
Abstract
Dementia, or major neurocognitive disorder, is one of the most common causes of disability and dependency in older adults with far-reaching social, physical, and economic impacts. In the absence of adequate treatment, much research has been directed towards prevention. Physical exercise has been shown to increase cerebral blood flow, amplify production of neurotrophic factors, and enhance brain volume. Whether these changes on a structural and cellular level result in cognitive preservation is less clear. This systematic review synthesizes findings from seventeen randomized controlled trials that examine the effects of physical activity on global cognition, memory, and executive function in older adults. Cognitive benefits of exercise are strongest for those who are cognitively intact or with mild cognitive impairment. In studies with long-term follow up, cognitive gains tended to decay after cessation of physical intervention suggesting that sustained physical exercise may be required to preserve cognitive function in older adults prior to onset of dementia.
“Physical fitness and cognitive gains were associated with increases in regional brain volume or blood flow in some studies.”
Introduction
Major neurocognitive disorder, or dementia, is characterized by progressive deterioration of cognitive function beyond what is considered a normal part of the aging process. In addition to memory, dementia can irreversibly impact behavior, language, learning ability, and comprehension and it remains 1 of the biggest threats to independence and identity. There are several different types of dementia, with Alzheimer’s disease (AD) accounting for greater than 60% of cases. 1 As the world’s population continues to age, the prevalence of dementia is expected to grow. The World Health Organization predicts that nearly 82 million people worldwide will be living with dementia by 2030. 2 This number does not include people living with mild cognitive impairment (MCI), which is characterized by cognitive deficits that do not yet interfere with daily functioning or independence. 3 Those with MCI are 6.7 times more likely to progress to Alzheimer’s disease than those without cognitive impairment. 4
As there is currently no cure or reversal agent for dementia, there is increased interest in strategies to prevent cognitive decline and halt disease progression. Physical exercise, particularly multicomponent aerobic exercise and strength training, is one of the most heavily researched and promoted lifestyle interventions to improve general health and longevity. Regular physical exercise for healthy adults is defined in the Physical Activity Guidelines issued by the U.S. Department of Health and Human Services as 150 minutes of moderate-intensity aerobic exercise in addition to at least 2 days of strength training per week. 2 Regular physical exercise has been shown to lower risk of heart disease, stroke, hypertension, and type II diabetes mellitus, all of which are modifiable risk factors for dementia.
There are several different mechanisms by which aerobic and strength training exercise may influence brain health. In this review, we define the term “physical exercise” and “exercise” to include both aerobic and strength training exercise regimens overall, unless specified otherwise. By increasing cardiac output, physical exercise raises cerebral blood flow which, if repeated on a regular basis, can positively impact neural function, and reduce oxidative stress. 5 Physical Exercise also increases production of several trophic factors, including brain-derived neurotrophic factor (BDNF), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF-1), leading to amplified neuroplasticity and angiogenesis. In addition, cellular senescence, or cell cycle arrest, is a key process that results in vascular endothelial dysfunction and contributes to many age-related diseases. 6 As compared to a sedentary lifestyle, habitual aerobic exercise prevents endothelial cell senescence, reduces oxidative and inflammatory responses, and protects the vascular endothelium, all of which contribute to healthy aging. 6 Self-reported aerobic exercise has specifically been shown to reverse the impact of APOE status on amyloid deposition in middle age to older adults. 7
In addition to molecular and biochemical enhancements, aerobic exercise can impact brain structure. In a randomized controlled trial by Colcombe et al, brain volumes were compared between healthy elderly volunteers who participated in either a 6-month aerobic exercise regimen or stretching program. MRI imaging pre- and post-intervention showed significantly increased brain volume in both pre-frontal and temporal cortices in the aerobic exercise group. Both areas mediate higher order cognitive functions and are affected in age-related cognitive decline. 1 The intervention group experienced average reductions in risk of brain volume loss of 42.1%, 33.7%, 27.2%, and 27.3% in the anterior cingulate cortex, right superior temporal gyrus, right middle frontal gyrus, and anterior white matter tracts of the corpus callosum as compared to non-aerobic controls. In another randomized controlled trial, Erickson found a 2% increase (P < .001) in bilateral anterior hippocampal volume of cognitively intact adults (mean age 67.6) who participated in 1-year of moderate-intensity exercise. This is compared to a 1.4% decline in hippocampal volume in the stretching control group (mean age 65.5) over the same period of time. 8 Although passive stretching does not improve brain health, stretching exercises that incorporate dynamic and postural movements with meditative practices (i.e.,. Tai chi and yoga) have also been shown to positively impact brain structure.9-12 Whether these changes on a cellular and structural level have a clinically meaningful effect on cognition is less clear. The primary objective of this review is to synthesize current data that examines the benefits of physical activity on brain health and prevention of cognitive decline.
Methods
Search Strategy
A systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. We identified all literature related to clinical outcomes of aerobic and strength training exercise or physical activity on cognition for individuals with different levels of cognition. We analyzed studies ranging from cognitively intact individuals to those with moderate cognitive impairment and a diagnosis of dementia that were published between January 2000 and March 2023. Two reviewers (P.D. and M.K.) independently conducted global searches in March 2023 using the following databases: PubMed, Google Scholar, and EMBASE. A search using the following MeSH terms of “cognitive impairment” or “Alzheimer’s disease” or “dementia” AND specific intervention (“physical activity” or “exercise”) was conducted to evaluate the literature base. Inclusion criteria consisted of randomized control studies written in or translated into English that evaluated the impact aerobics or strength training exercise and physical activity has on either cognitively intact participants or those with mild to moderate cognitive impairments. Exclusion criteria involved non–English language studies, studies without a proper control group of usual activity, and those that included confounding variables such as supplemental mental training or nutritional supplements (i.e., omega-3s). Additionally, articles studying those with severe dementia or with interventions less than 12 weeks in duration were excluded. After the literature search and application of inclusion/exclusion criteria, all articles selected for inclusion were cross-referenced to ensure no studies were overlooked during the initial search. The references of chosen articles were also reviewed for pertinent studies.
Study Selection and Quality Assessment
Studies were included if they were randomized controlled trials (RCT) published after January, 2000, had a sample population that was either cognitively intact, with MCI, or mild to moderate dementia and included at least 1 exercise intervention that lasted 3 months (12 weeks) or longer. Studies with sample populations diagnosed with severe cognitive impairment or with underlying psychiatric conditions were excluded to minimize confounding factors, as these have been reviewed elsewhere. 13 The Cochrane Risk of Bias Tool was used to assess the quality and risks of bias of studies identified in the investigation. The Cochrane Risk of Bias Tool criteria evaluate studies based upon 5 different domains of bias: selection, performance, attrition, reporting and other. 14 This tool has been typically used to evaluate randomized control trials and in each domain the rater (MK) is to evaluate the study for High, Low or Unclear risks of bias. 14
Results
Results of the search process are displayed in Figure 1. A total of 1607 studies were identified from our initial search. 171 of these studies were randomized controlled trials, 168 of which were published after January 2000. After assessing the title and abstract, 50 articles were selected for further evaluation. Of these, 37 were excluded for the following reasons: 4 evaluated caregivers of those with dementia, 17 had additional confounders representing a multimodal approach such as mental training, acute supplementation, and music for the intervention group (these included 2 studies investigating the impact of dance as well), 3 had duration of intervention less than 12 weeks or 3 months, 9 focused on mental health variables or only assessed cognitive impairment via the NPI (Neuropsychiatric Inventory), 2 were eliminated for the severity of dementia symptoms. One was excluded as they did not have a proper control group and another investigated mahjong and tai chi’s impact rather than robust aerobic or anaerobic exercises regimens. This yielded 13 studies and, after reviewing the references, 4 additional studies were added as they met all the listed criteria. After an extensive electronic search, 17 studies were found that met eligibility criteria. Flowsheet describing the search strategy.
Description of Randomized Controlled Trials.
IG/CG = intervention group/control group; SIVCI = subcortical ischemic vascular cognitive impairment; EMOD/EHIGH = moderate resistance/high resistance; rCBF = resting cerebral blood flow; HRR = heart rate reserve; MICT/LICT = moderate-intensity continuous training/low-intensity continuous training; RTx1/RTx2 = once weekly resistance training/twice weekly resistance training.
Cochrane Risk of Bias Tool Results.
Random Sequence Generation: Adequately described the randomization process to allow assessment of whether it should produce comparable groups. Allocation Concealment: Described method used to conceal the allocation sequence in sufficient detail to determine whether intervention allocation could have been foreseen before or during enrollment. Selective Reporting: Stated how the possibility of selective outcome reporting was examined by the authors and what was found. Blinding Participants and Personnel: Describes measures to blind study participants and personnel from which intervention a participant received. Blinding Outcome Assessment: Describes measures to blind outcome assessors from knowledge of which intervention participants received. Attrition Bias: Describes the completeness of outcome data including attrition and exclusions from analysis. Other: Any other important concerns about bias not addressed above.
Seventeen studies compared the intervention group to a non-aerobic control; however, there was significant variability in the prescribed activity for the control group. 33 Most studies compared the exercise group to an inactive, usual care control. Morris et al. compared 26 weeks of aerobic exercise to a non-aerobic control group that alternated between core strengthening, resistance training, and modified tai chi or yoga. 31 Varela et al implemented recreational activities, including playing cards or doing crafts and 2 studies compared the aerobic intervention to a stretching control.21,27 Sanders et al. compared both low- and high-intensity training to a control group that performed flexibility exercises and recreational activities. 28 Martin-Willett et al. compared cognitive outcomes between 2 intervention groups, a moderate intensity continuous training plus high-intensity interval training group (MICT + IT) and low-intensity continuous training group (LICT). 18 In the 3 RCTs that looked at the effect of resistance training on cognitive function, 1 study compared moderate resistance (50% of 1 repetition maximum) and high resistance (80% of 1 repetition maximum) training to a control group that did similar exercises without overload training 15 and the other 2 studies compared a resistance exercise protocol to a balance and tone or stretching program.32,34 Most studies reported >60% adherence to exercise intervention. Muscari et al included participants with at least 50% compliance in endurance exercise training and 3 studies did not specify degree of adherence.17,18,25 Strategies used to promote compliance included direct supervision, in-class attendance, and behavioral interventions (i.e., motivational telephone calls, target setting, visual reminders).
Characterization of Cognitive Tests.
WAIS-III = Wechsler Adult Intelligence Scale, Third Edition; WMS-IV = Wechsler Memory Scale, Fourth Edition; WMS-R = Wechsler Memory Scale-Revised; CLVT-II = California Verbal Learning Test, Second Edition; D-KEFS= Delis-Kaplan Executive Function System.
Exercise and Global Cognition
The ADAS-Cog and MMSE are 2 common tests of global cognitive impairment. The ADAS-Cog is an 11-item assessment of memory, language, and praxis that is routinely used as the primary neuropsychological test in many AD drug clinical trials. 34 The MMSE, which is the most frequently used test to screen for dementia in primary care settings, is also comprised of 11-questions that assess various cognitive domains; however, it is more influenced by educational level and may be less sensitive and reliable than the ADAS-Cog. 35
In studies that used the ADAS-Cog as the primary outcome measure, some showed superiority in global cognitive function among the aerobic exercise group over non-aerobic controls after completing the intervention; however, significance was lost by long-term follow-up. 36 Liu-Ambrose et al found a mean difference of 1.7 points on the ADAS-Cog between the exercise and control groups at the end of the 6-month aerobic intervention (P = .02); however, this is less than the accepted minimal clinically relevant difference of 3. This difference lessened to .63 and was not statistically significant at 12-month follow up (P = .46). Lautenschlager et al found similar results with an improvement of 1.3 points on the ADAS-Cog in the exercise group relative to the non-aerobic control at the end of the intervention, which lessened to .69 at six month follow-up (P = .04). In a pilot randomized controlled trial by Yu et al (n = 96), participants who engaged in 6 months of aerobic exercise experienced a smaller within-group change in the ADAS-Cog score at the end of the intervention than would be expected for typical Alzheimer’s disease progression, which was described as 3.2 +/− 6.3-point increase. There was not a significant difference in the change in ADAS-Cog score between the intervention and control groups at 6 and 12-months; however, this finding was expected as the pilot study was not powered to detect between-group differences. Given the heterogeneity within these studies, it is difficult to ascertain comprehensive conclusions. Further studies are needed to provide additional robustness to the current state of literature. Specifically, future studies should focus on the impact of a supervised exercise program for those with MCI. Liu-Ambrose et al demonstrated the largest effect size within the ADAS-CoG group and employed a supervised walking program. This suggests that despite its lower intensity, benefits can be realized from an escalating in intensity supervised exercise regimen rather than a prescribed home exercise program with less accountability. Further studies should assess the benefit of higher intensity supervised exercise and its impact on this test amongst those with MCI.
The Dementia and Physical Activity (DAPA) trial, which is the largest study included in this review (n = 494), generated contrasting results. There was no improvement in ADAS-Cog following exercise intervention and the ADAS-Cog scores worsened at 12-month follow up in both trial arms. Notably, the participants in this study already had a diagnosis of dementia and had significantly higher ADAS-Cog scores at baseline (21.4 in control group, 21.2 in exercise group), which is indicative of worse global cognitive function.
Out of the 6 studies that used MMSE scores as primary outcome measures, 2 studies showed marginal improvements post-intervention in the exercise group as compared to the control; however, these differences similarly dissipated on long-term follow up.17,24 Muscari et al found that healthy elderly participants had reduction in cognitive decline as assessed by the MMSE after 12-months of endurance exercise when compared to inactive controls. On immediate follow up, the intervention group had a 2.74 times higher likelihood of maintaining their cognitive status when compared to the control group; however, there is no long-term data to assess cognitive maintenance in this study population. 20 Of note, however, these 2 positive studies were performed on those who were deemed cognitively intact. Sanders et al compared MMSE scores of elderly adults who engaged in low- and high-intensity aerobic and resistance training to a flexibility control group and found no statistically significant between-group differences at the end of the 6-month intervention. Further long-term studies need to be conducted and the validity of the MMSE in varied levels of cognition needs to be more established. Out of the 6 studies that used MMSE scores to evaluate global cognitive function, 3 carried a diagnosis of mild to moderate dementia. All 3 of these studies showed that there was no statistically significant difference between baseline and post-intervention performances on MMSE for those with mild to moderate dementia.28-30
Exercise and Memory
Although there are several different types of memory, each can be broadly classified into short and long-term memory. Ten studies assessed components of memory through use of various neuropsychological tests as outlined in Table 3. Cassilhas et al demonstrated improvement in short-term and episodic, long-term memory after 24-weeks of moderate or high-intensity resistance training compared to non-overload controls. 15 This study also looked at serum IGF-1 levels as higher concentrations have been associated with improved cognitive function. 34 Both intervention groups had higher levels of IGF-1 following resistance training when compared to the control group, with no statistically significant difference in concentration when comparing moderate and high-intensity regimens.
Other components of memory that benefited from exercise included immediate recall 15 and delayed recall.16,22 Cognitively intact adults who completed 12-weeks of 1 hour thrice weekly supervised aerobic exercise improved in immediate and delayed text-level memory when compared to usual-care controls. 16 In addition to memory function, Chapman et al also looked at changes in regional cerebral blood flow (rCBF), a biological indicator of brain health and preclinical biomarker for AD. After 3 months of aerobic exercise, the intervention group showed a selective increase of rCBF in bilateral anterior cingulate cortices on pseudo-continuous arterial spin labeling (pCASL) MRI compared to the control group. Improvements in immediate and delayed memory post-intervention were also associated with an increase in hippocampal rCBF mid-intervention. All studies that showed some improvement in memory included participants who were either cognitively intact or with MCI. Four studies that did not find a significant difference in tests of memory after exercise included participants with known diagnosis of mild to moderate dementia.22,26,29,31 One of these studies, however, demonstrated a positive correlation on secondary analyses between peak VO2, a measure of cardiorespiratory fitness, bilateral hippocampal volume, and improvement in memory performance. 31
Exercise and Executive Function
Executive function involves higher level cognitive skills that control organization, attention, working memory, and planning. Deficits in executive function are common in dementia and associated with more severe cognitive disease and worse functional impairment. 37 Out of eleven studies that looked at executive function as either a primary or secondary outcome measure, 6 showed statistically significant improvement following exercise intervention.15,17,21,25 Cognitively intact elderly males who completed 24 weeks of moderate or high-intensity resistance training improved on tests of executive function when compared to controls. 15 These effects were not dependent on resistance intensity as there were no statistically significant differences between intervention groups. Yoon et al similarly found improvements in executive function as measured by the Frontal Assessment Battery and Trail Making Tests following 4-months of high-speed resistance training. Baker et al randomized thirty-three adults with mild cognitive impairment into a high-intensity aerobic exercise group (75-85% HRR) or supervised stretching group. Six months of supervised aerobic exercise improved several domains of executive function, including: multitasking, cognitive flexibility, processing efficiency, and attention. In addition, this study showed sex-specific differences in almost all tests of executive function, with women demonstrating more pronounced improvement in executive control processes after aerobic intervention. Women randomized to the stretching control group experienced worsening performance on tests of executive function at the end of the study. Liu Ambrose et al randomized cognitively intact, community-dwelling women into one of three groups: once-weekly resistance training (RTx1), twice-weekly resistance training (RTx2), or twice weekly toning and balance control group. Women who participated in 12-months of weekly or twice weekly resistance exercises improved by 12.6% and 10.9%, respectively, on the Stroop test, which is a measure of selective attention and cognitive flexibility that requires individuals to name the color of a portrayed word and not the word itself (i.e., participants see the word “red” in yellow-colored font and are supposed to identify “yellow”). This is in contrast to women in the toning and balance group who regressed by .5% at the end of intervention. This study did not, however, find significant differences in tests of set shifting or working memory. Martin-Willett et al randomized cognitively healthy adults into 2 exercise interventions and compared cognitive outcomes following 16-weeks of moderate-intensity exercise with high-intensity interval training (MICT + IT) to low-intensity continuous training (LICT). MICT + IT program started at 60% HRmax and progressed in intensity to include intervals at 85-85% HRmax. LICT group maintained 50% HRmax for all sessions during the intervention. Participants in both groups improved in Stroop effect on error and Category Switch effect reaction time when compared to their baseline, with no difference between exercise groups. Langlois et al found statistically significant improvements in working memory, processing speed and executive function in both frail and non-frail, cognitively intact adults after 12-weeks of moderate to high-intensity aerobic exercise (as measured by modified Borg Rating of Perceived Exertion Scale).
Discussion
This is a robust systematic review of 17 randomized controlled trials following the PRISMA framework that depicts the impact physical exercise has on cognition of cognitively intact adults and those with mild to moderate dementia. These studies were then evaluated for risks of bias, with the most prominent risk coming from inadequate blinding. In these studies where exercise is the intervention, there is an intrinsic difficulty to blind participants as they must actively participate in the prescribed physical activity. The other studies included in this review had no other attributes for high risks of bias. In evaluating this type of research, this is a required acceptable level of potential bias to make recommendations based on conclusions from studies on exercise and many lifestyle interventions.
Evidence Summary of the Impact of Exercise on Cognition.
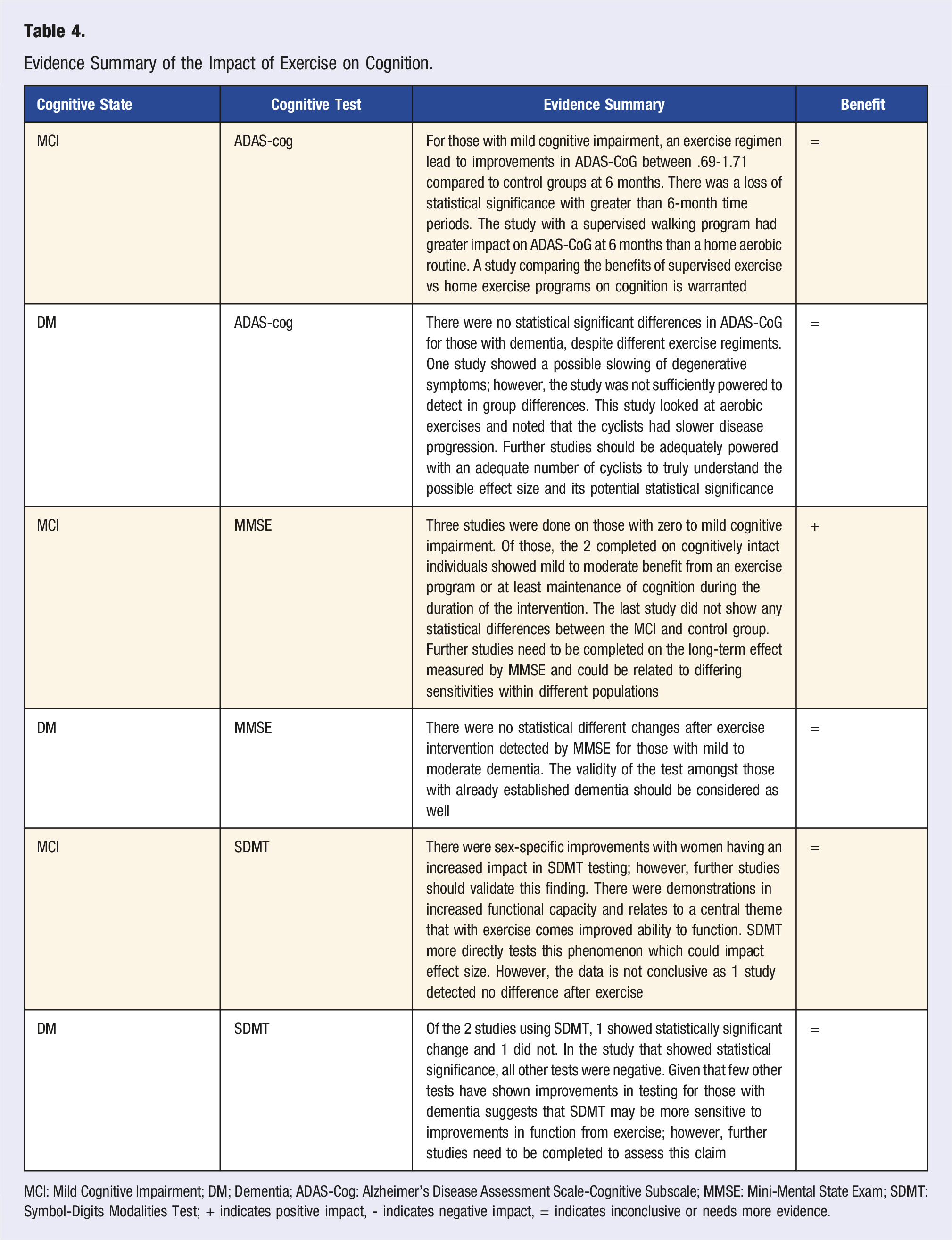
MCI: Mild Cognitive Impairment; DM; Dementia; ADAS-Cog: Alzheimer’s Disease Assessment Scale-Cognitive Subscale; MMSE: Mini-Mental State Exam; SDMT: Symbol-Digits Modalities Test; + indicates positive impact, - indicates negative impact, = indicates inconclusive or needs more evidence.
Previous work has indicated that epigenetic changes may occur following sustained physical exercise, particularly in mechanisms involved in BDNF synthesis, that might lead to sustained brain health benefits from a lifetime of physical activity. 39 There are few prospective studies that examine the effect of sustained physical exercise on cognitive function later in life. The Caerphilly Cohort study followed health behaviors of over 2000 men in Wales for 30 years. Regular physical activity, defined in the study as walking 2 or more miles or cycling at least ten miles per day, had the greatest effect on reducing risk of cognitive impairment (OR .64) and dementia (OR .41) when compared to other behaviors like healthy diet, tobacco avoidance, and moderate alcohol consumption. 40 As part of the Prospective Population Study of Women (PPSW), Hörder et al tracked dementia incidence over a period of 44 years and found risk of dementia to be lowest in those with high cardiovascular fitness in mid-life. 41 Studies in this review found decay in global cognitive improvements within 6 months after participants stopped participating in physical activity interventions, suggesting that permanent changes in cognition and brain health are unlikely in this age group following moderate duration interventions. This suggests that interventions to support ongoing lifestyle change are likely to have greater impact for global cognition than time-limited physical exercise interventions that depend on external motivation.
Improvements in specific components of memory and executive function were observed in response to exercise in many studies, although the strength of these findings was variable. The strongest effects were seen in short- and long-term memory and processing speed. The most beneficial effects were seen in studies that included cognitively intact participants or those with MCI, suggesting that physical exercise may have the greatest impact before people reach the stage of active dementia. However, 1 study did suggest that there may be a dose-response component to improvements in those with dementia with exercise. 28 Hoffmann et al showed that the per protocol analysis showed improvements while intention-to-treat analysis did not show statistically significant improvements in SDMT. 29 The majority of studies have not replicated this finding. This finding aligns with a prior systematic review that found more pronounced cognitive benefits after physical exercise in participants with MCI as compared to those with more advanced disease. 42 Additionally, the SDMT does suggest, however, that it could be more sensitive in detecting functional changes in cognition due to exercise compared to the other common cognitive tests (ADAS-CoG and MMSE) [Table 4]. Further studies should investigate the relative validity within this battery of tests amongst different levels of cognition. In the few studies that also looked at structural and biochemical changes in the brain, physical exercise augmented cerebrovascular blood flow, increased levels of peripheral IGF-1, and lessened hippocampal atrophy, all of which were associated with improved cognitive performance.
Most research has been done with aerobic exercise as the primary intervention. This work has not demonstrated a correlation between intensity of aerobic exercise and degree of cognitive benefit to date. Only 5 studies incorporated strength training as part of the exercise program, making it difficult to draw conclusions about impact. Four studies included group classes in their exercise intervention which could contribute to cognitive benefit by introducing social aspects similar to team and competitive sports. A 2022 meta-analysis by Balbim et al demonstrated no significant effects on cognitive function in individuals with all-cause dementia when exploring treatment-level moderators, including type of intervention (i.e., aerobic, resistance, or multimodal), intensity of exercise, or weekly exercise volume. 42 This study did, however, find an association between higher adherence to exercise intervention and improved cognitive performance. 1 Although multicomponent exercise is the current general health recommendation for physical activity in adults, more research is needed to determine the optimal exercise regimen for cognitive function and brain health over the lifespan.
The studies included in this review were all designed to evaluate the cumulative benefit of regular exercise over a period of exercise intervention. The response-decay cycle of changes in cognitive function around individual exercise sessions was not evaluated. 43 Previous research has demonstrated that peak metabolic and cognitive effects of physical exercise decay over hours to days. 44 The time course to optimal cognitive functioning following exercise is not well understood and may include both cumulative and peak effects. 45 Therefore, the temporal relationship between exercise sessions and cognitive testing could have impacted findings.
Current research on the effects of physical exercise on cognitive function in older adults is limited by small sample sizes and considerable heterogeneity in exercise intervention and primary outcome measures. There is also significant variability in the baseline physical activity of included participants. Although many studies only included participants who were considered underactive or frail, some did not outline specific exclusion criteria for baseline fitness level and may have included participants who were already regularly physically active. The MMSE and ADAS-Cog may not have the sensitivity and responsiveness to detect changes in higher order cognitive functions. The diversity of neuropsychological tests selected to assess cognitive performance make it difficult to synthesize the data and understand the significance of the results. Similarly, there is a lack of evidence evaluating the relative benefit of specific exercise interventions in preventing cognitive decline as the existing RCTs vary significantly on the type, duration, and frequency of exercise utilized as the primary intervention and many common types of exercise (e.g., team sports) have not been evaluated.
Limitations
The limitations of this study are intrinsic to the nature of the studies that were analyzed in our systematic review. Of our 17 studies, 12 had concerns for inadequate explanations of blinding or concerns for inadequate blinding. When studying lifestyle interventions, it is difficult to blind individuals to their lifestyle changes. Additionally, there are lifestyle changes beyond the scope of the study that can impact the results of our study. With increased exercise, there could be changes to diet and other healthy lifestyle choices that could be unaccounted during the course of intervention in our included studies. Furthermore, the category of exercise is so broad that it is difficult to provide comprehensive or universal results that could be expected after these interventions. From the type of exercise, level of coaching or supervision and varied intensity it is difficult to recommend a single exercise regimen based on an individual’s level of cognition. Furthermore, the presented studies have such a wide battery of objective measurement tools that it is difficult to determine the ultimate effect size of the interventions. Within the presented studies 2 different tests were used for global function, 13 were used for memory, and 17 were used to measure executive function.
While previous systematic reviews exist detailing how multicomponent exercise impacts cognition,46,47 our review differs in that our study only is analyzing studies that have at least the recommended 150 minutes of exercise per week. It has been demonstrated that that level of activity is safe for older adults and the authorship felt that it was important to make sure that participants had adequate dose of either aerobic or strength training exercise to determine the possible effect exercise can have.
Conclusion
We found the strongest evidence for improvements in components of memory in response to exercise among people who were cognitively intact or diagnosed with MCI, with weaker evidence of improvements in global cognition and executive function. Physical fitness and cognitive gains were associated with increases in regional brain volume or blood flow in some studies. Improvements tended to decay after interventions were completed. Less meaningful cognitive improvements were demonstrated in those with diagnoses of dementia rather than mild cognitive impairment.
Of note, this review necessitated studies had at least 150 minutes of exercise, the defined minimum for regular exercise per the Physical Activity Guidelines issued by the U.S. Department of Health and Human Services and 12 weeks of duration, which is unique compared to previous reviews. These findings suggest that sustained physical exercise can have a clinically meaningful impact on cognition and brain health among older adults prior to onset of dementia that decays when people stop exercising. This “on-off” phenomenon strengthens the association of cognitive function with current physical activity. Therefore, interventions to support ongoing physical activity may have the greatest potential for cognitive preservation and brain health in older adults in future research.
CME/CE Article Quiz
American College of Lifestyle Medicine (ACLM) members can earn FREE CME/CE credit by reading this approved CME/CE article and successfully completing the online CME/CE activity. Non-members can earn CME/CE for $40 per article. Visit lifestylemedicine.org to join the ACLM.
AJLM CME/CE Articles and Quizzes are offered online only through the American College of Lifestyle Medicine and are accessible at lifestylemedicine.org/store. ACLM Members can enroll in the activity, complete the quiz, and earn this CME/CE for free. Non-members will be charged $40 per article.
A Passing score of 80% or higher is required in order to be awarded the CME/CE credit.
Supplemental Material
Supplemental Material - The Role of Physical Exercise in Cognitive Preservation: A Systematic Review
Supplemental Material for The Role of Physical Exercise in Cognitive Preservation: A Systematic Review by Matt Kaufman, Paige Dyrek, Michael Fredericson, Marily Oppezzo, Megan Roche, Levi Frehlich and Douglas Noordsy in American Journal of Lifestyle Medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.