
Abstract
Produce prescription (PRx) programs improve access to fresh fruits and vegetables. However, many programs lack culinary focused nutrition education or behavioral support to promote sustainable lifestyle changes. The pilot Fresh Start PRx (FSPRx) program was a 20-week PRx program. The purpose of this study was to examine the impact of the FSPRx program on food literacy, lifestyle behaviors, and health outcomes (e.g., glycemic control) with rural, uninsured patients with type-2 diabetes. Adult patients (n = 56) diagnosed with type-2 diabetes enrolled in the pilot FSPRx program. The FSPRx program consisted of telephone-based health coaching, group educational sessions, and a PRx. Patients completed diet quality, food literacy, and physical activity questionnaires and had blood drawn for hemoglobin A1C (HbA1C) pre- and post-intervention. Twenty-seven patients had a significant improvement in both fruit and vegetable consumption. Nineteen patients had an increase in total food literacy scores, budgeting skills, meal planning and prepping, nutrition resourcefulness, and physical activity confidence after the intervention. Patients had an average HbA1C decline of .79% (n = 27, P = .01
Keywords
“Significant improvements in fruit and vegetable consumption were observed among FSPRx participants.”
Introduction
Chronic diseases- such as heart disease, cancer, and diabetes are the leading causes of death and disability in the United States and account for $4.1 trillion in annual health care expenditures. 1 Type-2 diabetes is one of the most prevalent and costly of these chronic conditions, affecting 1 in 10 Americans and over $327 billion is spent annually to treat this condition. 2 Prevention and management of type-2 diabetes and chronic diseases requires addressing underlying lifestyle risk factors such as poor nutrition and physical activity as these health behaviors contribute to 30% of an individual’s health outcomes. 3
Poor diet quality including the high consumption of starchy foods, saturated fats, and low fruit/vegetable consumption impedes optimal management of diabetes and other chronic diseases and is a contributing factor in over 50% of deaths globally. 4 In contrast, high nutrient intake through fruit and vegetable consumption in particular, has also been found to moderate the risk of developing chronic diseases. 5 Dietary patterns with a diverse array of fruits, vegetables, whole grains, lean protein, and healthful fats, for example, omega-3 fatty acids have demonstrated effectiveness in improving the management of common chronic diseases (e.g., diabetes, hypertension).5-11 Despite the benefits of fruits and vegetables, only 1 in 10 Americans are currently meeting the recommendations for 2 servings of fruit and 3 servings of vegetables per day. 12
One approach to support improved dietary quality and fruit and vegetable consumption is through the provision of a produce prescription (PRx), which is defined as “a medical treatment or preventative service for eligible patients due to diet-related health risks or conditions, food insecurity, or other documented challenges in access to nutritious foods, and are referred by a health care provider or health insurance plan.” 13 Produce prescription programs directly promote the consumption of fruits and vegetables by providing vouchers that can be redeemed for fresh produce. These programs have shown promise in increasing fruit and vegetable consumption and common cardiometabolic outcomes, in particular glycemic control.14-18
While PRx programs improve access to fresh fruits and vegetables, many programs lack culinary focused nutrition education or behavioral support to bolster and promote healthy, sustainable, food behavior changes. Nutrition education-focusing on food literacy—the knowledge and skills to plan, choose, and prepare a healthy meal is essential to support integration of fresh produce provided by a PRx into the diet. 19 Furthermore, food literacy is predictive of overall diet quality; therefore, education that supports food literacy offers additional nutrition benefits alongside the provision of a PRx.20,21 Food literacy and culinary focused nutrition education provided in a group setting can allow PRx participants to build their knowledge and skills.22,23 This offers the potential for cooking demonstrations and taste testing opportunities as well. Taste testing has been shown to improve the integration of new foods, especially new vegetables, into the diet. 24 Therefore, group class settings offer the potential to expose patients to new food and allow for hands-on skill building to complement the PRx.
Although group class setting may be beneficial for patients, they do not allow for individualized support, counseling, or goal setting around nutrition (e.g., fruit and vegetable consumption goals) which could further bolster a PRx in improving nutrition and health. Health coaching, a patient centered-approach, has been found to be successful at improving dietary behaviors and health through individualized goal setting.25,26 Integration of both individualized behavioral support and group education offer the potential for synergy between these components to build PRx participants capacity to sustain positive dietary behaviors. Multi-layered PRx programs that strategically integrate behavioral and educational support and resources are limited, however, warranted. Such comprehensive programming may be especially critical to implement and evaluate within under-resourced communities most at risk for nutrition and lifestyle driven chronic diseases.
The pilot Fresh Start PRx (FSPRx) program was developed to address type-2 diabetes disparities among uninsured patients in rural, Eastern North Carolina. Rural, uninsured patients with type-2 diabetes were prioritized as their risk of cardiometabolic, chronic disease disparities are elevated and their access to quality care, programming, and resources are limited.27-29 The FSPRx included 1-on-1 behavioral support and group education classes focusing on food literacy centered around a PRx. The purpose of this study was to examine the impact of the FSPRx program on food literacy, lifestyle behaviors, and health outcomes (e.g., glycemic control) of rural, uninsured patients with type-2 diabetes.
Methods and Materials
Study Design
The FSPRx program utilized a single group pretest-posttest design and was implemented over a 20-week period from January 2022 to May 2022. Inclusion criteria for the study include being a current patient at one of the participating clinics, an adult (age 18-65 years), and a medical diagnosis of type-2 diabetes. Participants could enroll in 3 main services: telephone-based health coaching, group education classes, and a PRx directly provided to patients. This study and all materials were approved by the “Blinded for Review” Institutional Review Board.
Recruitment, Sample, & Data Collection
Patients were recruited from two safety-net clinics in Eastern North Carolina, the Albemarle Hospital Foundation Community Care Clinic (AHFC) and the Community Care Clinic of Dare (CCCD). These two clinics serve 5 counties, and their patient population is uninsured. Both clinics are part of the North Carolina Association of Free and Charitable Clinics, the state branch of the National Association of Free and Charitable Clinics. Patients were selected for the FSPRx program based on provider referrals and electronic health record review. Members of the research team called potentially eligible patients and scheduled them for enrollment appointments in January and February of 2022 and providers referred patients while the research team was on-site at the clinics.
Patients enrolled in the study provided written informed consent, completed a questionnaire that included self-reported sociodemographic information, assessment of food literacy using a food skills confidence tool, diet quality, physical activity, and had blood drawn intravenously for hemoglobin A1C (HbA1C). All survey data were collected orally and recorded on iPads by trained members of the research team to ensure accurate data collection with a lower literacy patient population. These assessments were completed pre- and post-program. Post-program data collection occurred in May 2022 and was conducted via telephone; patients were scheduled with appointments at the clinics to have HbA1C measurements taken. All data were collected and managed with Research Electronic Data Capture (REDCap) a HIPAA secure, web-based application designed to support data capture for research studies. 30
Questionnaires
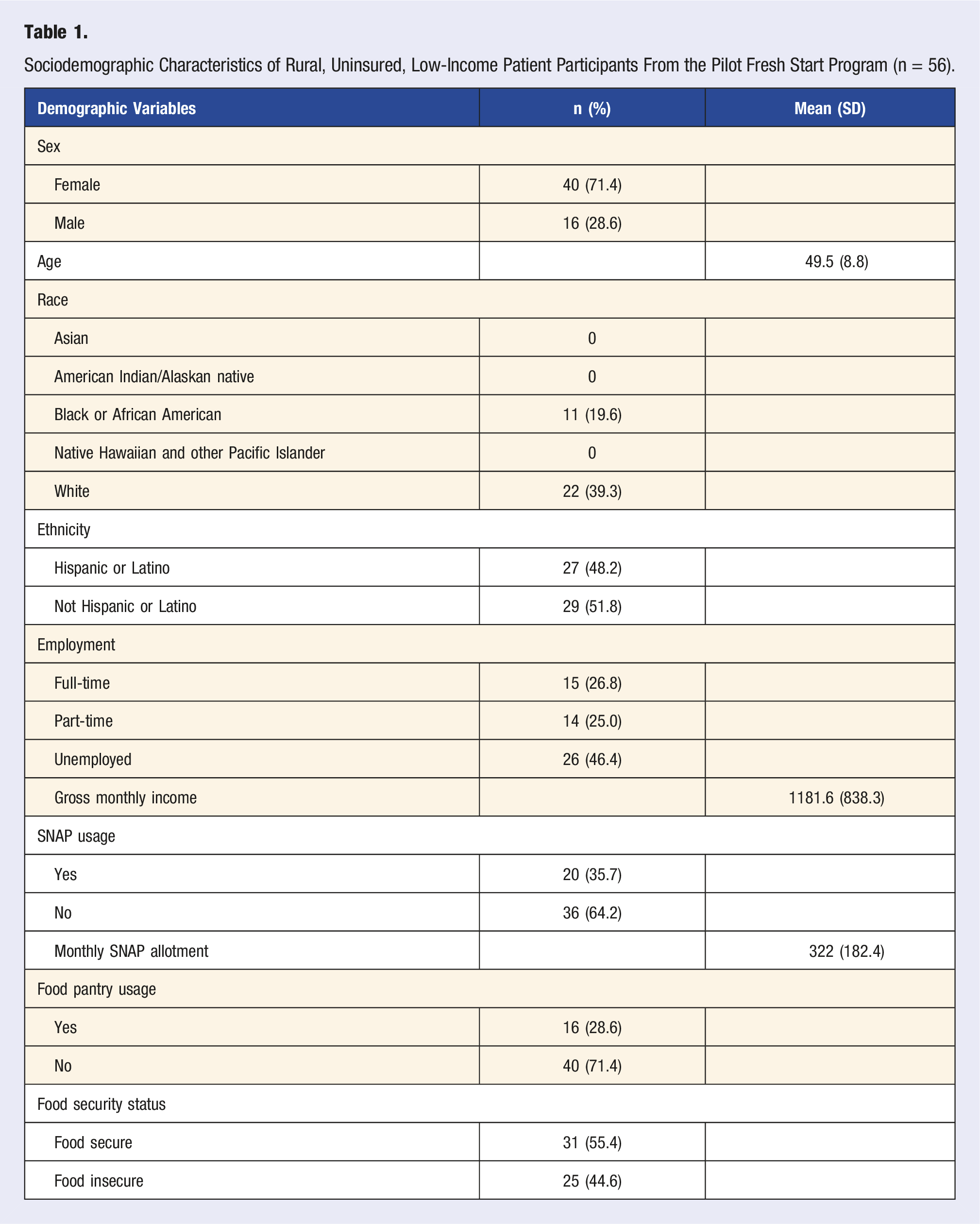
Race and ethnicity were self-reported and utilized the two questions from the Office of Management and Budget standards for collecting and reporting race/ethnicity data. 31 Patients self-reported race as American Indian or Alaskan Native, Asian, Black or African American, Native Hawaiian or Pacific Islander, and/or White and could select all races that applied to them. Ethnicities were reported as Hispanic/Latino or Non-Hispanic/Latino. Employment statuses were reported as full-time, part-time, or unemployed. Household sizes were reported by the number of adults (age 18+) and children (under the age of 18). Gross monthly income were reported to the closest dollar amount estimate and they were asked to select if they had used any food assistance (e.g., Women Infants and Children (WIC), Supplemental Nutrition Assistance Program (SNAP), food pantry, other) within the last twelve months. Food insecurity were assessed using the Hunger Vital Sign-2 question screener as it has shown efficacy in identifying food insecurity within a clinical setting. 32
Food literacy scores were calculated based on 19 questions from a food skills confidence tool that are broken into meal planning and prepping (n = 3), shopping (n = 3), budgeting (n = 4), nutrition resourcefulness (n = 5), and label reading/consumer awareness (n = 4). Questions were scored from 1-7 (1 = very poor, 7 = very good) for perceived self-efficacy/skill level and each category were summed individually. 33 All category scores were summed individually and a total food literacy score comprising all categories was also summed (19 questions x 7 = 133 maximum score). Diet quality was assessed using 3 questions on whole grain, fruit, and vegetable consumption. Each question asked how often patients consumed 2 servings of whole grains, fruits, or vegetables and answer choices included “rarely/never,” “1-2 times per week,” “3+ times per week,” “1-2 servings per day,” and “3+ servings per day.”
Confidence in including physical activity into their daily routine was also assessed utilizing a Likert scale which included very confident, confident, somewhat confident, not confident, and unsure. Each answer choice was assigned a numerical value where unsure = 0, not confident = 1, somewhat confident = 2, confident = 3, very confident = 4. Patients also had blood drawn intravenously pre- and post-program to measure HbA1C. HbA1C data were collected through retrospective chart review and reported to the nearest .1%.
Intervention
The FSPRx program consisted of 9 bi-weekly, 1.5-hour group sessions held at the CCCD and a church fellowship hall near the AHFC. Each group class included cooking/taste testing, physical activity demonstrations/lessons, health education lessons/activities, recipe/nutrition facts discussion, and distribution of the PRx. The cooking/taste testing focused on three different preparation techniques for non-starchy vegetables. Cooking was done using a mobile teaching kitchen which included a sink, prep station, induction burners, and a convection oven. Members of the research team cooked/prepared each recipe for the patients to taste to ensure time for each other class component. Each week there would be a new vegetable or vegetable combination for the cooking and taste testing. The same vegetables that patients taste tested they received through the PRx, and the recipes/nutrition facts sheets aligned with those vegetables. A range of 3-5lbs/patient of produce were most typically provided.
Physical activity demonstrations/lessons focused on low to moderate intensity aerobic and resistance training. Which included flexibility, mobility, chair-based exercises and yoga, resistance band exercises, and walking. These sessions were led by a certified personal trainer and kinesiology student who discussed the importance of that day's physical activity lessons and then encouraged patients to follow along with the exercises during the demonstrations. Patients also received handouts with additional physical activity information and exercises to take home with them to reinforce physical activity outside of the class.
The health education lessons/activities were taught by a registered dietitian nutritionist assisted by other research team members. Class topics included carbohydrates, fruits/vegetables, shopping/budgeting, weight loss/management, physical activity, stress/mental health, and heart health. Patients received short educational lectures on the daily topic followed by activities to bolster knowledge and skill building while reinforcing key takeaways. Patients also received educational handouts to take home with them to promote self-efficacy. These handouts came from trusted organizations such as the American Diabetes Association, American Heart Association, and United States Department of Agriculture.
Promotion of healthy lifestyle behaviors such as increasing physical activity, fruit/vegetable consumption, and water consumption, while decreasing sugar sweetened beverages, salty and processed snacks was encouraged by the one-on-one health coaching. The health coaches were undergraduate pre-health profession students who were trained on motivational interviewing, goal setting, physical activity, and nutrition recommendations for weight management. They were overseen by 2 licensed registered dietitian nutritionists.
Statistical Analysis
Descriptive statistics were conducted for all sociodemographic data. Paired sample t-tests evaluated changes in food literacy category scores, total food literacy scores, and HbA1C pre- and post-program. Independent sample t-tests examined HbA1C differences among health coach contact frequencies and group class attendance greater than 4. The number 4 was selected as this is an established threshold among previously conducted evidenced-based behavioral interventions. 31 Wilcoxon signed-rank test examined categorical changes in whole grain, fruit, and vegetable consumption and daily physical activity confidence. Statistical significance was set at P < .05. All data were analyzed using SPSS statistics software (Version 28.0 IBM corp.).
Results
Sociodemographic Characteristics of Rural, Uninsured, Low-Income Patient Participants From the Pilot Fresh Start Program (n = 56).
The majority (62.5%) enrolled in all three services: health coaching, group classes, and the PRx. Twenty-seven patients had an initial assessment with their health coach and at least one follow-up phone call, while (n = 24) had an initial assessment and 3 or more follow-up phone calls. Thirty-five patients attended the group class and received the PRx at least one time and (n = 20) patients attended the group classes and received the PRx 3 or more times. Twenty-seven patients completed pre- and post-intervention diet quality questions, while 19 patients completed all pre- and post-intervention food literacy and physical activity confidence questions. Pre- and post-intervention HbA1C measurements were collected from (n = 27) patients.
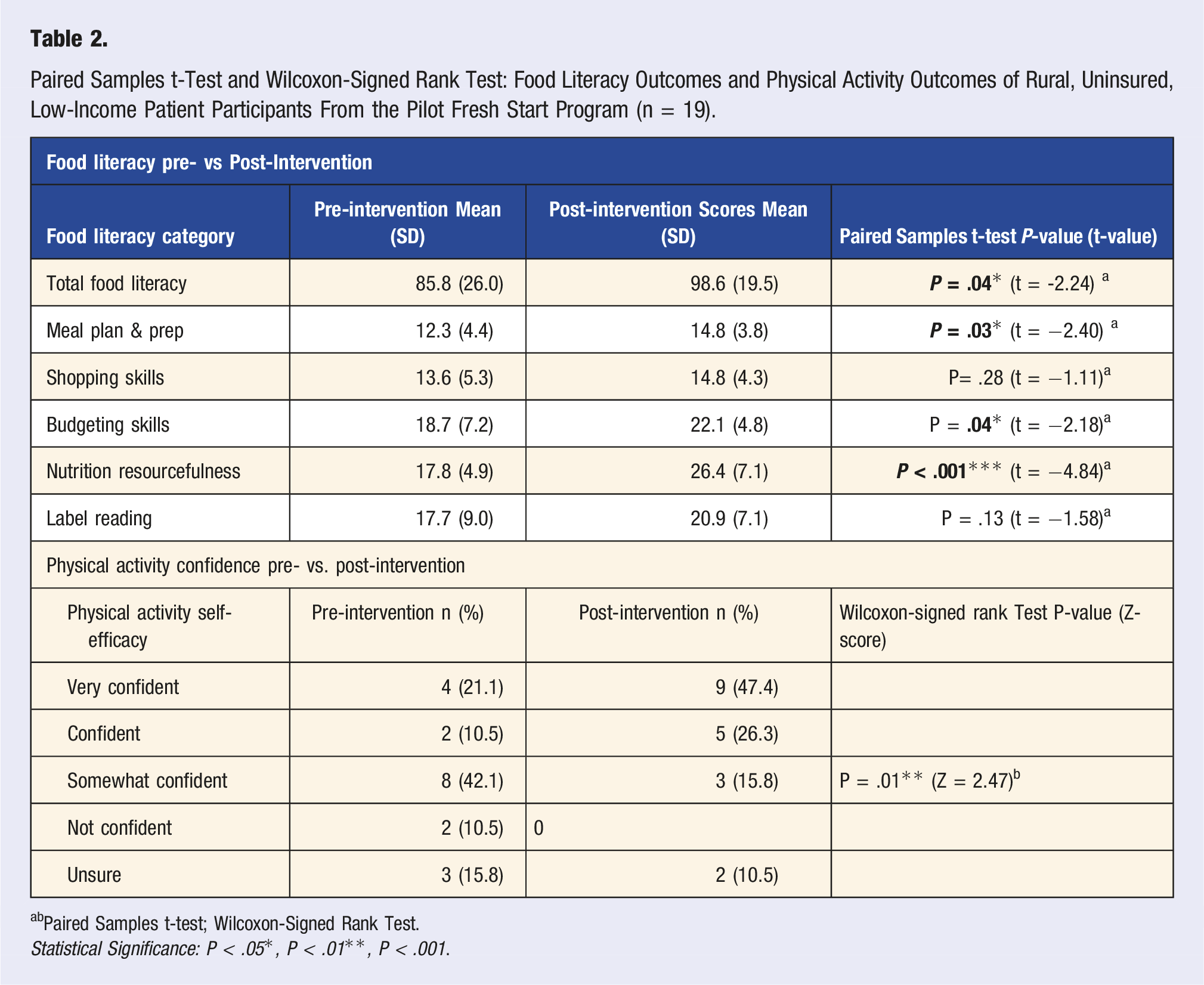
Paired Samples t-Test and Wilcoxon-Signed Rank Test: Food Literacy Outcomes and Physical Activity Outcomes of Rural, Uninsured, Low-Income Patient Participants From the Pilot Fresh Start Program (n = 19).
bPaired Samples t-test; Wilcoxon-Signed Rank Test.
Statistical Significance: P < .05*, P < .01**, P < .001.
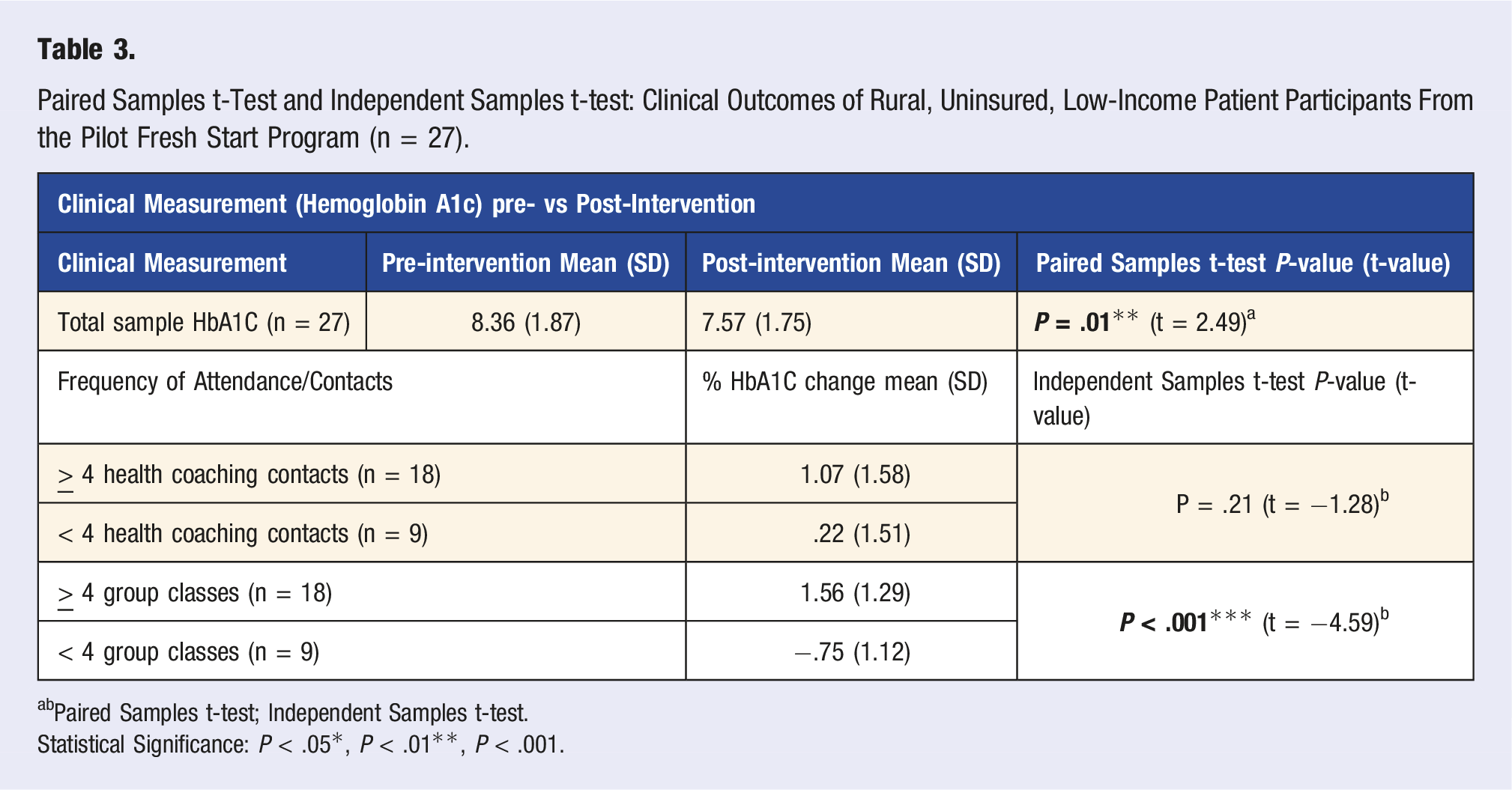
Paired Samples t-Test and Independent Samples t-test: Clinical Outcomes of Rural, Uninsured, Low-Income Patient Participants From the Pilot Fresh Start Program (n = 27).
bPaired Samples t-test; Independent Samples t-test.
Statistical Significance: P < .05*, P < .01**, P < .001.
Discussion
The pilot FSPRx program was a multi-layered PRx intervention that integrated behavioral support through health coaching and group educational classes focusing on food literacy and connected a variety of produce directly to participants. This comprehensive PRx approach was impactful with a highly vulnerable, medically underserved patient population and we observed significant improvements in fruit and vegetable consumption, food literacy scores, and glycemic control (e.g., HbA1C). Implications and discussion of the FSPRx pilot program which aligned improved access to healthful produce, food literacy nutrition education to utilize produce and individualized behavioral support to further improve diet and lifestyle behaviors are further outlined in the subsequent section.
Significant improvements in fruit and vegetable consumption were observed among FSPRx participants. There were also significant improvements in total food literacy, especially around nutrition resourcefulness, were observed in the FSPRx intervention. These findings were likely due to the in-person culinary and food focused nutrition education learning activities (e.g., how to plan for healthy meals on a budget), cooking demonstrations, and taste testing. The FSPRx program also aligned the culinary support with the PRx (3-5 lbs. produce/class) and ensured a diverse variety of produce with a focus on non-starchy vegetables. The quantity of produce connected to patients (3-5lbs/per class) exceeded amounts available with typical voucher programs averaging 15$. 34
Our unique PRx approach also ensured participants were exposed to a wide range of produce and were equipped with the knowledge and skills to prepare and use the food we provided. This is also different from most published PRx programs—for which participants receive vouchers and select their produce, which may decrease exposure to new fruit and vegetables and contribute to a less diverse diet. The culinary and food focused nutrition education and taste testing work together to expose participants to new/unfamiliar fruits and vegetables and provide them with the knowledge and skills to prepare them. Lastly, as most PRx programs evaluate increases in fruit and vegetable consumption broadly—it is unknown if dietary diversity improves. The FSPRx approach—ensures exposure, promotes variety within the diet and provides culinary focused nutrition education. This exposure and foundation of knowledge/skills may contribute to a lasting effect on participants dietary quality even after grant funds for PRx programs are exhausted.
In addition to improved food literacy- significant improvements in glycemic control were observed over only a few months with a highly vulnerable and medically underserved patient population. The mean decline in HbA1C observed across all FSPRX patients was .79% and declines of as little as .2% have been associated with an up to 10% reduction in mortality risk and improved quality of life. 35 There also was an average reduction in HbA1C of 1.78% among the 13 participants who attended at least 4 group classes and had at least 4 contacts with their health coach. Declines of 1.0% or greater have been associated with a 2% reduction in all-cause health care expenditures and 13% reduction in diabetes-related expenditures. 36 Furthermore, these reductions in HbA1C were similar to those typically achieved with common oral medication treatments for glycemic control (e.g., metformin). 37 The HbA1C declines observed in the FSPRx program were more pronounced than several previously published PRx programs, and were achieved with a highly vulnerable, under-resourced patient population (.79 vs .71 and .15).38,39 It is also notable that improvements in glycemic control were typically more pronounced when individuals participated more frequently in group educational classes. Group education along with peer support from others managing the same chronic condition has been shown to be effective in improving glycemic control in other studies and our findings suggest similarities. 40
While there are many strengths to the multi-layered approach of the Fresh Start PRx program, it is not without limitations. Our study lacked a control/comparison group which could have contributed to bias in our findings. The patient population was unique—for example, rural, low-income, uninsured with diabetes—and may not be comparable to others. However, it is also notable that such effects were observed with a patient population that is hard to access for research and experiences barriers to a healthy lifestyle and poor health outcomes. Our comprehensive program may be difficult to replicate and alternative approaches to the individual program components that are cost-effective may also be beneficial and worth exploring. Hybrid/virtual approaches and utilizing community partners who could be trained to offer similar services to support food literacy and/or provide behavioral support (e.g., cooperative extension, SNAP-Ed, community health workers) may be beneficial for other PRx programs. The direct provision of produce to participants during group classes provided exposure to a variety of produce; however, for participants who could not make a group class they were unable to access the PRx and this limited choice for participants. Additionally, the hands-on food literacy and culinary focused nutrition education occurred during group classes, which were hard for many rural, low-income participants to consistently attend. Creative strategies to improve access and connect participants with PRx and culinary/food literacy focused education resources to complement the PRx should be further explored as many participants struggled to make all classes. Lastly, training health coaches to work with participants on culinary and food skills may also be a feasible option.
Conclusion
The comprehensive FSPRx program demonstrated significant improvement in glycemic control, fruit and vegetable consumption, and food literacy with a highly vulnerable, medically under-resourced population—rural uninsured patients with type-2 diabetes. This was achieved through the coordination and integration of 3 different complementary evidence-based strategies: health coaching, group educational classes, and a PRx. While further research is warranted with larger sample sizes and other patient groups, this pilot suggests more comprehensive PRx programming—that integrates culinary and food literacy focused education and behavioral support may be especially effective in addressing chronic disease disparities, especially diabetes, with underserved and under-resourced patient populations. Future studies should examine and identify the most efficient and cost-effective approach within this framework. Lastly, the effectiveness of our approach should also be examined with other similar cardiometabolic related chronic diseases (e.g., hypertension, cardiovascular disease) as promotion of a healthy lifestyle is critical to managing these conditions as well.