
Abstract
Office-based workers typically have a sedentary lifestyle and spend the majority of their working hours sitting, which can lead to an increased risk of cardiometabolic diseases. This cross-sectional study aimed to quantify sedentary behavior and overall physical activity, and to determine their association with cardiometabolic risk factors in a cohort of 122 office workers. Sedentary behavior and physical activity were assessed using questionnaires and wrist-worn Axivity accelerometers. Weight, height, body mass index, waist circumference, waist-to-height ratio, blood pressure, and point-of-care blood variables (namely, lipids and lipoproteins, glucose, and glycated hemoglobin) were also measured. Most (68.0%) of the study participants were women, with a mean age of 40.2 ± 9.3 years. The self-reported total daily sedentary time for this cohort was 595.5 min/day (IQR: 413.5-863.4 min/day). Accelerometry-measured sedentary behavior was positively associated with light physical activity (β: .98, P = .001) and inversely associated with moderate-to-vigorous activity (β: −.08, P = .01). Both systolic (β: −.234, P = .037) and diastolic blood pressure (β: −.250, P < .001) were inversely associated with accelerometry-measured light physical activity. However, there was no association between sedentary behavior and cardiometabolic risk factors. Our findings show that South African office workers spend a substantial amount of time sitting during work hours and while commuting, and support the need for public health workplace interventions to mitigate the potential health risks of sedentary behavior.
Keywords
“The major strength of our study is the inclusion of self-reported and objective measures for assessing physical activity and sedentary behaviors.”
Introduction
Obesity and related cardiometabolic diseases continue to rise and are projected to double in prevalence by 2030, with low-and-middle-income countries having the highest rates of obesity. 1 In 2022, the World Health Organization reported that these diseases were the leading cause of premature death globally and that of all noncommunicable chronic disease-related deaths, approximately 77% occur in low- and middle-income countries such as South Africa. 2
Physical activity is the leading modifiable risk factor for cardiometabolic diseases and all-cause mortality.3,4 Moreover, in the last two decades, research has highlighted that sedentary behavior is an independent risk factor for poor health outcomes, regardless of meeting the recommended weekly minimum requirements for structured physical activity.5,6 Specifically, excessive sitting has adverse associations with obesity and related diseases resulting in increased mortality rates.6,7 The Sedentary Behavior Research Network defines sedentary behavior as any waking behavior characterized by an energy expenditure ≤1.5 metabolic equivalents while sitting, reclining, or lying. 8 In contrast, emerging evidence suggests that interruption of sitting time with light physical activity or even standing results in improvements in cardiometabolic biomarkers. 9
The working adult population typically spends the majority of their time in sedentary positions while at work, commuting to work, and during recreation.10,11 In particular, an average employee spends 75%-85% of their workday sitting behind their desk in high-income countries. Similarly, Gradidge et al. in their recent qualitative study found that South African office workers spend 6-8 h in sedentary positions. 12 According to a recent systematic review and meta-analysis comparing device-measured movement across occupations, 9 office-based workers reported low levels of physical activity and the highest sedentary time compared to their colleagues in other occupations. This is particularly concerning considering that developing countries such as South Africa are also experiencing a transition toward more sedentary occupations and its accompanying association with potential adverse health effects. 13
Existing evidence has predominantly employed self-reported questionnaires to measure physical activity and sedentary behaviors, which are prone to social recall, overestimation, and bias.14,15 However, there has been an increase in the number of studies reporting on accelerometry and other device-based measured physical activity and sedentary behaviors, although such data are more expensive to collect and time-consuming to analyze. 16
Previous systematic reviews examining strategies to decrease sedentary behavior and improve cardiometabolic risk factors among individuals working in office settings have yielded modest improvements or demonstrated the potential for ameliorating various cardiometabolic risk factors such as elevated blood pressure, excess central fat, reduced high-density lipoprotein (HDL) cholesterol, and elevated blood glucose levels.17,18 However, due to the lack of evidence on the relationships between objectively measured physical activity and sedentary behaviors with cardiometabolic risk factors amongst South African workers, further investigation is necessary to address this research gap, particularly as it relates to office-based workers. This study aimed to quantify sedentary behavior and overall physical activity using self-reported questionnaires and accelerometers. It also sought to determine the associations between these activity patterns and select cardiometabolic risk factors among South African office-based workers.
Methods
Study Design and Participants
The cross-sectional study of 122 workers was conducted at the University of the Witwatersrand, Johannesburg, and at a credit bureau company in Johannesburg, South Africa. Office-based workers from the University of the Witwatersrand were invited by e-mail to participate in this study, while credit bureau employees were recruited through e-mail invitations from the human resources department. Ethics approval was obtained from the Human Research Ethics Committee (Medical), University of the Witwatersrand (ethics certificate number M190224). All participants provided written consent. The inclusion criteria included adults aged 18 years and older who worked in an office for at least 3 days a week with access to a desk or workstation within an office, the ability to communicate in English, and the ability to walk and/or stand for at least 10 min.
Questionnaires
A demographic questionnaire was used to obtain information on age and sex. Monthly income was self-reported in South African Rands (ZAR) and then converted to United States Dollars (USD). The five categories used were: prefer not to answer, <1100 USD, 1100-1375 USD, 1376-1650 USD, and >1650 USD. Self-reported sedentary behavior for the previous 7 days was quantified using the Last 7 Days Sedentary Time Questionnaire (SIT-Q-7d). The SIT-Q-7d is acceptable for use in epidemiological studies, with criterion validity for domain-specific variables ranging from .22 to .76. 19
Anthropometry
Body weight was measured using a digital weighing scale to the nearest .1 kg (Omron HN288, Japan). Height was measured to the nearest .1 cm using a stadiometer (Seca 123, USA) and converted to meters (m). Obesity was defined as a body mass index (BMI) of ≥30.0 kg/m2 for both males and females. 20 Waist circumference (WC) was measured using a cloth inelastic measuring tape (Gulick, USA) at the narrowest part of the torso between the lowest ribs and the iliac crest, with feet together and arms hanging by the side. Central obesity was defined by a WC greater than 102 cm for males and 88 cm for females. 21 All measurements were administered with participants in minimal clothing by the principal investigator and trained research assistants.
Blood Pressure
The Omron M7 automated blood pressure (BP) monitor (Omron M7 Intelli IT (HEM-7322T-E), Omron, Kyoto, Japan) was used to measure brachial BP. In accordance with the American College of Sports Medicine’s standardized procedures, 20 three measurements were obtained after the participant had rested for at least 5 min in a seated position with the back supported and with an appropriately-sized cuff around the right upper arm, supported at the level of the heart. 22 The average of the last two BP measurements was recorded. Hypertension was defined as systolic BP (SBP) ≥ 140 mmHg and/or diastolic BP (DBP) ≥ 90 mmHg or a history of hypertension or use of antihypertensive medication(s). 22
Point-of-Care Blood Samples
A finger was pricked to draw non-fasting capillary blood samples. The HemoCue Glucose 201RT system (Ängelholm, Sweden) was used to measure random glucose. Glycated hemoglobin (HbA1c) was measured using the HemoCue HbAlc 501 system (Ängelholm, Sweden). 23 The HemoCue HbA1c 501 system correlates with laboratory HbA1c tests (rho = .995- P < .001).24,25 A diagnosis of diabetes was defined as random glucose ≥11.1 mmol/L, HbA1c ≥ 6.5%, use of antidiabetic medication(s), or history of diabetes. Total cholesterol, HDL cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides were measured using the CardioChek Plus analyzer (Polymer Technology Systems, Inc.). The CardioCheck Plus analyzer demonstrates good clinical agreement with a reference analyzer, ranging from 95% to 98%. 26 Abnormal total cholesterol was defined as ≥ 5.2 mmol/L or the use of medication(s) for the management of hypercholesterolemia. Participants previously undiagnosed for abnormal BP and/or blood values were advised to seek medical attention.
Accelerometer
Wrist-worn Axivity accelerometers (AX3; Newcastle-upon-Tyne, United Kingdom) were used to objectively measure sleep, sedentary behavior, light physical activity (LPA), and moderate-to-vigorous physical activity (MVPA). The AX3 monitor has been validated for total energy expenditure and has been used in large-scale surveillance studies such as the UK Biobank study. 27 Participants were instructed to wear the accelerometer for a minimum of 14 h a day for seven consecutive days, except during water-related activities (e.g., bathing and swimming). Raw continuous wave accelerometer data was processed using GGIR (version 2.8-2), an R-package (version 4.2.3). At least 4 days and ≥16 h of wear time during the 7 days was considered acceptable for data analysis.
Statistical Analysis
Statistica 13.1 (StatSoft, Tulsa, USA) was used for all analyses. Descriptive statistics were presented as mean ± standard deviation, median (interquartile range) for continuous data, and frequencies and percentages for categorical data. A multiple linear regression model was used to estimate the association between cardiometabolic risk factors and objectively measured physical activity and sedentary behavior, reporting the regression coefficients (β) and their respective adjusted R2 values. In the models, all independent variables were considered, while the dependent variables encompassed BMI, WC, SBP, DBP, Hb1AC, HDL cholesterol, triglycerides, sedentary behavior, LPA, and MVPA. The following independent variables were initially included in the regression models: gender, age, current smoking, WC, DBP, hours of sleep, sedentary behavior, LPA, and MVPA. Prior to multiple linear regression, simple univariate regressions were performed to identify the independent variables associated with the dependent variables, which were later included in the regression models. Backward, stepwise removal of non-significant variables was performed until the final model remained with significant variables. Significance was set at P < .05.
Results
Participant Demographics, Cardiometabolic Measures, Self-Reported Sedentary Behavior, and Accelerometry Data.
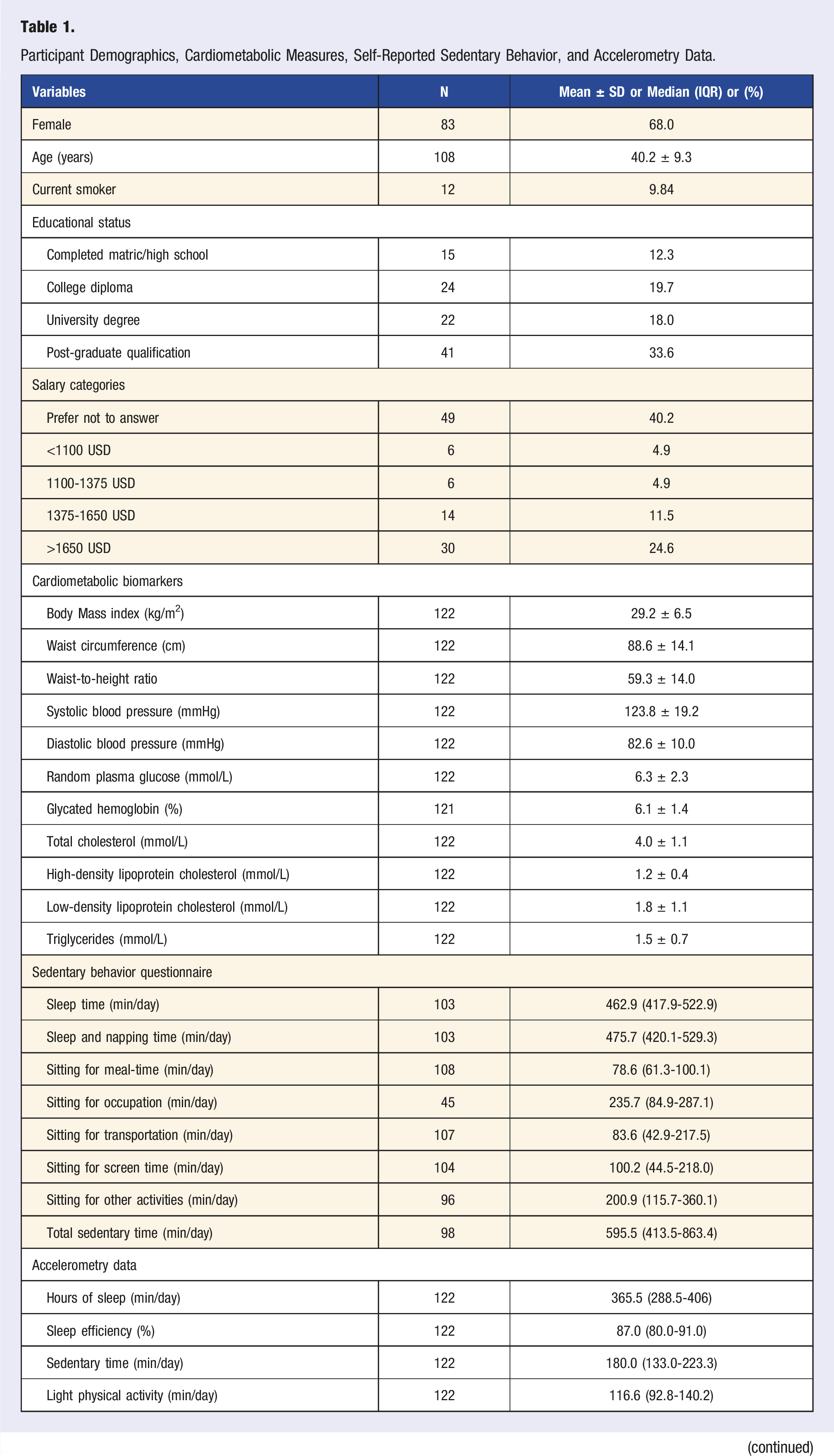
As can be seen in Table 1, the self-reported total daily sedentary time for this cohort, accumulated in different sitting activities, was 595.5 min/day (Interquartile ranges (IQR): 413.5-863.4 min/day). Furthermore, our participants reported sleeping for an average of 462.9 min/day (IQR: 417.9-522.9 min/day). Accelerometry data showed a sleep duration for an average of 365.5 min per night and sleep efficiency of 87.0%. When using the accelerometers, participants were sedentary for a mean of 180.0 min/day (IQR: 133.0-223.3 min/day), participated in LPA for 116.6 min/day (IQR: 92.8-140.2 min/day), and actively engaged in MVPA for 47.1 min/day (IQR: 24.2-83.6 min/day).
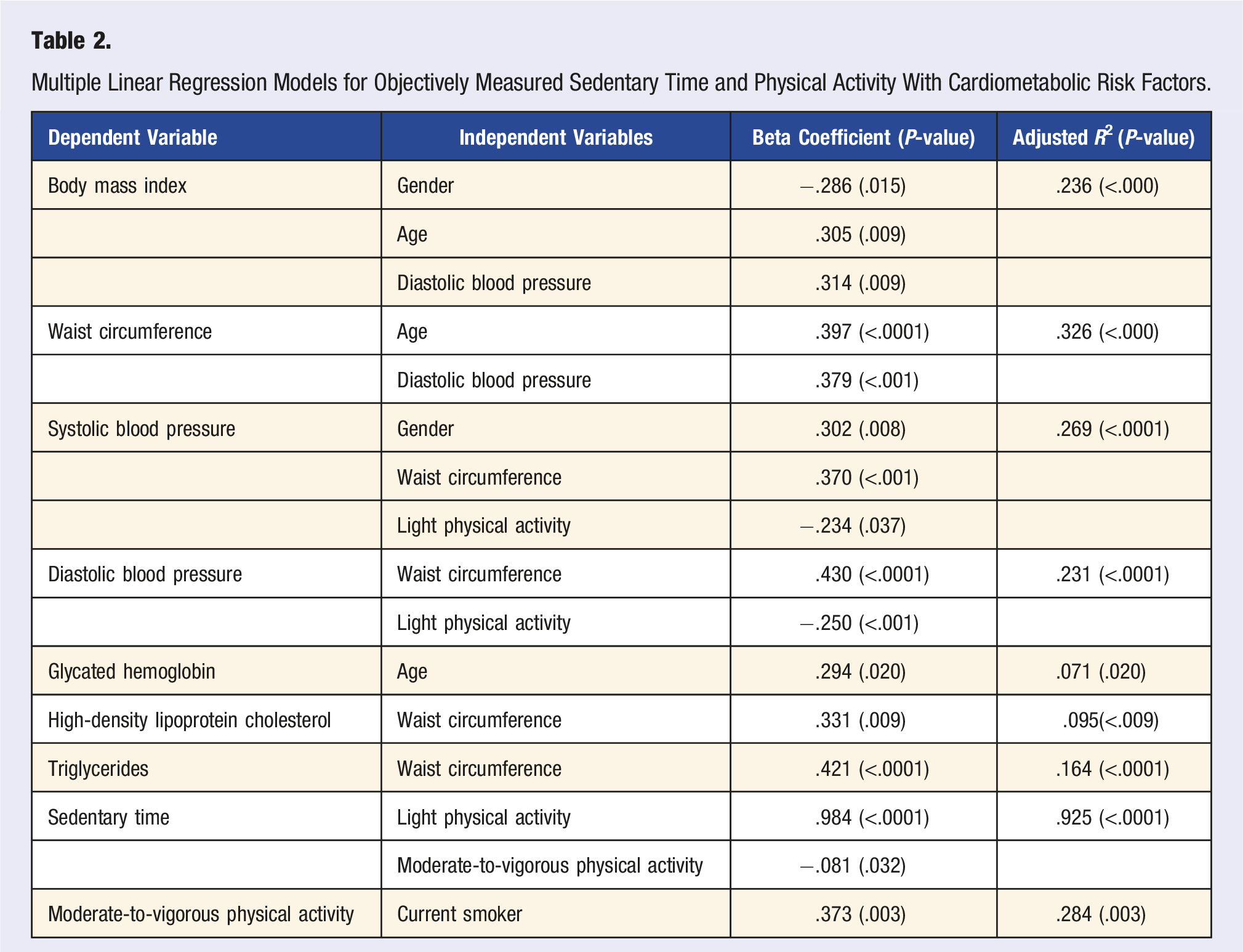
Multiple Linear Regression Models for Objectively Measured Sedentary Time and Physical Activity With Cardiometabolic Risk Factors.
Discussion
The purpose of the current study was to measure sedentary behavior and physical activity using self-reported questionnaires and accelerometers and examine their associations with specific cardiometabolic risk factors in a cohort of office-based workers in South Africa. Our self-reported questionnaire data indicate that South African office-based workers spend most of their wake time in sedentary positions with minimal energy expenditure. This observation is of importance because existing evidence has shown that physical activity outside the workplace does not offset the increased risks of mortality and morbidity that result from time in sedentary positions.11,16
Our study participants spent an average of about 235.7 min/day sitting at work and another 83.6 min/day sitting for transportation. Thus, it appears that there is an urgent need for public health interventions to promote both breaking prolonged sitting time at work by interspersed bouts of standing/physical activity and actively commuting to and from work, where feasible, to mitigate the future burden of cardiometabolic diseases among working South African adults.12,13
In agreement with extensive research attesting to the overestimation of subjectively-reported sedentary behavior, 28 our study shows higher self-reported sedentary behavior compared to objectively derived measures. Notably, our accelerometry results revealed significant negative (i.e., favorable) associations between both SBP and DBP and LPA, a finding that is consistent with previous research demonstrating that lower-intensity exercise training may lower BP as much or more than moderate- or higher-intensity exercise training.3,29,30 However, no association was observed between accelerometry-measured sedentary behavior and cardiometabolic biomarkers. This finding is similar to those of Silva et al who investigated different sedentary behavior patterns in Brazilian adults, their interrelationships, and associated factors 31 but inconsistent with those of other studies demonstrating a detrimental association between sedentary time and cardiometabolic biomarkers.32,33 The lack of a significant relationship between sedentary behavior and cardiometabolic biomarkers in our study could potentially be explained by the relatively high levels of physical activity in this cohort of South African office workers. Regarding the latter, many of our participants met the recommended guidelines for participation in MVPA (namely, at least 150 min/week) despite being employed in a sedentary occupation. 34
The major strength of our study is the inclusion of self-reported and objective measures for assessing physical activity and sedentary behaviors. The major limitation of our study is the relatively small sample size which was further compounded by the fact that almost 40% of the study participants did not comply with the seven-day minimum requirement of wearing the AX3 accelerometer monitors. Additionally, the fact that our study was conducted in only two employer organizations may limit the generalizability of the findings beyond university office-based workers and credit bureau employees. Clearly, future research should include a larger sample size to establish a possible independent association between sedentary behaviors/physical activity and cardiometabolic risk factors in clusters of South African office-based workers from multiple diverse employer organizations.
Conclusions
In our study, South African office-based workers spent considerable time sitting while at work and commuting to and from work. When active, workers spent more time engaged in LPA than MVPA. Although no association was observed between accelerometry-measured sedentary behavior and cardiometabolic biomarkers, there was a favorable association between SBP, DBP, and LPA. Although additional research is warranted, our findings support the need for public health workplace intervention programs to mitigate the health risks associated with sedentary behavior and insufficient physical activity. In particular, our observations show that workplace interventions to address sedentary behavior and cardiometabolic risk factors in South African populations should focus on breaking sitting time by standing and moving more and, where feasible, promoting physically active modes of transportation to and from work.
Footnotes
Acknowledgments
The authors acknowledge the participants and the research assistants.
Author Contributions
MP and PJG conceived the study design. MP analyzed and interpreted the data, and drafted the manuscript. NG and PJG provided interpretive and editorial input. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MP is supported by the South African NRF Thuthuka grant. PJG is supported by the South African Medical Research Council [SAMRC] with funds received from the Self-Initiated Research Grant [SIR]. Any opinion, finding, conclusion, or recommendation expressed in this material is that of the author(s) and the NRF does not accept any liability in this regard.