
Abstract
Patients with Ulcerative Colitis (UC) seek a variety of methods to manage the physical and psychosocial burdens of illness on daily life. This study examines how individuals with UC: (1) utilize treatment and self-management methods and (2) make decisions regarding their use of these methods throughout the disease course. Adults living with UC ≥5 years and experienced ≥1 disease flare, participated in individual, semi-structured qualitative interviews. Transcripts were thematically analyzed using a constant comparative approach in NVivo12®. Participants (N = 21) described their decisions to utilize medical, lifestyle, and complementary methods, which were shaped by sources of information, attitudes toward self-management, and personal motivations. The poor quality of life associated with the daily burden of living with UC emerged as a primary motive for exploration and utilization of treatment and management methods. Participants reported primarily utilizing treatment and management methods as reactive responses to flares instead of preventive measures. Results provide insight into patient decision-making and may inform individualized patient care, improve patient–provider communication, and guide interdisciplinary efforts to support self-management among patients with UC. Findings highlight a need for greater focus on promoting preventive self-management lifestyle behaviors to protect against disease activity and progressive impairment.
“The poor quality of life associated with the daily burden of living with UC emerged as a primary motive for exploration and utilization of treatment and management methods.”
Introduction
Ulcerative Colitis (UC) is an inflammatory bowel disease (IBD) defined by inflammation and ulcerations of the mucosal lining of the colon with widely variable pathogenesis. Ulcerative Colitis is characterized by unpredictable periods of disease activity, or flares, with prominent localized physical symptoms including rectal bleeding, bowel urgency, bowel frequency, diarrhea, and abdominal pain. Patients also experience a range of extraintestinal symptoms, such as joint pain, and various comorbidities. Medical treatment for UC aims to reduce symptoms and induce remission using pharmaceutical therapies. For many individuals with UC, pharmacotherapy is often reported as insufficient to maintain a “normal” lifestyle. Moreover, the use of multiple concurrent medications, with implications for drug-drug and drug-diet interactions, is common in attempts to control symptoms.1,2
Individuals with UC experience a significant burden of illness. The burden of illness is a cumulative biopsychosocial experience which impacts biological, cognitive, emotional, and social domains in everyday life. 3 In addition to gastrointestinal (GI) symptoms, patients also report considerable physical and cognitive fatigue, isolation, reduced productivity, “brain fog”, distress and embarrassment, diminished self-concept, anxiety, and depression, as well as strained physical, emotional, and social functioning.1,4,5 This burden of illness affects daily functioning and overall quality of life. While GI symptoms typically fluctuate in severity throughout the disease course, the physical and psychosocial burden of illness often continues during periods of remission.
Many patients with UC seek a combination of medical, lifestyle, and/or alternative treatment and management methods to mitigate disease symptoms, reduce pharmaceutical dependence, and respond to daily challenges of living with UC. Seeking out individual preference-based management options for UC treatment has been associated with a high quality of life (QoL) and successful self-management. 6 While existing research indicates the use of various methods to manage UC, current literature is lacking evidence for how patients choose treatment and management methods throughout the disease course.7,8 This study examines how and why individuals with UC make treatment and management decisions, aiming to inform evidence-based programs to promote self-management and improve provision of care for patients with UC throughout the disease course.
Methods
Qualitative data were collected using individual semi-structured interviews to obtain data on perspectives and experiences of individuals with UC regarding treatment and management methods. This study was approved by the University of South Carolina’s Institutional Review Board.
Eligibility and Recruitment
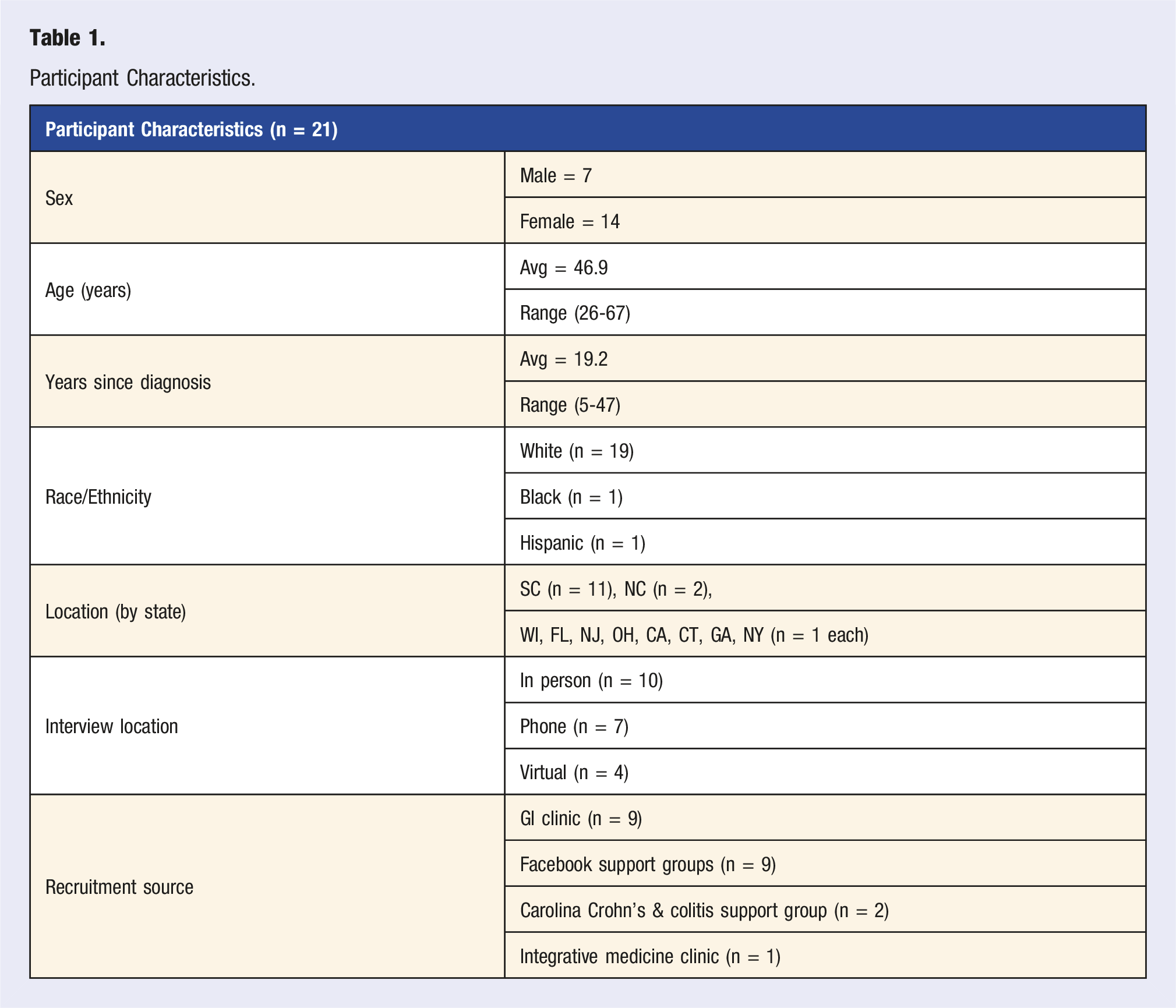
Patients were recruited in collaboration with a large gastroenterology clinic in South Carolina, a support group for individuals experiencing IBD, an integrative medicine clinic in South Carolina, and from UC-focused Facebook support groups. Recruitment used a purposive sampling strategy. Eligibility criteria included: (1) diagnosis of UC; (2) duration of illness ≥5 years; (3) ≥1 disease flare during the illness trajectory; and (4) English speaking.
Data Collection
Interviews were conducted by KD in person, over a secure web-based platform, or over the phone according to participant preference. All participants provided verbal informed consent. Interviews lasted approximately 1 hour and addressed the participant’s self-report of their retrospective illness trajectory, impact of UC on daily life, experiences with medical, complementary, and/or alternative treatment methods, methods for self-managing the impact of UC on daily living, and decision-making regarding treatment and management options. Participants shared their experiences using treatment and self-management methods and described factors contributing to their decisions to use such methods. See Supplemental Table 1 for selected examples of interview guide questions and accompanying probes.
Analysis
Interviews were audio recorded, transcribed verbatim, and reviewed for accuracy. Data were analyzed using QSR International NVivo 12® software.
9
Thematic analysis was conducted using a constant comparative analysis approach to compare context-rich cases and identify cross-case themes.
10
The constant comparative methods is an iterative process of qualitative data analysis that involves moving back and forth from the themes identified to compare to the meaning expressed in the full transcript throughout the data analysis process.
10
This approach allowed for systematic coding of both unique variations within participant experiences and emerging commonalities.
10
The primary coder (KD) led the analysis with input from a secondary coder (CB). Multiple steps that involve application of the constant comparative method were taken to strengthen the integrity of findings: • First, transcriptions were read in whole to capture overall passage context (KD). • An initial codebook was developed from analysis of the first 5 interviews using an emergent inductive approach. • This guided coding of subsequent transcripts, allowing for additional codes to be added as they emerged from the data.10-12 • All interviews were coded to reflect the content and meaning of each passage, identifying themes addressing burden of illness, treatment and management methods, attributions of UC and disease activity, decision-making processes, motivating factors, information sources, and impact of methods on daily life experiences, disease activity, and disease course. • Content and meaning of passages were discussed and clarified in biweekly meetings with KD and CB to ensure accurate data representation in analysis.
11
• Codes were iteratively organized into meaningful themes and sub-themes to capture key elements of participants’ experiences.
12
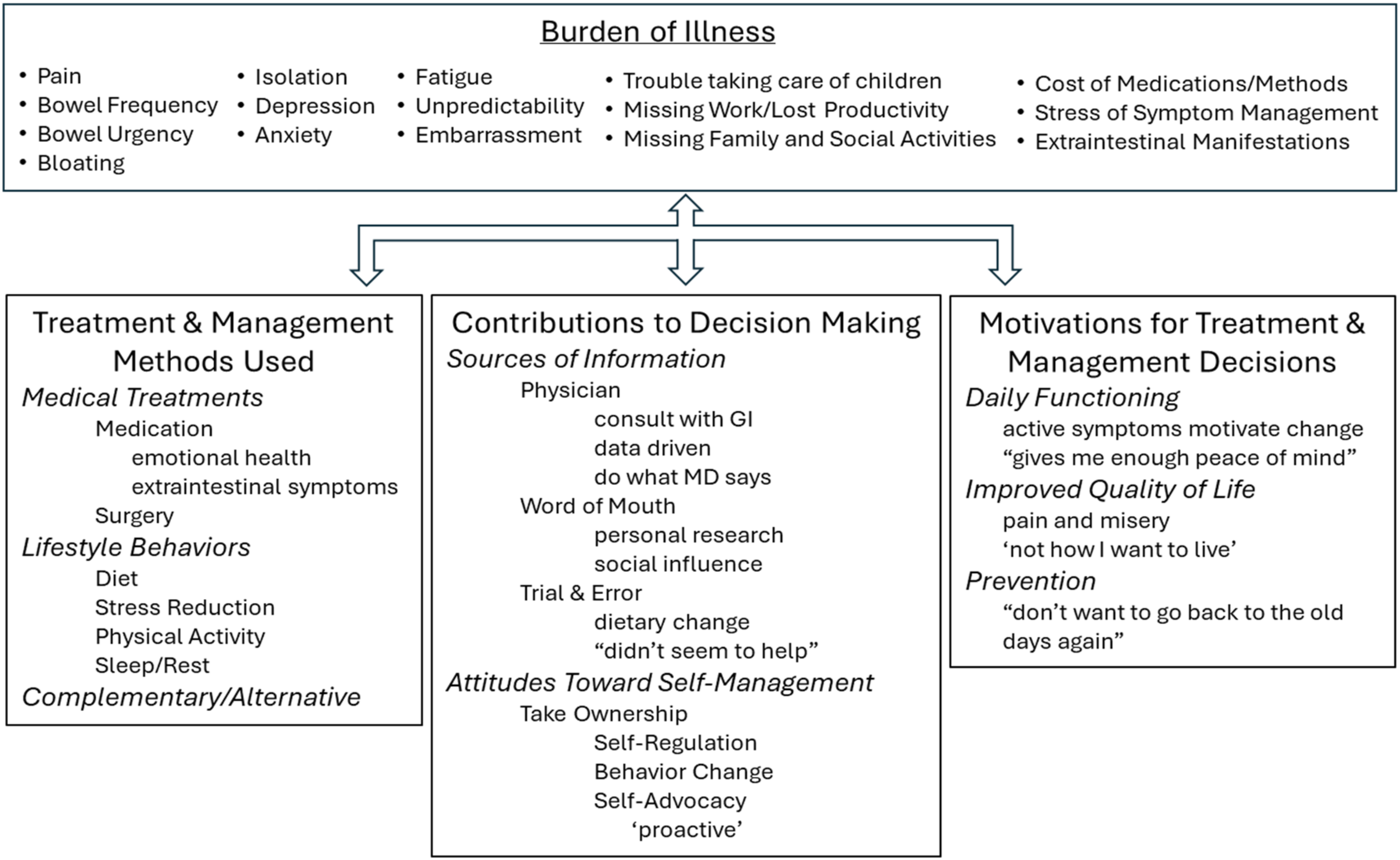
See Figure 1 for predominant themes and selected sub-themes that emerged from the data. • Memos were written to capture additional insights and observations throughout data analysis. Organized themes and selected sub-themes.
Results
Study Participants
Participant Characteristics.
Treatment and Self-Management Methods Used Over the Disease Trajectory
Participants described their disease history and experiences with treatment and management methods throughout their course of illness. Participants employed various methods to avoid GI and extraintestinal symptoms, mitigate disease activity over the course of illness, and ease the daily burden of living with UC. Dose, frequency, duration, and engagement of methods varied across participants. Three categories of predominantly used methods emerged from the data: Medical Treatments, Lifestyle Behaviors, and Complementary/Alternative Treatments.
Medical Treatments
Participants identified medication and surgery as predominant medical methods for treatment and management of UC.
Medication
All participants reported involvement with a gastroenterologist for disease management and were advised to use medication (including aminosalicylates, biologics, immunomodulators, and corticosteroids) as a primary treatment approach to manage disease activity. Many participants used medication as continual maintenance therapy, while a few used medications as a short-term response to GI symptoms. Some used both maintenance medications as well as short-term medications in response to flares. Most participants reported reduced responsiveness to medications over time, and described having to use newer, “stronger” medications as their illness progressed. Use of prescription medication was also reported by some to manage depression, anxiety, pain, and sleep quality.
Surgery
The 3 participants who had bowel surgery to remove diseased portions of their colon all reported expecting that the UC trajectory would be eliminated after surgery, yet they continued to experience significant fatigue, needed self-management of GI symptoms, and faced other complications (e.g., J-pouch twists, blockages). These patients reported experiencing bowel frequency, abdominal pain, stress of ostomy management, and psychosocial challenges post-surgery. One woman who experienced blockages, pain, and extraintestinal manifestations of illness post-surgery explained:
“…it’s not a cure all…you had an auto immune [disease]…you’re never going to be normal” (8)
Lifestyle Behaviors
Participants employed multiple lifestyle behavioral methods to mitigate the daily burden of UC. Manipulating dietary intake, reducing stress, engaging in physical activity, and obtaining sufficient rest each emerged as prominent lifestyle methods most participants utilized for managing UC.
Diet
Most participants reported believing, at some point during their disease trajectory, that diet played a role in managing the burden of UC. Among those participants, a spectrum of approaches and attitudes towards diet were evident. Most described enduring efforts to identify dietary triggers responsible for UC symptoms. A common management strategy among many participants was to skip or delay meals to avoid GI symptoms. One woman tried to avoid any potential public embarrassment by not eating before venturing out of her home, saying:
“If I want to go somewhere, what I have to do is by five o’clock I cut myself off from eatin’ if I want to do something the next day.” (6)
Stress Reduction
Reducing stress was frequently described as essential for self-management of symptoms and prevention of flares. To cope with or reduce stress, many participants changed employment or reduced their daily workloads, including dropping out of school and seeking disability benefits. Additionally, participants limited their professional and social commitments, avoided stressful situations, engaged in exercise, spent time outdoors, found enjoyment in various hobbies, made conscious efforts to reframe thoughts and mindsets, enjoyed the companionship of a pet, and relied on faith and prayer. One participant enjoyed moments of heated relaxation to help her self-manage her UC:
“I have one of those blankets that you plug in…oh, that helps tremendously. I just lock the door, put the seat back, and curl up…heat helps…it relaxes me, and I think the fact that I’m relaxed relieves some of the UC.” (10)
Another woman described her efforts to alleviate stress, particularly when experiencing flares:
“I would not make plans with people at all because I knew every ounce of energy had to be given to doing my work, so I just wouldn’t plan things. It was horrible. …Trying to get rid of things, not adding anything to your plate, saying no to people more, or not taking more things on that you could, just trying to simplify your life as much as possible.” (15)
Physical Activity
Although GI symptoms often limited engagement in physical activity, many participants used exercise as a method to reduce stress, reduce joint pain, increase energy, improve sleep, and improve overall health and well-being. Spending time walking outside was reported by an individual to help improve health, reduce stress, and mentally reframe the burden of UC on daily life. He explained:
“I walk and jog at times. As far as the stress and just on its own, I think it helps. I’ll go for a walk around the block, and I’ll look at the houses… just gets my mind to a different place…putting it in perspective of - I’m in my house having these digestive issues, I have colitis, but yet, outside of my world,…there’s a million other things going on… that have nothing to do with what my perceived huge troubles are.” (13)
Sleep and Rest
Many participants reported sufficient sleep and rest as essential to prevent and recover from flares. Rest was a predominant method for managing daily life with UC as participants not only felt deeply fatigued during flares and periods of remission, but also as a method to reduce stress and inflammation in efforts to mitigate disease activity. One woman shared:
“I need to make sure I sleep. It sounds kind of lame, but I just lay around and try to heal…if you don’t get rest, it gets worse.” (16)
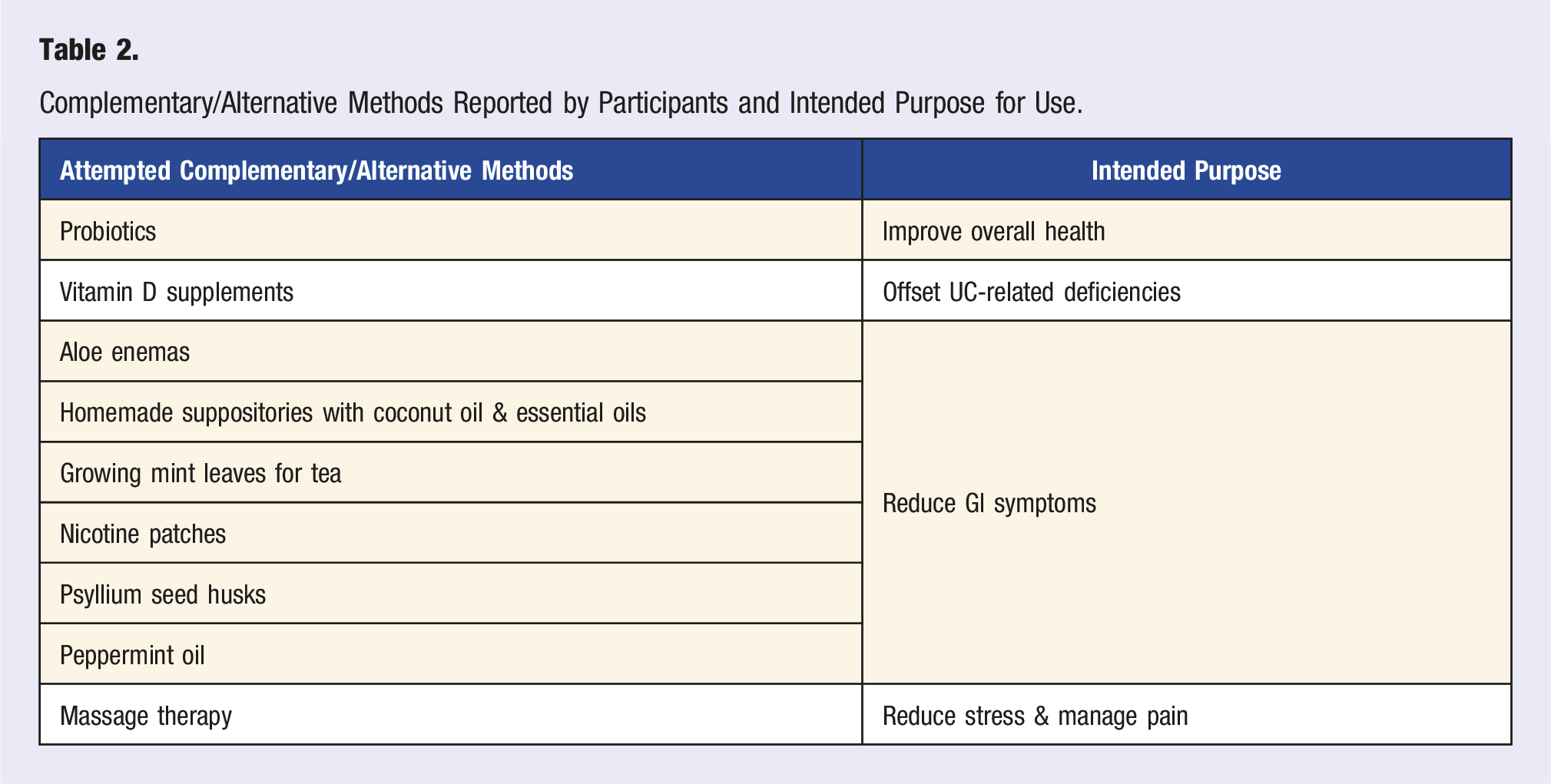
Complementary/Alternative Treatments
Complementary/Alternative Methods Reported by Participants and Intended Purpose for Use.
Contributions to Decision-Making
Participants described making decisions about how and when to use treatment and management methods. Decisions were influenced by 3 main categories of contributing factors: sources of information, attitudes toward self-management, and personal motivations.
Sources of Information
Physician
Most participants described following physician recommendations for UC treatment, trusting that their provider was more knowledgeable on best practices. A few of those participants described shared decision-making based on physician’s analysis of blood and stool test data, others trusted physician recommendations “because they haven’t steered me wrong” (14), and many followed physician guidance blindly. For example, a woman described her treatment regimen by saying:
“I don’t even know if that does anything, really, but my doctor said to take it.” (16)
At the same time, many participants described searching the Internet as more accessible than seeking information from physicians, particularly for information on diet and medication side-effects.
Word of Mouth
While nearly all participants reported not personally knowing anyone with UC, most gained information and recommendations from their extended social circle or social media. One participant explained:
“I utilize the Facebook pages a lot because it’s other people that actually have what I have…I know that even though doctors are there with all this information, they’re not experiencing it themselves. So, people that actually have what I have, I feel like they’re the best sources of information because they have personal experience.” (18)
Patients reported that information shared through word of mouth often inspired a willingness to try new things, generated confusion from mixed messages, or ignited fear and aversion towards treatment methods, specifically surgery and certain medications.
Trial and Error
Most participants described extensive trial and error with treatment and management methods. As many insurance companies require a progressive treatment approach to approved UC medications, participants commonly experienced a pre-determined, trial and error approach with their physician to identify medication that could induce and maintain remission. Before resorting to certain medications or UC surgery, some participants preferred taking time to first try all other options for disease management. One woman felt overwhelmed by the impact a multi-step J-pouch surgery would have on her life and explained:
“I decided at that point I just needed to take some time off and just try every possible approach that I could before I do surgery. (9)
Trial and error predominantly shaped participants’ perspectives on diet as a self-management method. Some participants reported trying diet manipulation as a treatment method for varying periods of time, observed little to no perceived success, and consequently disregarded diet as a treatment and management method. One woman, for example, felt that the efforts she made to change her diet were ineffective, and explained:
“I tried fixing my diet of going gluten free…that didn’t do anything…I started doing dairy free. That didn’t do anything. So for me, diet hasn’t made me any better.” (18)
In contrast, others perceived dietary changes to alter their experience with UC, and therefore adopted new dietary behaviors long term. Many participants made associations between specific foods and disease activity based on immediately observed GI symptoms. For example, a woman described how she identified packaged lunch meat as a food that “triggered” UC symptoms using trial and error observations:
“As long as I buy deli meat, like, fresh sliced deli meat, it doesn’t bother me, but if I buy packaged, like off the shelf, yeah, it kicks my tail…packaged meat and I’m like ‘whew’, you know? Two or three times I’ll go to the bathroom after that. And for the longest time I couldn’t figure out what it was… I had a sandwich, why’d it bother me today? It’s a sandwich. But then I got putting two and two together that it was deli meat and that was, so, I don’t know.” (4)
Another man described his observations over time as he sought to identify patterns between diet intake and UC symptoms:
“You learn food that sort of will trigger things. The pepperoni pizza…four hours later I’ll be spending some time in the bathroom. You know, I mean, you avoid certain things. I won’t eat very spicy foods, they will just go through me. And there’s other times I can have chicken soup and I’ll be in the bathroom three or four times after that. So, it’s hard, you know, inflammatory bowel disease is a strange auto-immune type of disorder.” (21)
Attitude Toward Self-Management
Very rarely did participants attribute disease onset and the unpredictable nature of the disease course to personal health behaviors. However, some participants believed their individual choices and behaviors could modify the disease course and mitigate the burden of living with UC. These individuals aimed to feel in control of their illness and made efforts, in varying degrees, to take charge of how they experienced life with UC. In these cases, some patients self-regulated treatment, changed lifestyle behaviors, and proactively self-advocated for quality care and support.
Self-Regulation
Some participants described making their own decisions regarding how and when to use treatment and management methods. Of these participants, some felt free to self-assess and make minor adjustments to medication dosing. For example, one man described adjusting his daily maintenance medication dose based on symptom activity, saying: “I actually take one in the morning unless I have some sort of flaring going on, in which case I'll take three.” (19)
Behavior Change
Many described making changes in their own daily health behaviors in attempts to mitigate disease activity before seeking medical treatment. In response to a flare, many participants described trying to reduce stress, adjust dietary intake, and/or rest. One woman shared: “Despite the fact that I despise Prednisone with every fiber of my being, it does work. I only take it when I’ve done everything else on my own. I go through the process on my own first. I know when I need to ask for help.” (14)
Self-Advocacy
Some participants sought greater satisfaction with treatment options and patient–provider communication. These participants emphasized the value of being their own advocate and effectively communicating needs to their physician in order to “get the best treatment that you can” (17). One young woman described:
“…you really have to advocate for yourself…It’s like a job that, you have to pay attention” (16)
Some patients learned over time to be proactive in their medical treatment. Staying informed, advocating for treatment changes, and keeping current with disease management was described as important for self-management. One man shared:
“…when I would go to the doctor early on, it was just like okay, a last resort type thing. I’m not getting any better, I need to schedule an appointment…over the years I’ve learned…I need to stay ahead of my appointments, stay up with my lab work, get ahead of everything.” (17)
A handful of participants reported making significant efforts to research the disease and available treatment options to educate themselves and become an active participant in decision-making. A few participants also reported taking personal action to seek out support groups or professional therapy to help manage the emotional burden associated with UC.
Motivations for Treatment & Management Decisions
Overall, participants’ motivation to utilize treatment and management methods centered on both daily functioning and obtaining an improved quality of life. Participants described desires to keep up with the demands of daily life, raise a family, be productive, and have peace of mind. Most participants aimed to reduce GI symptoms and physical pain, overcome and recover from fatigue, avoid embarrassment, and cope with both physical and emotional isolation, as well as the fear and distress of an unpredictable illness. While the burden of living with UC motivated decision-making and usage of treatment and management methods, a preventive approach towards disease management was lacking among most participants.
Daily Functioning
Daily functioning was frequently prioritized in decision-making, particularly in regard to pharmaceutical treatment methods. Despite potential side-effects, long-term repercussions, and desires for more “natural” treatment methods, many participants often resigned to “keep doing what I’m doing for now” (8) and maintain treatment options that seemed to be keeping disease activity at bay. One woman explained her willingness to receive treatment despite her fears of the future by saying:
“I’m scared that the infusions one day are going to cause another problem, which is really scary, cause it’s like a really serious strong drug that I’m taking…but I’m okay with it cause it helps me right now.” (5)
Another woman echoed:
“They say a lot of [specific medication] can cause liver cancer…I can’t worry about that later on. I have to be able to function today.” (3)
Improved Quality of Life
The predominant motivator for change was the diminished quality of life associated with UC. Participants emphasized a desire to reduce the physical and psychosocial burden of living with a chronic illness. Multiple participants described feeling “miserable” and “desperate” to change their quality of life, stating: “this is not how I want to live” (3), “I can’t do this…anymore” (5), “I couldn’t even hardly function” (4), “I did not want it to control my life” (7), and “I don’t want to go back to the old days again” (2). A woman who reported significant physical and emotional UC-related distress described her determination to take action towards improving her quality of life, sharing:
“I just wanna, you know, keep going. Being mobile. Because people sit around in pain…there’s stuff out there. If there’s stuff out there, get it. If you need it, get on it. Just make your life better. Why suffer?” (3)
Feelings of being “miserable” motivated a willingness to adopt new or additional treatment methods. For example, a woman described the effect a recent flare had on her role as a mother, sharing:
“I was having trouble…taking care of my kids because I just, I was that miserable, and I was like, I’m sorry, I have to just lay down like all day and they don’t understand. And they’re looking at me like, why are you not playing with me? You know, take ‘em to the park. And I’m like, I can’t be away from a bathroom for more than five minutes.” (8)
She continued to describe how her misery motivated her willingness to try alternative methods, such as peppermint capsules, saying:
“I think I was just desperate and then I just started burping up like peppermint and I was like, eh, I’ve got good breath. But, eh, it’s not, it’s not, you know, helping. Um, but that’s how miserable I was.” (8)
Another young woman felt hesitant to begin taking a Biologic therapy but wanted relief from the impact of UC on her daily life. Having to weigh her decisions, she explained:
“So, I can either not function, or lose my colon…, or I can just bite the bullet and get this done.” (15)
Some participants avoided physician treatment until symptoms were too much to bear. One participant shared:
“I thought maybe it [flare] would just go away by itself. It would kind of ease off and it would get worse, and finally…I said, you guys got to do something. I’m going to die, this thing is killing me. And so they [physician’s office] gave me a month’s worth of Prednisone.” (20)
The desire for improved quality of life motivated a few participants to make significant lifestyle changes. One man reported making successful long-term changes to his dietary patterns, in addition to continuing maintenance medication, to avoid living with active disease symptoms. Another young man explained how his initial experience with UC motivated him to increase his physical activity to live a healthy life:
“I used to like just sit around all day. Now I bike, I run, I walk everywhere. …Probably like a month after I started getting symptoms,…like I was having symptoms and I was trying to be active…I wanted to be healthier in general. Just, I knew I had to change.” (11)
Prevention
Outside of maintenance medications, efforts to reduce stress, and avoiding perceived “trigger” foods, participants rarely described the use of treatment and management methods as preventive measures against disease activity and disease progression. Preventive self-management was often perceived as challenging to maintain, given the common belief that:
“…preventing a flare would be to continue [living as if] you are in a flare even when you’re not, and I’m not good at that.” (15)
Discussion
Promotion of healthy lifestyle behaviors among the UC population is needed, as UC is increasingly recognized to be a progressive illness with a growing need for preventive action to protect against additional damage and impairment. 13 While participants in this study aimed to avoid UC symptoms and maintain remission by taking medications, reducing stress, and avoiding perceived “trigger” foods, individuals primarily described utilizing treatment and management methods as responses to flares instead of as preventive measures against disease activity and disease progression. In fact, the behaviors many patients viewed as needed to prevent flares, such as highly restrictive diets, isolation from stress, and significant rest, were described as difficult to maintain.
The poor quality of life associated with the daily burden of living with UC emerged as a primary motive for exploration and utilization of treatment and management methods. Findings from this study suggest patients are willing, especially during times of active disease, to try new methods of management and overlook long-term implications to reduce pain and suffering and be able to “function” in the present day. Similar findings are reported by Kamp and Brittain (2018), who found that increased IBD related symptoms was a primary factor in treatment related decisions. Participants expressed efforts to adjust lifestyle behaviors and try new treatment methods in reaction to the poor physical and psychosocial QoL they experienced. For a few patients in this study, the burden of living with UC motivated long-term health behavior change. These findings are consistent with multiple behavior change theories, particularly Rosenstock’s Health Belief Model (HBM), which recognize that individuals who desire change first feel substantially threatened by some perceived or actual environmental experience. 14
Participants rarely expressed feeling a personal responsibility for the unpredictable course of illness, but some believe that they can, to varying degrees, take charge of their experience with UC. Understanding the behaviors and perspectives of these particular patients may provide healthcare professionals additional insight needed to improve individualized care and guide patients with UC towards a higher quality of life. Patients in this study often described adapting to and self-managing UC predominantly on their own through trial and error and research. At the same time, collaborative care between patients and providers helps patients feel a sense of control over their illness, which improves self-management overall. 15
As dietary manipulation is a primary self-management method, research is needed to understand associations between dietary intake, inflammation, and biopsychosocial health among patients with UC. Individuals with UC have reported diet manipulation as a strategy for managing GI symptoms for some time, 16 yet research examining diet as a behavioral treatment and management method for mitigating disease activity is relatively new.17-19 This study found that participants evaluate diet’s impact on disease activity primarily on immediately observed GI symptoms while dietary change as a management method often evolves over time through extensive trial and error. Similar findings report that while a large majority of patients believe dietary change to be important for their disease management, the main source of disease-related nutritional knowledge was based on personal experiences with GI symptoms.7,20 Viewing diet’s influence on disease activity solely based on observed GI symptoms leads to misguided conclusions and negates the key role of diet in regulating inflammation. Research suggests that a focus on removing “pro-inflammatory” foods, such as refined carbohydrates and processed foods, and increasing intake of “anti-inflammatory” foods should guide dietary choices among patients with UC. 21 , 22 Additionally, research identifies the important role of diet in regulating the immune system overall. 23 Studies have found that diet can either increase or reduce systemic and localized inflammation, suggesting that diet likely plays an important role in the treatment and management of inflammation associated with UC.24-26 Additional work is needed to understand how patients make decisions about diet and understand links between diet and GI symptoms, in order to develop effective interventions to promote adoption of healthy diet patterns among UC patients.
Findings from this study are limited to patient perspectives, as we did not objectively measure effectiveness of method use and do not assess the biopsychosocial effectiveness on reducing the burden of UC. Participants who were willing to share their experiences with UC were recruited as volunteers, which may introduce bias and reduce sample variability. Although this study included recruitment through social media and integrative health care clinics, all participants reported treatment under physician care, which may have limited collection of data on use of alternative therapies. Representation of individuals minoritized by race and/or ethnicity is a prominent limitation of health-related research, including this study. 27 This study’s sample consisted primarily of White participants, which limits generalizability to other groups.
This qualitative study provides an in-depth understanding of the perspectives and experiences of patients with UC. Findings expand upon the lived experiences of patients with UC to examine how and why patients make decisions on the use of treatment and self-management methods over the disease course. An additional strength of this study is the inclusion of participants from ten different states across the US, as the participant sample provided perspectives and experiences from patients who receive care at varying health facilities.
In partnership with physician care, additional resources are needed to support and empower patients with UC to self-manage disease activity and increase understanding on how behavioral management methods influence the disease course.28,29 Patient-reported experiences highlight the need for expanded patient care models and evidence-based health promotion programs to reduce disease symptoms, maintain remission, and improve psychosocial well-being. Recent research calls for an expanded view of self-management in IBD research; to expand beyond symptom management and explore methods for improving emotional, social, and psychological well-being among individuals with IBD.28,29 Our findings support current literature, as studies have found that patients desire holistic, multidisciplinary care from physician and health care settings to address disease activity and quality of life domains yet rely on self-identified strategies to manage the physical and psychosocial burden of UC.8,30,31
This study offers added insight into how and why patients with UC use treatment and management methods to manage the physical and psychosocial burden of illness on daily life and supports the importance of disease prevention and management both inside and outside of the clinical setting. The present study’s findings can aid in framing patient education and evidence-based behavioral interventions that assist patients in adopting and sustaining self-management behaviors. Additional research is needed to design and evaluate methods to shift treatment and management approaches from being reactive to preventive.
Supplemental Material
Supplemental Material - Use of Treatment and Self-Management Methods: Perspectives and Decisions of Patients With Ulcerative Colitis
Supplemental Material for Use of Treatment and Self-Management Methods: Perspectives and Decisions of Patients With Ulcerative Colitis by Kelli E. DuBois, Christine E. Blake, Caroline Rudisill, Sayward E. Harrison, and James R. Hébert in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
We greatly appreciate and acknowledge Dr Anjani Jammula and office staff at Prisma Health Gastroenterology and Liver Center, Greenville SC, for their support with patient recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by a SPARC Graduate Research Grant from the Office of the Vice President for Research at the University of South Carolina. Dr Hébert was supported by the National Institute of Health [grant U01 CA272977-01].
Data Availability Statement
The qualitative data that support the findings of this study are not publicly available in order to protect study participant privacy.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.