
Abstract
“One large nationwide population study from Sweden evaluated the cause of death of over 57,000 men with localized prostate cancer.”
Introduction
Men with prostate cancer often have undiagnosed or poorly-managed comorbidities. These can often have a greater impact on their overall quality of life and longevity compared to a prostate cancer diagnosis; however, the myriad of chronic diseases frequently seen alongside a prostate cancer diagnosis is rarely considered the domain of urologists, thus becoming a missed opportunity for patient education. Treating a patient’s prostate cancer as an isolated disease represents incomplete care for these patients because cancer development is commonly associated with various comorbidities and unhealthy lifestyles, including diet and exercise habits, which the patient would benefit from having addressed and treated.
Prior studies have demonstrated that patients with prostate cancer have a high prevalence of comorbidities.1,2 A plethora of information has been published describing the benefits that well-controlled comorbidities can have on patients’ quality of life and longevity; however, there is little information regarding the adequacy of chronic disease screening and management when initiating prostate cancer care.3-6 With treatment for prostate cancer becoming more effective, there has been a shift in treating prostate cancer more as a chronic disease rather than a terminal diagnosis. One large US population study evaluated 3.1 million new prostate cancer cases from 2001-2017 and showed that the 10-year relative survival for all patients was greater than 97%, and 100% for men with localized prostate cancer. 7 Therefore, addressing patients’ overall heath is critical as this oftentimes has a greater impact on their longevity as cardiovascular disease remains the most common cause of death in men and a significant cause of death in men with prostate cancer.8-12
This study aims to characterize diagnosed and undiagnosed chronic comorbid conditions as well as the sufficiency of their management in order to demonstrate the opportunities available to improve the overall health in men presenting with a new prostate cancer diagnosis.
Methods
After approval from the Medical College of Wisconsin Institutional Review Board, a retrospective case-controlled study was performed with patients presenting to a single institution with a new prostate cancer diagnosis between January of 2020 and March of 2022. Patients were identified using visit type and billing codes via the Clinical Practice Services Production data warehouse managed by the institution’s clinical practice services. Patients were excluded if they had received prior prostate cancer treatment, presented with metastatic disease, were enrolled in a clinical trial, or if their primary care was obtained at an outside institution without accessible electronic medical records.
Demographics including age, race, body mass index (BMI), past medical history, and comorbidities were obtained. Additional information, including vitals, lab results, and prostate cancer data was also obtained. Data was collected retrospectively from our institution’s electronic medical record by 3 members of the research team. Patients were identified to have comorbidities based on documentation and objective data (including, but not limited to, vitals and labs). For patients with no previously documented diagnosis, established guidelines were used to determine undiagnosed conditions as well as the adequacy of screening and management of the following diagnoses: diabetes mellitus (DM), hypertension (HTN), and hyperlipidemia (HLD). All patients were also assessed for the presence of metabolic syndrome.
Guidelines
• Diabetes mellitus13,14 ○ Screening: ⁃ U.S. Preventative Services Task Force (USPSTF)- adults 35-70 years old who are overweight/obese, repeating every 3 years if results are normal. ⁃ American Diabetes Association- annual screening for adults over 45 with a fasting or random plasma glucose (FPG), A1c or oral glucose intolerance test. ○ Diagnosis: ⁃ Prediabetes (A1c 5.7-6.4, FPG 100-125), Diabetes (A1c > 6.5, FPG >126). • Blood Pressure (BP)15,16 ○ Screening: USPSTF recommends annual screening for all adults over 18. ○ Diagnosis: according to the American College of Cardiology/American Heart Association (ACC/AHA), BP is consistently >130 and/or >80 mmHg. • Hyperlipidemia
17
○ Screening: USPSTF recommends screening with a lipid panel for adults 40 years or older. ○ Diagnosis: Total cholesterol >200, high-density lipoprotein (LDL) > 130. • Metabolic Syndrome
18
○ Defined by the Adult Treatment Panel III (ATP III) as at least 3 of the 5 conditions: central obesity (waist circumference: men >40 inches, women >35 inches), elevated triglycerides (>150 mg/dL or on treatment), reduced high-density lipoprotein (HDL) (<40 for men, <50 for women), HTN (BP >130/85 or on treatment), and abnormal fasting plasma glucose (>110 mg/dL or on treatment). ○ Due to the lack of measured waist circumference we elected to use a modified criteria which used a BMI cutoff of greater than 30 for a marker of central obesity.
18
A basic descriptive statistical analysis was performed on the demographic data to provide a baseline for the patient population. The data was further stratified by comorbidities and the status of comorbidities into the following categories: screened and appropriately treated, screened and inadequately treated, not appropriately screened or not diagnosed. 10-year atherosclerotic cardiovascular disease (ASCVD) risk was calculated using the American College of Cardiology’s online ASCVD Risk Estimator. 19 Two sample t-tests were performed by members of the research team to evaluate the difference between ASCVD risk among the stratified groups. A P-value of <.05 was considered to be statistically significant.
Results
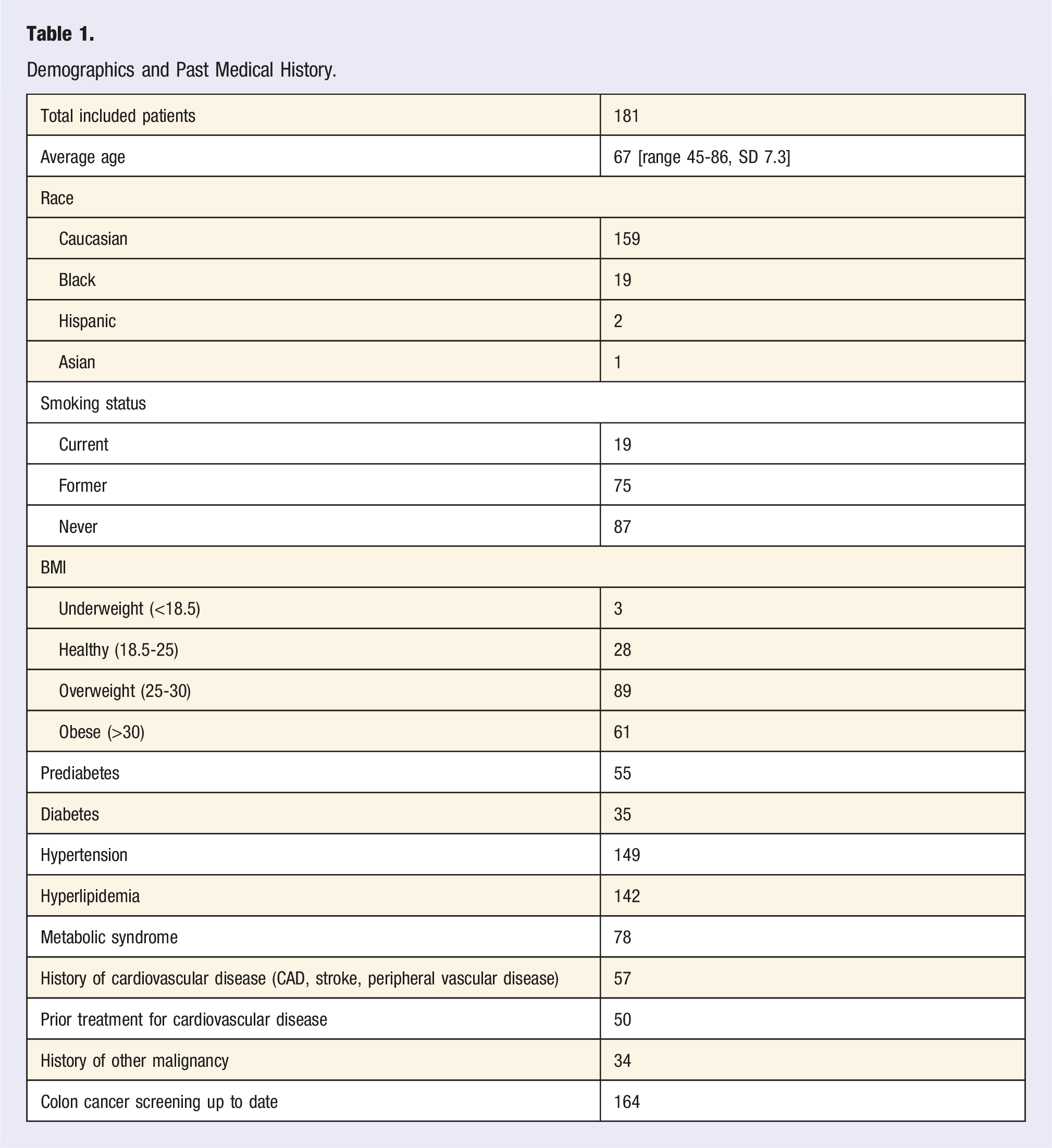
Demographics and Past Medical History.
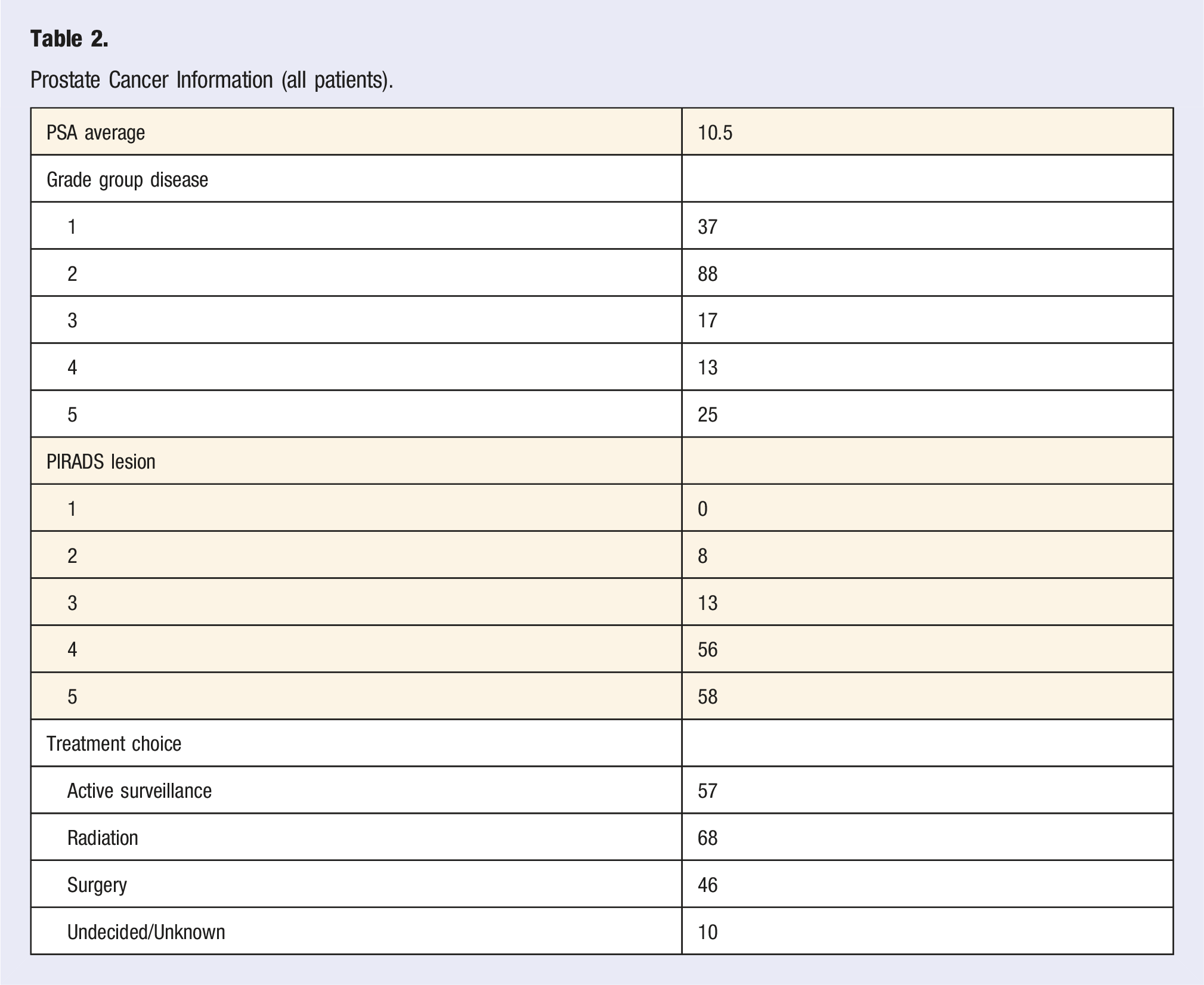
Prostate Cancer Information (all patients).
Comorbidities were then analyzed, determining that 55 (30.4%) patients were found to have prediabetes, 35 (19.3%) had DM, 149 (82.3%) had HTN, 142 (78.5%) had HLD, and 78 (43.1%) had metabolic syndrome. Only 15 patients had no diagnosis of DM, HTN or HLD meaning that the remaining 166 patients had at least 1 of these 3 diagnoses. 109 (60.2%) patients had 2 or more of the 3 diagnoses.
Adequacy of Co-Morbidity Management.
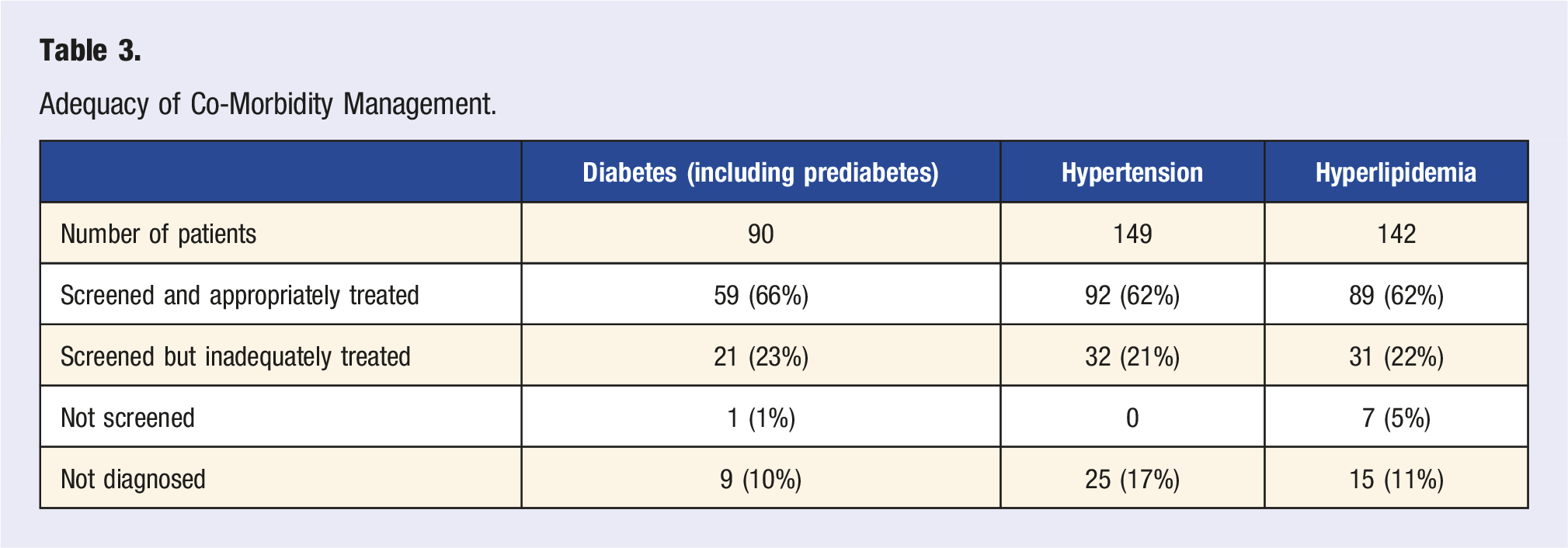
The average 10-year ASCVD risk for patients who had been screened and treated per guidelines for chronic diseases was 15.1% compared to 21.8% for those who were inadequately screened and/or treated (P < .001). The average 10-year ASCVD risk was also assessed in patients with metabolic syndrome, which was 25.6% for patients with metabolic syndrome vs 15.1% in those without metabolic syndrome (P < .001).
A thorough review of documentation in the electronic medical record also revealed that physician-patient discussions regarding lifestyle changes were only recorded in 80 (44.2%) patient charts. Additionally, a documented discussion regarding lifestyle changes by a member of the Urology department was only documented in 48 (26.5%) patient charts. Breaking this down further, one of the urology providers is certified in lifestyle medicine by the American Board of Lifestyle Medicine. Requirements for this American Board of Medical Specialties certification include additional CME and examination beyond what is normally received in urologic residency or fellowship. Patients seen by the lifestyle medicine board certified urologist were counseled about lifestyle changes 44.2% of the time, compared to 2.6% by non-lifestyle medicine board certified urologists. In summary, only 4% of lifestyle discussions were conducted by a non-lifestyle medicine board certified urologist.
Discussion
The leading cause of premature death in men with prostate cancer is cardiovascular disease. 11 Thus, it is imperative to maximize every teachable moment to help at risk men improve their health and risk factors. Often, it is a health scare like a prostate cancer diagnosis that has men wanting better health and listening to their providers. Unfortunately, the field of Men’s Health is all too often focused on sexual health, building muscle, and testosterone replacement. This misappropriation of ideas ignores and minimizes the lifestyle related, chronic disease epidemics that are at the root cause of poor sexual health and vitality. The primary reasons for the focus on the symptoms and not on the underlying problems bely much of western medicine, and the impacts are clear: our men are unhealthy and missing countless opportunities to find the health they seek. This research demonstrates both the epidemic of chronic disease in men with prostate cancer, as well as the opportunity for the urologists who treat these patients to play a larger role in their overall health.
Teachable moments can occur anytime a patient is in contact with a health care professional for their prostate cancer diagnosis. Every appointment whether it be routine follow up, pre-op or post-op can be viewed as an opportunity for patient education regarding their health. Since prostate cancer is a disease that typically requires close follow up with Urology, there is an opportunity to address health concerns and lifestyle changes that can be followed up at future appointments thus treating not only patient’s prostate cancer but also their overall health and wellness. One qualitative analysis of men with early stage prostate cancer revealed that men generally expressed a positive attitude about lifestyle change. 20 In this analysis of men from the prostate cancer lifestyle trial, participation in the trial contributed to feelings of hope, optimism and fighting spirit. 20 Another study investigated dietary changes in nearly 4000 men after a receiving a prostate cancer diagnosis without any formal dietary interventions. 21 This showed that approximately one third of men spontaneously adopted healthier diets and also consumed more “prostate-healthy” foods such as tomatoes. 21 These studies demonstrate that men are prone to having positive attitudes toward making lifestyle changes and often make changes on their own in an effort to become healthier following a prostate cancer diagnosis. Therefore, with a focused effort on taking advantage of the aforementioned “teachable moments” urology providers could make an impactful difference for patient’s by encouraging and guiding these lifestyle changes.
In this study, approximately 1 in 3 men were found to be inadequately screened, diagnosed, or treated for common chronic disease when presenting to a tertiary center after a new prostate cancer diagnosis. As a result, these men had a significantly elevated 10-year ASCVD risk compared to those who had been screened, diagnosed, and treated per guidelines. Lifestyle modifications to address these disparities were only discussed with 44.2% of patients by their PCP, and even fewer (2.6%) with non-lifestyle medicine trained urologists. If we are to make an impact on the health span of our patients, this must change.
The leading cause of death in men over 45 years old is heart disease. 8 As the average patient presenting with prostate cancer is typically over the age of 45, it is critical to access their risk of heart disease. The 10-year ASCVD risk calculator is a reliable tool to predict the risk of patients having a cardiovascular-related event. The calculated 10-year ASCVD risk then places patients into categories which include low-risk (<5%), borderline risk (5%–7.4%), intermediate risk (7.5%–19.9%), and high risk (>20%). 22 Our study results demonstrated that the average patient had an ASCVD risk of 19.3%, placing them on the verge of being high risk. Additionally, 31.5% of patients presented with a history of cardiovascular disease with 87.7% of those already requiring some form of previous intervention. When the ASCVD risk was stratified by comorbidities (DM, HTN, HLD, or metabolic syndrome), all patients crossed into the ASCVD high-risk category. Additionally, patients who had been inadequately screened and/or treated also had a significantly increased ASCVD risk of 21.8% compared to 15.1% in patients who had been screened and treated per guidelines for chronic diseases. Thus, insufficient screening or treatment alone places patients at a higher risk for cardiovascular-related events. We must learn to recognize that cardiovascular disease and prostate cancer are frequently seen together, and must maximize the opportunity to educate our patients and intervene on both of these as appropriate.
This issue of men’s overall health becomes even more important when the most common causes of death are assessed in men with prostate cancer. One large nationwide population study from Sweden evaluated the cause of death of over 57,000 men with localized prostate cancer. It demonstrated that men with low-risk prostate cancer had a 10-year prostate-specific mortality rate of .4%, 1%, and 3% when diagnosed at ages 50, 60, and 70, respectively. Additionally, it showed that prostate cancer was the third most common cause of death (18%) behind cardiovascular disease (31%) and other malignancies (30%). 11 Even when looking at men with metastatic prostate cancer, the most common non-cancer causes of death were cardiovascular diseases, chronic obstructive pulmonary disease, and cerebrovascular diseases. 12 Lastly, when accounting for the impact of comorbidities, a U.S population-based cohort study of men with prostate cancer performed by Daskivich et al. showed that, over a 14-year period, other-cause mortality rates were 24%, 33%, 46%, and 57% for men with 0, 1, 2, and 3 or more comorbid conditions, respectively. 2 This further supports the need to focus on men’s comprehensive health in the setting of a prostate cancer diagnosis, as many men with localized low risk disease are at greater risk of dying from cardiovascular disease rather than their prostate cancer. It also emphasizes the opportunity to improve the longevity of a significant number of patients presenting with prostate cancer.
The results of this study and previous studies all demonstrate the importance of urologists playing a larger role in men’s overall health care. As previously stated, non-lifestyle medicine board certified urologists only discussed lifestyle changes with 2.6% of patients. This is an important distinction to make as nearly all urologists are not trained in lifestyle medicine. This represents a substantial opportunity to improve the impact of urologists on men’s health. If all urologists took additional time to address comorbidities and risk factors of cardiovascular disease when first meeting a patient with a new prostate cancer diagnosis, it would have the potential for a profound impact of these patients’ overall health. This concept was confirmed by a recent metanalysis by the USPSTF, which showed that behavioral counseling to improve diet and increase physical activity for patients with HTN and HLD was effective in reducing cardiovascular events, BP, and LDL. 23
Further impacts of improved diet can be gathered from 2 recent studies which demonstrated the benefits of a plant-based diet for men with prostate cancer.24,25 In a prospective cohort study following over 47,000 men from 1986-2014, 6655 men were diagnosed with prostate cancer. 24 Greater overall plant-based consumption was associated with a significantly lower risk of fatal prostate cancer. 24 For men 65 years old and younger, a plant predominate diet was also associated with both a lower risk of advanced stage disease and fatal prostate cancer. 24 Liu et al. followed over 2000 men with prostate cancer and found that men with the highest degree of plant-based diets had a 52% lower risk of progression and 53% lower risk of recurrence compared to men with the lowest degree of plant-based diets. 25
Our study has clearly demonstrated the need for improved overall health care in men presenting with a prostate cancer diagnosis, and the opportunity for urologists to be at the forefront of this improved patient care. Taking time with each new prostate cancer patient to provide comprehensive men’s health care and advocating for general health improvements could have significant impacts on our patients’ overall health, beyond their prostate cancer, to improve both quality of life and longevity. This comprehensive care would ideally involve the review of patient’s past medical history, social history, medication list, recent vitals and labs aside from PSA results in order to address any area of concern that could have the potential to positively impact a patient’s quality of life.
There are several limitations of this study. First, this was a single institution study with a smaller sample size compared to larger population studies. This may impact the ability to extrapolate these results to a larger population or population of other ethnicity, as most of our patients were Caucasian. Second, the retrospective nature of this study placed limitations on data collection based on what was documented in patient charts. The lack of or inaccuracy of documentation has the potential for impacting the results, as not every provider may have documented lifestyle modification conversations or all diagnoses correctly. Third, the standard criteria for metabolic syndrome was unable to be used for our study due to the lack of waist circumference measurements for these patients. Therefore, a surrogate marker for waist circumference was used, which was BMI. While this is not the standardized best-known guideline, a study by Kobo et al in 2019 determined that a BMI below 30 provided a negative predictive value of 91% for metabolic syndrome; therefore, this substitution was determined to be efficacious. 18
Conclusion
In this series, the majority of patients (91.7%) presented with at least 1 comorbidity, and only 15.5% of patients were considered a healthy weight according to BMI. Approximately one third (34%–38%) of patients presented with poorly-managed or undiagnosed comorbidities at the time of their new prostate cancer diagnosis. As a result, these patients had a significantly increased 10-year ASCVD risk from 15.1% to 21.8%. Similarly, when accounting for obesity and comorbidities with metabolic syndrome, the 10-year ASCVD risk further increased from 15.1% to 25.6%. The overall high rates of comorbidities, obesity and, specifically, undermanaged chronic disease, represents a significant unmet health care need and an opportunity for urologists to champion men’s health in new prostate cancer patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.