
Abstract
Background
Therapeutic lifestyle change can be challenging, and not every attempt is successful.
Purpose
To identify predictors of making progress toward lifestyle change among patients who participate in a lifestyle medicine program.
Methods
This was a single-center, retrospective cohort study of 205 adults who enrolled in a goal-directed, individualized, interprofessional lifestyle medicine program. The primary outcome was whether, by the end of participation with the program, a patient reported making progress toward lifestyle change. Candidate predictors included sociodemographic, psychological, and health-related variables.
Results
Among 205 patients (median (IQR) age 58 (44-66) years, 164 (80%) female), 93 (45%) made progress toward lifestyle change during program participation. A predictor of making progress was being motivated by stress reduction (OR 2.8 [95% CI 1.1-7.6], P = .038). Predictors of not making progress included having a primary goal of losing weight (OR .3 [.2-.8], P = .012) and having a history of depression (OR .4 [.2-.7], P = .041).
Conclusions
To maximize a patient’s likelihood of successfully making lifestyle changes, clinicians and patients may consider focusing on identifying goals that are immediately and palpably affected by lifestyle change. Additional research is warranted to identify effective program-level approaches to maximize the likelihood of success for patients with a history of depression.
“Nearly half (45%) of patients who enrolled in an interprofessional lifestyle medicine program made progress toward lifestyle change during their participation in the program.”
Introduction
Lifestyle medicine is the evidence-based field of medicine which uses “therapeutic lifestyle intervention as a primary modality to treat chronic conditions” such as obesity, heart disease, diabetes, anxiety, depression, and musculoskeletal pain.1,2 The six pillars of lifestyle medicine are a whole-food plant-predominant diet, physical activity, avoidance of risky substance use, restorative sleep, stress management, and positive social connections. 3 Implementation of these six pillars is associated with measurable improvement in numerous clinical outcomes and, at a therapeutic dose, can reverse morbidity and lead to disease remission for some chronic conditions.4-15
Nevertheless, changing lifestyle habits is challenging, and not every attempt results in successful lifestyle change.16-21 Behavioral factors that impact clinical success have been identified in programs that predominantly focus on unidimensional metrics such as weight loss or exercise, but the power of lifestyle medicine is maximized by addressing health holistically across all six pillars.22-25 If we can identify factors that impact whether patients are likely to successfully make progress with lifestyle change (and subsequently enjoy improved health and function) when they engage with an interprofessional lifestyle medicine program, we can work to address modifiable factors via clinical, research, and healthy policy initiatives.
The goal of this study was to identify predictors of making progress toward lifestyle change among patients who participate in an interprofessional lifestyle medicine program. We hypothesized that: (1) increased self-reported self-efficacy and readiness for change, and (2) less social deprivation would be associated with a greater likelihood of making progress toward lifestyle change.
Methods
This was a single-center retrospective cohort study that involved analysis of systematically and prospectively collected data from patient encounters at a US academic medical center between November 6, 2018 and February 14, 2023. Data analysis was performed in 2023. All research activities were performed in accordance with the ethical standards of the Washington University Human Research Protection Office and with the 1964 Helsinki declaration and its later amendments, and the study was approved via a waiver of informed consent under IRB number 202203103. This study reports on a subgroup of patients who were previously described in an analysis regarding predictors of engagement with an interprofessional lifestyle medicine program. 26 Reporting is in accordance with STROBE guidelines. 27
Interprofessional Lifestyle Medicine Program
The interprofessional lifestyle medicine program has previously been described.16,26 Notably, it follows evidence-based lifestyle change principles and uses shared decision making to identify a patient-centered, measurable goal that guides development of a personalized program for each patient. 25 The program is housed in an orthopedic department, and as such, many patients have a goal related to reducing musculoskeletal pain and/or dysfunction (e.g., increasing walking tolerance to enjoy a walk in the park with friends, increasing lifting tolerance to care for grandchildren, reducing weight and/or HgbA1c to reduce perioperative risk and meet pre-operative criteria to qualify for elective joint replacement). Nevertheless, patients can have other goals (e.g., to improve function after developing Long COVID), and all patients who enroll in the program have lifestyle-related habits and comorbidities which can be addressed using lifestyle medicine. Although patients can refer themselves to the program, over 90% of patients have been referred from an orthopedic surgeon, non-operative musculoskeletal specialist, primary care clinician, or clinician who specializes in Long COVID care. At initial consultation, patients complete several self-reported health-related measures and are evaluated by a physical medicine and rehabilitation physician (physiatrist) or board-certified lifestyle medicine PA (physician assistant). Patients who enroll in the program participate in a person-specific combination of goal-setting and behavioral health counseling, nutrition counseling, smoking cessation counseling, sleep hygiene counseling, physical activity counseling, mindfulness and stress reduction counseling, physical therapy, medical management, and acupuncture and medical massage therapy (to facilitate behavior change by addressing pain). The program offers individual appointments and has offered group visits via lifestyle medicine shared medical appointments (SMAs) since January 2022.28-30
Patients
The study cohort included adult patients who presented for consultation and initiated participation in the interprofessional lifestyle medicine program. Patients were excluded if they: (1) chose not to enroll in the program after the initial consultation, (2) were less than 18 years old, or (3) were still enrolled in the program at the time of data analysis. Eligible patients were identified from the program’s clinical data repository.
Measures
The primary study outcome was whether, by the end of participation with the interprofessional lifestyle medicine program (i.e., by completion of the program or by choosing to discontinue the program prematurely), a patient was making progress toward lifestyle change. Patients were defined as “making progress” if they reported that they either: (1) achieved their pre-specified functional goal as a result of lifestyle change, (2) demonstrated progress toward their goal and were maintaining lifestyle changes to facilitate continued independent progress (e.g., maintaining a plant-predominant eating pattern as part of a weight loss goal), or (3) had developed the skills needed for independent lifestyle self-management (e.g., reported independence with stress management, healthy food choices, etc.). Patients were defined as “not making progress” if they: (1) elected to discontinue program services prior to meeting the above criteria, or (2) continued participation in the program for at least six months but were not making demonstrable progress toward their goal.
Descriptive baseline characteristics were collected at patients’ initial consultation. Sociodemographic variables included self-reported age, sex, race, ethnicity, type of insurance coverage, and social deprivation (operationalized as patients’ national Area Deprivation Index (ADI) percentile).31,32 Psychological profile characteristics included participants’ self-reported primary goal of participation in the lifestyle medicine program, resiliency (measured by the Brief Resilience Scale), 33 self-efficacy (measured using the Adult Patient-Reported Outcomes Measurement Information System (PROMIS) Computer Adaptive Test (CAT)), 34 transtheoretical stage of change, 35 perceived importance of change, 36 readiness to change,36,37 confidence in ability to change, 36 motivators for change, 38 and barriers to change. 38 Medical history variables included patients’ body mass index (BMI), waist-to-height ratio (measured by the clinical team), and history of hypertension, hyperlipidemia, cardiovascular/heart disease, obstructive sleep apnea, lung disease, diabetes, anxiety, depression, and/or chronic pain (documented in the medical record). Self-reported assessments of physical function, pain interference, anxiety, and depression symptoms were also collected using Adult PROMIS CAT measures. 34 Lifestyle-related variables included self-reported nicotine use, average nightly sleep duration, nutrition habits (i.e., frequency of processed food consumption, daily quantity of fruit/vegetable consumption), average weekly minutes of moderate/strenuous exercise, frequency of sense of purpose/meaning, and frequency of feeling connected with a support network.38,39
Statistical Analysis
Descriptive statistics were calculated for each baseline variable for the entire cohort and for the subgroups of patients who made vs did not make progress toward lifestyle change. Next, select baseline variables were tested as candidate predictors of making progress toward lifestyle change. Candidate predictors largely focused on sociodemographic and psychological profile characteristics, and they were selected based on the a priori hypotheses, known predictors of engagement with the lifestyle medicine program, 26 and the distributions of the baseline variables among the patient subgroups. The candidate predictors that were considered included patients’ age; sex; race; type of insurance coverage; ADI; primary goal of participation; PROMIS Self-Efficacy; transtheoretical stage of change; importance, readiness, and confidence in ability to change; number of motivators to change; the most frequently reported motivators (i.e., increased energy, decreased stress, weight loss, and body image); body mass index; history of anxiety and depression; and current anxiety and depression symptoms reported using PROMIS.
Univariable logistic regression was used to test the null hypothesis that each candidate predictor is associated with the probability of the patient making vs not making progress toward lifestyle change, and univariable (unadjusted) odds ratios (ORs) with 95% confidence intervals (CIs) are reported (Appendix 1). Odds ratios for unordered categorical predictors are expressed compared to the referent category. Odds ratios for ordered predictors are expressed for a one-unit increase in the predictor, except where noted. Due to skewed distributions and/or poor model fit, some inherently continuous variables were categorized for analyses. ADI national percentiles were a priori categorized into quartiles. All univariable candidate predictors with P < .1 were included in a multivariable logistic regression model using forward selection, and predictors in the multivariable model with P < .05 were considered statistically significant. Adjusted odds ratios with 95% CIs are reported for each variable included in the final multivariable model, adjusted for all variables in the model. Diagnostics of collinearity was performed using linear regression, and lack of collinearity was verified by a variance inflation factor of two or less. 40 There were no issues with collinearity. Patients who had missing data for candidate predictors in the multivariable logistic regression model were excluded from the final analysis. Of note, confidence in ability to change met criteria to be included in the multivariable model, but 26% of patients were missing this data point because it was not systematically collected when the clinical data repository was first launched. We initially ran the multivariable logistic regression model with all candidate variables (n = 136), and confidence to change was not selected in the model. We therefore excluded the variable and re-ran the forward selection multivariable logistic regression model with the full available sample size. All eligible patients available at the time of analysis were included in the sample. Analyses were performed with SAS software v9.4 (SAS Institute Inc., Cary, NC, USA).
Results
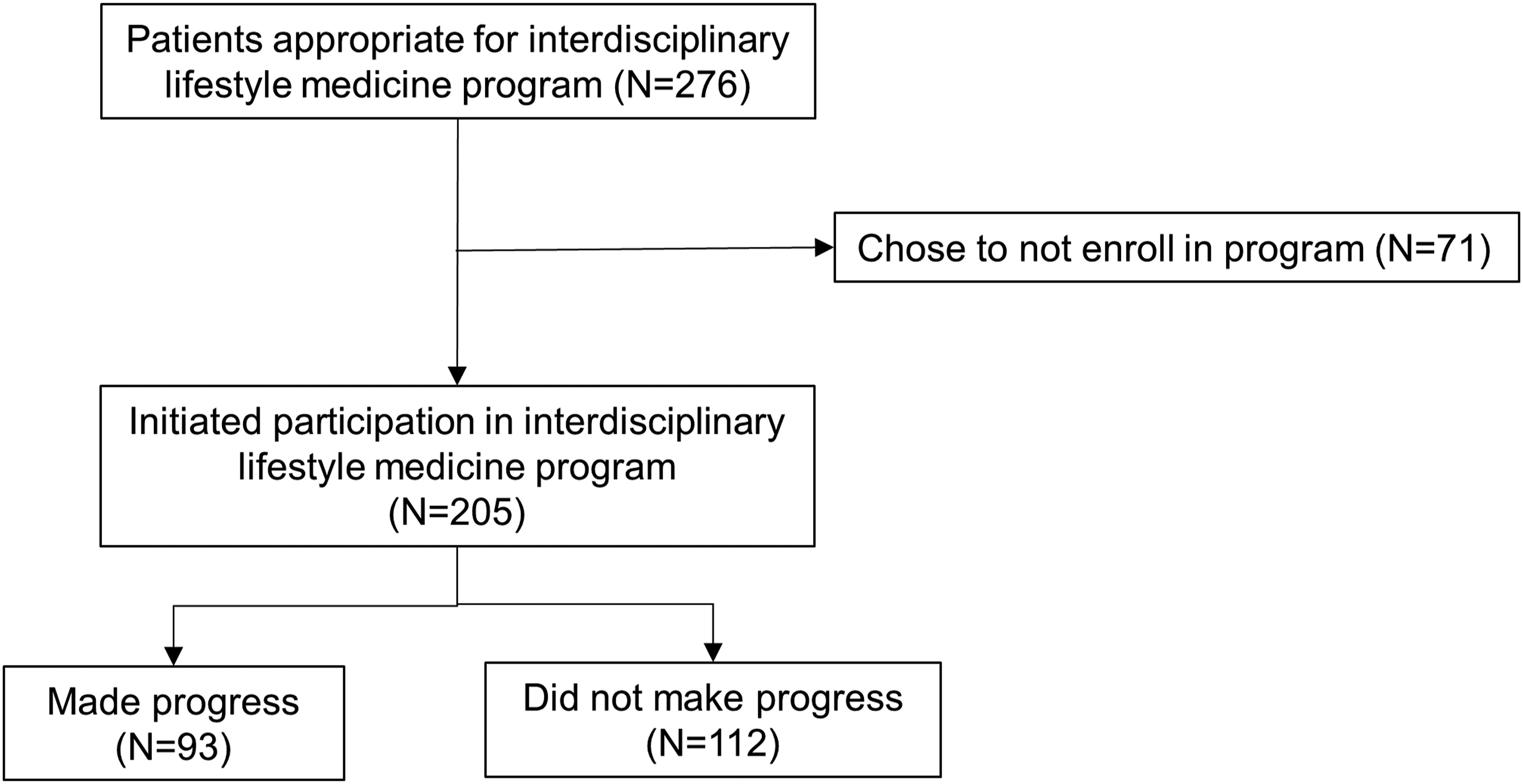
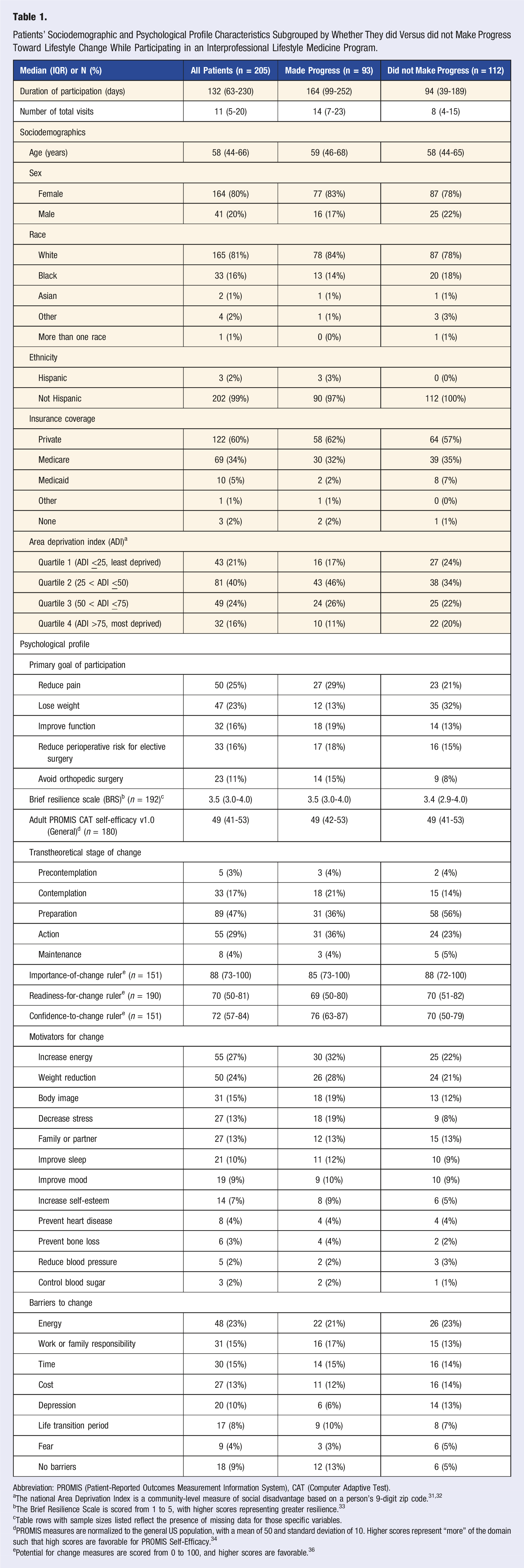
Of 276 patients who presented for consultation and were assessed to be appropriate for the lifestyle medicine program, 205 initiated participation in the program and were eligible for analysis (Figure 1). This cohort had a median (IQR) age 58 (44-66) years, 164 (80%) were female, and 93 (45%) made progress toward lifestyle change during participation in the program, whereas 112 (55%) did not (Table 1). Inclusion flowsheet. Patients’ Sociodemographic and Psychological Profile Characteristics Subgrouped by Whether They did Versus did not Make Progress Toward Lifestyle Change While Participating in an Interprofessional Lifestyle Medicine Program. Abbreviation: PROMIS (Patient-Reported Outcomes Measurement Information System), CAT (Computer Adaptive Test). aThe national Area Deprivation Index is a community-level measure of social disadvantage based on a person’s 9-digit zip code.31,32 bThe Brief Resilience Scale is scored from 1 to 5, with higher scores representing greater resilience.
33
cTable rows with sample sizes listed reflect the presence of missing data for those specific variables. dPROMIS measures are normalized to the general US population, with a mean of 50 and standard deviation of 10. Higher scores represent “more” of the domain such that high scores are favorable for PROMIS Self-Efficacy.
34
ePotential for change measures are scored from 0 to 100, and higher scores are favorable.
36
Patients’ Medical, Self-Reported Health, and Lifestyle Characteristics Subgrouped by Whether They did Versus did not Make Progress Toward Lifestyle Change While Participating in an Interprofessional Lifestyle Medicine Program.
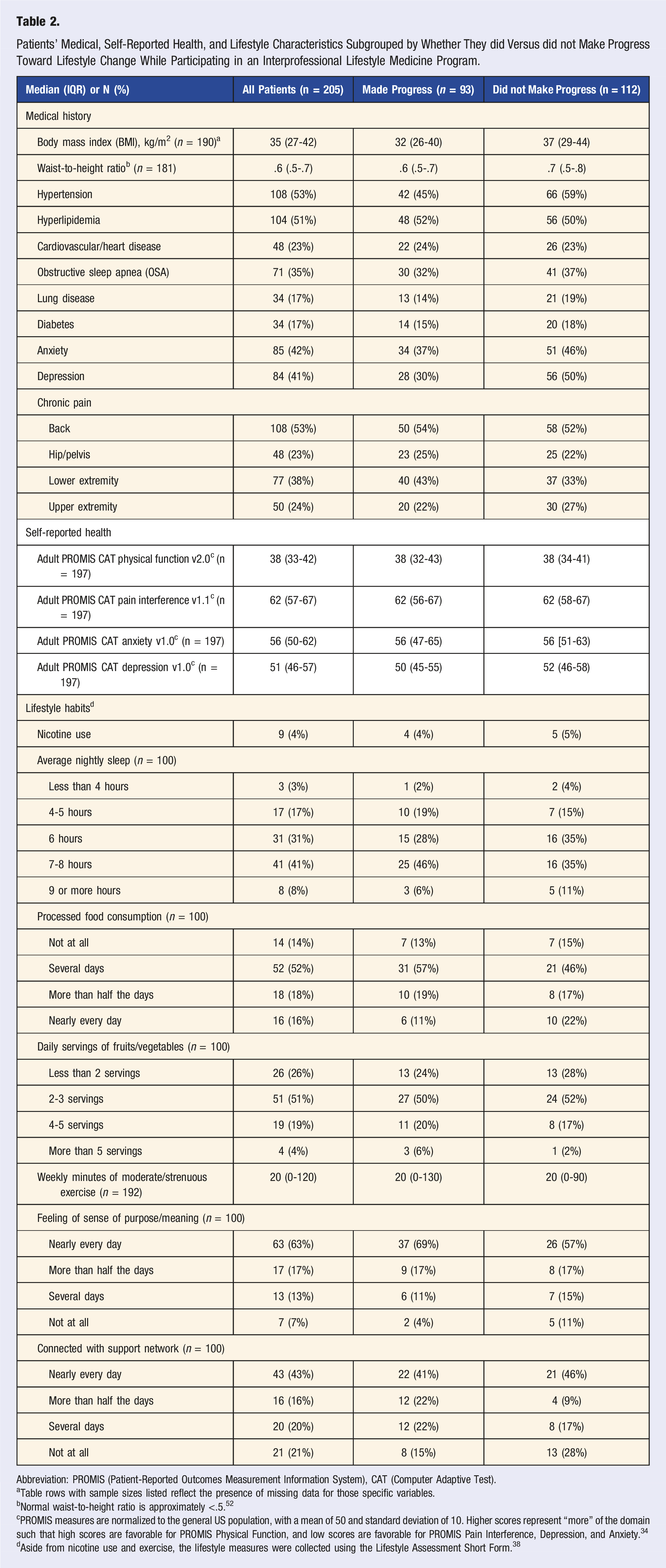
Abbreviation: PROMIS (Patient-Reported Outcomes Measurement Information System), CAT (Computer Adaptive Test).
aTable rows with sample sizes listed reflect the presence of missing data for those specific variables.
bNormal waist-to-height ratio is approximately <.5. 52
cPROMIS measures are normalized to the general US population, with a mean of 50 and standard deviation of 10. Higher scores represent “more” of the domain such that high scores are favorable for PROMIS Physical Function, and low scores are favorable for PROMIS Pain Interference, Depression, and Anxiety. 34
dAside from nicotine use and exercise, the lifestyle measures were collected using the Lifestyle Assessment Short Form. 38
In the final multivariable model which adjusted for associations between baseline variables, a predictor of making progress toward lifestyle change was being motivated by stress reduction (OR 2.8 [95% CI 1.1 to 7.6], P = .038), and predictors of not making progress toward lifestyle change included having a primary goal of losing weight (OR .3 [.2 to .8], P = .012) and having a history of depression (OR .4 [.2 to .7], P = .041) (Figure 2). Candidate predictors of making progress (versus not making progress) toward lifestyle change (N = 187). Adjusted odds ratios from the multivariable models are depicted, and error bars represent 95% confidence intervals.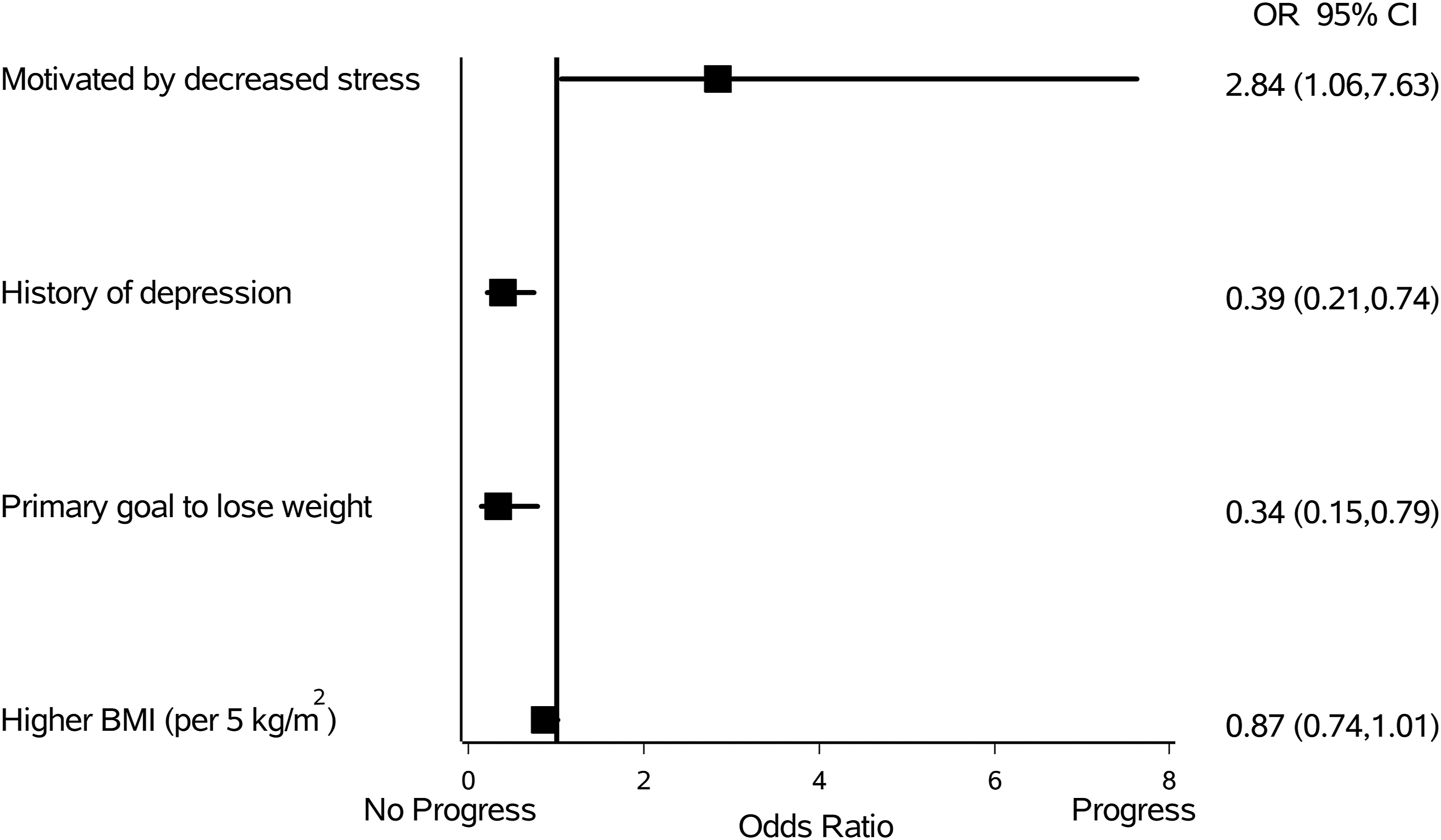
Discussion
In this retrospective cohort study, nearly half (45%) of patients who enrolled in an interprofessional lifestyle medicine program made progress toward lifestyle change during their participation in the program. Psychological and medical factors that were associated with making progress included patients’ primary goal of participation, number of motivators to make lifestyle change, the specific motivator of decreasing stress, confidence in ability to change, body mass index, and history of depression. When considering all these variables together, being motivated by stress reduction was independently associated with making progress toward lifestyle change, and having a primary goal to lose weight or having a history of depression were independently associated with not making progress toward lifestyle change during participation in the interprofessional lifestyle medicine program.
The predictors we identified are partially consistent with relevant factors that have been identified in previous qualitative syntheses and lifestyle-related programs for other patient populations (e.g., weight loss and exercise focused programs). Specifically, identifying meaningful goals, having autonomous motivation, having symptoms related to depression (e.g., pessimism, feelings of helplessness), high baseline weight, and having a focus on weight loss have all been found to be important predictors of whether a person will make sustainable lifestyle changes.23-25,41 However, contrary to our hypotheses and previous research, patients’ self-reported self-efficacy and readiness to change were not associated with their clinical trajectories during participation in the interprofessional lifestyle medicine program.22,24 Furthermore, although some sociodemographic characteristics are associated with whether patients will enroll with such a lifestyle medicine program, 26 in this study, age, race, and insurance coverage were not associated with patients’ likelihood of making progress toward lifestyle change among patients who did choose to enroll.
Implications
To maximize patients’ likelihood of making lifestyle changes, this study suggests that facilitating patients in identifying stress reduction as a relevant motivator for change may be uniquely beneficial. It is well established that motivation is a key factor for successful behavior change, 42 and it is also known that autonomous, intrinsic motivation (e.g., to impact one’s own life) is a more effective contributor to successful behavior change than purely extrinsic motivation (e.g., to appease a family member or to qualify for a health-related workplace incentive).43-45 However, to our knowledge, the specific intrinsic motivator of stress reduction has not been widely investigated even though it is applicable to a substantial proportion of the population. 46 If clinicians can help patients make the connection that: (1) stress management is a pillar of lifestyle medicine, and (2) lifestyle change can lead to stress reduction, it may increase patients’ intrinsic motivation, and therefore likelihood of success, related to lifestyle change. Further investigation is warranted.
Additionally, patients who have a history of depression should be considered to be at higher risk of not making progress, and additional research to identify effective methods of facilitating lifestyle change in these patients is warranted. Possible interventions to investigate include optimization of pharmacotherapy prior to or during participation in the lifestyle medicine program, more intense face-to-face behavioral health counseling as part of the lifestyle medicine program, and/or increased social support and touch points (e.g., face-to-face or via a digital mental health intervention) during program participation in order to counteract low motivation that is often associated with depression. Clinicians could also focus on lifestyle strategies that are specifically known to improve depression symptoms (e.g., exercise, mindfulness-based practices, and positive psychology).47-49 Of note, patients’ self-reported depression symptoms at the time of program consultation did not predict their likelihood of making progress toward lifestyle change. This may be because patients were uncomfortable endorsing the full severity of their mood symptoms or because their depression symptoms fluctuated during their time in the program. 50 In any case, patients who report well-controlled symptoms of depression at the time of program initiation may still need to be monitored closely to facilitate optimal progress and lifestyle change.
Limitations
Some limitations exist which should be considered when interpreting the generalizability of the study findings. First, this was a single-center study, so the findings may be somewhat unique to the patient population and treatment protocol of the program under investigation. Of note, the study findings represent an “all-comers” patient population which includes patients who were referred to the program by a health care provider or who referred themselves, and patients had varying degrees of understanding regarding lifestyle medicine at the time of initial consultation. The proportion of patients who made progress toward lifestyle change should be interpreted in this context. Second, the regression analyses considered a large number of candidate predictors relative to the available sample size, so it is possible that other relevant predictors exist and were not detected. We reduced the likelihood of missing relevant predictors by taking an exploratory statistical approach and not adjusting for multiple comparisons, and additional investigation could be helpful to confirm the study findings. Third, as with many lifestyle medicine interventions, especially for those which are often not sufficiently covered by third party payers, the patient population in this study had limited sociodemographic diversity. In particular, our study population was predominantly White, female, and had private or Medicare insurance. Analysis of a more diverse cohort may reveal some sociodemographic predictors of patients’ likelihood of making progress toward lifestyle change that were not identified in this study. Finally, additional potential influencers of successful lifestyle change were not systematically documented and therefore could not be assessed as relevant predictors or potential confounders in our population. Relevant factors may include a history of, and contributors to, previous unsuccessful attempts with lifestyle change, in addition to whether a patient is attempting lifestyle change alone vs in tandem with a friend or family member. 51
Conclusion
In this study, patients who identified the intrinsic motivator of stress reduction were more likely to make progress toward lifestyle change during participation in an interprofessional lifestyle medicine program, and patients who had a primary goal to lose weight or who had a history of depression were less likely to make progress toward lifestyle change. To maximize a patient’s likelihood of successfully making lifestyle changes, clinicians and patients may consider focusing on identifying a primary goal and related intrinsic motivating factors that will be immediately and palpably affected by lifestyle change efforts, such as stress reduction. Additional research is warranted to identify effective program-level approaches to maximize success for patients with a history of depression.
Supplemental Material
Supplemental Material - Predictors of Progressing Toward Lifestyle Change Among Participants of an Interprofessional Lifestyle Medicine Program
Supplemental Material for Predictors of Progressing Toward Lifestyle Change Among Participants of an Interprofessional Lifestyle Medicine Program by Abby L Cheng, Mollie E Dwivedi, Adriana Martin, JD, Christina G Leslie, Daniel E Fulkerson, Kirk H Bonner, Julia B Huecker, Elizabeth A Salerno, Karen Steger-May in American Journal of Lifestyle Medicine.
Footnotes
Acknowledgements
The authors would like to thank the Washington University Living Well Center clinical team members for their contributions to data collection as part of standard clinical care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported by the National Institutes of Health (K23AR074520, UL1TR002345, P30CA091842); Doris Duke Charitable Foundation; and Jacqueline N. Baker Washington University Living Well Center Fund.
Ethical Statement
Data Availability Statement
As instructed by the Washington University IRB, de-identified data from this study are not available because data were obtained from the retrospective review of clinical medical records such that patients did not have an opportunity to consent for data sharing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.