
Abstract
Transforming research into practice via implementation science may improve institution-wide implementation success rates for lifestyle medicine (LM). Implementation science (IS) is the study of methods that facilitate the uptake of evidence-based practice and research into regular use by practitioners and policymakers. Multiple IS frameworks, such as the Reach, Effectiveness, Adoption, Implementation, Maintenance/Practical Robust Implementation Strategy Model (RE-AIM/PRISM) model, Exploration, Preparation, Implementation, Sustainment (EPIS) model, and Consolidated Framework for Implementation Research (CFIR) model, have been developed. IS frameworks provide a strong yet adaptable foundation for launching initiatives, minimizing barriers by challenging implementers to identify and address problems that impede implementation, and promoting long-term sustainability and positive outcomes. The trouble-shooting tips provided in this article are strategically aligned with the RE-AIM/PRISM model of IS to maximize the likelihood of implementation success within the LM space. These tips provide guidance on how to effectively implement interventions, sustain their delivery, and avoid or overcome barriers to implementation. This article presents 12 tips intended as a list of options to facilitate the implementation phases of an initiative, as opposed to offering an all-or-nothing approach to implementation strategy. Current IS priorities emphasize system change and sustainability, which are essential components of successful implementation of LM initiatives.
Keywords
“IS research is being pursued both nationally and internationally as a way to promote healthcare system change.”
Introduction
The institutional setting presents a unique opportunity for the implementation of effective strategies to address the promotion of health, prevention of illness, and treatment/reversal of chronic disease. Lifestyle medicine (LM) is defined by the American College of Lifestyle Medicine (ACLM) as the “medical specialty that uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions … Applying the six pillars of lifestyle medicine—a whole food, plant-predominant eating pattern, physical activity, restorative sleep, stress management, avoidance of risky substances and positive social connections.” 1 Adoption of the six pillars of LM can decrease healthcare costs in the US and improve health equity of the country. 2 According to the United Nations “The combination of 4 healthy lifestyle factors -- maintaining a healthy weight, exercising regularly, following a healthy diet, and not smoking -- seem to be associated with as much as an 80% reduction in the risk of developing the most common and deadly chronic diseases." 3 The ACLM further emphasizes the power of LM stating “A lifestyle medicine approach to population care has the potential to arrest the decades-long rise in the prevalence of chronic conditions and their burdensome costs … which strongly aligns the field with the Quintuple Aim of better health outcomes, lower cost, improved patient satisfaction, improved provider well-being, and advancement in health equity, in addition to its alignment with planetary health.” 4 A resolution was passed by the American Medical Association in 2017 recognizing the critical role of lifestyle medicine in public health and supporting the incorporation of LM curricula into medical schools.5-8
The implementation phase of change initiatives, from planning to piloting, can be a point of failure for many new LM programs despite the vested interest of many healthcare practitioners. An international study published in 2018 revealed that 59% of change initiatives lacking clear and organized implementation strategies failed to reach all their objectives, resulting in the failure of the initiative as a whole. 5 A change in behavior is necessary at both the individual level and the group level to implement new practices or change existing practices in organizations, services, or systems. Lack of resources, improper implementation strategies, and stakeholder opposition are often cited as barriers to successful implementation of new initiatives in healthcare. 9 Barriers to LM program implementation include insufficient LM training, startup costs, the culture of Western medicine, and lack of training of healthcare providers in starting new and sustainable programs. 10 A multitude of survey studies over time have revealed low self-perceived lifestyle counseling proficiency and limited understanding of approaches to obesity prevention and management among primary care residents.11-18 Research has suggested that quantitative evidence, building trusting partnerships, human resources support, and an enabling and supportive internal and external environment are factors that facilitate the diffusion and implementation of innovations in healthcare services across a wide range of sectors. 19
Transforming research into practice via implementation science (IS) may improve institution-wide implementation success rates for LM. IS is the scientific study of methods that facilitate the uptake of evidence-based practice and research into regular use by practitioners and policymakers. 9 Multiple IS frameworks, such as the Reach, Effectiveness, Adoption, Implementation, Maintenance/Practical Robust Implementation Strategy Model (RE-AIM/PRISM) model, Exploration, Preparation, Implementation, Sustainment (EPIS) model, and Consolidated Framework for Implementation Research (CFIR) model, have been developed with varying focuses on implementation, existing barriers to implementation, and ways to bridge the gap between what is known and what is practiced.20-23 IS frameworks provide a strong yet adaptable foundation for launching initiatives, minimizing barriers by challenging implementers to identify and address problems that slow or halt the implementation of evidence-based practices and proven health interventions, and promoting long-term sustainability and positive outcomes.24,25
The RE-AIM framework serves as the system behind the 12 tips proposed in this article given its effectiveness regarding practicality, ease of use, user-friendly toolkits, and flexible layout. Each of the 12 tips for LM initiative success at the institutional level addresses a particular letter of RE-AIM. Of note, many of these tips benefit multiple parts of RE-AIM, and all components of the framework can be considered equally important. This report discusses the PRISM model as a supplement to the RE-AIM model (See Figure 1). This article presents LM implementation tips intended as a list of options to enhance the likelihood of implementation success, as opposed to offering an all-or-nothing implementation strategy. A needs analysis of priorities and perceptions among constituents within the institution, healthcare system, or organization can be conducted to identify which domain(s) of RE-AIM must be strengthened for optimal success, followed by the use of the strategies provided to address these domains, and expansion to other domains as necessary. The key to implementation success is not necessarily addressing all 12 tips, but rather focusing on one or more tips that may best address the challenges that are most crucial and relevant to each institution. The RE-AIM model provides a structure for planning, implementation, sustainability, research, evaluation, holistic assessment of situational strengths and weaknesses, and analysis of current and future initiatives that is in all stages of implementation. The first two domains of the RE-AIM model (Reach and Effectiveness) assess individual level factors of implementation, while the latter 3 domains (Adoption, Implementation, and Maintenance) assess the settings of the initiative (e.g., community, institution, and clinic).
Reach
A program’s reach measures the absolute number, proportion, and representation of people willing to participate in an initiative, intervention, or program, as well as their reasons for or against participation. This domain requires a definition and understanding of the target population (e.g., students, residents, patients, children, and adults) as well as effective methods of reaching the targeted population. The success of a program can be determined quantitatively by comparing the number of participants to the total population eligible for the program. It is possible to identify significant differences between participants and non-participants based on comparisons of their characteristics, which can enable adjustments or expansions of the program to be made upon assessment.
Tip 1: Reach Out to Preexisting Similar or Relevant Initiatives to Recruit Interested Parties for Potential Collaboration Opportunities
Taking the time to investigate and engage with various active initiatives at one’s institution is strategic and resourceful with regard to time, effort, people, services, and finances. Opportunities to co-brand and collaborate with like-minded individuals, groups, and organizations through established models, data sets, programs, and institutional resources can confer mutual benefit to both parties, as well as their initiatives. LM has a broad reach and relevance as a primary prevention and/or treatment model. It may be useful and beneficial to add the LM perspective to numerous active projects. Benefits of reaching out include: 1. Identifies potential colleagues who may be interested in LM, which can lead to partnership, networking, and team formation. The principles of LM remain unfamiliar to many healthcare professionals despite the growth of the field of LM. A quick review of the principles of LM allows colleagues to assess whether they align with the goals and values promoted in LM. Common goals and shared values facilitate productive partnerships and collaboration. 2. Promotes LM in established projects. Many active projects are executed under grant funding and may have the potential to provide financial resources or support for LM initiatives. There may also be opportunities to position LM initiatives as a subset of a project with funding, which imparts resources to develop, grow, and implement LM ideas and goals. 3. Connects different departments and reduces silos in institutions while promoting LM efforts. Many thought leaders are looking to start projects, expand on existing opportunities, and surround themselves with a strong peer support network. Facilitating connections through common priorities may lead interested parties to reach out to assist with projects, pitch new ideas, and create new opportunities by capitalizing on the previously unexplored motivations, values, and beliefs. 4. Minimizes wasted efforts by discerning established resources, materials, contacts, organizational structures, pre-existing frameworks, etc., that can be adapted to fit LM programs and initiatives. 5. Provides a recruitment opportunity for the targeted population. Identifying a cohort of interested individuals within the target population can facilitate the development of focus groups and establish targeted marketing and educational materials that are conducive to optimal participation, engagement, and participant satisfaction.
Tip 2: Determine Areas of Focus in Which LM Initiatives May be Implemented
Choosing an initiative to launch should be based on a particular area of interest. Initial efforts should be directed at one area (e.g., a LM pillar, such as physical activity; one type of intervention, such as health coaching; a single disease, such as diabetes), then expanded based on initiative success and adoption by other stakeholders. Proponents of LM can engage in a variety of sectors for the purpose of promoting and implementing their initiatives. Examples include medical education, community outreach/education, and direct patient care.
For someone interested in medical education, implementing a GME or UME curricula at a healthcare institution may be easier to accomplish due to elevated interest. Reach out to appropriate educational leadership to see if a general needs or targeted needs assessment was performed. The needs assessment may uncover educational deficiencies that can be solved or improved by LM education. Those interested in community outreach/education can reach out to local community organizations, institutional community outreach leadership, and to specialized populations (migrant workers, undocumented, undomiciled, etc.) to assess what needs are present and how LM may address these needs. For direct patient care, creating a LM clinic with one-on-one visits or lifestyle medicine shared medical appointments may be a practical option. The ACLM provides an ACLM primary care practice toolkit, a FQHC/CHC toolkit, and a LM shared medical appointment toolkit which has guidelines for such an initiative. Alternative ways to implement direct care include partnering with other clinics of similar interest such as obesity medicine, preventive medicine, integrative medicine, or complementary/alternative medicine. Using one of the established formats published by the ACLM may prove more efficient and/or effective than creating an initiative de novo.
Effectiveness
Effectiveness is the impact of an intervention on important individual outcomes, including potential negative effects, and broader impact including quality of life and economic outcomes, as well as variability across subgroups. The effectiveness of any program can be enhanced by setting objective outcome measures of participants. Appropriate collaborative efforts, resources, and ongoing feedback from the associated organization or institution are also key to implementing effective initiatives. Evidence-based programs are often evaluated based on their effectiveness, given that objective measures can be easily tracked. Effectiveness is at the core of most research on evidence-based programs and is an essential component of peer-reviewed publications.
Tip 3: Perform a DICE Change Management Calculation
The Duration, Integrity, Commitment, and Effort (DICE) framework was developed by the Boston Consulting Group to predict the likeliness of future success of change initiatives. The DICE calculation of change initiatives is a percentage that can be used to measure potential weaknesses in program implementation to determine if they are barriers to success. It is possible to enhance success odds by addressing potential problem areas as soon as they are identified. The DICE calculator can be found at https://dice.bcg.com/dice-calculator/. Components of the DICE framework may be described as follows:
Duration
Projects that have a longer duration are more likely to face unforeseen obstacles. Performing routine course corrections with frequent assessments and identification of obstacles mitigates the risk of programs failing due to shifts in motivation, changes in personnel involved, and closed opportunities. Regular milestone checks can ensure that a program remains on track and progress is made between checkpoints. The frequency of check-ins matters more than the lifespan of the project. 26
Integrity
There are several factors that may affect integrity, including motivations, conflict resolution skills, administrative skills, individual experience with materials related to the project, and resilience in the setting of obstacles. Strategic and cohesive team composition, role allocation, and task delegation are essential components of ensuring the success of a change initiative. Weakness in any of these sectors may be addressed by obtaining a certification in LM to increase knowledge of the subject, reviewing successfully implemented models and adapting as needed, creating a team of mentors and associates who may assist with different skill sets required of the project, reframing mentality on failures and setbacks by using them as opportunities to cultivate team culture, promoting growth on individual and team levels, and facilitating creative thinking and problem-solving.
Commitment to Change (Senior Level)
The chances of success can be greatly increased with the commitment and support of senior level administration. The most ideal form of project support comes from those who have high influence and are highly impacted by its results. The support of esteemed individuals and the wider public, especially those within the department or institution associated with the project, has the power to reduce resistance to implementation, raise awareness and participation, and increase the possibility of receiving secure funding sources for project initiatives. Having initiatives supported and aligned with the values adopted by senior management helps foster commitment to successful change and facilitates a clear and inspiring message to the organization or institution.
Commitment to Change (Team Level)
Team dynamics can be examined from a top-down and bottom-up perspective. It is important to understand the impact of the project on the frontlines and that support on the ground can either propel or derail a project’s momentum. The leaders of an initiative should understand who will implement the changes, how these changes will be implemented, and what is required for them to be successful in their efforts. A successful initiative can be driven by a clear understanding of the objectives, goals, and expectations of the initiative that is shared among all team members. The ability to engage in open dialogue among team members during all phases of program development and implementation is a crucial determinant of program productivity, innovation, quality, support, team member satisfaction, and task performance. Discussions with the team/employees can help identify the steps that need to be taken to promote cohesion and reduce concerns expressed by individuals involved in the initiative. Team members must be equipped with the tools needed to succeed. This can be accomplished by providing the necessary training and resources needed to improve the effectiveness of the initiative.
Effort
It is pertinent to consider the extent to which the implementation team will be required to perform additional work outside of base duties. The average team can handle approximately 10% extra work without incident, but any additional effort beyond their normal duties may cause resentment among members. It is best to create protected time for activities related to change implementation or to distribute work to prevent overburdening the implementation team. Notably, overworking even the most motivated individuals can lead to burnout. Those in leadership positions should ensure sufficient support is provided, time is being managed efficiently, workload is minimized as necessary, and efficiency is maximized. When effort cannot be lowered sufficiently, splitting the project into smaller, more manageable goals, and extending the implementation timeframe can prevent burnout or overexertion.
Tip 4: Reach Out to External Institutions That Have Implemented Similar Initiatives
Those leading implementation initiatives can consult other healthcare institutions that have established a similar initiative after considering all the factors relevant to your institution to elucidate unforeseen barriers, establish a network of support, find mentors who have succeeded in similar efforts, and possibly develop multi-institutional projects that will allow a broader scope/reach in the future. The ACLM Health Systems Council (HSC) serves as a network of healthcare institutions dedicated to the LM movement. The ACLM defines the ACLM HSC as “a collaborative learning community of health systems that have actively begun integrating lifestyle medicine programs into their organizations and have made a commitment to the following: 1) Strengthen their efforts by embracing strategies that are most effective in enhancing health and achieving organization-level goals; and 2) Share their learnings with other Council members' health systems.”
27
The ACLM provides dedicated staff to support the HSC in its efforts to integrate a therapeutic dose of lifestyle medicine into patient care, employee health, and communities.
Once an external organization to contact is chosen, it is advisable to request a meeting, plan for the meeting, and set a firm date in order to increase the likelihood of it taking place. It is recommended to initiate contact with other institutions through an elevator pitch approach to maximize the amount of time available and the efficiency of the delivery process. An elevator pitch provides a one-minute high-level summary of the problem the initiative intends to address, the solution to this problem, and how the program, if implemented, can contribute to the solution. There may also be a discussion of how information was acquired regarding the institution and its initiative, as well as a short list of questions for which advice is sought. Establishing a relationship with the other institution to identify what worked for their initiative, how to avoid identified barriers, and understanding what resources are needed to improve the effectiveness of a comparable project can be helpful. Materials created by other institutions can be adopted with permission in the setting of a compatible connection, thereby reducing the need for development time and cost.
Adoption
A program’s adoption can be identified by the absolute number, proportion, and representativeness of settings and intervention agents (those responsible for delivering the program) who are interested in implementing the initiative, as well as the reasons they are willing to do so. Of note, adoption can have many nested levels. The team, people, processes, and settings of the implementation site can impact ease of adoption. Assessment of initiatives can be conducted by visiting implementation sites, understanding the operational systems, and learning about the populations that may be involved with and impacted by the initiative. It is crucial to connect and stay in close contact with sites and frontline staff to create cohesion, generate support, and inspire others to make the project a success. Several factors may be considered when assessing the adoption of an initiative: (1) How does the initiative align with the goals and objectives of the sites of implementation? (2) Are there enough resources, training, and staff to successfully complete the required components? (3) Is there support and commitment from multiple levels (e.g., senior management, frontline staff, and mediatory managers) at the sites of implementation?
Tip 5: Perform a Stakeholder Analysis
The performance of stakeholder analysis can provide a complete framework to identify, evaluate, and prioritize all stakeholders relevant to or involved with an initiative at an institution to minimize resistance and gain support from those at high influence. A stakeholder is an individual or organization who is actively involved in the project, or whose interests may be positively or negatively affected as a result of project execution or successful project completion that has the potential to play a pivotal role in the success or failure of an initiative. The following section outlines the steps to properly complete a stakeholder analysis.
Step 1: Identify Stakeholders for the Initiative
Stakeholders are individuals who may be affected by or interested in the work being executed by the LM initiative. People from diverse backgrounds, disciplines, and levels of work can be included on this list. A typical list of stakeholders in the LM field includes but is not limited to patients, healthcare providers, administration, project managers, educational faculty, students, and residents, as well as related departments, specialties, or community organizations. Categories of stakeholders may include mental and behavioral health workers, integrative medicine, preventive medicine, sports medicine, registered dietitian nutritionists, non-profit organizations, and religious groups.
Step 2: Prioritize the Stakeholders
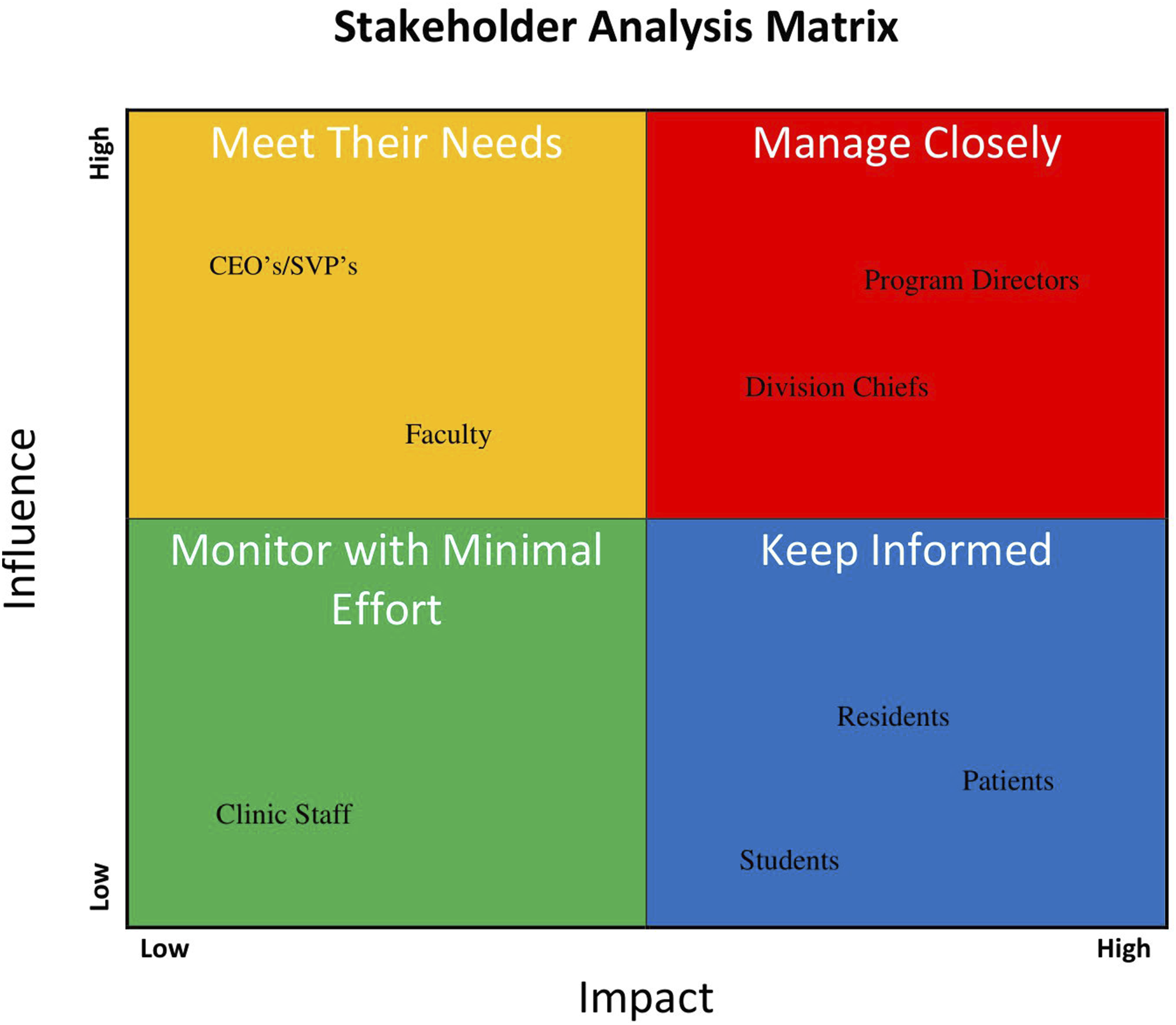
Stakeholders may be categorized and thereby prioritized via utilization of the interactive stakeholder analysis spreadsheet in the supplementary index. Implementers can create a graph with an X axis representing “Impact on stakeholders” and a Y axis representing “Influence of stakeholders” upon drafting the list of stakeholders. Plotting stakeholders along this chart, then dividing the chart into 4 quadrants can help determine the most appropriate action to be taken with each stakeholder (See Figure 2). The stakeholders may be classified and handled in accordance with the following categories:
High Influence, High Impact
A full engagement and best-practice approach is often the most effective way to maximize the value of the connection with these stakeholders. It is expected that this group will receive the greatest level of partnership and satisfaction. The initiative leadership and team members are advised to determine what is needed for a full commitment to the implementation and support of the LM initiatives.
High Influence, Low Impact
It is essential to maintain and appeal to stakeholder satisfaction in order to maximize connections with stakeholders in this category. A consistent stream of updates without excessive detail or frequency is typically the best strategy to maintain interest and engagement at an appropriate level.
Low Influence, High Impact
It is important to provide adequate information and clear communication to these stakeholders to maintain effective relationships. The stakeholders in this category can often be of assistance with the details of the project, and if supported sufficiently, can even influence stakeholder groups with a higher level of influence.
Low Influence, Low Impact
Implementers should maintain an awareness of stakeholders within this category and monitor their ability to influence populations and provide active support and/or resources for the initiative. A periodic effort to keep those within this category informed and engaged may occasionally lead to action or result in a positive outcome.
Step 3: Understand the Stakeholders
Direct, open dialogue with stakeholders can be an effective tool for gaining clarity about their interests, attitudes (e.g., supportive, neutral, oppositional), and perceptions. Initiative leadership may be able to determine how to inspire stakeholders to support an initiative when such measures become necessary by examining their perspectives regarding concepts such as competition with other programs, financial viability, and relevance and significance to the community and its needs.
Tip 6: Discover/Review Initiatives Associated With or Relevant to LM at the Institution
Understanding the level of interest in LM within healthcare institutions can inform aspects of implementation strategy. An institution with a greater number of active projects or initiatives is more likely to be open to ideas and may have access to funding, program models, and/or project support, thereby increasing the likelihood of successful implementation. A better understanding of LM projects at institutions of interest can assist initiative leaders in devising a strategy with regard to how the initiative can fit within the broader scope and context of the institution. Initiative leadership must evaluate the proposed project to determine how it can be innovative or collaborative compared to existing initiatives, as this will facilitate the identification of a need for implementing the program while bolstering efforts to leverage existing programs. It may be beneficial to contact leaders of different LM initiatives who might be able to provide a network of assistance, resources, and advice during the implementation process. Strategic alignment and connection with leaders within the LM space can also enhance influence and outreach for the initiative, as well as improve its likelihood of securing senior management support.
Tip 7: Increase Avenues of Communication to Promote Collaboration
Communication channels provide a convenient means of gathering and facilitating discussions, meetings, feedback, and troubleshooting, as well as the creation of new connections between those involved in or affected by an initiative (e.g., interested parties, colleagues in related fields), thereby increasing creativity, maximizing resources, fostering adoption of initiatives, and inspiring the development of new initiatives. Creating a community with shared interests that emphasizes the goals and objectives of the initiative garners motivation and creates an avenue for routine updates and connections to stakeholders and team members via a variety of communication methods, such as social media groups, group chats through apps (e.g., Microsoft Teams, GroupME, WhatsApp), a LM interest group (LMIG), or phone group chats. Communication is a versatile process with many modality options. The best approach to optimizing communication surrounding an initiative is to survey the communication preferences and needs of the stakeholders and team members within an institution to determine which avenue will produce the greatest success and participation.
Implementation
Initiative implementation refers to the extent to which intervention agents adhere to its key functions or components, including the consistency of delivery, the duration, the cost, and the adaptations made to interventions and implementation strategies. Structured programs with clear implementation guidelines, milestones, and evaluation tools are more likely to be successfully implemented. Successful implementation of an initiative requires adaptation as needed based on barriers or obstacles encountered throughout the implementation process. Costs are often a major barrier to implementation. Establishing a method or strategy for securing funding is an important step in facilitating the successful implementation of an initiative.
Tip 8: Utilize/Adapt Established LM Models From the ACLM
ACLM provides a variety of established curriculums for multiple levels of education to provide a structured opportunity to introduce lifestyle medicine into healthcare institutions. a. The LM101 course developed by Beth Frates, Michelle Tollefson, and Gia Merlo is a free open-access curriculum that covers material in the Lifestyle Medicine Handbook by Beth Frates, as well as all six pillars of lifestyle medicine, and can be integrated into any undergraduate program. b. The Lifestyle Medical Education curriculum is an open-access curriculum geared toward educating future physicians (i.e., medical students). This curriculum is divided by organ system and can be easily integrated into existing medical school curricula. This program is offered by the University of South Carolina School of Medicine at Greenville and endorsed by the American College of Lifestyle Medicine. c. The ACLM culinary medicine program provides an interactive and engaging curriculum based on the work of Michele Hauser. The purpose of this program is to train and teach medical students, residents, and faculty how to properly counsel patients on healthy eating through a variety of approaches, such as case-based teaching, nutrition counseling, and culinary skills training. This is an open-access curriculum that can be adapted to fit any institution’s needs. d. LMIGs provide health systems, medical schools, and other healthcare professional schools with an opportunity to start a LM chapter under the ACLM and organize events, projects, and collaborations aimed at raising awareness of LM and improving the health of the community. e. The Lifestyle Medicine Residency Curriculum (LMRC) provides a resident-level education curriculum with the unique opportunity for board eligibility upon completion of the program components. The LMRC consists of an educational program consisting of 100 hours of training designed by Loma Linda University in collaboration with ACLM. The program consists of an academic component and a practicum component that provides residents extensive training in LM. Individuals can choose from synchronous, resident-led sessions or online asynchronous modules based on their residency program structure. A contract signed under one Designated Institutional Official (DIO) allows multiple residencies within an institution to adopt the curriculum at the same price, which reduces overall costs and promotes sustainability of the program. f. The ACLM also provides a number of CME-granting courses covering a variety of topics and content areas. g. The ACLM HSC offers health systems the opportunity to join, collaborate, and learn from other healthcare systems concerning established LM models being practiced and implemented across the country. An institution may benefit from this opportunity to determine which initiatives will be most successful in the setting of a particular organization.
Tip 9: Understand the Contextual Domain Related to Your Initiative Utilizing the PRISM Model
The Practical Implementation Sustainability Model (PRISM) includes multilevel contextual factors relevant to program implementation. PRISM domains encompass multiple levels of contextual consideration, including characteristics of members within the community, stakeholder perspectives, settings in which interventions are conducted, the external environment (e.g., policies, regulations, financial incentives or disincentives, clinical guidelines, historical considerations), and infrastructure for implementation and sustainability. Contextual factors in the setting of implementation are relevant factors (e.g., policies, organizational climate, incentives, workflow, and the targeted population) that are not part of the intervention itself. Contextual factors are present throughout all stages of implementation, from planning through maintenance. The concept of context is central to dissemination and implementation models and is crucial to understanding translation of healthcare delivery interventions.
Infrastructure is one of the most significant domains in the PRISM model. The contextual study of infrastructure addresses issues related to initial implementation and sustained delivery of the intervention. Implementing and adapting an initiative within the current infrastructure minimizes the burden of implementation. It is important to understand that changing infrastructure may not be feasible in the setting of a particular institution, so adaptability is necessary to adjust the initiative as needed throughout the implementation process. For example, clinical workflows, electronic health record templates, and the availability of physical space are institutional factors that may prove difficult to change. Minimization of complications and increased odds of implementation success can be achieved by taking these factors into consideration prior to the initiation of implementation efforts, as well as partnering with institutions to mitigate these factors. The PRISM domains can facilitate the planning and implementation phases of interventions and guide purposeful adaptations by providing insights into possible barriers to the successful implementation of an initiative.
Tip 10: Secure Funding Opportunities
Identifying a method of mitigating the implementation barrier of cost is essential to avoid financial limitations from ultimately preventing the successful implementation of an initiative. Resources, materials, and employees are required to launch new initiatives. Therefore, direct, or indirect costs are associated with the majority of initiatives. The process of securing funding for an initiative can be highly variable.
Grants
Grants are available from a variety of private, state, and federal institutions across the country. Institutions often create grants for initiatives that align with their interests and different programs. It may be possible to narrow down the grant search to those that match the initiative being proposed by consulting the grant team at the institution of interest or the grant team at ACLM. The ACLM also publishes a list of grants aligned with LM for ACLM members titled “Grant Opportunities” on the ACLM Connect Open Forum. Grant funding offers the benefit of covering a portion of the necessary initiative funds, thus providing protected time to invest in the growth and development of the program.
Distributable Costs
Multiple departments or divisions may benefit from the program, depending on its scope. Administrative leaders of an institution may be more likely to justify the cost of an initiative if the cost is split across multiple divisions or departments.
Philanthropy
It is typically necessary to connect with departments within an institution that manage philanthropic networks and efforts to use philanthropy as an initiative funding source. Philanthropy can have value as a source of initiative funding because it enables a long-term relationship, which can lead to further funding for future initiatives.
Collaborating and Associating with Funded Programs
The process of finding other LM initiatives may lead to the discovery of similar or related programs that are already funded. These programs may have leftover or additional funding depending on their funding source, allowing other initiatives to obtain funding. It is important to consider discussing funding methods with programs supported by preexisting sources of funds, as well as whether they may be willing to sponsor another program.
Maintenance
An initiative’s sustainability depends on maintenance. Maintenance is the extent to which a program or policy is institutionalized or integrated into routine organizational practices and policies. Of note, the RE-AIM framework also involves maintenance at the individual level. Maintenance at the individual level can be defined as the long-term effects of a program on individual outcomes after completion. The timeframe for assessments of maintenance or sustainability varies depending on the type of project. Assessing barriers, costs, leadership, staffing, and other resources necessary to continue an initiative enhances leadership’s ability to devise an implementation plan built for success. The following questions can be considered to gain a comprehensive understanding of what needs to be accomplished to ensure the long-term success of a program: (1) Can the program continue in the absence of a particular leadership figure? (2) Is the program self-sustaining or does it require continued efforts to ensure sustainability is maintained? (3) Does the program delivery infrastructure meet the needs of the program? (4) Are there appropriate milestone check-ins to ensure the initiative is operating as intended? (5) Are there ways to reduce the burden of implementation and better facilitate the integration of the program into regular practice?
Tip 11: Utilize ACLM Resources, Administration, and Departments for Assistance, Ideas, and Support
There are a variety of administrative leaders and departments within the ACLM that can be contacted via email. LM initiatives may be implemented or sustained with the assistance of the ACLM’s constituents who can plan, pitch, and find funding sources—as well as facilitate implementation, sustainability, and expansion of the initiative. a. The ACLM Health Systems Council holds quarterly meetings where representatives from various health systems present lifestyle medicine models used in their institutions. These meetings aim to provide participants with the opportunity to generate new ideas, network with individuals who have established models, and determine how to ensure the sustainability of initiative efforts. b. The LMRC team is a subset of the ACLM educational department that supports the establishment of graduate LM medical education at institutions, provides partial funding, and reduces the administrative burden associated with the implementation and maintenance of LM initiatives at institutions. c. The ACLM undergraduate medical education team is part of the ACLM educational department that is responsible for assisting with the delivery of LM education in medical schools. The ACLM also offers accreditation based on the incorporation of LM into the medical school program curriculum of an institution. The extent to which LM contact may be integrated into medical school curricula varies according to institutional capacity, ranging from bronze to platinum. Thus, LM initiatives can grow in a sustainable manner that is aligned with institutional objectives. d. The ACLM LMIG team can assist institutions in establishing LM chapters. Orientation and training are offered multiple times a year, and LMIGs may be eligible for ACLM grants to assist institutional LMIGs with the cost of LM events, education, and promotion. e. It is the responsibility of the ACLM grants team to help identify local, regional, or national grant opportunities that may align with certain initiatives providing funds for program implementation or expansion based on the specific needs of each project. The funds provided by these grants may be used to implement or expand LM initiatives as needed. f. The ACLM connect platform offers an opportunity for peer support networking through the variety of Member Interest Groups established within the ACLM. Members of the ACLM have access to like-minded individuals, workshop ideas, shared resources, and the ability to ask questions to those who may have gone through similar situations.
Tip 12: Strategically Seek Opportunities to Reduce Clinician Distress and Burnout
Lifestyle interventions may be significant in preventing and decreasing the burden of clinician burnout and distress. 28 Both planned and unplanned networking opportunities with individuals with a vested interest in LM that arise throughout the initial implementation process can provide new resources, extra assistance with an initiative, and greater influence within an institution, as well as mentorship and guidance. It may be strategic to set firm meeting times with new stakeholders/collaborators in order to protect the time of initiative leaders involved in the meeting, as these initial connections may not result in a direct or immediate collaborative relationship. The implementation, maintenance, and sustainability of an initiative depend on networking opportunities and outreach, but it is important to note that accepting every opportunity may lead to distress, overburdening, burnout, and distraction from the main objectives and framework for the initiative. Burnout can be prevented or minimized by saying yes only to opportunities with clear benefits and guaranteed outcomes, a proposed timeline for project collaboration that may include action items, deliverables, and a budget estimate. It may be in the best interests of the initiative and those involved to turn down or postpone opportunities if there is any hesitation upon consideration by initiative leadership. Any new opportunities can be aligned with the initial goals and the bandwidth of the implementation team members and can therefore be accepted without causing burnout or resentment.
Conclusion
Successful LM program implementation at any stage of development requires 5 components of the RE-AIM model of IS: reach, effectiveness, adoption, implementation, and maintenance/sustainability. The RE-AIM model provides a practical structure for implementation, sustainability, research, evaluation, and assessment of LM initiatives within the context of a strong need for LM within the healthcare sector. IS facilitates the uptake of evidence-based practice and research into regular use by practitioners and policymakers and provides initiative leadership with a multilayered perspective to maximize the success of an initiative. It is widely acknowledged that Lifestyle Medicine contributes significantly to current evidence-based practices and is reshaping the way medicine is taught and practiced.
It is important to note that a multitude of IS strategies, theories, and frameworks exist. This article focused on the RE-AIM/PRISM model. PRISM extends the RE-AIM framework to identify critical multilevel contextual factors relevant to program implementation at all stages. PRISM domains further inform the planning and implementation phases of interventions and provide guidance for adaptations. An important domain of the PRISM model is implementation and sustainability infrastructure. The troubleshooting tips provided in this article have been strategically aligned with the RE-AIM/PRISM models of IS to maximize the likelihood of implementation success within the LM space. These tips are framed under IS to provide guidance on the various components needed for successful implementation. Paired with other proven business models, available resources, step by step instructions, this article seeks to increase the skill set of its readers and their capacity for implementing interventions, sustaining their delivery, and avoiding or overcoming barriers to implementation.
Scientists and healthcare professionals, as well as evidence-based funding organizations, are becoming increasingly aware that innovative approaches to healthcare require more than the generation and presentation of evidence. IS research is being pursued both nationally and internationally as a way to promote healthcare system change. The National Institutes of Health, the Patient Outcomes Research Institute, and the Department of Veterans Affairs have recently committed funds and developed research initiatives to increase IS research within healthcare and public health.29-31 Developing and enhancing current models and frameworks that guide implementation efforts through the identification of relevant processes and the organization of data requires further research. Current IS priorities emphasize system change and sustainability, which are essential components of successful implementation of LM initiatives. PRISM/RE-AIM model utilized under creative commons license. Original article Glasgow RE, Harden SM, Gaglio B, et al. RE-AIM Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-Year Review. Front Public Health. 2019;7:64. Published 2019 Mar 29. doi:10.3389/fpubh.2019.00064. An example stakeholder analysis chart. This theoretical sample places multiple types of stakeholders along the chart based on a proposed lifestyle medicine residency curriculum initiative. Given this those with the highest influence over the direct decision would be those most closely related to the residency program including faculty, program directors, and division chiefs. While those most likely to be impacted would be those who will receive the curriculum such as residents and medical students.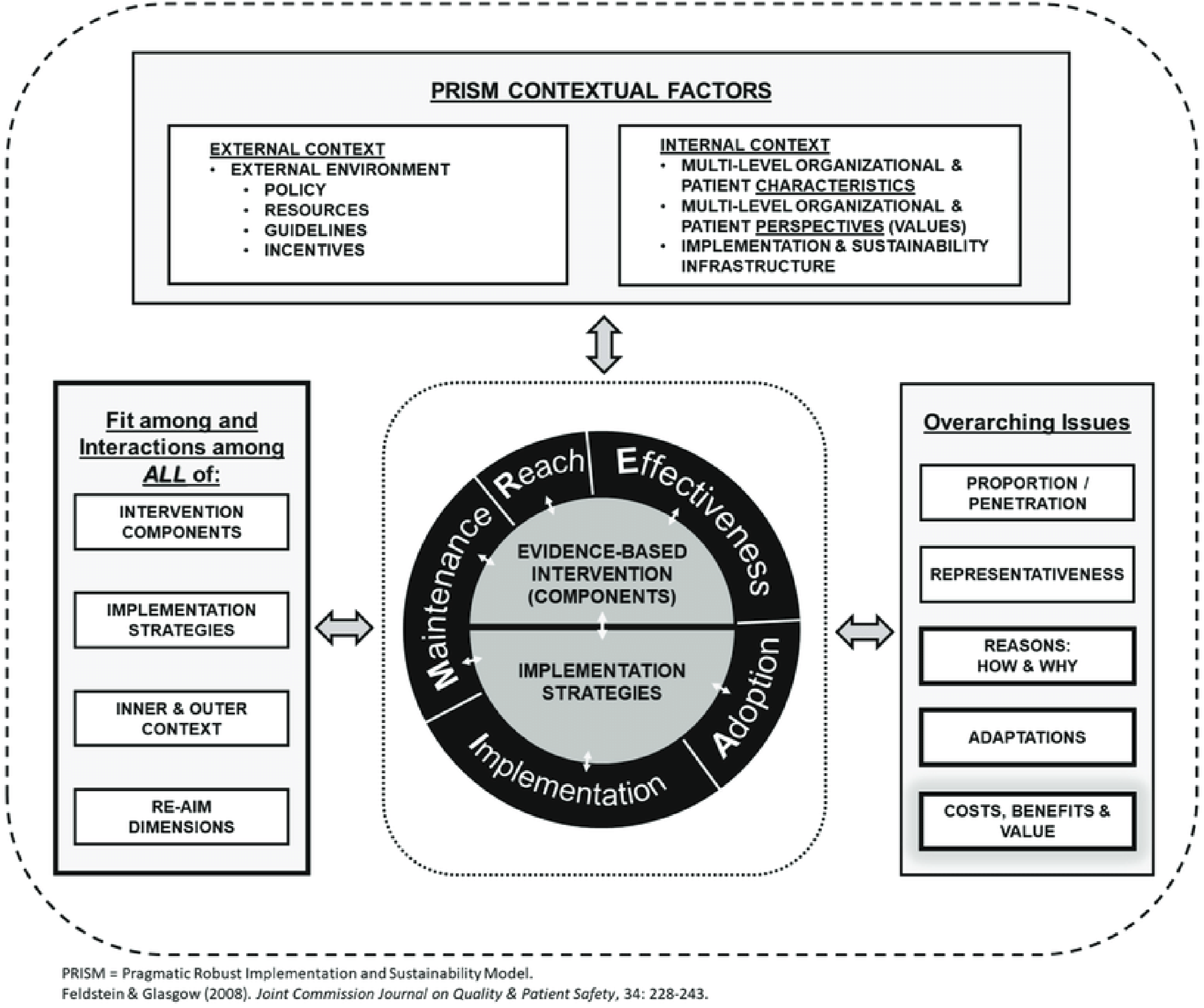
Supplemental Material
Supplemental Material - LM Initiative Success at the Institutional Level Through the RE-AIM Approach: 12 Tips and Implementation Science Strategies
Supplemental Material for LM Initiative Success at the Institutional Level Through the RE-AIM Approach: 12 Tips and Implementation Science Strategies by Hugo Ortega, MD, Christina Tache, MD, Gabrielle Bachtel, and Gia Merlo, MD, MBA, MEd in American Journal of Lifestyle Medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.