
Abstract
About 16 million adults present with chronic back pain, the sixth most costly condition in the United States (US). Estimates suggest that about 60% of initial back surgeries have a successful outcome; however, many don’t, leaving over 80,000 failed back surgeries per year. Failed Back Surgery Syndrome (FBSS) is defined by the International Association for the Study of Pain as back pain, with or without radiating pain, located in the lower limbs, of unknown origin, which persists or begins after surgical procedures are performed to treat lumbar disc herniations. Psychiatric comorbidities and psychosocial factors have been associated with patients presenting with this syndrome. A retrospective cross-sectional study was performed to identify the prevalence of FBSS in a population of patients during the period of January 2019-December 2020 across Hospital Corporation of America (HCA) Healthcare in the US. With a sample of 28,426 patients who underwent back surgery only 8% had FBSS. Those with FBSS (N = 2434) were mainly females (54.27%) with a mood disorder (61.18%), P-value <.0001. Among those with FBSS, there was a statistically significant relationship between mood disorder and smoking (57.37%) and obesity (54.61%) compared to non-smokers and non-obese. Lifestyle interventions may ameliorate disabling symptoms and improve the well-being of this population.
“Identifying a correlation between mood disorders and FBSS is important as it is a poor prognostic indicator that affects the outcome of surgery.”
Background
About 16 million adults present with persistent or chronic back pain making it the sixth most costly condition in the US. 1 Estimates suggest that 60% or more of initial back surgeries have a successful outcome; however, many don’t, indicating there may be over 80,000 failed back surgeries per year. 2 Post-laminectomy syndrome, or Failed Back Surgery Syndrome (FBSS), is defined by the International Association for the Study of Pain as back pain, with or without referred or radiating pain, that is located mainly in the lower limbs, is of unknown origin and persists or begins after surgical procedures are performed to treat lumbar disc herniations. 3 This syndrome is reported to affect between 10 to 40% of patients following back surgery, but estimating the incidence is difficult given the heterogenous etiology.4,5 This syndrome is challenging to treat leading to lower quality of life for the patient, creating more disability, maladaptive opioid use, among others. 6 Failed back surgery syndrome has not been thoroughly studied; however, a study by Slipman et al suggests there was approximately an equal distribution between the incidences of nonsurgical and surgical diagnoses; 44.4% had nonsurgical diagnoses and 55.6% had surgical diagnoses. Psychiatric comorbidities and psychosocial factors have been found to be an influencing factor associated with development of FBSS.7,8 According to the diagnostic interview data from National Comorbidity Survey Replication, the prevalence of any mood disorder among US adults aged 18 or older over the past year was 9.7%. 9 In a study by Batista et al 55.6% of patients were found to have moderate or severe anxiety and 50% were classified as having moderate or severe depression.10,11 A survey done by Long et al found that 67 of 78 patients with FBSS suffered from depression, most of them experiencing an onset of depressive symptoms following the initial onset of pain. Other studies done in Korea found that there is a relationship between pain intensity, anxiety, and functional disability in patients with lumbar disk herniations. 12
Methods
Subjects
In this study we analyzed 28,426 patients ages 18-80
Design and Methodology
A retrospective cross-sectional study was performed to identify the prevalence of failed back surgeries in a population of patients with persistent back pain after back surgery during the period of January 2019-December 2020 in all HCA Healthcare hospitals in the US. Patients with FBSS were identified as defined by an emergency department visit or hospital admission for back pain between 90-450 days after surgery. The exclusion criteria for the study were: patients with FBSS diagnosis on first admission, patients who expired during first admission, patients with infective or inflammatory conditions, malignancy, osteoporosis, Paget’s disease, and patients with the symptoms listed in the appendix. Refer to the summary of exclusion in the Figure 1 for more details.
The prevalence of mood disorders as defined by ICD-10 codes or the use of medications listed in the appendix was identified in FBSS patients. Covariates studied included sex, race, smoking, obesity, and Elixhauser comorbidity index and were compared between the population with and without FBSS. The prevalence of mood disorder in patients with FBSS was also compared between men and women, smokers and non-smokers, and obese and non-obese.
Statistical Analysis
Bivariate analysis including chi-square and t-tests was performed. A P-value <.05 was considered statistically significant. Data cleaning and statistical analysis were performed in SAS 9.4 (Cary, NC).
Results
Characteristics of Patients Who Underwent Back Surgery from 2019-2020 Across All HCA Hospitals in the United States (N = 28,426) by Presence of Failed Back Surgery Syndrome during 90-450 day follow-up period.
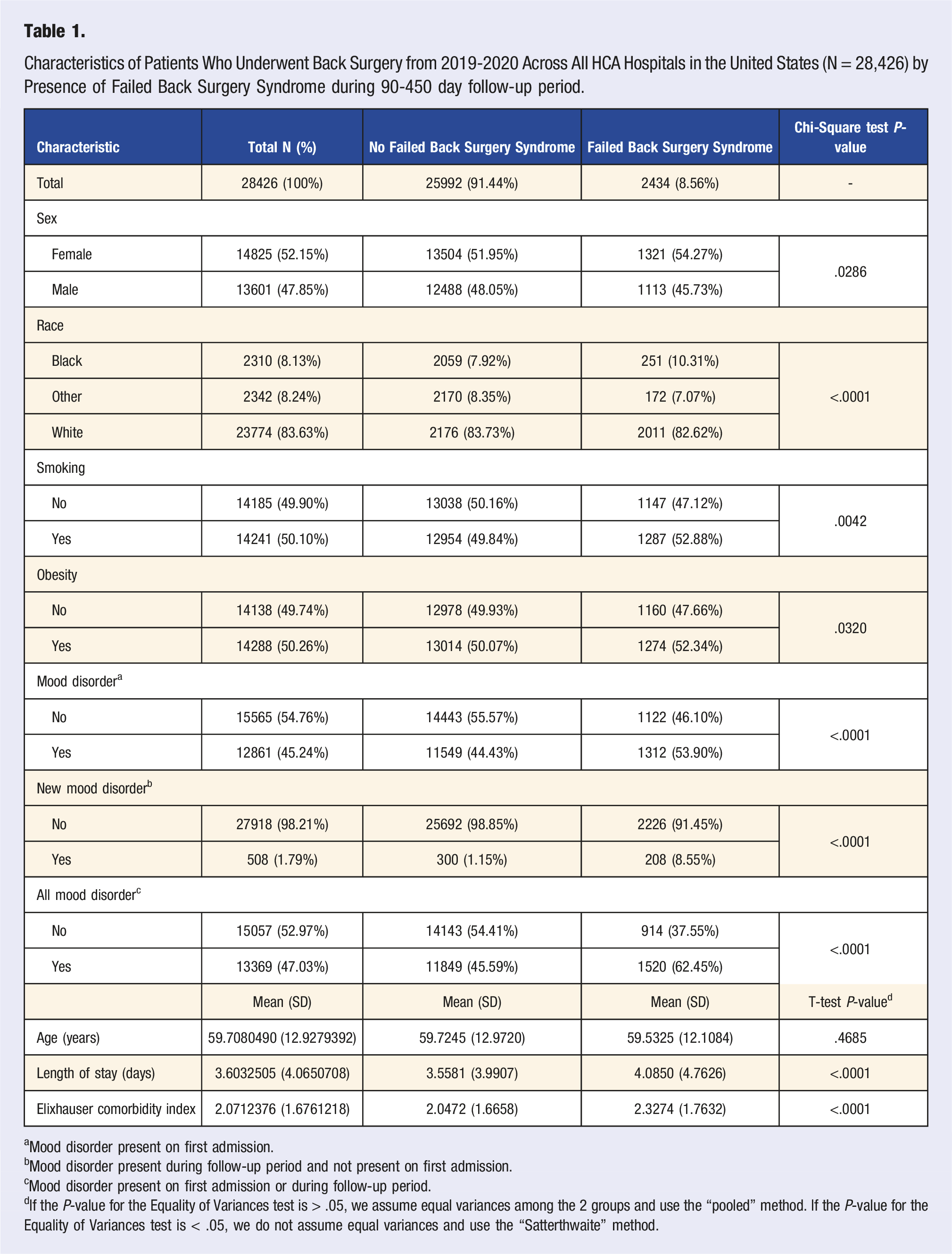
aMood disorder present on first admission.
bMood disorder present during follow-up period and not present on first admission.
cMood disorder present on first admission or during follow-up period.
dIf the P-value for the Equality of Variances test is > .05, we assume equal variances among the 2 groups and use the “pooled” method. If the P-value for the Equality of Variances test is < .05, we do not assume equal variances and use the “Satterthwaite” method.
Characteristics of Patients Who Underwent Back Surgery from 2019-2020 and had Failed Back Surgery Syndrome during 90-450 day follow-up period (N = 2434) by Presence of Mood Disorder. a
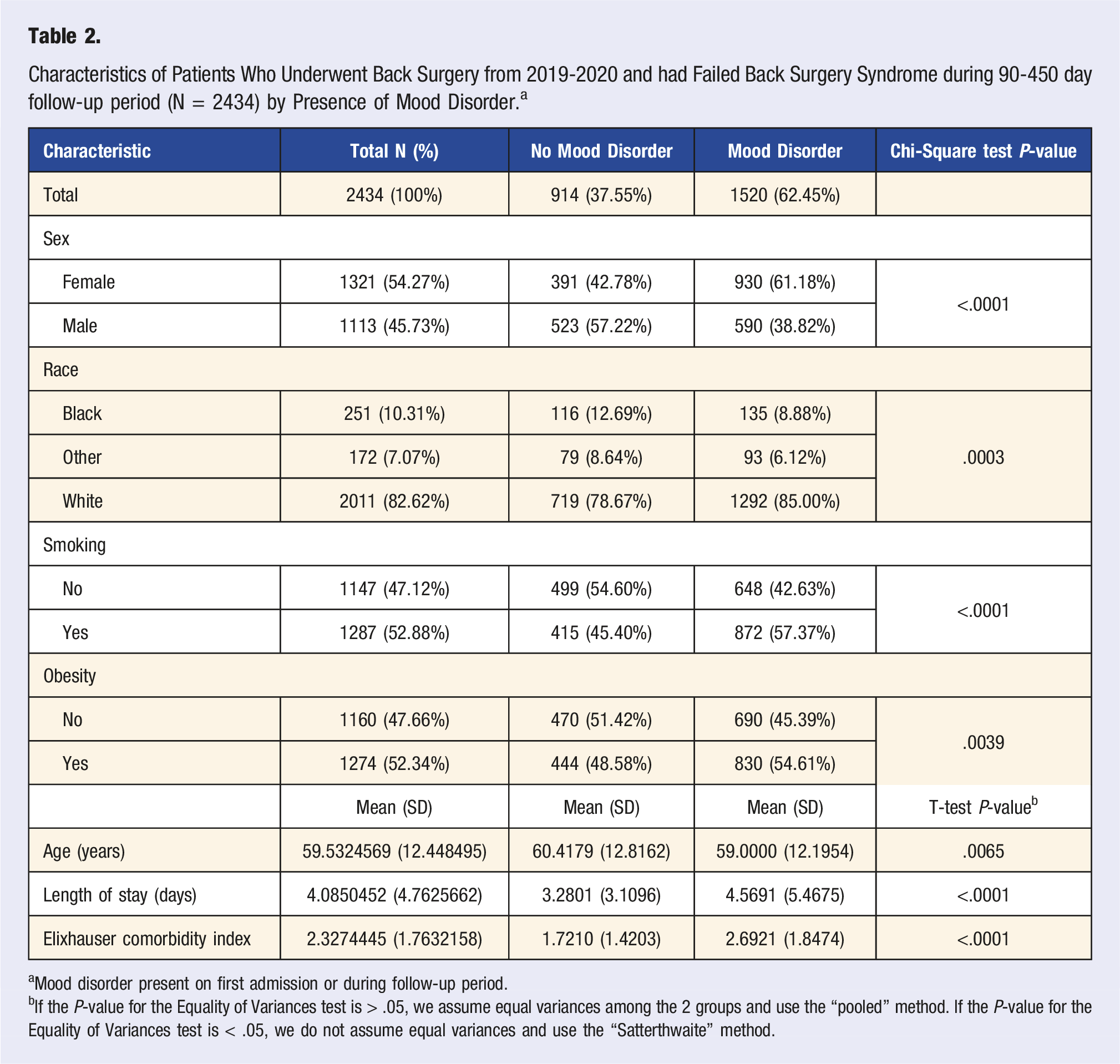
aMood disorder present on first admission or during follow-up period.
bIf the P-value for the Equality of Variances test is > .05, we assume equal variances among the 2 groups and use the “pooled” method. If the P-value for the Equality of Variances test is < .05, we do not assume equal variances and use the “Satterthwaite” method.
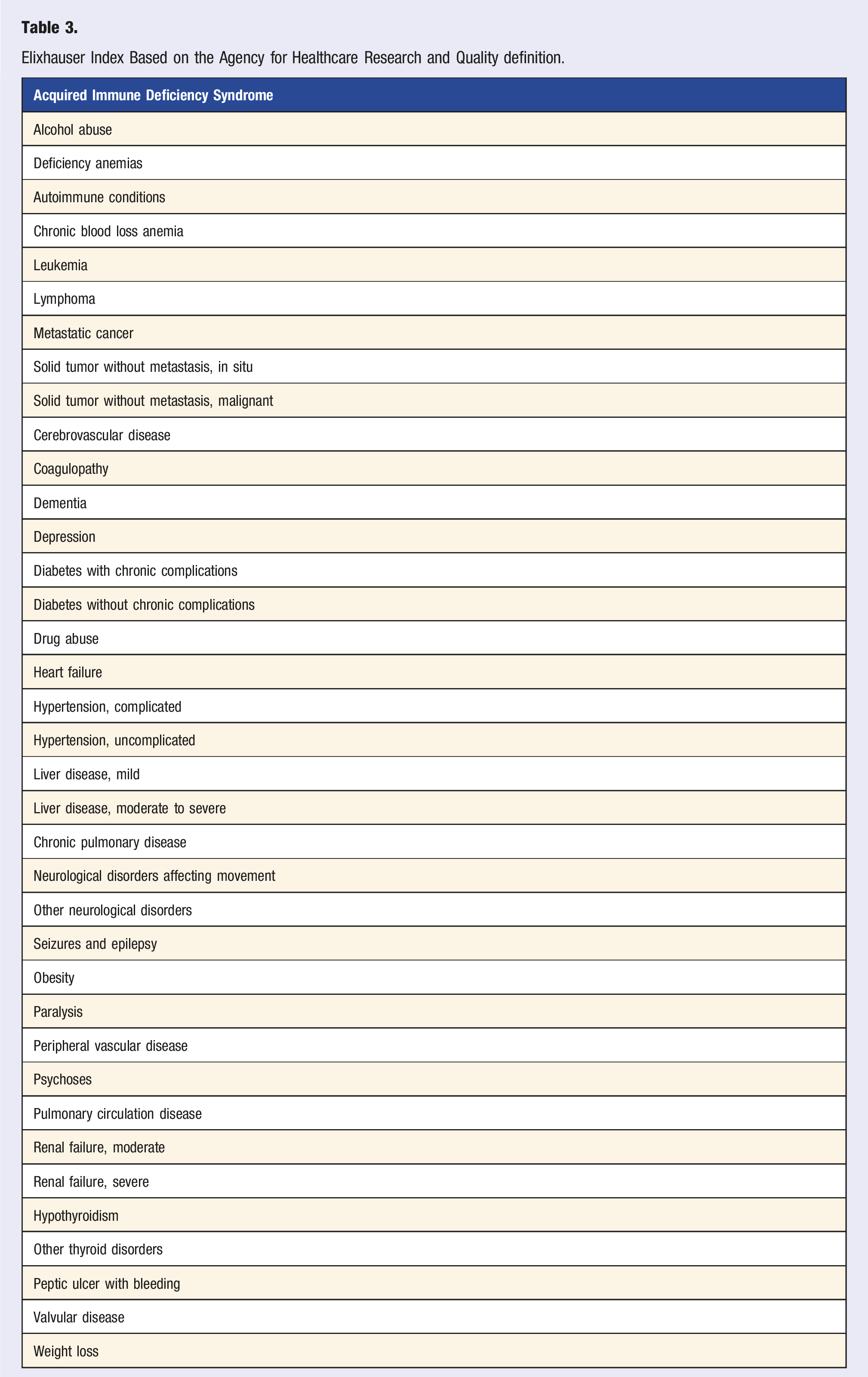
Elixhauser Index Based on the Agency for Healthcare Research and Quality definition.
Patients who had FBSS and mood disorder during the 90-450 day follow-up period (N = 2434) were mainly whites (85.00%), followed by blacks (8.88%), and other races (6.12%) with a P-value of .0003. There was also statistical difference in patients who were smokers (57.37%) compared to non-smokers (42.63%) with a P-value of <.0001 and obese (54.61%) compared to non-obese patients (45.39%) with a P-value of .0039. Patients with mood disorders had a higher length of stay (4.57 days), compared to those without mood disorders (3.28 days) with a P-value of <.0001. They had a higher Elixhauser comorbidity index (2.6921), than those without mood disorder (1.72) with a P-value of <.001 (Table 3). The average age was 59 years compared to those without mood disorders who had an average age of 60.42 years with a P-value of .0065. Summary of exclusions.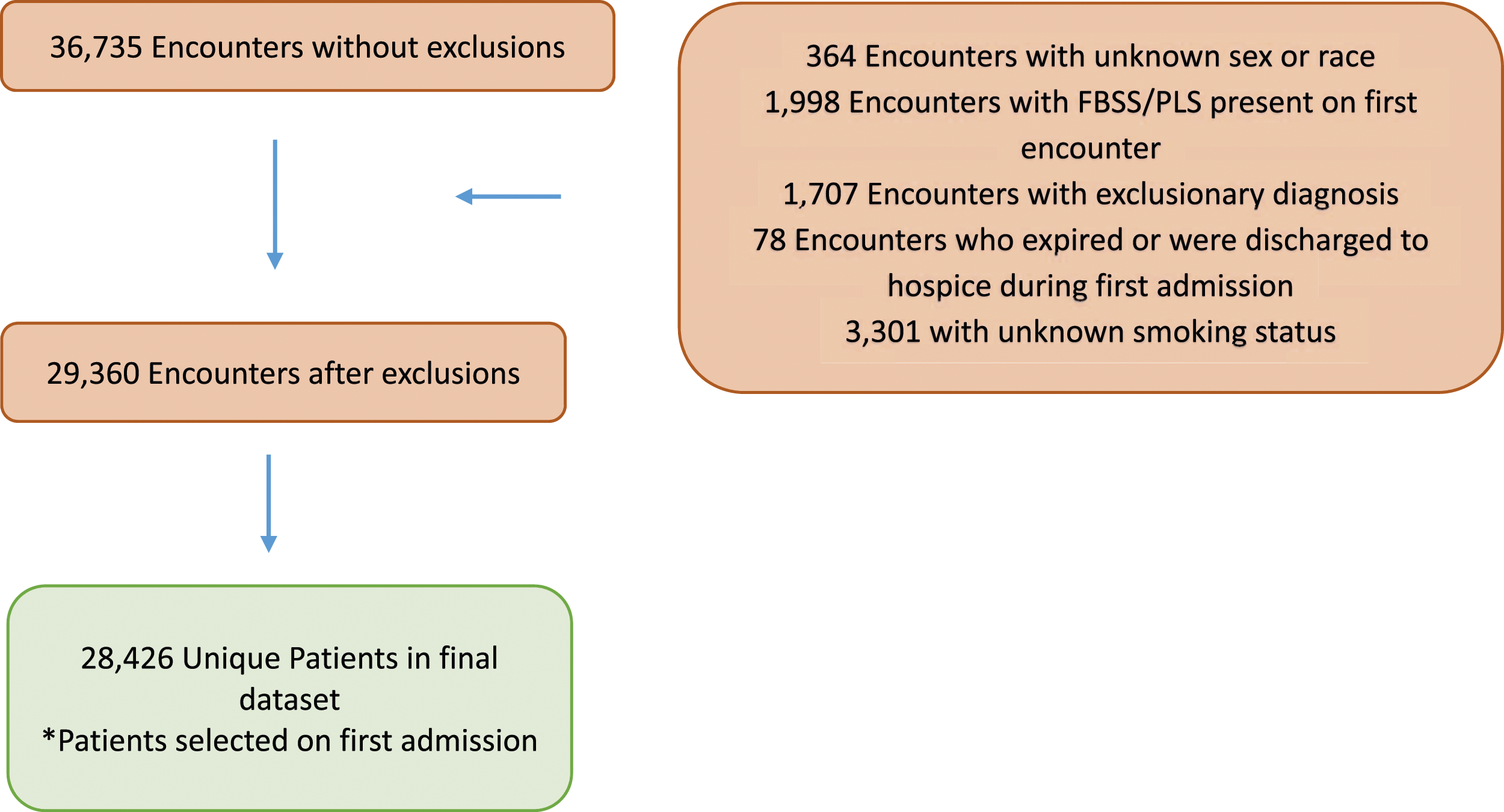
Discussion
Failed Back Surgery Syndrome was not common in patients receiving back surgery at HCA Healthcare hospitals during the period of January 1st, 2019 to December 31st, 2020. Although it has been estimated to have a global incidence of 9.4% it creates more disabilities than other conditions. 13 Rehabilitative medicine is poorly developed, focusing mainly on pain relief, thus patients with FBSS live with the constant anxiety of relapse and steady deterioration of neurological symptoms. 14 Several indicators have been identified in prior studies that lead to FBBS such as litigation and workers’ compensation, smoking, obesity, and preoperative psychiatric disorders as the etiologies of back pain. 15 Sebaaly et al describe psychosocial factors, like anxiety and depression, as preoperative factors to FBSS. Also, inaccurate diagnosis has been found in 58% of FBSS per Burton et al, which may affect the prognosis for the psychiatric population. Identifying a correlation between mood disorders and FBSS is important as it is a poor prognostic indicator that affects the outcome of surgery. A study published in 2019 reported, that patients with underlying psychological disease have higher rates of delirium, readmission, longer hospital stays, and higher rates of non-routine discharge following spine surgery. They also have higher rates of chronic post-operative narcotic use and may experience worse surgical outcomes thus identification and treatment of these disorders prior to surgery may significantly improve surgical outcomes. 16
There is also statistical significance in the presence of risk factors and comorbidities affecting outcomes such as smoking and obesity. Obesity is related to back pain due to its risk of disk degeneration and sciatica. 17 Jackson et al describe other studies and meta-analysis reviewing imaging on obese patients and how there is a significantly higher incidence of finding disk degeneration in these patients. This leads to pathology and possible requirement of surgery. Smoking contributes to operative risk in many ways. It is known to affect the vasculature, therefore, impairs spinal tissue vascular supply inducing hypoxia and inflammation and accelerating spondylosis. It affects the disc, cartilage, synovium, bone, and blood vessels. Surgeries become a risk as there can be delayed wound healing, failed fusion, surgical site infections, and chronic spinal pain. 18
Lifestyle medicine interventions can be applied to these populations to improve their chronic back pain avoiding future surgeries which could potentially fail. Studies have been done looking into the implementation of short-term yoga programs for patients with chronic low back pain and reduction of pain, use of analgesics, anxiety, depression, and improvement in spinal mobility. 18 Cognitive behavioral techniques and lumbar stabilization treatments have been used and resulted in positive outcomes in patients with chronic low back pain. 19
Limitations of the Study
Patients who presented after 450 days were not included in the study. Patients who visited a different hospital over the 90 day period with complaints of back pain would be missed on the FBSS group. The study did not directly look at an important population of patients that can be susceptible to FBSS such as patients with spondyloarthropathies or axial psoriatic arthritis. Differentiating inflammatory back pain from mechanical back pain is of critical importance to be able to choose the most appropriate diagnostic work-up for a timely and accurate diagnosis in patients suffering from low back pain in order to avoid unnecessary interventions. If patients are evaluated and treated appropriately other concomitant conditions leading to back pain, for example, herniated discs, may be followed and controlled to prevent a surgery that may fail in the future.
Possible bias includes information bias as some data may be missing among patients, generalizability by evaluating only a specific population, sampling bias, and confounding variables that may relate to persistent back pain. There may be other confounding variables limiting a conclusion of cause and effect.
Future suggestions include obtaining information regarding post-operative rehabilitation and length of treatment and post-operative pain medication consumption. 20
Conclusion
Failed Back Surgery Syndrome is not common; however, those who suffer from it have poor quality of life. Those with comorbidities like mood disorders, smoking, and obesity may benefit from lifestyle medicine interventions to ameliorate disabling symptoms and improve their well-being. Rehabilitative medicine should include a multidisciplinary approach looking at different aspects of the patient and not only focusing on pain control. The goal for these patients is that they can reincorporate back into the community, work, and social life.
No causality between mood disorder and FBSS can be obtained from the study as patients presenting with back pain complaints to the ED may not have reported their underlying mood during their first visit and would not be present as a diagnosis code in the medical record. However, the correlation exists, and interventions to modulate these cognitive factors are important when managing this population.
Future studies should be done to identify the prevalence of patients with underdiagnosed inflammatory back pain who will benefit from appropriate treatment before failing a back surgery.
Footnotes
Acknowledgments
We want to thank Natalie Hurlock, Research Manager, and Dr Nayda Parisio-Poldiak, Division Research Director, and Desr’ee Groover for their assistance in the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
Inclusion: Patients who underwent back surgery defined by: M43.20 (Fusion of spine), M43.26 (Fusion of spine, lumbar), M43.25 (Fusion of spine thoracolumbar), M43.28 (Fusion of spine sacrococcygeal), M43.27 (Fusion of spine lumbosacral), 00NY0ZZ (Release lumbar spinal cord, open approach), Other fusion of vertebral joint procedure codes: 0SG00AJ, 0SG03AJ, 0SG04AJ, 0SGl0AJ, 0SG13AJ, 0SG14AJ, 0SG0071, 0SG00Jl, 0SG00 Kl, 0SG0371, 0SG03Jl, 0SG0471, 0SG04J1, 0SG04 Kl, 0SG1071, 0SG107 J, 0SGl0Jl, 0SGl0Kl, 0SG1371, 0SG13J1, 0SG13 Kl, 0SG1471, 0SG14Jl, 0SG14 Kl, 0SG30AJ, 0SG3071. Excision of lumbar vertebral disc, open approach (0SB20ZZ, 0SB40ZZ). The following CPT Codes: 22630, 22632, 22854, 22614, 22634, 22612, 22633, 22899, 22586, 22846, 22845, 22841.
Exclusion: Patients with following symptoms: saddle anesthesia or bowel/bladder incontinence indicative of cauda equina syndrome: MG83.4 (Cauda equina syndrome), S34.3 (Injury of cauda equina), N31 (Neuromuscular dysfunction of bladder), N39.498 (Other specified urinary incontinence), R15 (fecal incontinence), N39.42 (incontinence without sensory awareness), R15.9 (full incontinence of feces), N39.45 (continuous leakage), spinal cord injury S14.109 A. Patients with malignancy in bones, primary or metastasis: C40.9 (Malignant neoplasm of unspecified bones and articular cartilage of limb), C40.20 (Malignant neoplasm of long bones of unspecified lower limb), C41.4 (Malignant neoplasm of pelvic bones, sacrum, and coccyx), C79.51 (Secondary malignant neoplasm of bone), C41.2 (Malignant neoplasm of vertebral column), D48 (Neoplasm of uncertain behavior of bone and articular cartilage), M48.4 (Fatigue fracture of vertebra). D49.2 (Neoplasm of unspecified behavior of bone, soft tissue, and skin), M48.5 (Collapsed vertebrae), M49.89 (Neoplasm of unspecified behavior of other specific sites), M84.58 (Pathological fracture in neoplastic disease, other specified site, initial encounter for fracture) Patients with vertebral infections: M00.08 (Staphylococcal arthritis of vertebrae), M00.18 (Pneumococcal arthritis of vertebrae), M01.X8 (Direct infection of vertebrae in infectious and parasitic diseases classified elsewhere), T84.63 (Infection and inflammatory reaction due to internal fixation device of spine, initial encounter). Patients with postimmunization arthropathy: M02.28. Patients with rheumatoid bursitis: M06.28. Patients with Paget’s disease of the bone. M88.9 (osteitis deformans of unspecified bone), M88.89 (Osteitis deformans of multiple sites), M88.1 (Osteitis deformans of vertebrae). Patients with osteoporosis: Pertinent codes: M81.6 (Localized osteoporosis), M81.0 (Age-related osteoporosis without current pathological fracture), M81.8 (Other osteoporosis without current pathological fracture), M80.08 (Age-related osteoporosis with current pathological fracture, vertebra, initial encounter), M80.80 (Other osteoporosis with current pathological fracture, unspecified site).
Mood disorder—initial and new mood disorder during the follow-up period. ICD-10 codes F25 (Schizoaffective Disorder), F31 (Bipolar disorder), F32 (Depressive episode), F33 (Major depressive disorder), F34 (Persistent mood/affective disorder), F41.1 (Generalized anxiety disorder), F41.8 (Other specified anxiety disorder), F41.9 (Anxiety disorder) or self-reported home medications or medications received during hospital admission: Selective serotonin reuptake inhibitors (SSRI) (Citalopram-Celexa, Escitalopram-Lexapro, Fluoxetine-Prozac, Paroxetine-Paxil, Sertraline-Zoloft, Fluvoxamine-Luvox), Serotonin Norepinephrine reuptake inhibitors (SNRI) (Venlafaxine-Effexor, Desvenlafaxine-Pristiq, Duloxetine-Cymbalta, Levomilnacipran-Fetzima), Atypical antidepressants (Bupropion-Wellbutrin, Mirtazapine-Remeron, Nefazodone, Trazodone-Desyrel), Serotonin dopamine activity modulator (Aripripazole-Abilify), Tricyclic antidepressants (TCA) (Amitriptyline-Elavil, Clomipramine-Anafranil, Desipramine-Norpramin, Doxepin-Sinequan, lmipramine-Tofranil, Nortriptyline-Pamelor, Protriptylin-Vivactil, Trimipramine-Surmontil), Monoamine oxidase inhibitors (MAO) (isocarboxazid-Marplan, Phenelzine-Nardil, Selegiline-Emsam, Tranylcypromine-Parnate), Atypical antipsychotic (Lithium, Clozapine-Clozaril, Ziprasidone-Geodon, Paliperidone-lnvega, Risperidone-Risperdal, Quetiapine-Seroquel, Olanzapine-Zyprexa, Cariprazine-Vraylar.