
Abstract
Objective. A systematic review with a meta-analysis explored effects of cognitively loaded physical activity interventions on global cognition in community-dwelling older adults (≥65 years of age) experiencing mild cognitive impairment (MCI), compared to any control. Methods. A literature search was conducted in 4 databases (MEDLINE [OvidSP], PubMed, CINAHL, and the Cochrane Central Register of Controlled Trials [Wiley]) from inception until January 30, 2018. The meta-analysis was conducted with Review Manager 5.3. Results. Six randomized controlled trials (RCTs) with 547 participants were identified. The interventions ranged from 4 to 52 weeks. Baseline and initial follow-up assessments were used. The primary pooled analysis of all RCTs demonstrated a nonsignificant trivial effect (standardized mean difference [SMD] 0.07, 95% confidence interval [CI] −0.44 to 0.58) favoring the intervention. In pooled subanalysis of 4 RCTs (n = 405) using the same global cognition measure (Mini-Mental State Examination) and duration of intervention >12 weeks, the intervention group achieved a small but significant improvement for global cognition (SMD 0.45, 95% CI 0.14 to 0.75). Conclusion. When all the RCTs were pooled, the effect of cognitively loaded physical activity intervention on global cognitive function in older adults with MCI remained unclear. The subgroup analysis provides translation evidence for future RCT study designs.
‘Investigating the effect of cognitively loaded physical activity interventions on global cognition is necessary because many daily activities are not sequential (executing one step/task after another).’
Dementia is described by the World Health Organization as a global epidemic 1 with a looming economic burden. Mild cognitive impairment (MCI) is defined as objective evidence of significant cognitive impairment, possibly causing small functional impairments beyond expectation for age and education without limiting activities of daily living or representing dementia. 2 It is presumed to be a transitional state preceding the onset of dementia, although some individuals with MCI remain stable and some return to normal cognition. 3 MCI is an important public health concern, as there is a higher conversion of those with MCI to dementia (14% to 18%) than seen in cognitively normal older adults (1% to 2%). 4 Since no pharmaceutical agent has yet been shown to prevent or reverse the progression of cognitive decline in those with MCI, 5 exploring modifiable lifestyle factors such as physical and cognitive activities for their impact on cognitive function could facilitate understanding of their potential for therapeutic approaches.
Investigating the effect of cognitively loaded physical activity interventions on global cognition is necessary because many daily activities are not sequential (executing one step/task after another). Integrated (changing between 2 or more tasks) and concurrent (executing 2 or more tasks simultaneously), these activities require persons continuously to draw on more than one domain of cognition and physical abilities. The reasons include evidence that both cognitive and physical activity increase cerebral perfusion in healthy adults 6 and their simultaneous delivery appears to facilitate neuroplasticity and cognitive function in animal studies. 7 The latter result gains support from a meta-analysis of 20 studies of sequential and simultaneous activity interventions among cognitively healthy older adults aged 65 to 82 years. 8 Secondary analysis revealed that simultaneous interventions had a greater effect on cognitive function than did sequential interventions (simultaneous effect size 0.43, 95% confidence interval [CI] [0.01, 0.86]; sequential effect size 0.27, 95% CI [0.08, 0.46]). 8
Recently, prior systematic reviews have been conducted on simultaneous or sequential cognitive and physical interventions for persons with cognitive decline 9 and healthy cognition, respectively. 10 One of these reviews was narrative and lacked a meta-analysis. 10 Another was a meta-analysis but limited its search strategy to physical and cognitive activity terms. 9 It appears to have treated activities such as dance as physical activities, negating and underestimating their inherent cognitive and social demands. No additional analysis examined potential differences between sequential and cognitively loaded physical activity.
Simultaneous activity, such as cognitively loaded physical activity, may be more effective at improving cognitive function than individual activities delivered sequentially because simultaneous activity requires multiple components of the intervention to work together in a synergistic, mutually reinforcing manner. Their delivery as simultaneous activities could facilitate neuroplasticity and cognitive function according to animal studies. 7 Accordingly, cognitively loaded physical activity interventions should be examined in persons with MCI. Findings from previous systematic reviews remain equivocal as to the effects of cognitively loaded physical activity for persons with MCI.8,9 Therefore, we updated the reviews with recent evidence and performed a meta-analysis of randomized controlled trials (RCTs) systematically identified in the literature. We examined whether cognitively loaded physical activity interventions can in some way influence global cognitive function, be it by maintaining performance levels (relative to groups not getting the intervention) or improving performance in older community-dwelling adults with MCI.
Methods
Design
The meta-analysis was designed, performed, and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 11 (Supplemental Digital Content 1, available online). Systematic searches were conducted in the databases MEDLINE (OvidSP), PubMed, CINAHL, and the Cochrane Central Register of Controlled Trials (Wiley) from their inception through to January 2018. The Supplemental Digital Content 2 (available online) details the search strategy, which was limited to English language publications. No outcome terms were included in the search strategy to avoid excluding trials in which global cognitive function was a secondary outcome measure. Supplementary searches, conducted through Turning Research into Practice, Google Scholar, and Google, included a thorough manual review of references from extracted studies. This search strategy was created, designed, and executed in consultation with a University of Auckland librarian and research services advisor.
Studies were included if they (1) were published, peer-reviewed, full-length articles; (2) were written in English; (3) were RCTs; (4) involved community-dwelling older adults, with more than half aged ≥65; (5) identified MCI using any accepted diagnostic criteria2,12-14 (all the participants met criteria for MCI or a subgroup analysis was completed separately for participants meeting MCI criteria); (6) had interventions where all aspects were delivered as cognitively loaded physical activity, defined and pragmatically selected to include any interventions that simultaneously delivered physical and cognitive components in any activity form, or regimen, in more than one activity session; (7) included a comparison group that did not participate in cognitively loaded physical activity; and (8) measured and reported global cognitive function, a validated measurement tool for assessing multiple cognitive domains, at baseline and follow-up.
Data Selection, Extraction, and Risk of Bias
KZ and RF independently assessed the eligibility of the titles and abstracts through the Rayyan QCRI web platform (rayyan.qcri.org) 15 and full text articles; conducted data extraction and assessed risk of bias. Discrepancies were solved through consensus and with the input of a third author (NK), if necessary. We extracted data on study details, study design, intervention, participant characteristics, MCI diagnosis, and global cognitive function outcomes from each study onto an a priori developed standardized data extraction table, which had been pilot tested in advance. The reviewers (KZ and RF) independently assessed the risk of bias using the Risk of Bias Tool for interventions. 16 Seven items were assessed: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other sources of bias. All these items were scored as having a high risk, low risk, or unclear risk of bias using the tool’s set criteria.
Statistical Analysis
Meta-analysis was completed using Review Manager 5.3 (Cochrane Collaboration) to review our data. Data pooling was carried out for all studies meeting inclusion criteria and completed when 3 or more RCTs reported the same outcome or met the criteria for either subgroup or sensitivity analysis.
All meta-analyses used random-effect models and 95% CIs and compared intervention with control at the most proximal follow-up assessment to the completion of the intervention. The meta-analyses were conducted on standardized mean differences (SMDs) when varying outcome tests were combined. Mean differences (MDs) were calculated when the same outcomes were used. The pooled SMD was used to calculate the effect size. If a trial did not report variability measures—reporting only standard errors, P values, or CIs—the standard deviations (SDs) of the mean change were calculated in accordance with previous methodology. 17 The interpretation of effect sizes adhered to Cohen’s scale on which <0.2 is trivial, ≥0.2 to <0.5 is small, ≥0.5 to <0.8 is moderate, and ≥0.8 is large. 18 Heterogeneity was quantified by the I2 statistic, which is independent of the number of studies in the meta-analysis. An I2 statistic of 0%, 25%, 50%, or 75% equates with no, low, moderate, or high heterogeneity, respectively. 19
As determined a priori, subgroup analyses explored any differential effects by (1) combining similar global cognitive function measures; according to (2) duration of intervention: ≤12 weeks, >12 weeks; and (3) control group: passive group, active group. Sensitivity analysis was conducted to examine the effects of combining a non–cognitively loaded physical activity with the control group. Owing to the limited number of studies included, funnel plot asymmetry was not conducted to examine publication bias. 17 Two-sided P values <.05 were considered statistically significant.
Results
Search Results
The PRISMA flow diagram depicts a summary of search results in Figure 1. The search strategy yielded 389 potentially eligible trials, which were narrowed down to 16 after removing duplicates and completing title and abstract screening. Full text-retrieval screening determined the suitability for inclusion of 6 (38%) trials including 547 participants.20-25 Supplemental Digital Content 3 (available online) outlines reasons for exclusion.
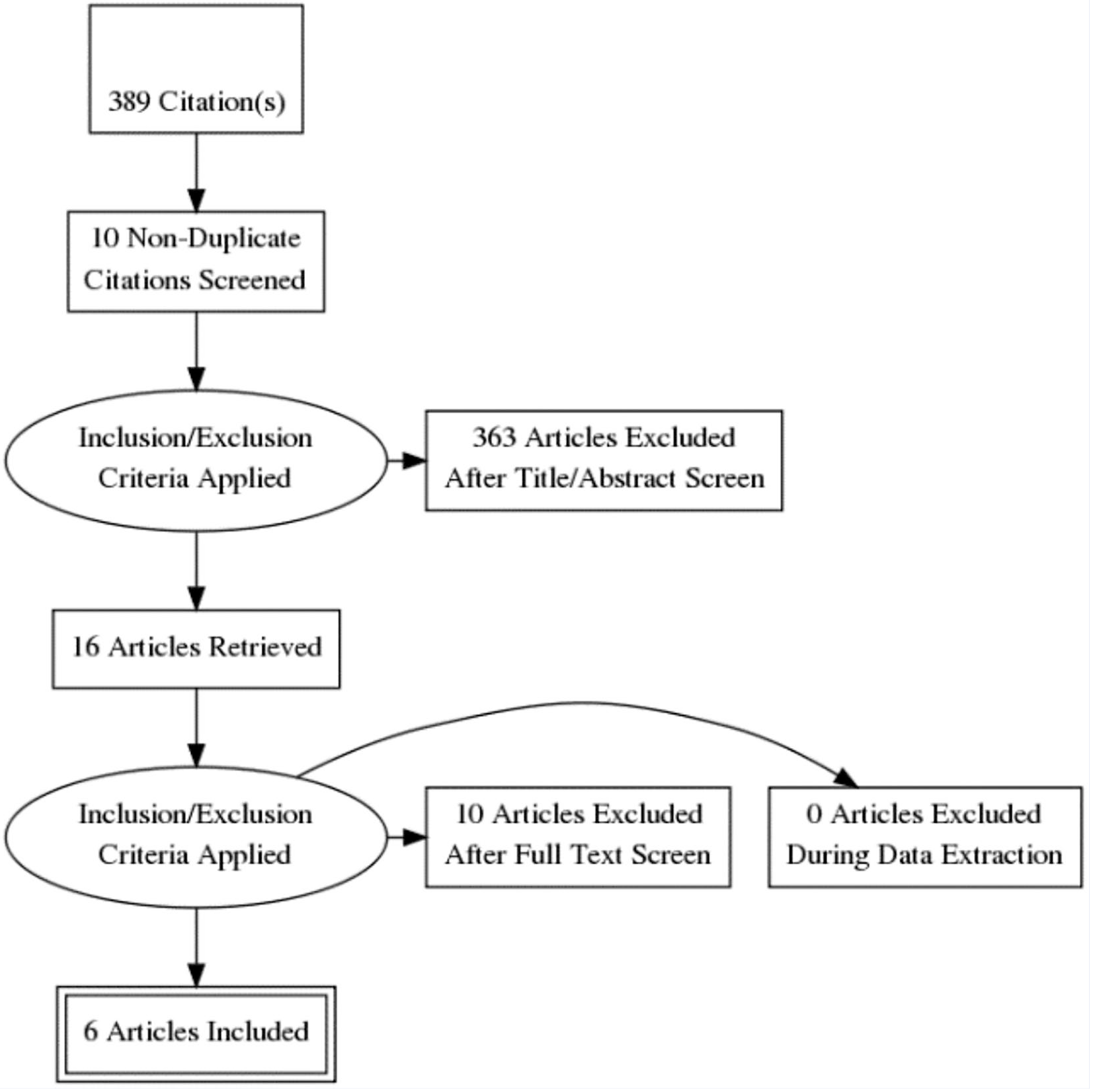
PRISMA flow diagram of literature search.
Study Quality Assessment and Risk of Bias
As cognitively loaded physical activity is a behavioral intervention, it is not possible to blind participants to allocation, 17 and therefore we judged all trials as having a high risk of bias (Figure 2). Generation of the randomization sequence and concealment of allocation were clearly stated in all trials except one. 24 One trial provided insufficient information on the blinding of participant outcome data assessments, 25 so we judged its detection bias as unclear. All trials included reported attrition. Four trials were rated at low risk of attrition bias as they had few missing data and were balanced across study arms with detailed reasons.20,23-25 Losses, although well justified, were unbalanced in one trial. The application of intention-to-treat analysis was unclear, since the analysis section indicated its application while the study flow chart did not, 22 resulting in a rating of high risk of bias. One trial incompletely described their study flow chart. 21 This chart provided insufficient rationale for the attrition of participants, as well as those (n = 15) who “did not receive allocated intervention”, although it was shown that they were allocated to the intervention arm. Within the study flow chart provided, the phrase “give reasons” was used multiple times without further explanation. We assessed this trial as having a high risk of bias. One trial 21 did not report the results of all described outcome measures. We judged it as having a high risk of bias for selective reporting.
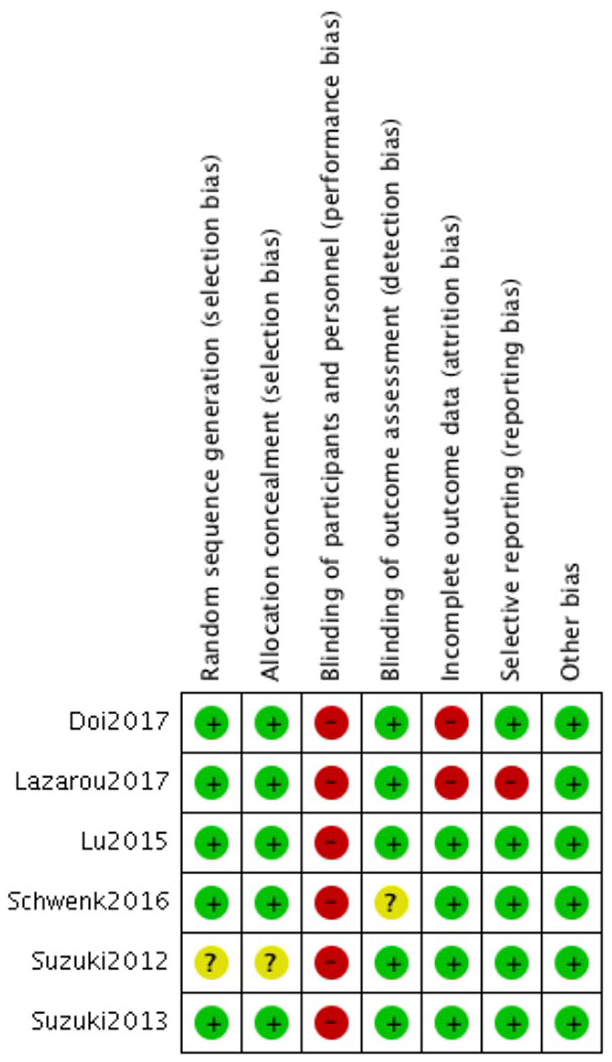
“Risk of bias” summary review authors’ judgements about each risk of bias item for each included trial: +, low risk; ?, risk uncertain; −, high risk.
Characteristics of Included Studies
Table 1 summarizes the main characteristics of each study. Half of the studies were published in Japan,22-24 with one study each from Greece, 21 the United States, 25 and China. 20 Participants were diagnosed with MCI20,22-24 or amnestic-MCI,21,23,25 classified at baseline via conventional diagnostic criteria.2,12 The average age of participants was 75.0 ± 4.1 years, and most were women. Sample sizes varied considerably (mean 85), and the size of the intervention and control groups ranged from 1225 to 8921 participants, with equal allocation to intervention and control groups occurring in only half of the RCTs.22-24
Characteristics of Included Studies in a Meta-Analysis of Studies of Cognitively Challenging Physical Activity.
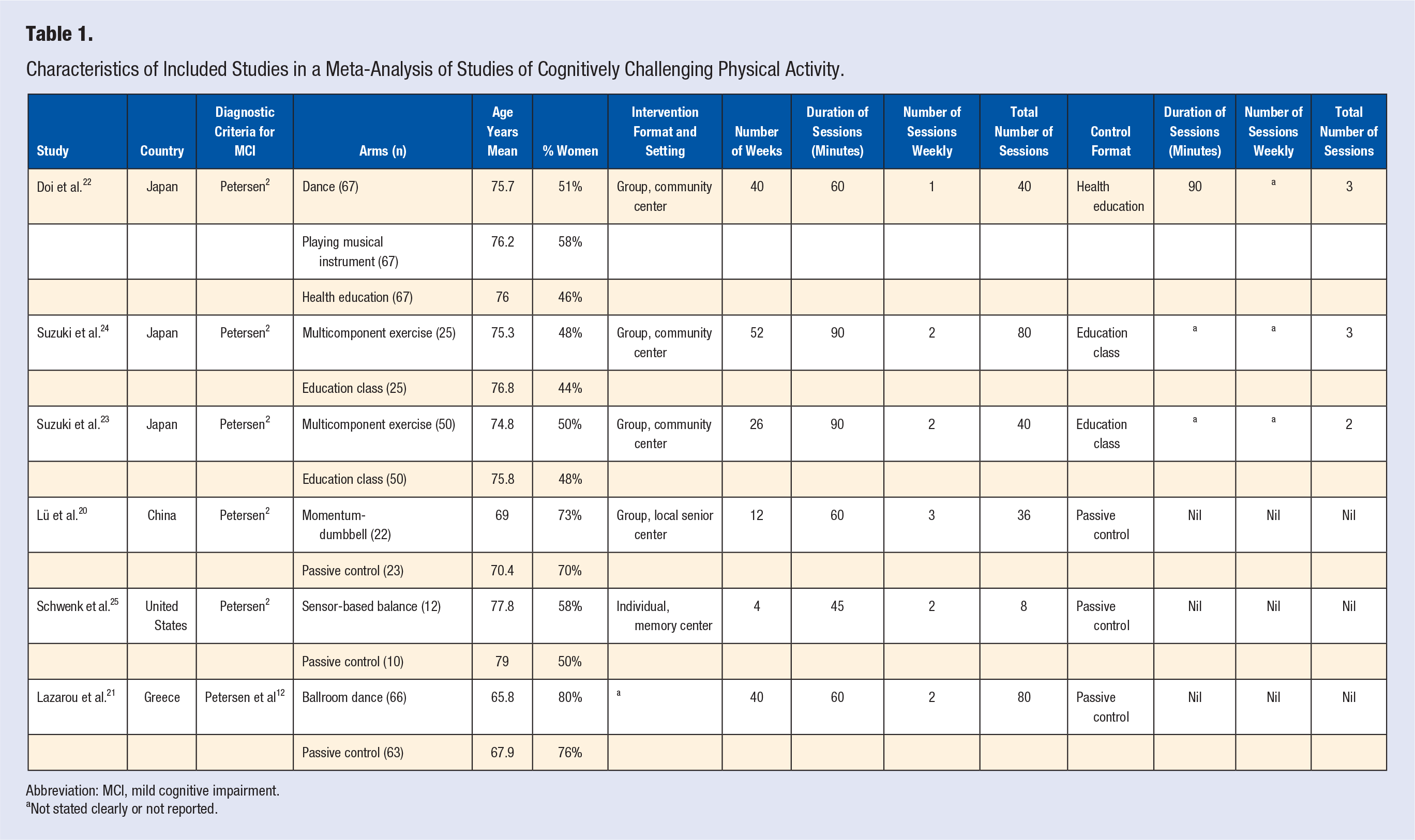
Abbreviation: MCI, mild cognitive impairment.
Not stated clearly or not reported.
The interventions were diverse in technique; 2 RCTs used dance,21,22 2 applied a simultaneous multicomponent exercise group (eg, walking and coming up with a poem),23,24 1 applied a momentum-dumbbell training program, 20 and the remaining RCT used exercise training technology. 25 The duration of the interventions ranged between 4 and 52 weeks, with an average of 30 weeks. The activities occurred usually 2 times weekly for approximately 70 minutes, the total number of sessions ranging from 425 to 80.24,26 One trial was delivered individually. 25 The other RCTs were delivered in a class or group format with the single exception 21 of a trial for which the delivery format was not described. Constant supervision was provided in all group-format trials. The individual program provided training supervision in the initial session, and in all subsequent sessions participants depended on sensor feedback while being supervised from a distance to ensure their safety. 25
The control groups were either passive control conditions20,21,25 or health and/or education classes.22-24 Measurement of global cognitive function was typically through the Mini-Mental State Examination (MMSE). One study applied the Montréal Cognitive Assessment 25 and another applied the Alzheimer’s Disease Assessment Scale. 20 Short-term, postintervention follow-up was most commonly reported but one study by Suzuki et al. 24 included 2 assessment periods.
Outcome Measures
The focus of all of the RCTs was to improve cognitive function. Meta-analyses were performed on measures of global cognitive function with results presented in Figure 3. When all studies were pooled, high heterogeneity (I2 = 85%) was detected, possibly due to diversity in trial characteristics. The analysis of all the studies combined revealed that cognitively loaded physical activity intervention did not result in significant improvement in global cognitive function compared to any type of control (Z = 0.26, P = .80; Figure 3A). Closer evaluation of the forest plot uncovered a statistically significant result 21 as well as positive trends22-24 without significant P values favoring the intervention.
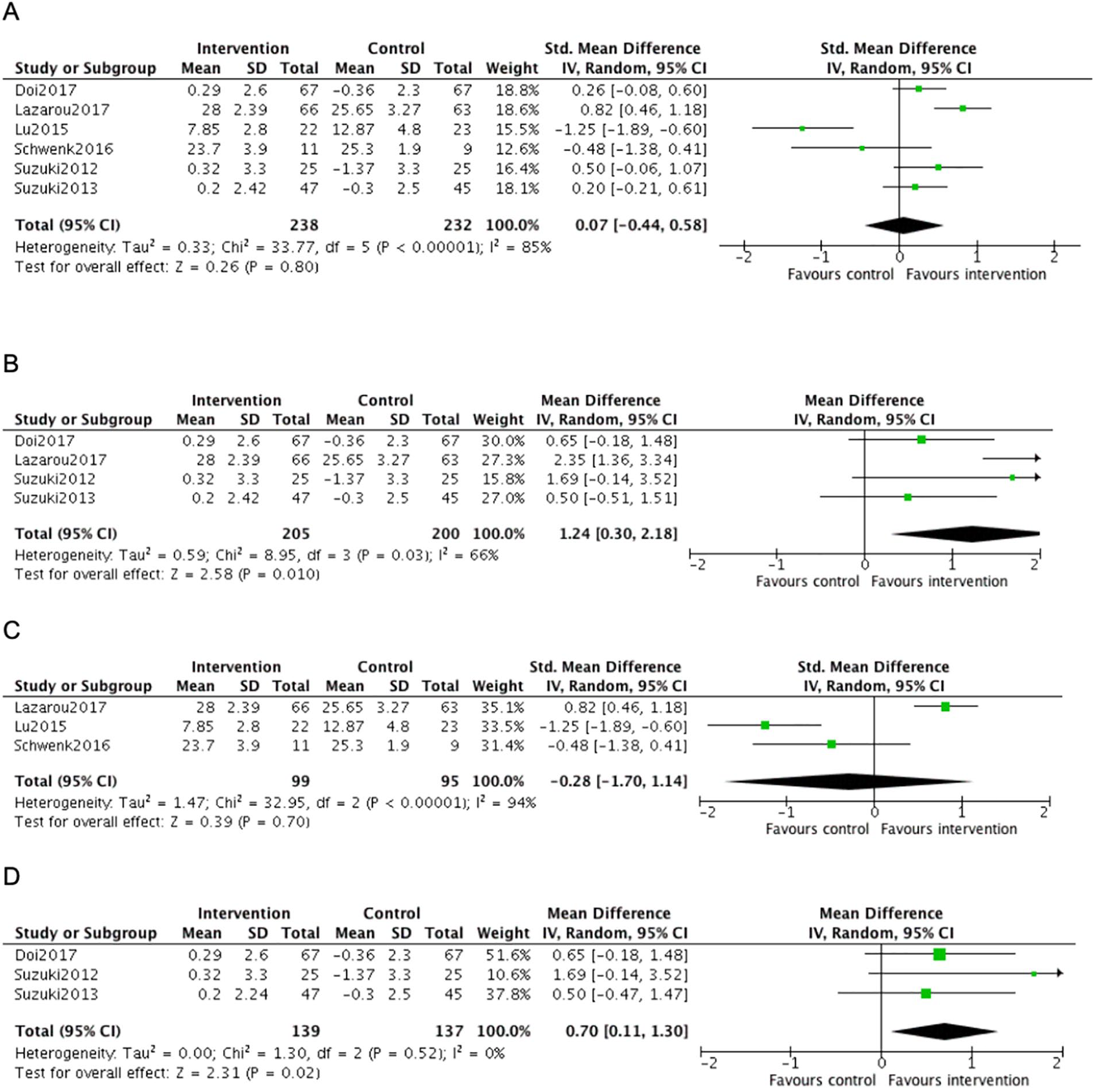
(A) Cognitively loaded physical activity (all types of global cognitive function measures); (B) Cognitively loaded physical activity (only Modified Mini-Mental State Examination global cognitive function measure); (C) Cognitively loaded physical activity (passive control); (D) Cognitively loaded physical activity (active control, all Modified Mini-Mental State Examination).
The pooled estimate for the subgroup analysis of studies that assessed global cognitive function through the MMSE, as well as studies that continued for >12 weeks, suggests that mean improvement for participants randomly allocated to the cognitively loaded physical activity was 1.24 points greater than for the control group (Z = 2.58, P = .01). The heterogeneity was moderate to high (I2 = 66%; Figure 3B) and the effect size was small (SMD 0.45, 95% CI [0.14, 0.75]; figure not displayed).
Additional subgroup analysis was conducted to determine if the various control groups had any effect on global cognitive function. Cognitively loaded physical activity was not associated with significant change compared to passive control (Z = 0.39, P = .70; Figure 3C), but there was high heterogeneity (I2 = 94%). In contrast, pooled results for cognitively loaded physical activity compared with active control suggested improvement in the global cognitive function (MMSE) score in the intervention group, compared to active controls (Z = 2.31, P = .02), without heterogeneity (I2 = 0%; Figure 3D), but with a small effect size favoring the intervention (SMD 0.29, 95% CI [0.05, 0.53]; figure not displayed).
Sensitivity Analysis
Sensitivity analyses (all trials, MMSE only trials, and active control trials) were completed to evaluate the effects of combining the control group with a non–cognitively loaded physical activity arm for Doi et al. 22 These analyses had no statistically significant impact on findings (analysis not shown).
Discussion
Summary
To our knowledge, this systematic review with a meta-analysis is the first to focus on the effect of cognitively loaded physical activity intervention on global cognitive function in older adults with MCI. The primary findings indicate no overall effect. This result may reflect heterogeneity within this analysis, indicating possible variation in the study design, specifically the cognitive-load component within trials and the use of different global cognitive function measures. In the subgroup analysis, a small but significant effect size appeared in favor of the intervention group when the same global cognitive function measure (MMSE) and >12 weeks were used or when compared to an active control. These results are comparable to the findings by Karssemeijer et al. 9 of the impact of activity intervention on MCI (SMD = 0.39, P < .05). The effect size yielded by our subanalysis was greater than that reported by Karssemeijer et al. 9 An explanation may be that only one trial included by Karssemeijer et al. 9 in their MCI analysis had a cognitively loaded physical activity intervention, the remaining trials evaluating sequential interventions. Thus, cognitively loaded physical activity may benefit global cognitive function more than sequential interventions. Further investigations are needed to explore this hypothesis.
Investigation of other potentially important factors that might influence the likelihood an intervention will induce cognitive improvement were beyond the scope of this systematic review with meta-analysis. For example, how much (frequency/intensity/duration) physical exercise is needed to induce positive cognitive change and how demanding does the cognitive-load need to be? Does more benefit accrue from one type of physical activity (ie, aerobic, resistance training, etc.) than another? Are positive effects of cognitively loaded physical activities enhanced when carried out in groups? The interventions in the 6 studies included in the meta-analysis were heterogeneous on many dimensions (ranging from dance,21,22 simultaneous multicomponent exercise,23,24 momentum-dumbbell training, 20 and exercise training technology 25 ). Classifying each intervention post hoc as aerobic versus nonaerobic is difficult, as to some extent this depends on the intensity with which they were conducted. Additionally, even within each intervention the aerobic demands may vary. For example, learning a new task increases cognitive demands, 27 which frequently reduces cardiovascular engagement through slower paced movements. As the learning process proceeds, the pace of movement increases and the aerobic demands increase. None of the studies quantified the cognitive-load of their interventions, and the duration of the interventions ranged between 4 and 52 weeks. Systematically varying some of these dimensions in future research could provide insight into the importance of each dimension in improving overall cognitive function. In this sense our conclusions are very similar to those reported by the extensive Lancet Commission on dementia. 28 It likewise indicated unclear outcomes from both cognitive training interventions for MCI and physical exercise interventions for MCI. 28 More research is needed to understand the impact of simultaneously combined cognitively loaded physical activity interventions for MCI.
Strengths and Limitations
The results of this systematic review with a meta-analysis should be interpreted with caution. The main limitations were the small number of published RCTs (n = 6) meeting our inclusion criteria and the small sample sizes. The small sample sizes might have reflected the challenging nature of cognitively loaded physical activity interventions and/or older community-dwelling adults either not wanting to acknowledge their cognitive deficits or not being aware of them. In light of these challenges, future studies need to be designed to achieve larger sample sizes. The trials included in our review also need to be considered with regard to the heterogeneity in their study designs, variation in the global cognitive function measures used, and different intervention designs, somewhat limiting the comparability of trials and findings.
Future Research
The evidence from our review warrants further examination. The included studies comprised interventions over intervals ranging from 4 to 52 weeks. Future studies need to explore the influence of study designs on the synergetic effect of novel, cognitively loaded physical activity, particularly beyond 12 weeks, to assess improvement of global cognitive function in older adults with MCI. Longer follow-up assessment periods should be considered to examine longitudinal global cognitive function change, as should including an active control arm to provide information on the isolated benefits of cognitively loaded physical activity interventions. The variability in measures of cognitive function might have limited comparability in our review, indicating a need to develop standardized tools to assess cognitive function with ease across studies. Given the current absence of a standard measure, future research could also explore methods for converting scores from different measures of global cognition to the same metric.
Conclusion
This systematic review with a meta-analysis evaluated the benefits of cognitively loaded physical activity on global cognitive function in older adults with MCI. It found no overall effect but small, statistically significant evidence from subgroup analysis that favors the intervention. Continued research of cognitively loaded physical activity in older adults with MCI is warranted.
Supplemental Material
Supplemental_1_1 – Supplemental material for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis
Supplemental material, Supplemental_1_1 for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis by Kristina Zawaly, Richard Fortier, Stephen Buetow, Lynette Tippett and Ngaire Kerse in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental_2 – Supplemental material for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis
Supplemental material, Supplemental_2 for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis by Kristina Zawaly, Richard Fortier, Stephen Buetow, Lynette Tippett and Ngaire Kerse in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental_3 – Supplemental material for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis
Supplemental material, Supplemental_3 for Exploring Cognitively Loaded Physical Activity Compared With Control to Improve Global Cognitive Function in Older Community-Dwelling Adults With Mild Cognitive Impairment: Systematic Review With Meta-Analysis by Kristina Zawaly, Richard Fortier, Stephen Buetow, Lynette Tippett and Ngaire Kerse in American Journal of Lifestyle Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: KZ was funded by a University of Auckland doctoral scholarship.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.