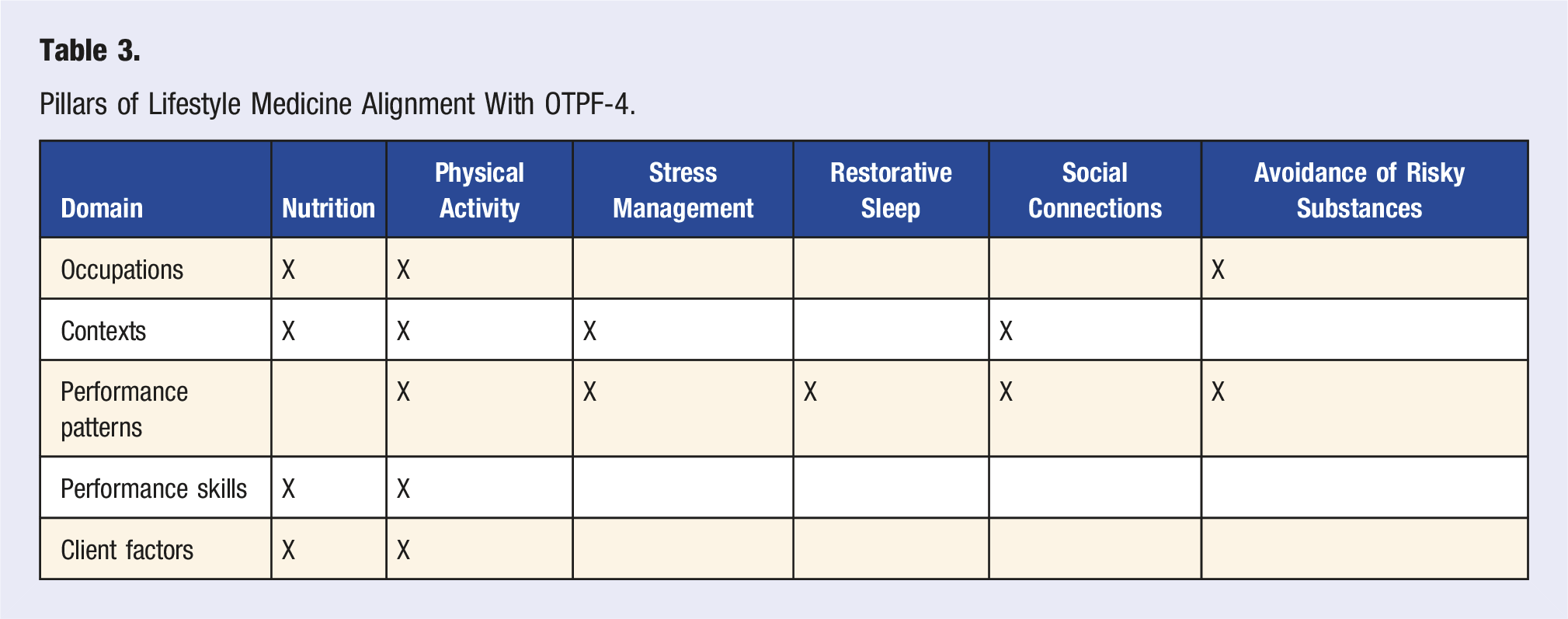
Pillars of Lifestyle Medicine Alignment With OTPF-4.
Despite these alignments, there exists a notable gap in the existing evidence regarding the integration of lifestyle medicine into occupational therapy curricula. In contrast, several other health science professions, such as physician, physician assistant, and pharmacy programs, have successfully integrated lifestyle medicine principles into their programs, showcasing the feasibility of incorporating these insights into occupational therapy education. This integration would equip OT students with a versatile toolkit to effectively address various aspects of client well-being, bridging the gap between profession-specific knowledge and emerging evidence from the field of lifestyle medicine.
The purpose of this scoping review was to investigate current approaches to disseminating lifestyle medicine knowledge within post-secondary health education and describing the potential of integrating LM principles into occupational therapy education.
Methods
The protocol for this scoping review was published through the Open Science Framework (OSF) on 3 July 2023 to support the systematic literature review. The content of this scoping review is reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines for Scoping Reviews (PRISMA-ScR) guidelines. 11 Due to the nature of a scoping review, no risk of bias evaluation was performed.
Search Strategy and Review Criteria
Database and Search Strategy.
Study Selection
Two authors (ALP & AMR) discussed the inclusion and exclusion criteria prior to screening. Following this, all titles and abstracts were blindly screened for eligibility by these authors. Full-text articles were recovered, and each full text was blindly screened by both authors. Title and abstract and full-text article disputes were resolved via discussion between the two authors. Included full-text articles were retrieved through the university online database (i.e., MEDLINE, Ovid, etc.) and PubMed Central. Title and abstract screening and full-text screening were performed using the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia).
Data Extraction
When creating the review protocol, ALP and AMR identified the data that needed to be extracted from the articles. After this, an existing data extraction template was edited on Covidence systematic review software. Two authors extracted data for each study using this pre-designed template. After both authors extracted data from all papers, the data was compared, and disagreements were resolved through discussion. Data extraction included the author, title, year, country, type of health profession and/or the department the profession is within, name of the institution, how many courses implement Lifestyle Medicine education, in what stage of post-secondary education Lifestyle Medicine is taught, the pillars of Lifestyle Medicine addressed, whether the course is a core part of curriculum or elective, credit hours of the course(s), whether the education is didactic or experiential(application/residency/patient care etc.), if there is a partial pathway for Lifestyle Medicine certification, and if available: competencies, assignments, and assessment related to Lifestyle Medicine.
Results
From the 304 study abstracts screened, 60 full-text articles were reviewed, and 16 were included in this scoping review. This process is illustrated in Figure 1 with a modified PRISMA diagram.
11
To analyze the data extracted from these papers, frequency counts and percentages were used to present the data. Out of the 16 papers, 20 program were mentioned; 3 papers did not provide the department; 4 programs did not provide a total number of courses; and 1 paper did not specify whether their lifestyle medicine courses were core or elective courses. The study characteristics are presented in Table 5, with Physician being the health profession that used lifestyle medicine curriculums the most. No occupational therapy program curriculums were found. A modified PRISMA diagram. Study Characteristics.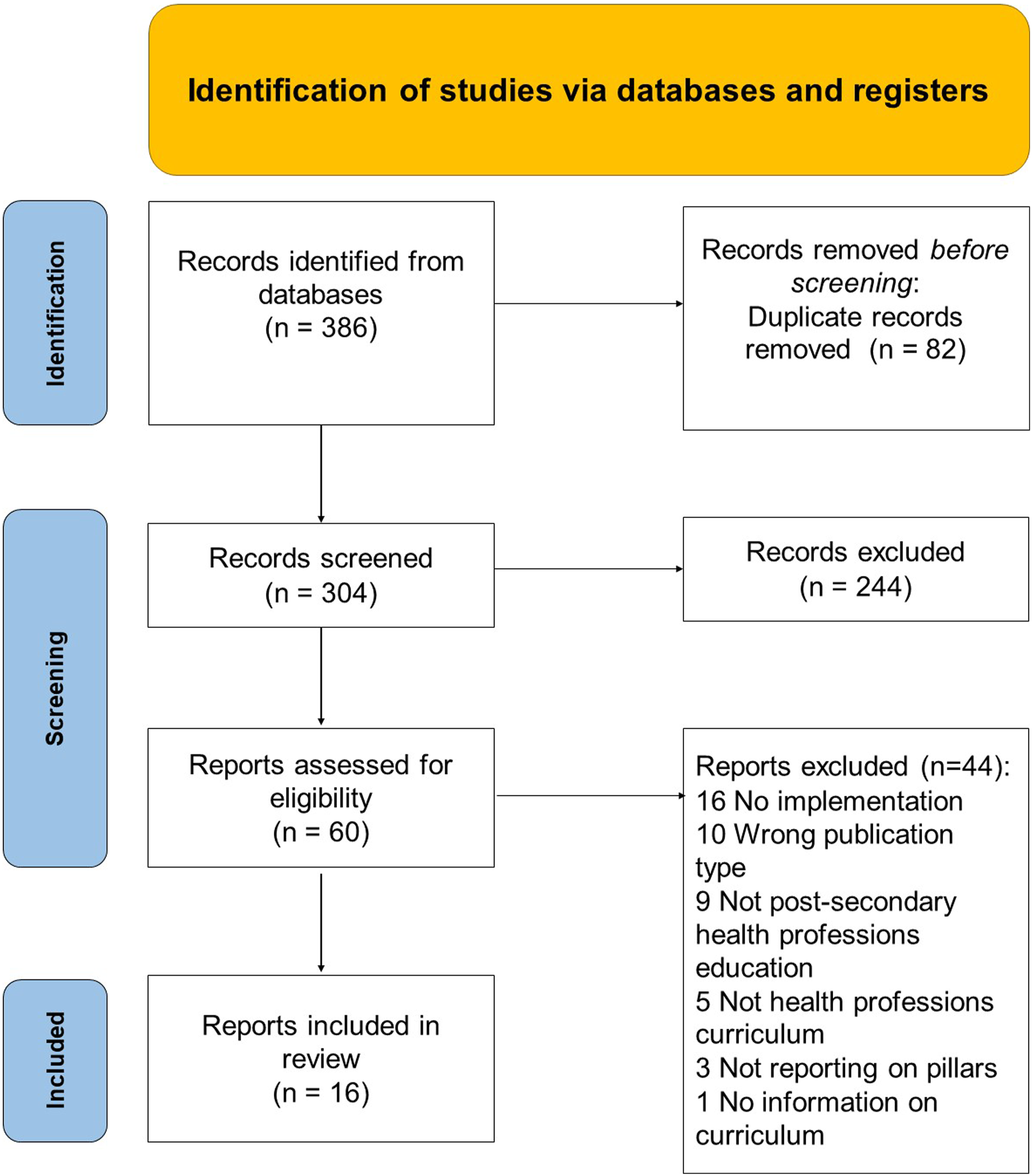
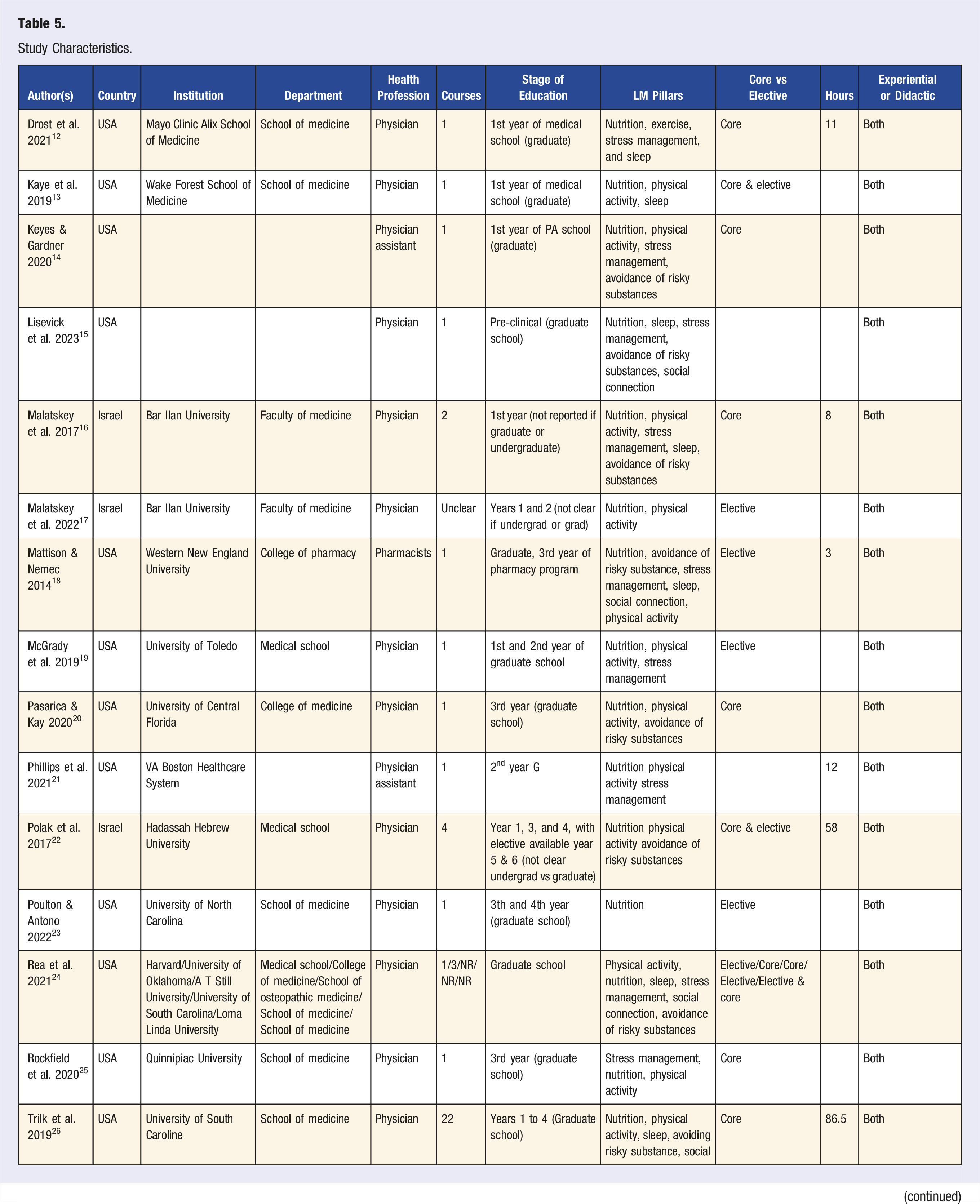
The pillars (Figure 2) covered in lifestyle medicine curriculum include Nutrition, Physical Activity, Stress Management, Avoidance of Risky Substances, Restorative Sleep, and Social Connection, with Social Connection being the least utilized in Lifestyle Medicine curriculum. The information extracted from each article, including: the number of courses covering lifestyle medicine, whether they are core or elective, the hours of content, and whether the content was experiential or didactic is presented in Table 5. Over half, 60% of programs that include lifestyle medicine in their curriculum have lifestyle medicine as a core component and of all of the programs, 95% include both experiential and didactic education on lifestyle medicine. A visual depiction of how many programs cover each LM pillar.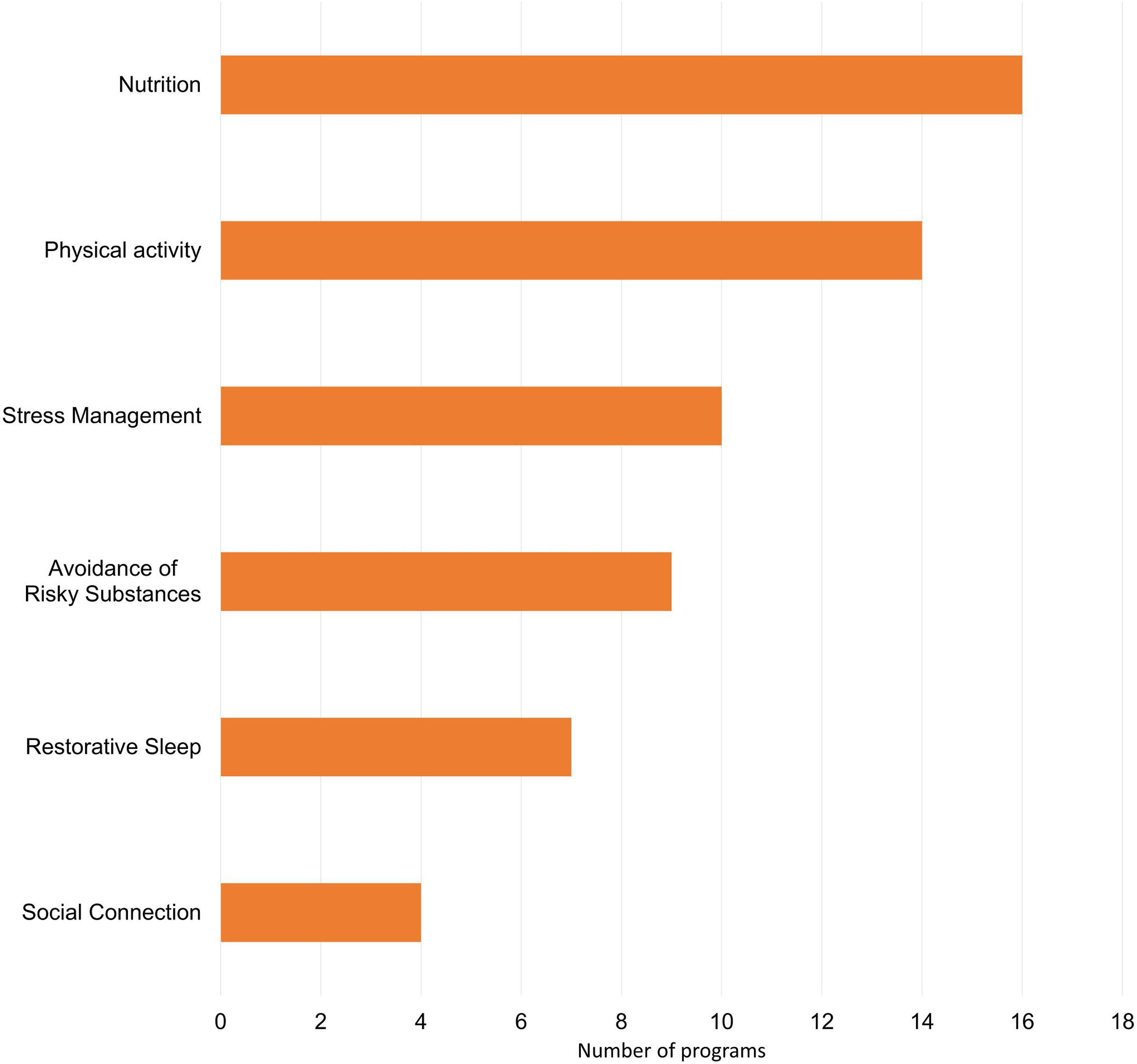
Lifestyle Medicine Competencies and Assignment Examples.
Discussion
While no articles were found that explore lifestyle medicine in occupational therapy education, this discussion will use the findings from the included papers to consider how lifestyle medicine education may be applicable in occupational therapy education. The pillars of lifestyle medicine can enhance the content of occupational therapy programs, while conversely, occupational therapy education can provide support for lifestyle medicine education. The six pillars of lifestyle medicine can be aligned with the 2018 standards set forth by the ACOTE, 9 alongside the parameters delineated in the OTFP-4. 10 While the OTPF-4 serves as a structure for practice, occupational therapy modules that are commonly taught in occupational therapy education support approaches to wellness that are preventative and focused on individuals, communities, and entire populations. This confluence of resources and foundational knowledge can serve as valuable tools for occupational therapy programs to meet accreditation requirements while simultaneously elevating the less-emphasized aspects of lifestyle medicine. This section delves into the underrepresented pillars among programs incorporating lifestyle medicine in their curricula, explains connections between lifestyle medicine competencies and established occupational therapy curricula, and explores the instrumental role of the occupational therapy perspective in supporting lifestyle medicine education.
Least Utilized Pillars
The findings from this scoping review highlight that the Social Connection Pillar received the least attention, with the Restorative Sleep pillar following closely behind. The Social Connections pillar emphasizes the importance of fostering positive relationships with others. In occupational therapy education, students are instructed to use the OTPF-4 framework to assist clients in enhancing their social connections, thereby enhancing their physical, mental, and emotional well-being. The models currently taught in occupational therapy education encourage students to consider social connection within a client’s context. The Ecology of Human Performance facilitates consideration of a client’s skills or abilities to engage in social connection. Whereas the Person-Environment-Occupation-Performance model guides students to examine the characteristics of a person, features of the environment, and characteristics of activity associated with social connection. Furthermore, this approach aids occupational therapy programs in fulfilling ACOTE standards concerning sociocultural factors, areas of occupation, and the distinct nature of occupation. Occupational therapy students can utilize resources from the Social Connections pillar combined with guidance from the OTPF-4 and occupation therapy models to improve social connections of clients. At the same time, occupational therapy programs can highlight the effectiveness of this combined approach by generating evidence that can inform lifestyle medicine practices. This can facilitate collaborative efforts that are beneficial to both lifestyle medicine and occupational therapy.
Within the OTPF-4 framework, sleep quality is considered an integral aspect of daily life and habits, thus falling under the category of performance patterns. Occupational therapy students are taught the significance of establishing a consistent sleep routine, recognizing that adequate sleep is essential for everyone. The Restorative Sleep pillar within lifestyle medicine primarily focuses on enhancing attention span, mood, and mitigating issues such as insulin resistance and hunger through the attainment of high-quality sleep. The focus of this pillar is similar to Model of Human Occupations where clients make changes to their occupations based on interactions with the environment. The prevention piece from this pillar could serve as the catalyst that has an impact on the occupation of sleeping. Integrating resources from this pillar into an occupational therapy curriculum would be instrumental in aligning with ACOTE standards related to lifestyle choices and preventive measures for addressing health concerns. This could serve as the basis for further collaboration with professions that specialize in sleep issues.
The Avoidance of Risky Substances pillar, utilized by slightly more than half of the programs in the scoping review, advises against excessive tobacco and alcohol consumption to decrease the risk of chronic diseases and death. Occupational therapy students are instructed in this principle to equip them with the knowledge needed to guide their future clients in maintaining a balanced and health-conscious lifestyle, aligning with the standards set by the ACOTE. The preparation of OT students in this regard also adheres to the performance patterns of habits and routines, as well as the occupations of leisure and health management as outlined in OTPF-4. Lifestyle medicine could be utilized to help OT students learn how to address and prevent the habits and routines that lead to use of risky substances.
Most Utilized Pillars
All 20 programs included in the scoping review integrated the nutrition pillar into their curriculum. Following closely, the second most emphasized pillar was physical activity, with stress management ranking as the third most emphasized pillar. These three pillars can also be paired closely with the OTPF-4 and the education requirements of the ACOTE standards.
The nutrition pillar in lifestyle medicine emphasizes the importance of a plant-based diet for health prevention and management. OT students need to understand the significance of nutrition to guide their future clients in making healthy dietary choices and appreciating the impact of diet on health. They should also consider the need for adjusting daily habits and routines influenced by values and beliefs when helping clients adopt dietary guidelines. This aligns with the standards set by ACOTE and addresses activities of daily living and Health Management domains outlined in OTPF-4.
The physical activity pillar in lifestyle medicine emphasizes the importance of regular physical activity for overall well-being. OT students are required to incorporate physical activity considerations into their client assessments, treatments, and education, which aligns with specific ACOTE standards. These standards encompass understanding human body structure and function, the relationship between occupation and activity, the unique nature of occupation, balancing various areas of occupation, and the role of occupation in health promotion and prevention. These principles closely correlate with the physical activity pillar, which can be applied to various occupations through the OTPF-4, including activities of daily living, health management, play, leisure, and social participation. This also involves comprehending client factors such as values, beliefs, body functions, and body structures.
The stress management pillar in lifestyle medicine emphasizes the importance of effectively addressing negative stress to enhance overall well-being by reducing anxiety, depression, and immune-related issues. This pillar aligns with several ACOTE standards, encompassing sociocultural, socioeconomic, diversity factors, and lifestyle choices, as well as the balance of different areas of occupation and the role of occupational therapy in health promotion and prevention. As occupational therapy students learn to assist clients in managing stress, they must possess the tools and strategies to address potential stressors arising from various sources, individually or in combination. They should also understand the challenges clients face in balancing different aspects of daily life. Moreover, students must appreciate their role in promoting health and preventing issues, necessitating a deep understanding of clients' personal and environmental factors, habits, routines, roles, and beliefs, as outlined in the OTPF-4. Recognizing clients' values and beliefs is vital for crafting effective stress management plans, and the stress management pillar in lifestyle medicine provides valuable additional resources to aid students in this process.
Competencies
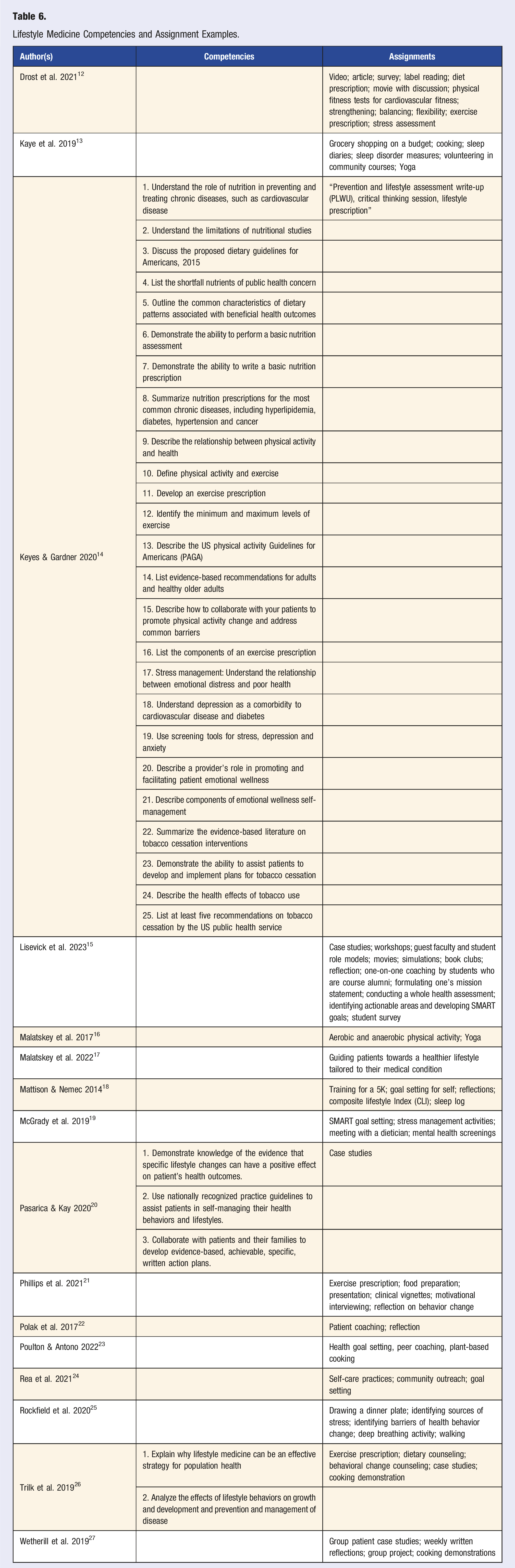
Some of the reviewed articles, Pasarica, 20 Keyes, 14 Trilk, 26 and Wetherill, 27 include competencies used for assessing student comprehension of the components of LM. Many of these competencies pertain to domains within the occupational therapy scope of practice. Utilizing these competencies has the potential to fulfill the standards and guidelines set forth by ACOTE and the OTPF-4.
Pasarica 20 defined three lifestyle medicine competencies, the first being that students need to be able to “demonstrate knowledge of evidence that specific lifestyle changes can have a positive effect on patient health outcomes.” The second competency is that students need to be able to “use nationally recognized practice guidelines to assist patients in self-managing their health behaviors and lifestyle.” While the third competency indicated that students need to “collaborate with patients and their families to develop evidence-based, achievable, specific, written action plans.” The competencies outlined by Pasarica are in alignment with both ACOTE standards and OTPF-4. The first competency parallels the emphasis on evidence-based practice articulated in the standards and practice framework. The second competency corresponds with ACOTE standards B.3.4. and B.4.21, emphasizing health promotion, prevention, and health literacy, while also addressing the performance patterns of habits and routines as established by OTPF-4.9,10 The third competency shares similarities with the client-centered nature of occupational therapy.
Similarly, Keyes 14 and Trilk 26 encompass competencies appropriate for assessing occupational therapy students on ACOTE standards B.3.4., B.4.21., and the performance patterns domain in the OTPF-4. The competencies delineated by Keyes and Trilk have potential to address ACOTE standards concerning sociocultural and socioeconomic factors. Specifically, one of the competencies requires students to list the shortfall of nutrient intake as a public health concern and demonstrate knowledge of the role of nutrition in the prevention of chronic diseases.
Pasarica, 20 Keyes, 14 and Trilk 26 employed specific competencies in their assessments. In contrast, Wetherill 27 utilized quizzes and a final examination to assess student proficiency in LM. OT education uses a combination of competency-based assessment along with quizzes and final exams to determine student competency of ACOTE standards and OTFP-4 guidelines.
The alignment between the ACOTE standards and OTPF-4 is further substantiated by consistency with the recently revised lifestyle medicine competencies in the article by Lianov. 28 Among the 88 identified competencies, those within the domains of The Role of the Practitioner’s Personal Health and Community Advocacy; Physical Activity Science, Assessment, and Prescription; Sleep Health Science and Interventions; Fundamentals of Health Behavior Change; and Emotional and Mental Health Assessment and Intervention exhibit the closest alignment with OT education. Specifically, these competencies resonate with ACOTE standards B.1.2., B.3.2., B.3.3., B.3.4., and B.4.21., as well as with the Context, Performance Patterns, and Client Factors domains within the OTPF-4.
A Summary of The Occupational Therapy Perspective
Occupational therapists approach preventive health from a client-centered standpoint. While the pillars of lifestyle medicine can contribute to occupational therapy education, the occupational therapy perspective can reciprocally influence lifestyle medicine education. Most notably, the Social Connection pillar was the least emphasized among the programs in the reviewed articles. However, the social component is a focal point in occupational therapy education, evident in the emphasis placed on it in ACOTE standards B.1.2., B.3.2., and B.3.3., as well as within the domains of Context and Performance Patterns in the OTPF-4. The same could be about the Restorative Sleep and Avoidance of Risky Substance pillars, as these are related to performance patterns addressed by occupational therapy.
Conclusions
While this review was able to explore the breadth of lifestyle medicine education and discuss possibilities in occupational therapy education, it would be of future interest to explore the depth to which occupational therapy education could implement this piece. A connection forged between lifestyle medicine education and occupational therapy could facilitate exploration of how occupational perspectives of humans and health, grounded in occupational science, support positive lifestyle behavior. The pillars of lifestyle medicine education possess the potential to increase educational resources available to occupational therapy programs, while establishing a reciprocal dynamic where the occupational therapy perspective lends support to lifestyle medicine. This alignment adheres to the ACOTE standards and OTPF-4. The combination of these resources forms an invaluable toolkit, equipping occupational therapy students, along with students in other health professions, to comprehensively address diverse facets of client care and overall well-being.
Footnotes
Acknowledgments
The authors thank Rudy Barreras of the Harriet K. and Philip Pumerantz Library for guidance on search terms and journals and Tina Lekas, an OT colleague, for support in initial idea refinement.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.