
Abstract
Physical activity (PA) and self-compassion (SC) have been shown to positively impact mental and physical health. Findings from a prior review provided evidence of the positive effect of PA on SC. The increased interest and published studies in this area in recent years are not surprising. Since the last review, we have experienced surges in stress and inactivity as well as a global pandemic. Thus, the aims of the current review are to provide an update on the state of the science for PA activity and SC, pinpoint gaps and advances, and provide future directions for this burgeoning literature. A total of 10 recent studies, with n = 6808 participants, were reviewed, including 7 non-experimental and 3 experimental studies. Most (6 out of 7) of the non-experimental studies reported a significant association between SC and PA or related variables in varying populations. Overall, this review corroborated past findings on the relationship between SC and PA, highlighted the extension of this work to new populations and physical activities, and identified interesting emerging trends. A better understanding of how these critical components of self-care “work” could help dramatically improve quality of life and have important public health implications, especially in our post-pandemic world.
“Findings from recent studies shed new light on how SC can influence physical activity.”
Introduction
Physical activity (PA) and self-compassion (SC) have both been shown to positively impact mental and physical health. Regular PA is strongly associated with lower risk of all-cause mortality, cardiovascular disease, hypertension, type 2 diabetes, hyperlipidemia, certain cancers, dementia, depression, and falls, as well as improvements in cognition, quality of life, anxiety, sleep, weight control, bone health, and physical function. 1 While the benefits of PA are already well-established, there is emerging evidence connecting SC with lower perceived stress,2,3 better physical health,4-6 and participation in health-enhancing behaviors. 7
Self-compassion, as posited by Neff et al, is comprised of three elements (self-kindness, mindfulness, and common humanity), all of which likely play an important role in initiating and sustaining health behavior change. 8 For example, when trying to become more active, people inexorably slip up (e.g., leave the fitness tracker on the counter, or skip a scheduled workout). Self-criticism and judgment can be demotivating in such situations, whereas acknowledging that everyone makes mistakes, accepting/observing related negative thoughts or feelings, and showing oneself sympathy and understanding may represent healthier alternatives. Such self-compassionate approaches may prevent minor setbacks from becoming full relapses to a sedentary lifestyle.
A prior review in this area described the positive effects of PA on SC. 9 The results of this study suggest that there is both a direct path and an indirect path between SC and PA, suggesting PA has a significant impact on SC. The positive effects elicited from PA and SC include a reduction of mental vulnerabilities, namely, depression, anxiety, and negative perceptions of self-worth. 9 The effects of this relationship conversely have been found to bolster psychological well-being, with PA and SC increasing self-esteem and multiple modalities of self-worth. 9 Yet, the relationship between these two variables is likely more complicated, perhaps even bidirectional, and requires further investigation. Moreover, studies included in the prior review focused mostly on women and mind-body exercise (e.g., yoga-based, tai chi) which limits the generalizability of the findings to the general population (men) and other exercise types (e.g., brisk walking). 9
There has been a rapid increase in the number of published studies on SC and PA in recent years. In fact, given recent surges in stress, inactivity, and the global pandemic, this topic is likely more pertinent than ever. Recent literature reviews have found that the COVID-19 pandemic has resulted in marked increases in sedentary behaviors as well as diminished PA, with some studies suggesting that only 40% of adults carried out some form of exercise throughout of lockdown. 10 Further, mental health was found to worsen greatly worldwide during this period, with anxiety and depression rates increasing by 25% during the first year of the COVID-19 lockdown. 11 A better understanding of the subtleties/nuances in the relationship between PA and SC could have important clinical and public health implications. Thus, the current review aims to provide an update on the state of the science of PA and SC and pinpoint gaps and advances in this burgeoning field since the last review.
Search Strategy and Study Selection
The primary searches were conducted to identify and retrieve peer-reviewed experimental and non-experimental (correlational, observational, descriptive, longitudinal) studies that examined the relationship between PA and SC. The initial search was conducted in February 2022 with a follow-up search in April 2022. The initial search engines used were PubMed, CINAHL, SCOPUS, and PsychInfo, while the follow-up search focused on PubMed’s database. Terms used in the search included: “exercise,” “physical activity,” or “physical fitness,” and “self-compassion.” Boolean operators were utilized to ensure both components were present in prospective studies. The follow-up search included the additional term “self-kindness” and was limited to studies published between 2019 and 2022.
Inclusion criteria were constructed broadly to ensure a complete review of the literature. Included studies (1) had measures of both SC and PA or related constructs and (2) were published in English. The exclusion criteria were: (1) literature reviews, (2) protocol-only reports, (3) published prior to 2002, and (4) studies previously reviewed by Wong et al.’s 2021 systemic review and meta-analysis.
Results
Results of the article selection process are provided in the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flowchart in Figure 1. Of the 430 records identified, 257 were excluded based on title and abstract screening, leaving 173 records. A total of 52 duplicate records were then removed. The remaining 121 records were screened for eligibility at the full-text level. During the full-text review, 111 articles were excluded. This resulted in 10 articles that met the inclusion criteria for the analysis, including 3 experimental studies and 7 non-experimental studies (Figure 1). Flow diagram of literature search and study selection.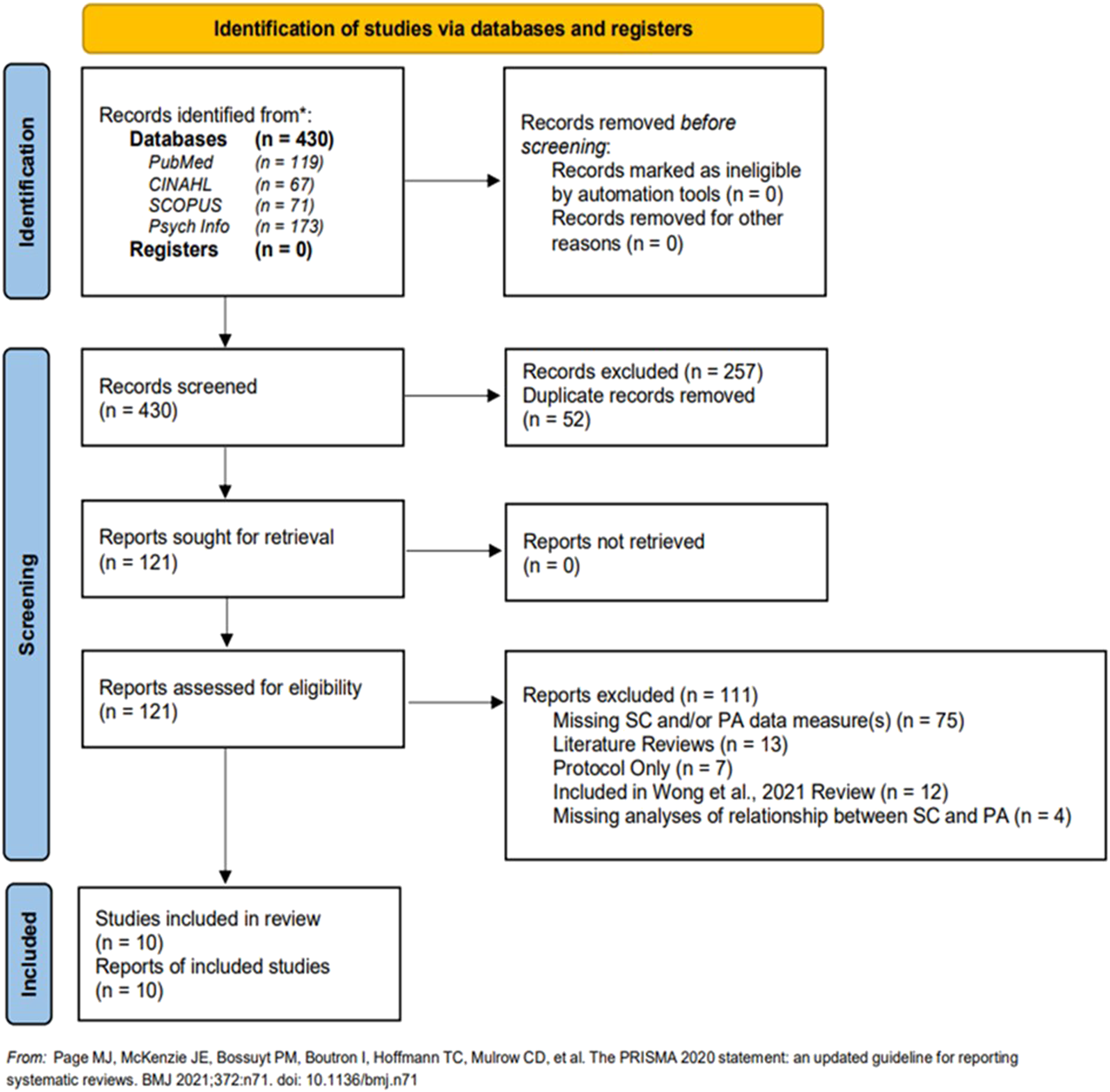
Risk of Bias
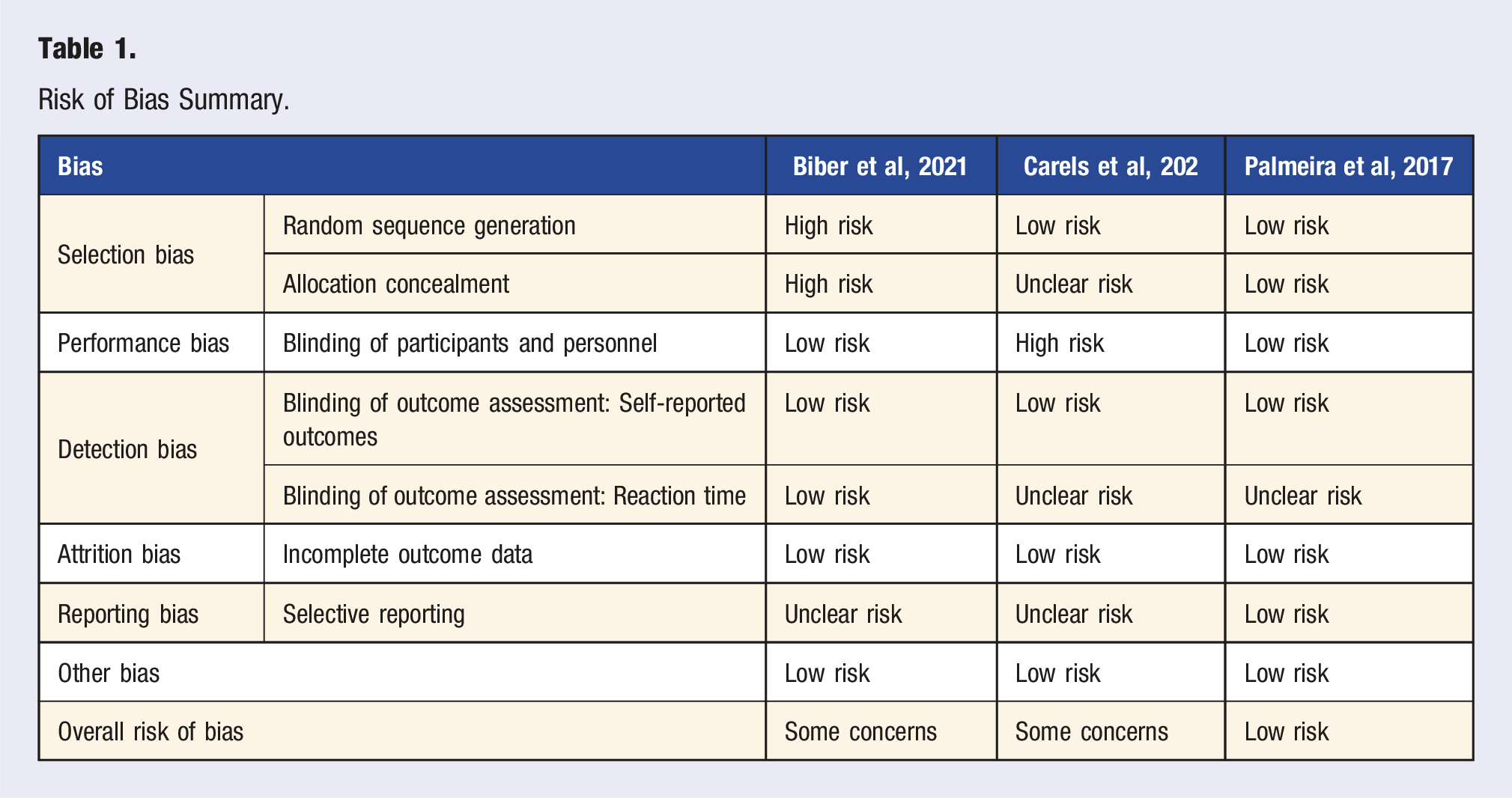
Quality assessment for the randomized control trials was performed utilizing the RoB 2 tool, 12 in accordance with the Cochrane Handbook 13 to assess the risk of bias associated with the effects of assignment to intervention, specifically the impacts on PA and SC as they relate to these interventions Table 1. Two of the studies were noted to have some concerns;14,15 however, the bias risks in question are unlikely to significantly alter the results of the PA and SC relationship. Biber, Rice, Ellis, 15 a workplace intervention, lacked randomization which raises some concerns for selection bias due to participants being assigned to a group at the department level. Study administrators matched departments based on comparable demographic qualities and department size in hopes of maintaining comparable baseline data while also reducing communication between control and intervention groups. Meanwhile, concerns of unclear blinding with no mention of intention to treat principles utilized in analysis and varied lengths of participation between treatment and control groups were present in Carels, Miller, Shonrock, Byrd, Haley. 14
Sample Descriptions
Intervention Studies
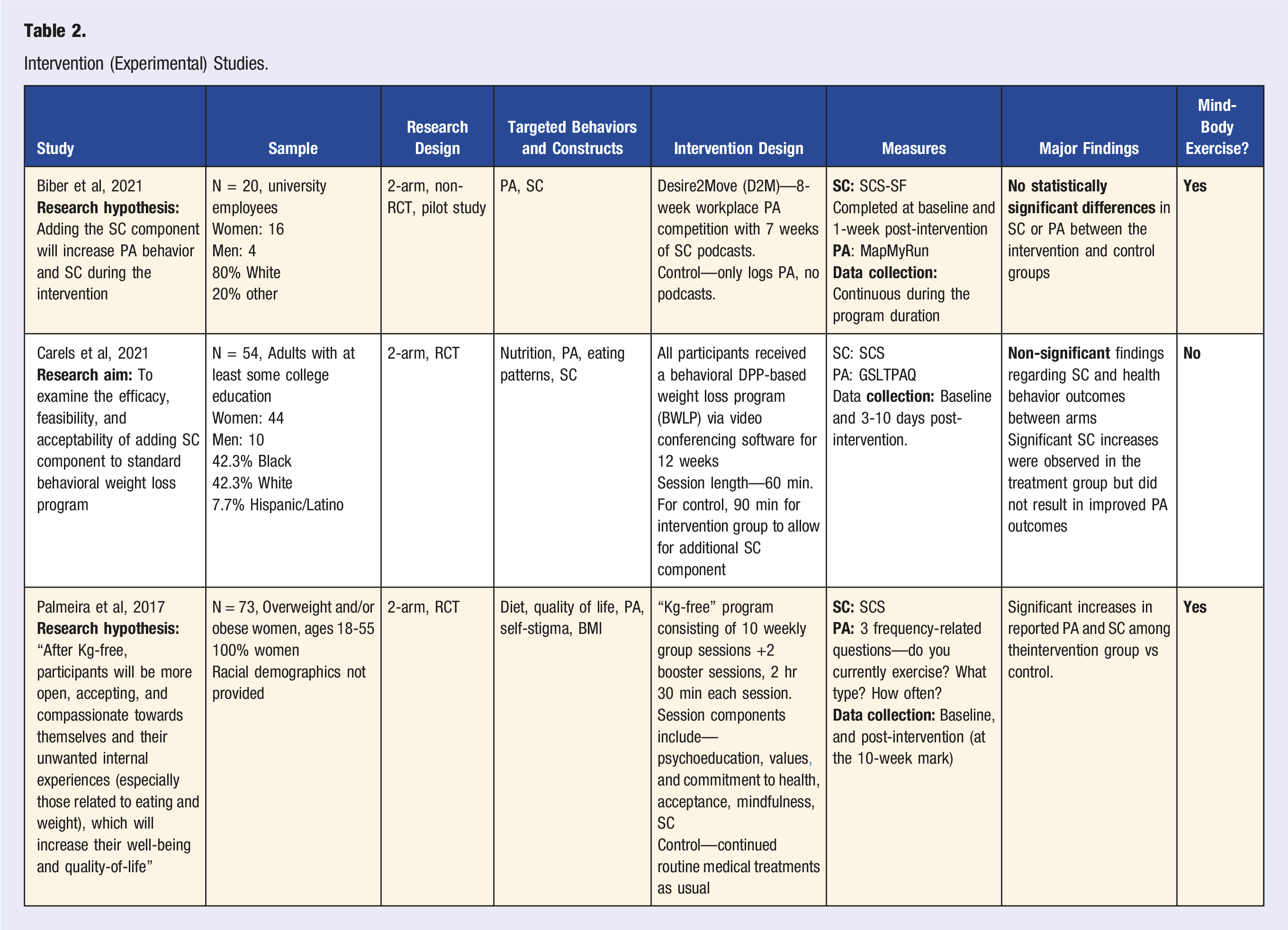
Three intervention studies met the criteria for inclusion in the review (total N = 147 participants) Table 2. Sample sizes ranged from 20 to 73 participants (M sample size = 49). The average age was 45.73 years (SD = 1.18 years) with an average of 87.17% of these three samples identifying as female.14-16
Two of the studies were conducted in the United States14,15 and the other was conducted in Portugal. 16 While Carels, Miller, Shonrock, Byrd, Haley 14 reported an equal ratio of black and white participants in their intervention arm (42.3% white, 42.3% black, 7.7% other), other samples reported mostly (80%) white participants, 15 or did not report race or ethnicity as in the study from Portugal. 16 Only one of the studies reported the sexual orientation of their participants; 14 however, results and discussion did not revisit differences among participants based on sexual orientation. This may have been due to the limited number of participants reporting orientations other than heterosexual. Two of the studies were limited to participants with a minimum of some college-level education.14,15 This limitation was due to the connection of these studies to university populations. Biber, Rice, Ellis 15 recruited university employees in their workplace study, while Carels, Miller, Shonrock, Byrd, Haley 14 recruited through an e-mail listserv announcement distributed to individuals at a university. Employment was only reported in Biber, Rice, Ellis, 15 but as this was a workplace study there was a 100% employment rate, and therefore no data analysis to reflect intervention about employment was provided. Similarly, Palmeira, Pinto-Gouveia, Cunha 16 was the only study to include marital status in their participant demographic information but did not provide further analysis of intervention results in comparison to this variable.
Income and socioeconomic status reporting was handled differently among the three studies. Two studies utilized income brackets to categorize participants. Of these, one reported 42.2% of participants with incomes of $100,000 or greater.15,16 Of those below this income, Biber, Rice, Ellis 15 noted 35% of their participants reported incomes between $50,000 and $99,000. Palmeira, Pinto-Gouveia, Cunha 16 categorized socioeconomic status (SES) as lower, medium, or high income with the majority reporting medium SES (72%).
Observational Studies
The seven observational studies included in our review resulted in a total of 6661 participants Table 3. These seven reviewed studies spanned several countries, with participants being found in the United States, Canada, Italy, Spain, the United Kingdom, Lithuania, Portugal, Japan, Hungary, Australia, and China. These studies’ sample sizes ranged from 39 to 3161 participants (M sample of 952). While most studies assessed SC and PA within participants over the age of 18 (overall mean age = 32.49 years old, SD = 8.78 years), two studies included adolescents.17,18 Most of the studies did not describe race or ethnicity9,18-21 but the two that did reported predominantly white participants.22,23 Across the samples, males made up 41.13% of participants (N = 2740) while the remaining 58.79% consisted of women (N = 3916). Additionally, five participants did not identify as male or female. Of the articles reviewed, two studies had a majority or close to equal male sample.17,21 The remaining five articles consisted mostly of women,18-20,22,24 with two of these including solely female participants.20,22 Finally, of the seven studies, only three (43%) asked participants about their socioeconomic situation which limits the ability of researchers to compare results against these variables.
Study Design
Intervention Study Design
Two of the intervention studies were randomized controlled trials (RCT) utilizing 2-arm designs,14,16 while another utilized a non-randomized control design in which university employees were assigned to treatment conditions at a department level. 15 Two of the intervention studies analyzed in this review utilized attention control conditions,14,15 while the other utilized a true control group. 16
Duration of the interventions ranged from 1 to 12 weeks in length with a mean length of 10 weeks (SD = 2 weeks). All three of the interventions targeted SC as a part of their interventions to determine the effects on PA. Biber, Rice, Ellis 15 sent participants daily, SC-themed podcasts to listen to, while the other interventions utilized weekly group sessions during which SC was discussed among participants.14,16 It is worth noting that Carels, Miller, Shonrock, Byrd, Haley 14 held their sessions through online video conferencing software, while Palmeira, Pinto-Gouveia, Cunha 16 conducted in-person sessions.
As for PA intervention components, two of the interventions included mindfulness meditation practices within their interventions.15,16 One study utilized SC to encourage healthy dietary choices along with increased exercise engagement; however, recommendations were to increase general activity levels and did not assign or suggest specific exercise types or parameters. 14
Non-Experimental Study Design
The seven non-experimental studies included six cross-sectional studies, in which (mostly online) survey data was collected on SC and PA and related variables (lapses). One study used a paper questionnaire. 19 A non-experimental longitudinal study was also included, which examined how participation in Barre fitness classes over 2 months affected SC over time and included 2 assessment time points (baseline and 2 months later) with mind-body exercises and other activities used as covariates in the analyses. 20
Measures
Self-Compassion Measures
SC and PA measures varied across the studies in our review. All ten of the reviewed studies included a variation of Dr. Kristin Neff’s Self-Compassion Scale. 25 Within the reviewed literature two variants of Neff’s Self-Compassion Scale were used, these being the standard 26-item Self-Compassion Scale (SCS) and the 12-item Short Form Self-Compassion Scale (SCS-SF). 25 These scales assess SC by having the participant rate various situations related to SC on a scale of 1-5, with 1 being “almost never” and 5 being “almost always.” 25 These scales have demonstrated both strong test-retest reliability and good validity. 26 Despite the difference in items between the SCS-SF and SCS measures, their internal validities are comparable to one another. SCS has a Cronbach Alpha Score of .922 while the SCS-SF has an internal validity of .957. 27
Physical Activity Measures
Physical activity measures were more varied than their SC counterparts. Only three of the ten reviewed studies shared a common PA assessment tool.14,21,22 These studies utilized the Godin-Shephard Leisure-Time Physical Activity Questionnaire (GSLTPAQ). This self-report measure assesses the frequency and intensity of mild, moderate, or strenuous weekly PA. 28 This questionnaire has demonstrated strong test-retest reliability and validity. 28 Additionally, one study used the International Physical Activity Questionnaire Short Form (IPAQ), which is a nine-item questionnaire on the amount of PA undergone each week.19,29 This questionnaire has also been shown to have good reliability as well as validity. 29 Unlike the GSLTPAQ, the IPAQ investigates sedentary activities such as sitting as well as physically moderate and vigorous activities. 29 The six studies that did not share PA measurement tools used an array of various scales, with unique, self-administered questionnaires being commonplace.9,15,16,18,20,24 These questions asked about the frequency and/or intensity of exercise but were unique to each study and lacked reliability or validity information.
Results
Intervention Studies
The intervention studies produced mixed results. All three interventions targeted SC and two resulted in increased SC among participants.14,16 The latter two studies both utilized the SCS. 25
Only one study reported significant increases in PA with weekly exercise frequency among intervention participants (from 1 to 4/5 times per week). 16 While Palmeira and colleagues conducted their study in person with a nontreatment control, the other two studies which did not show improved PA among intervention participants, were conducted remotely14,15 and involved attention control conditions.
Observational Studies
We reviewed seven studies that used non-experimental methodology. Most (six) of the studies reported a significant association between SC and PA or PA-related variables in varying populations (e.g., students, community sample, new mothers).9,15,19-22 Overall, greater SC was linked to more PA (or related variables, e.g., response to relapse). For example, Hamel and colleagues found that among a sample of gym members, there was a positive association between the number of exercise classes (N = 39) attended (retrospectively) and SC while controlling for self-esteem. 20 Among secondary students in Hong Kong (N = 1074), Wong and colleagues found that PA was associated with all three aspects of SC: self-kindness, common humanity, and mindfulness, and that SC decreased as students aged regardless of PA status. 17 Biber and colleagues reported a positive association between SC and exercise identity in a large community sample in the United States. 15 Similarly, among mothers of young children who previously identified as exercisers (before motherhood), SC was positively associated with current exercise behavior, acceptance of reduced PA (after controlling for age and number of children), and engagement in exercise after a lapse in an exercise program. 22 In another cross-sectional study, SC was also associated with a more adaptive response to an exercise lapse among college students and a sample recruited online, along with higher levels of intrinsic motivation to exercise, but negatively associated with maladaptive emotional reactions to an exercise lapse, controlling for self-esteem, age, and perceived importance of the exercise lapse. 21
Risk of Bias Summary.
Intervention (Experimental) Studies.
Observational (Non-Experimental) Studies.
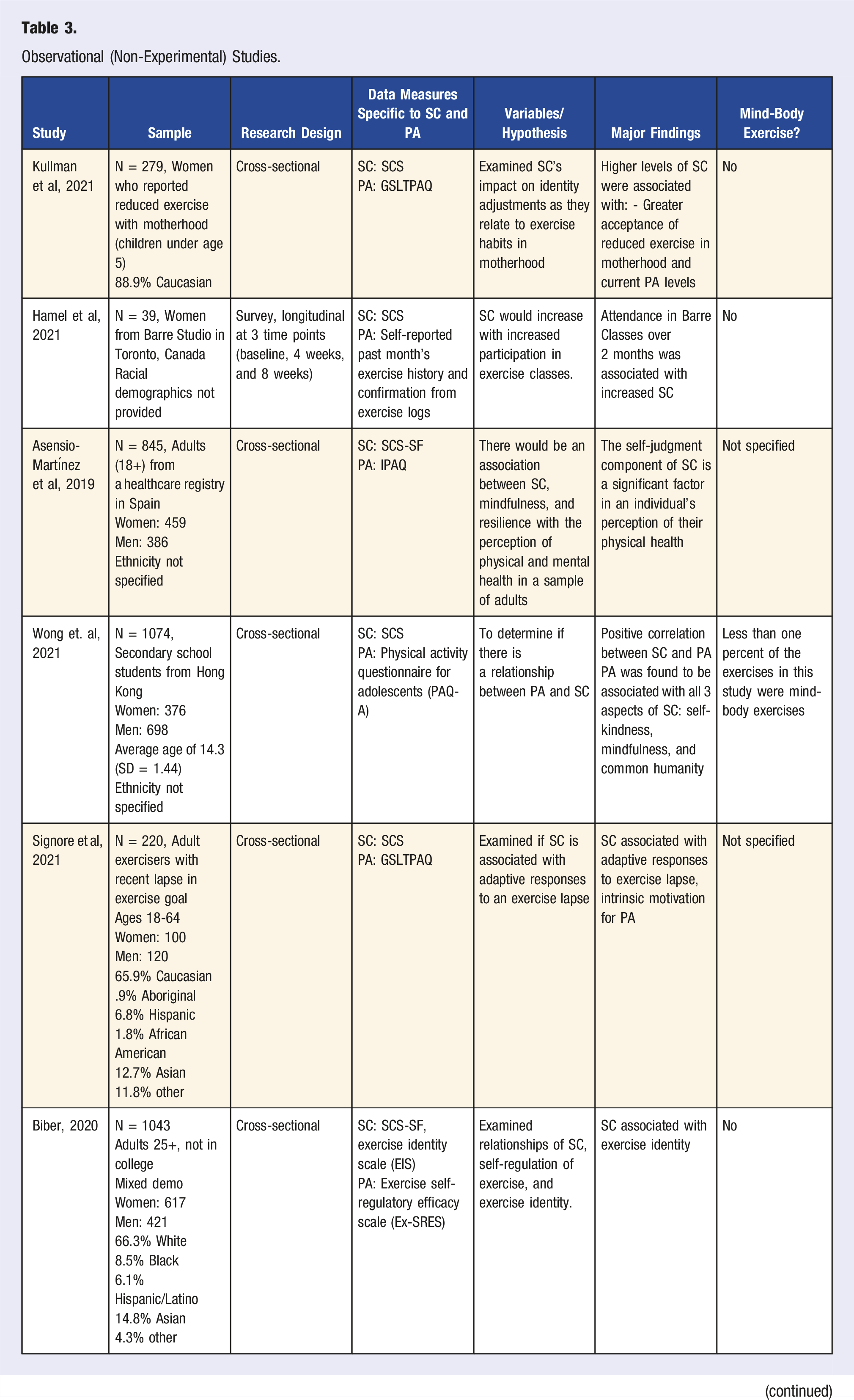
In summary, it appears that SC is related to different aspects of PA, and these findings were supported across diverse samples. While Dores, Carvalho, Burkauskas, Simonato, De Luca, Mooney, Ioannidis, Gómez-Martínez, Demetrovics, Ábel, Szabo, Fujiwara, Shibata, Ventola, Arroyo-Anlló, Santos-Labrador, Griskova-Bulanova, Pranckeviciene, Kobayashi, Martinotti, Fineberg, Barbosa, Corazza 18 did not find an association between PA and SC, a variety of other studies did support the relationship between these factors. Three studies reported SC can play a role in increasing the amount of PA conducted among participants.15,20,22 Additionally, two studies found SC to play a role in how someone views their identity as an exerciser.15,22 Three studies reported SC to have a role in how individuals respond to a lapse in their PA behaviors.19,21,22 Lastly, one study reported PA’s role in increasing SC. 17
Discussion
Wong and colleagues 9 conducted a systemic review of the literature to determine if there is a causal relationship between PA and SC. While they found evidence to support causality of PA influencing SC, it’s likely that the relationship between these two variables is more complicated and perhaps bidirectional. The goal of the current study was to expand on Wong’s review and assess the nature of the PA-SC relationship. Indeed, findings from recent studies shed new light on how SC can influence physical activity.
There were only three experimental studies included in this review; yet, most of these interventions targeted and significantly improved SC through PA.14,16 Identifying positive effects in PA seemed more of a challenge, with only one of the three interventions reporting improvements in this area. 16 Trends in findings from the experimental studies indicated a slight advantage for more intensive intervention duration/contact frequency and face to face (vs. virtual) delivery channels. For instance, the two studies that reported improved SC involved weekly 60-to-150-min sessions for 10-12 weeks,14,16 while the Biber, Rice, Ellis 15 study required only seven, brief (5-24 min) weekly podcasts.
The way the intervention was delivered, modality was likely a factor in the effectiveness of some of these intervention studies. For instance, one intervention that reported increases in PA was delivered in-person, 16 while the other two interventions, without significant changes in PA, were administered remotely,14,15 as necessitated by the COVID-19 pandemic. While the differences in findings could be a result of the remote vs in-person format, the inclusion of a new variable, COVID-19, cannot be overlooked, especially reports that found significant decreases in PA during the duration of the lockdown. 10 Such design considerations should be further explored in future intervention efforts targeting PA and SC, as the available intervention studies (and their methodological differences, e.g., in the rigor of comparison conditions, outcome assessment, etc.) still do not allow us to draw firm conclusions on best practices or relationship direction at this time.
Moreover, studies included in the Wong review focused mostly on mind-body exercise (such as mindfulness meditation, yoga, and tai chi) which limited the generalizability of the findings to other exercise types (e.g., brisk walking). The mind-body exercises are utilized frequently. Research in SC and PA literature is largely biased towards women with 82.2% of yoga practitioners being women. This illustrates that mind-body exercises are largely skewed to a female population, limiting the generalizability of using solely these exercises. Finding the exercise types that are more evenly distributed would be beneficial for study’s generalizability. Researchers observed that three prior observational studies that contained large male sample sizes largely did not utilize mind-body exercises, instead opting for other forms of exercise such as aerobics, sports, or going to the gym. With this in mind, future research should emphasize on varying exercises as a means of increasing the diversity of samples. In Wong et al.’s 2021 study, researchers described the lack of younger samples in SC and PA literature. The present review found a continuation of this pattern, with only one study of secondary school students as well as a single study addressing undergraduate students. Research is needed among these younger populations, especially considering the vulnerability of these age groups amidst mental health issues.
Improvements in gender representation were observed among observational studies with 41.13% of participants reporting their gender as male when compared to the prior review. 9 Unfortunately, this representation was lacking in interventional studies with only 12.83% of participants reporting gender as male. This is a consistent problem in both the obesity 30 and mindfulness literature as well. 31
There continue to be gaps in the diversity of samples, as the average of Caucasian participants reported nearly seventy percent (68.7%) among those studies that reported racial demographics. Wong 9 reported a saturation of middle-aged to older adult samples in their review, lacking studies in adolescent and young adult populations. This review found a continuation of this pattern, with only one study of secondary school students as well as a single study addressing undergraduate students. Research is needed among these younger populations, especially considering the vulnerability of these age groups amidst mental health issues.
Strengths and Limitations
Similarly to Wong, 9 this review saw a standardized pattern of using Dr. Neff’s Self-Compassion Scale (in full or short forms) to measure SC among participants. However, a lack of standardization among PA measures was noted in this review as well as a potential overuse of self-report measures. Biber, Rice, Ellis 15 suggested future studies should assess PA through the use of direct measures to improve the accuracy of findings. Additionally, moving towards a more standardized and commonly used measure for PA would improve external validity.
Among intervention studies, limitations with the implementation of SC components presented a common theme. Carels, Miller, Shonrock, Byrd, Haley 14 reported a limited dosage of their SC component. Additionally, Biber, Rice, Ellis 15 acknowledged that while motivation for change was provided to participants, little to no clear, step-by-step guidance on how to make changes necessary to improve SC was provided. Palmeira, Pinto-Gouveia, Cunha 16 did not add SC materials until towards the end of their intervention, leaving participants minimal time to practice and develop skills to improve SC before post-intervention measures. While SC did see improvements across these studies, it appears the best application of this newer construct may not be fully identified.
Furthermore, when looking at how to apply SC to interventions, it is worth looking at the various components of SC, as described by Dr. Neff. 8 Don, Van Cappellen, Fredrickson 32 analyzed how different components of SC (mindfulness vs loving-kindness) impacted physical activity, which may provide insight into which of Dr. Neff’s SC components are most helpful in application of interventions. Don, Van Cappellen, Fredrickson 32 noted that mindfulness meditation provided greater increases in physical activity than loving-kindness among participants in their studies; however, further research regarding the application of these constructs is needed.
Suggestions for Future Research
There have been some efforts to improve male representation in samples, with the number of participants reporting their gender as male in observational studies being 41.13%. Unfortunately, this representation was lacking in interventional studies with only 12.83% of participants reporting gender as male. Furthermore, racial and ethnic diversity is needed, specifically minority representation. Race was only reported in five of the ten studies (50%), one of which was based in Hong Kong. The remaining four studies reported average participant samples to be comprised of approximately 69% Caucasian participants (80%, 42.3%, 88.9%, and 65.2% white; M = 69.1%; SD 4.27). Additionally, Wong 9 reported a saturation of middle-age to older adult samples in their review lacking studies in adolescent and young adult populations. This review found a continuation of this pattern, with only one study of secondary school students 17 as well as a single study addressing undergraduate students. 14 Further research is needed among these younger populations, especially considering the vulnerability of these age groups amidst mental health issues.
Future studies should also consider the inclusion of sexual orientation as a demographic category, in accordance with guidance from the American Psychological Association (APA) 33 as these identifiers may provide insight that would otherwise be missed during data analysis. The absence of this data inclusion risks promoting social and lifestyle stereotypes of LGBTQ+ individuals. 33
Furthermore, when looking at how to apply SC to interventions, it is worth looking at the various components of SC, as described by Dr. Neff. 8 Don, Van Cappellen, Fredrickson 32 analyzed how different components of SC (mindfulness vs loving-kindness) impacted PA, which may provide insight into which of Dr. Neff’s SC components are most helpful in application of interventions. Don, Van Cappellen, Fredrickson 32 noted that mindfulness meditation provided greater increases in PA than loving-kindness among participants in their studies; however, further research regarding the application of these constructs is needed.
Clinical Implications
While it is still unclear the direction of the relationship between PA and SC, the literature we reviewed does suggest that SC may play a role in being physically active. Therefore, SC exercises could be useful in working with clients who are trying to increase PA or in athletes who struggling with plateaus or performance issues. SC strategies could be a useful tool to help facilitate increased movement and have the added benefit of helping encourage self-kindness and beneficial cognitions that can often be barriers to being more active.
Conclusion
Overall, there is still much to learn about the bidirectionality of the relationship between SC and PA. This review shows the clear potential for the use of SC as a tool to improve PA among individuals and calls for further understanding of these variables’ relationship.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.