
Abstract
The Transtheoretical Model of Change identifies key stages in behavior change, including a maintenance stage occurring when a behavior has been upheld for at least 6 months. Health and wellness coaching has demonstrated support for health behavior change, but maintenance of gains has received little attention. Our rapid systematic literature review characterizes both the research exploring sustained gains with health and wellness coaching and what is known about sustained gains after the completion of a health and wellness coaching engagement. Guided by The Cochrane Rapid Reviews Methods Group “Interim Guidance,” we drew 231 studies from the 2018 and 2020 Sforzo et al “Compendium of the health and wellness coaching literature,” and “Addendum…” appendices. Initial screening and coding for inclusion and exclusion criteria yielded 28 studies for data extraction. We examined studies across outcome categories (physiological, behavioral, psychological, and health risk assessment) to determine whether outcome measures were: not sustained; partially sustained; fully sustained; or improved from immediate post-intervention to a later follow-up period. Twenty-five of the 28 studies reviewed demonstrated partially, or fully, sustained or improved outcomes in one or more variables studied, with sustained gains demonstrated across outcome categories, strengthening confidence in HWC as a facilitator of lasting change.
“With growing rates of chronic disease, and an ever increasing push towards lowering healthcare costs, exploring the effectiveness of emerging interventions such as HWC is critical.”
Background
Health and wellness coaching (HWC) is an emerging profession supporting health behavior change. As described in the National Board for Health and Wellness Coaching’s (NBHWC) Health & Wellness Coach Scope of Practice:
1
Health and wellness coaches engage individuals and groups in evidence-based, client-centered processes that facilitate and empower clients to develop and achieve self-determined, health and wellness goals. Coaches assist clients to use their own insight, personal strengths, and resources to set goals, commit to action steps, and establish accountability in building an envisioned healthy lifestyle. In this way, coaches empower clients through encouragement, exploration, the mobilization of internal strengths, the identification and utilization of external resources, and through the support and development of self-management strategies for executing sustainable, healthy lifestyle changes.1(para1)
Several systematic and integrative literature reviews, ranging in size from 13 to 219 studies, and including either only RCTs, or varied quantitative and qualitative methodologies, have explored outcomes of health and wellness coaching.2-6 The studies explored HWC across a range of conditions and diagnoses, including cancer, diabetes, heart disease, hypertension, obesity, and wellness, among others. Collectively, these reviews point to HWC as a promising and/or favorable intervention supporting beneficial effects on “patients’ physiological, behavioral and psychological conditions and … social life.”2(p147) They demonstrate an impact of HWC on prevention, as well as improved management, of chronic conditions.
The Transtheoretical Model of Change (TTM) is a well-researched model identifying 5 stages as key to lasting behavior change: precontemplation, contemplation, preparation, action, and maintenance. 7 The maintenance stage is said to occur when a behavior has been continued, or maintained, for at least 6 months.
Application of the TTM is part of the process of HWC. 8 Clients typically enter a coaching relationship in the earlier stages of the change process: sometimes in precontemplation, but more likely in contemplation or preparation related to self-identified goal(s). 9 The coaching process is designed to support movement through the stages of the TTM, ideally to the maintenance stage of change. 8 However, some research has documented that certain behavior change (e.g., weight loss) can be marked by frequent relapse, 10 and some studies have demonstrated that combining behavior therapy with other varied, ongoing interventions or “maintenance” activities may be more effective in supporting maintenance than behavior therapy, such as HWC, alone.11,12 Most literature reviews of HWC to date2-6 were based largely on outcomes measured at the completion of HWC interventions and did not explore whether gains made as a result of coaching were sustained over time.
Dejonghe et al published a systematic literature review, through June, 2015, on the long-term effectiveness, or maintenance of gains, of health coaching in rehabilitation (of health conditions) and prevention. They identified 14 randomized controlled trials (RCTs) each with follow-up of at least 24 weeks (6 months) after the end of the intervention period. 13 6 of these studies—3 prevention and 3 rehabilitation—demonstrated “statistically significant long-term effectiveness” of coaching.13(p1643) Dejonghe et al urged further study of long-term outcomes of HWC.
Health and wellness coaching can be variously defined in the research literature, making studies difficult to compare.6,14,15 The Wolever et al definition was derived from a systematic review of the literature on health and wellness coaching (see Box 1 below) and defines both “conceptual and interventional components” of coaching.15(p51) Use of this clear and widely accepted definition of health and wellness coaching in further study of long-term outcomes of HWC will augment generalizability of findings about sustained gains made as a result of coaching. Health and wellness coaching [is]: A patient-centered approach wherein patients at least partially determine their goals, use self-discovery or active learning processes together with content education to work toward their goals, and self-monitor behaviors to increase accountability, all within the context of an interpersonal relationship with a coach. The coach is a healthcare professional trained in behavior change theory, motivational strategies, and communication techniques, which are used to assist patients to develop intrinsic motivation and obtain skills to create sustainable change for improved health and well-being. Source: Wolever et al15(pp51-2)BOX 1: Definition of Health and Wellness Coaching (Wolever et al.
15
)
Our rapid systematic literature review utilizes an operationalized definition of HWC based on the widely-accepted Wolever et al 15 definition. Our review explores what is known about health and wellness coaching and sustained gains from the HWC research literature prior to 2019. Additionally, our review expands on the Dejonghe et al study 13 by looking broadly at the HWC literature, including a range of study designs, not only RCTs. It further expands on the Dejonghe et al study by exploring sustained gains over any period of time, not limited to the 6 months or more characterizing the maintenance stage in the TTM. 7
Key Research Questions
How can we characterize the body of literature exploring sustained gains with health and wellness coaching? What is known about sustained gains for clients after the completion of a health and wellness coaching engagement?
Methods
There is no single approach to a rapid review. The Cochrane Rapid Reviews Methods Group, 16 in their “Interim Guidance” document, provides the following working definition from Hamel et al: “A rapid review is a form of knowledge synthesis that accelerates the process of conducting a traditional systematic review through streamlining or omitting specific methods to produce evidence for stakeholders in a resource-efficient manner.”17(p74) Our literature review constitutes a rapid systematic review primarily because we use a single database. We also use some, but not all, of the methods recommended by the Cochrane Rapid Reviews Methods Group, in their “Interim Guidance” document. 16
Database
The database for our rapid systematic review comprised Appendix A from both the Sforzoet et al 6 “Compendium of the health and wellness coaching literature” and the Sforzo et al 5 Addendum to this “Compendium.” We chose these sources as our database because the “Compendium” was based on a systematic review process, using the widely accepted Wolever et al 15 definition of HWC, and we saw no need to repeat the comprehensive search that Sforzo et al5,6 had completed. The Sforzo et al. Compendium and Addendum did not systematically include data on follow-up after the immediate post-intervention data collection (our interest) so we had to search the articles in their database for those meeting our inclusion criteria. A subsequent Sforzo et al compendia project (currently underway) will include collection of follow-up data from studies published since the 2020 Addendum (G. Sforzo, personal communication to K. Smith, January 14, 2022), so we did not see a need to search the literature subsequent to that publication.
To understand the database we used, we briefly describe here the Sforzo et al5,6 methods: • The Wolever et al
15
definition of health and wellness coaching was operationalized (see Box 2, below) for inclusion of articles in the identification of a compendia of literature on HWC.6(p438) • The literature was gathered via a systematic review process, was peer-reviewed and in the English language.6(pp436-438) • The Sforzo et al search strategy was developed by a professional librarian and used 3 databases: PubMed, CINAHL via EBSCO, and PsycInfo via ProQuest.5,6 The syntax for each of these searches is found in Appendix C of the 2018 Compendium (available at http://journals.sagepub.com/doi/suppl/10.1177/1559827617708562). • The search was further described as follows: “The terms searched were limited to the title or abstract fields within each database. Furthermore, article acquisition from the personal libraries of our authors, and reference daisy-chaining, were added to ensure a more complete HWC review.”6(p438) • The 2018 review included literature from 1990 forward since the thorough Wolever et al
15
review had not identified any HWC articles before that date.6(p438) • The 2020 review was limited to literature published subsequent to that collected for the 2018 article.
5
• The aim of the compendia was to be inclusive, so neither search was limited to RCTs, a common focus of systematic reviews.
For a full description of the Sforzo et al search strategy, please see the original publications.5,6 [The] 5 criteria for inclusion coding were the following: HC1: Training: Health coach was trained and used behavior change theory and coaching processes. HC2: Professionals: Health coach was a trained health care professional. HC3: Goals: Patient partially or wholly determined behavior change or health goals. HC4: Accountability: Patient progress was monitored. HC5: Relationship: Patient-clinician relationship provided opportunity to develop (1 coach per patient and at least 3 sessions). Ultimately, inclusion was at the discretion of the reviewer in that not all criteria had to be met for an article to be retained. For example, a study sometimes met most criteria but coaching was conducted using well-trained peers or medical assistants; after deliberation, reviewers often chose to retain these as HWC despite not meeting the HC2 criterion. This was deemed acceptable in the spirit of not excluding articles describing a HWC process our expert reviewers otherwise deemed appropriate. Source: Sforzo et al.6(p439) BOX 2: Sforzo et al.
6
Operational Definition of HWC
The Sforzo et al. “Compendium of the health and wellness coaching literature” 6 and Addendum to the “Compendium” 5 each include several appendices. Appendix A for each of these articles consists of a database listing all data-related research studies identified in the search, and identifies key characteristics and findings of each study on health and wellness coaching. The Sforzo et al.5,6 Appendix A are available online at https://journals.sagepub.com/doi/suppl/10.1177/15598276231180117 (2018) and https://journals.sagepub.com/doi/suppl/10.1177/15598276231180117 (2020). Appendix A of the 2018 Sforzo et al. Compendium 6 included 150 articles; Appendix A of the 2020 Addendum 5 included 81. We combined these 2 sets of articles into a database of 231 peer-reviewed data-based articles for our search.
Search Strategy
The Sforzo et al.5,6 Appendix A databases included peer-reviewed, data-based articles meeting a modified version of the Wolever et al 15 definition of HWC.
We reviewed the 231 primary articles from the database with the following inclusion and exclusion criteria: • Inclusion: any completed study exploring client-related outcomes including a follow-up data collection (quantitative) subsequent to the immediate or first post-intervention data collection. • Exclusion: Study designs, systematic reviews, meta-analysis, studies that did not explore client outcomes of coaching, and, of course, studies that did not include follow-up data collection subsequent to an initial post-(coaching) intervention data collection. (Note: We retained all other study designs, including case studies.)
Our search process is diagrammed in Figure 1. PRISMA Flow Diagram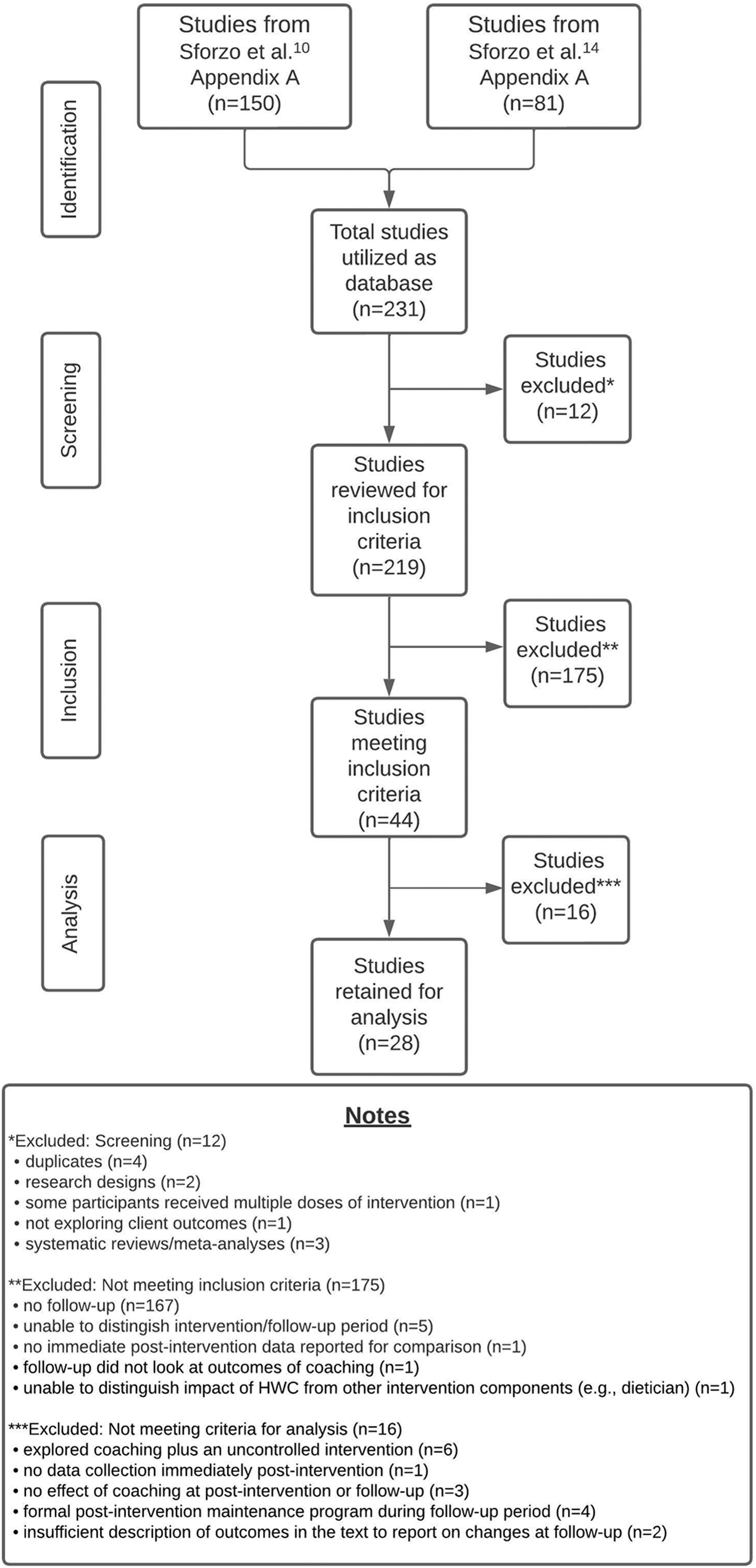
Our research team divided the database to each gather and screen a portion of the full-text articles for analysis. In the screening process, we identified and excluded 12 articles, as indicated in Figure 1. This left us with 219 articles in the database to review for our study.
Five study team members reviewed articles for inclusion criteria (EA, RDM, BI, MS, KS); 2 members of the research team were assigned to review each article. These reviewers were blind to each other’s reviews. We searched the entire article to assure we understood the length of the coaching intervention and whether any data collection had occurred subsequent to the immediate or first post-intervention data collection. While we used terms such as “follow-up, long-term, and maintenance” to assist us in these efforts, in the end we based inclusion on a full understanding of the intervention, its length, and the data collection time points described. In the process of completing reviews, we noticed that there were varied approaches to the follow-up period and decided to re-review to separately track articles meeting inclusion criteria in the following categories: • No coaching between intervention and follow-up • Some coaching may have occurred between intervention and follow-up, but at a lesser frequency (e.g., optional sessions or maintenance coaching) • Other (e.g., first data collection was significantly separate in time from end of the intervention; only 1 arm of a study had a follow-up, etc.)
Reviewer decisions on inclusion were compared: we achieved 78.5% (172/219) agreement. One article was identified by 2 reviewers as “unable to ascertain” and was sent to the study team for review. At this stage, 47 articles coded differently by 2 reviewers were reviewed by a third member of the study team. In these cases, agreement of 2 of the 3 reviewers was adhered to. If 2 of the 3 did not agree, the article was brought to the study team for discussion and final decision; this occurred 18 times.
Of the 219 articles reviewed, 44 met study inclusion criteria of a follow-up data collection subsequent to the immediate or first post-intervention data collection (see Figure 1 for explanation).
Data Extraction
Once we had identified the articles for inclusion in our study, a single reviewer (EA) coded and extracted data from included articles and a second reviewer (LC) reviewed the articles and the coded/extracted data to “check for correctness and completeness of extracted data,” following the guidance for data extraction from the Cochrane Rapid Reviews Methods Group, in their “Interim Guidance” document.16(p2) Discrepancies between the initial and second review were discussed and resolved by those reviewers.
Coding Key for Follow-up Study Variables Extracted
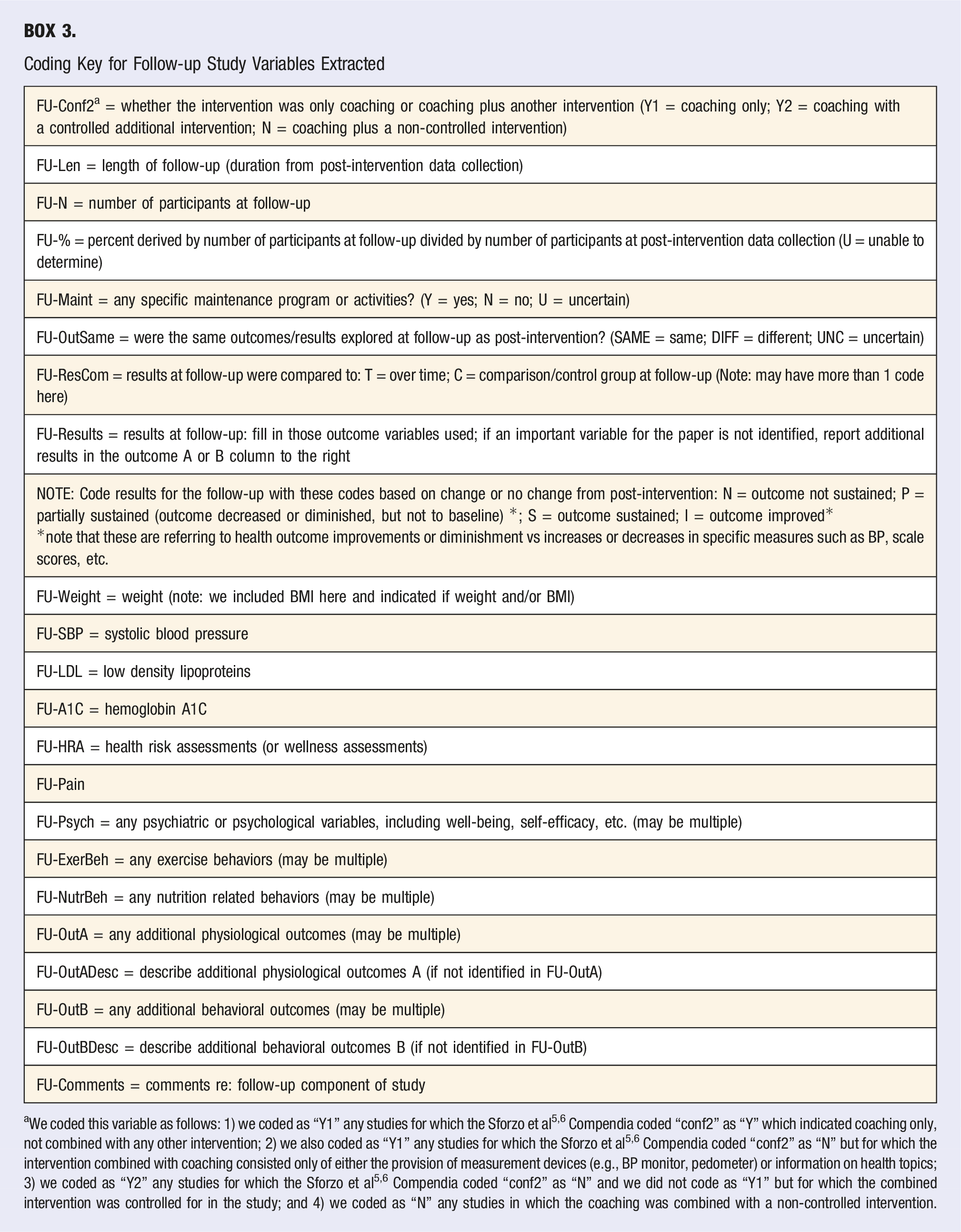
aWe coded this variable as follows: 1) we coded as “Y1” any studies for which the Sforzo et al5,6 Compendia coded “conf2” as “Y” which indicated coaching only, not combined with any other intervention; 2) we also coded as “Y1” any studies for which the Sforzo et al5,6 Compendia coded “conf2” as “N” but for which the intervention combined with coaching consisted only of either the provision of measurement devices (e.g., BP monitor, pedometer) or information on health topics; 3) we coded as “Y2” any studies for which the Sforzo et al5,6 Compendia coded “conf2” as “N” and we did not code as “Y1” but for which the combined intervention was controlled for in the study; and 4) we coded as “N” any studies in which the coaching was combined with a non-controlled intervention.
Because of widely varied study designs, statistical analyses, and reporting approaches, and since we were not doing a meta-analysis, in reporting results at follow-up, we chose to extract information reported primarily in the text of each article and its abstract; we specifically chose not to interpret tabular material ourselves. In general, we reported results in relation to a comparison group, if used, and if statistically significant. We chose not to report author-reported “trends.” Further, for some variables the data provided in the text was insufficient for us to draw conclusions, and thus we did not extract data or report on these. While this approach may in some measure impact the thoroughness of results reported here, we intended to minimize the risk of interpretation on our part as we extracted data from each reviewed study. At the same time, in our choice to use the author’s own characterization of findings whenever possible, we recognize several limitations: this approach may have introduced some bias as well as some differing interpretation of terminology regarding sustained gains.
In extracting and reporting on whether or not gains were sustained, we used 4 categories, each of which was, in most cases, based on comparison to the immediate post-intervention outcomes. The 4 categories related to whether, and the extent to which, gains were sustained were as follows: a) gains not sustained; b) gains partially sustained (diminished or decreased at follow-up compared to post-intervention, but not back to baseline); c) gains sustained (fully) at follow-up; and d) gains improved at follow-up compared to post-intervention. These categories of “gains” refer to health outcome improvements or diminishments as opposed to increases or decreases in specific measures such as BP, scale scores, etc. This distinction is important as, for example, an increase in blood pressure over time is an increased measurement but a diminished or decreased health outcome; similarly, a decrease in depression scores is a decrease in the measurement but an increase in the health outcome.
Sometimes we easily extracted data from the text of an article on whether or not gains were maintained. This was straightforward when a study clearly compared intervention group outcomes over time. At other times, this was less straightforward. As an example, in some studies comparisons were made to a control group over time vs simply to the immediate post-intervention period. In this case, if a significant difference was reported between intervention and control group at the immediate post-intervention period, but no significant difference was reported at follow-up, we reported this as gains not sustained. We did this even though, technically, the intervention group on its own might have demonstrated sustained gains. A similar challenge occurred when a study combined analysis of group and time. A review of tabular data was not always a clear way to resolve questions of interpretation. Consequently, we made our best judgment of how outcomes for the intervention group had changed from post-intervention to follow-up based on what authors reported in the text. Further, if individual measures were also reported as part of a composite measure, we only extracted data on the composite measure so as not to over-report on variables.
Once this process was complete, we merged data collected related to follow-up with most of the extant data about each included study from the Sforzo et al. Compendia Appendix A databases.5,6 The only columns we did not carry over from the Compendia were: “inclusion”; “comments” (on inclusion); “qual results”; and “comments” (on results). This gave us a full descriptive database for each article meeting our study criteria.
Analysis
To report on study outcomes, 2 researchers (EA, MS) jointly sorted outcome variables into 4 categories: physiological (e.g., weight, BP, and other measurements); behavioral (e.g., nutrition or fitness behaviors); psychological (any measure or self-report of psychological functioning or attitudes); and health risk assessment. (Additional examples of variables in each category are provided in the notes for Table 3.) 2 reviewers (EA, MS) separately did all counts to create tables and then compared for accuracy. We used Microsoft Excel to obtain statistics, where reported.
Quality Assessment
The Sforzo et al5,6 Compendia databases include data relevant to assessing study quality; these data are included in our full descriptive database. We did not conduct a separate risk of bias or certainty of findings assessment.
Findings
As detailed in Figure 1, of the 219 articles initially reviewed, 44 met study inclusion criteria of a follow-up data collection subsequent to the immediate or first post-intervention data collection. Of these 44, six studies explored coaching plus an uncontrolled additional intervention, and we did not examine these further due to potential confounding18-23 (note: the 2019 Eisenberg study 19 was listed as 2017 in the Sforzo et al5,6 Compendia, as date first published online). One study did not collect data immediately post-intervention, 24 and 3 studies25-27 found no effect of coaching at either the immediate post-intervention period or a later follow-up (notes: in the Alley et al 25 study, we looked at the coaching plus tailoring group vs only tailoring group; the Viester et al 27 2015 study was listed as 2014 in the Sforzo et al5,6 Compendia, as date first published online), so we did not analyze these studies further. Four studies had a formal post-intervention maintenance program during the follow-up period,28-31 so we did not include these studies in further analysis, although we did retain several studies that had optional maintenance activities. An additional study 32 included an arm with 6 months of coaching, and an arm with 3 months and a maintenance phase, but we retained this study for further analysis, looking at the third arm which had 3 months of coaching and did not have a maintenance phase. Two studies did not have sufficient description of outcomes in the text to report on changes at follow-up,33,34 so we did not report further on these. This left us with 28 studies for further analysis.
Description of Studies Retained for Analysis
Changes in Study Outcomes Post-intervention to Follow-up (Best Outcome) a .
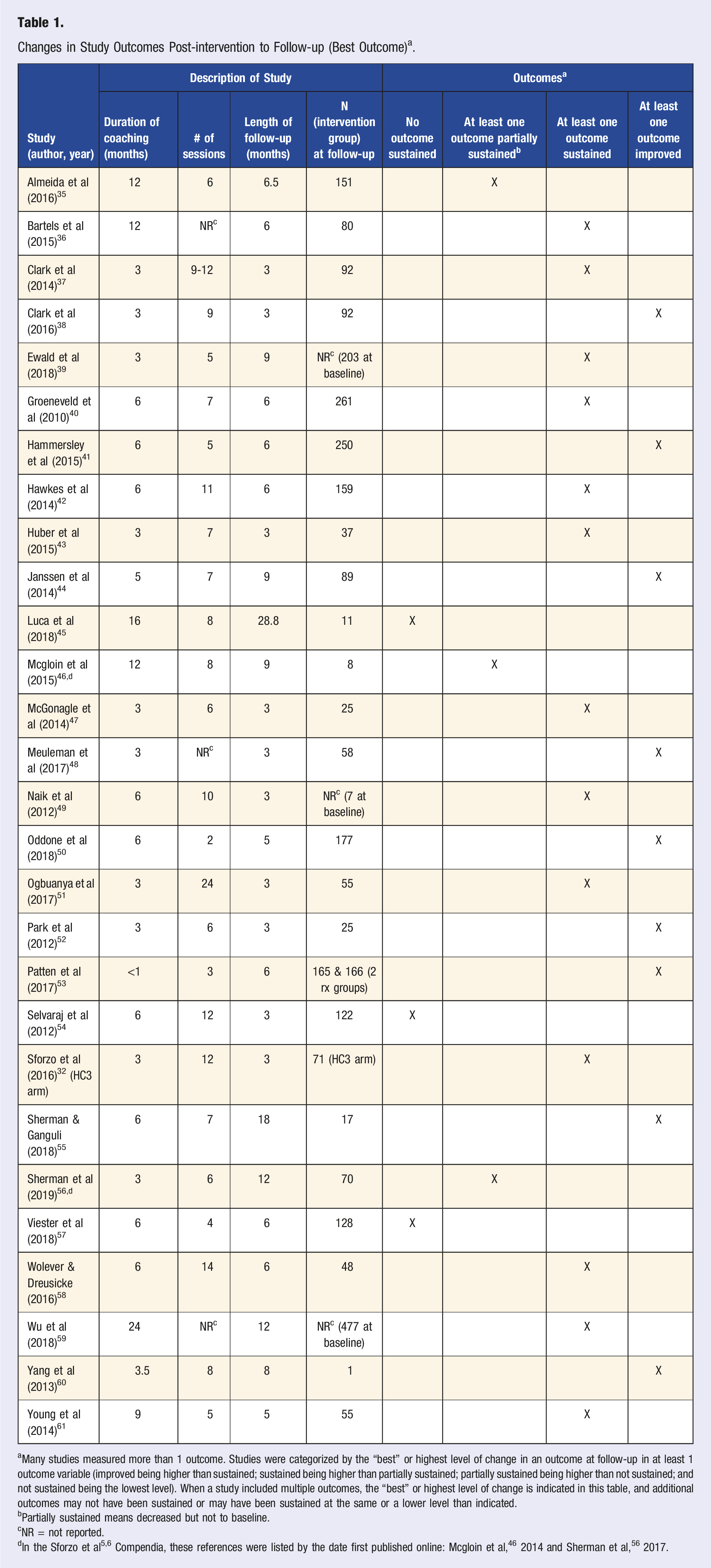
aMany studies measured more than 1 outcome. Studies were categorized by the “best” or highest level of change in an outcome at follow-up in at least 1 outcome variable (improved being higher than sustained; sustained being higher than partially sustained; partially sustained being higher than not sustained; and not sustained being the lowest level). When a study included multiple outcomes, the “best” or highest level of change is indicated in this table, and additional outcomes may not have been sustained or may have been sustained at the same or a lower level than indicated.
bPartially sustained means decreased but not to baseline.
cNR = not reported.
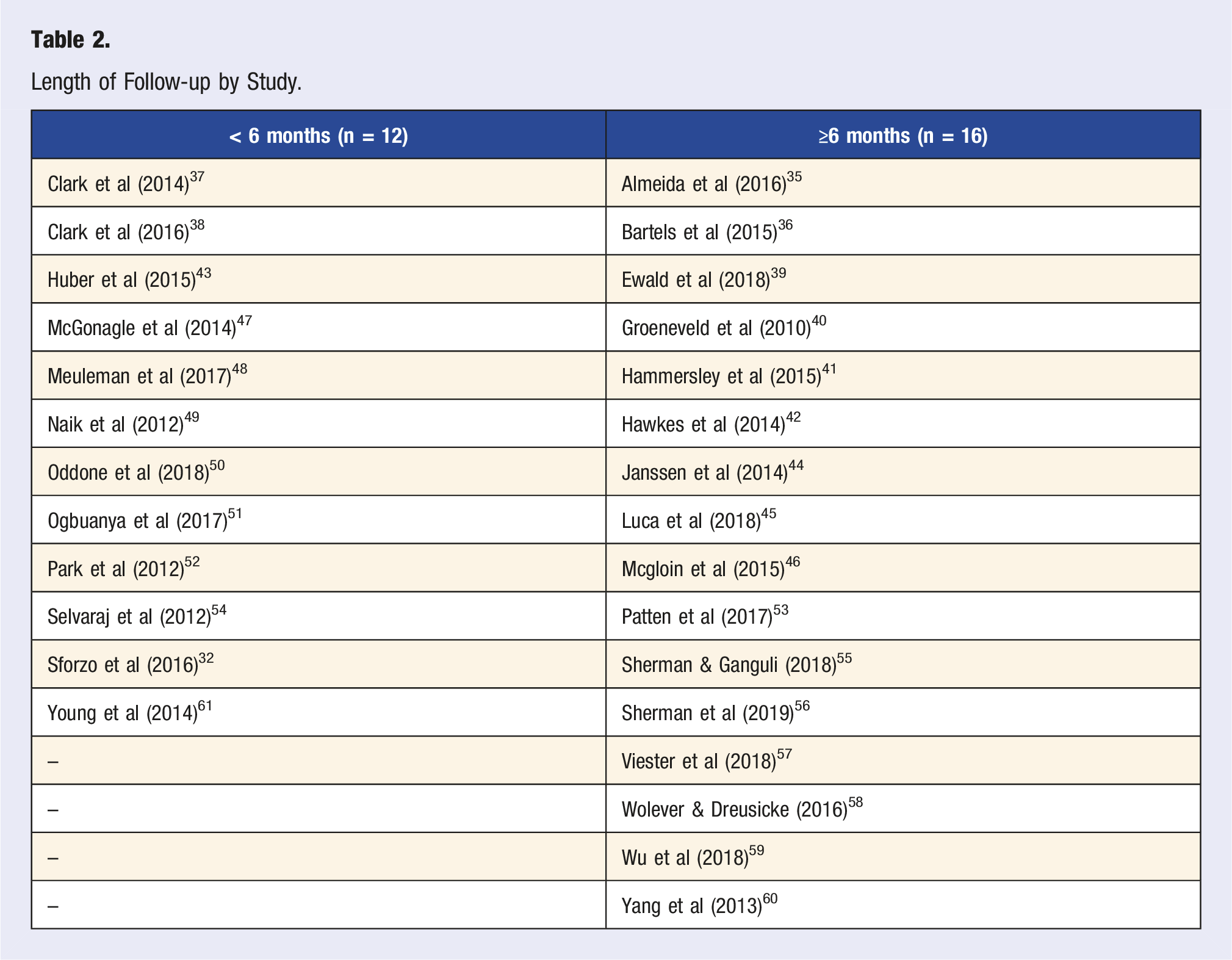
Length of Follow-up by Study.
One study 53 had more than 1 intervention group (we are not including Sforzo et al 32 in this group for reasons described above), and 3 studies did not report the number of intervention participants at follow-up. Excluding these, the remaining 24 studies had a mean of 87 intervention participants at the latest follow-up (SD = 71.23; range = 1-261).
Best Outcomes
Many studies measured more than 1 outcome. Table 1 identifies the best, or highest, level of change in any outcome variable at follow-up. Our approach to categorization of the “best” is detailed in the first note in Table 1. When a study included multiple outcomes, additional outcomes may not have been sustained or may have been sustained at the same or a lower level than indicated for the best outcome in Table 1.
Table 1 illustrates that 3 studies had no outcome sustained over time, while 3 had at least one outcome partially sustained, 13 had at least 1 outcome sustained, and nine had at least 1 outcome measure that improved over time. A visual inspection of Table 1 does not suggest any relationship between the duration of coaching, the numbers of sessions of coaching, the length of follow-up, or the combination of duration of coaching and length of follow-up, or number of participants, and whether, or the extent to which, gains achieved in the intervention period were sustained.
Categories of Outcomes
Changes in Study Outcomes a Post-intervention to Follow-up (by Study).
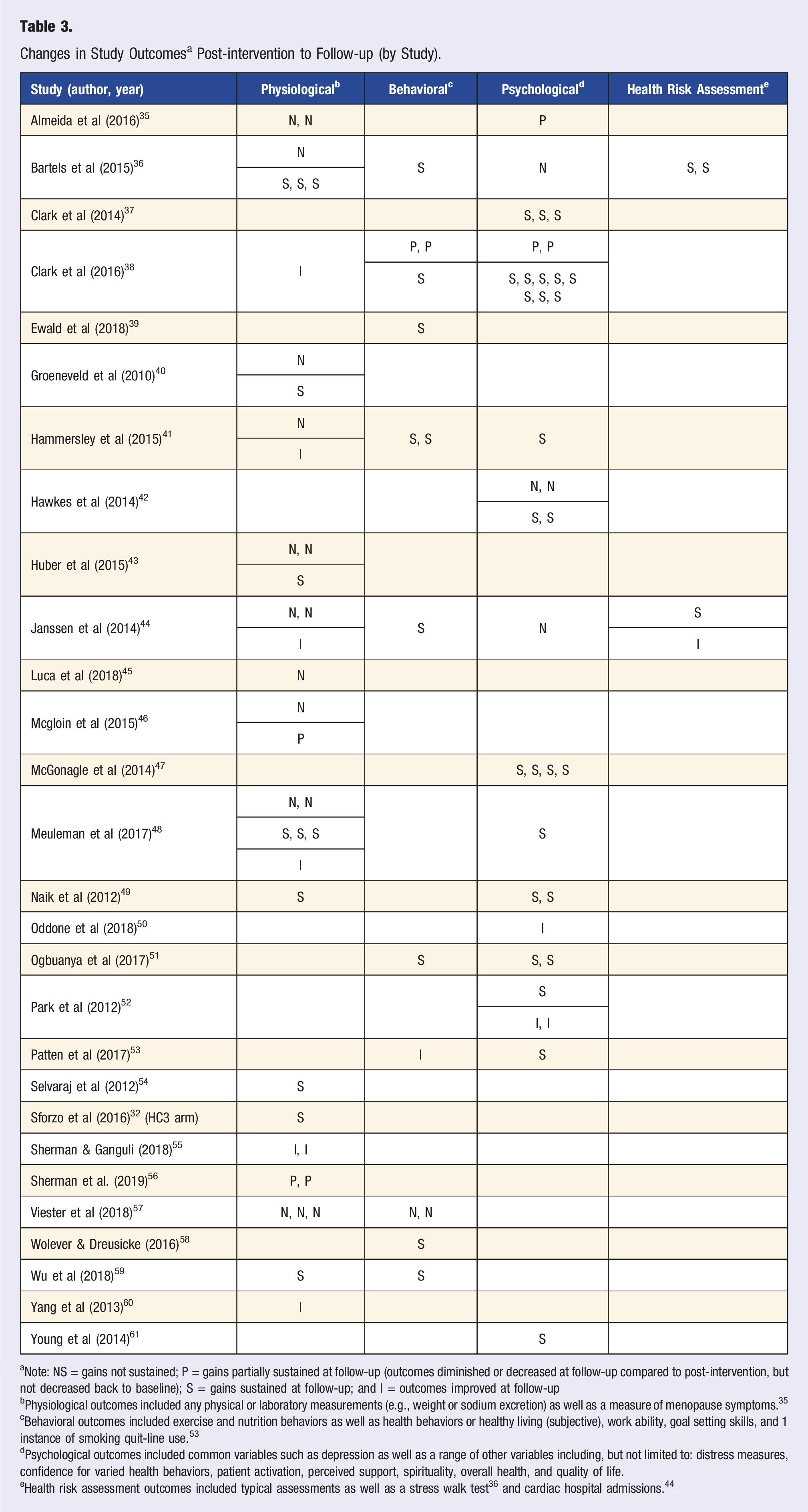
aNote: NS = gains not sustained; P = gains partially sustained at follow-up (outcomes diminished or decreased at follow-up compared to post-intervention, but not decreased back to baseline); S = gains sustained at follow-up; and I = outcomes improved at follow-up
bPhysiological outcomes included any physical or laboratory measurements (e.g., weight or sodium excretion) as well as a measure of menopause symptoms. 35
cBehavioral outcomes included exercise and nutrition behaviors as well as health behaviors or healthy living (subjective), work ability, goal setting skills, and 1 instance of smoking quit-line use. 53
dPsychological outcomes included common variables such as depression as well as a range of other variables including, but not limited to: distress measures, confidence for varied health behaviors, patient activation, perceived support, spirituality, overall health, and quality of life.
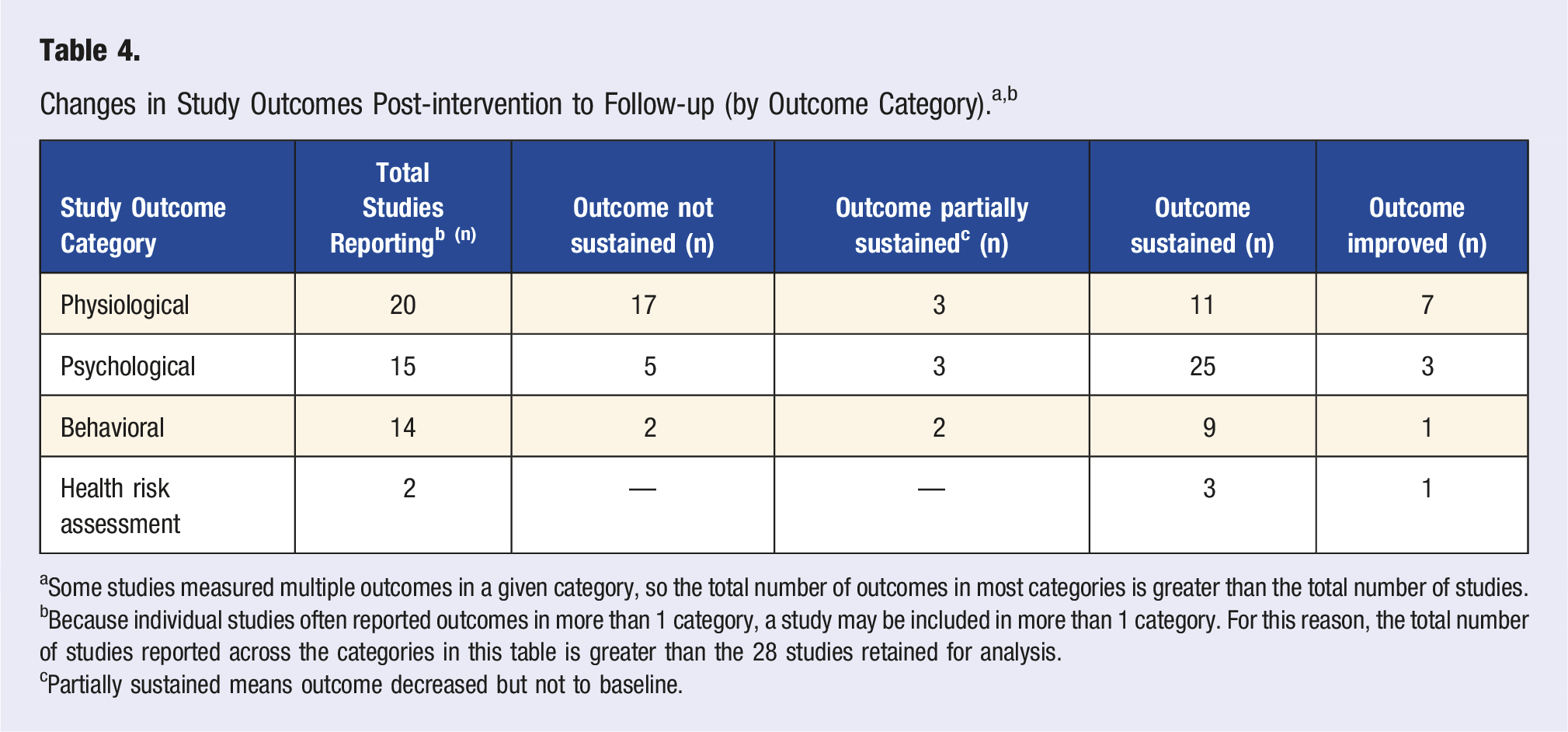
aSome studies measured multiple outcomes in a given category, so the total number of outcomes in most categories is greater than the total number of studies.
bBecause individual studies often reported outcomes in more than 1 category, a study may be included in more than 1 category. For this reason, the total number of studies reported across the categories in this table is greater than the 28 studies retained for analysis.
cPartially sustained means outcome decreased but not to baseline.
Discussion
Best Outcomes
Of the 12 studies in this review exploring sustained gains at less than 6 months (see Table 1), 11 (91.67%) demonstrated some gains made at post-intervention that were partially sustained, and/or sustained, and/or, in some cases, improved, over the follow-up period. No other review to date has explored gains sustained at less than 6 months after an HWC intervention. While these findings are very encouraging, the TTM suggests that a behavioral change can only be considered “maintained” if it continues for at least 6 months. 7 For this reason, while improvements were sustained in many variables in these 11 studies, clear conclusions cannot be drawn about gains maintained. Using the TTM as a framework, 7 future research on outcomes of health and wellness coaching might ideally include follow-up data collection at 6 or more months after completion of the intervention.
Of the 16 studies in this review exploring sustained gains at 6 or more months, 57 14 (87.5%) demonstrated some gains that were either partially sustained, sustained and/or, in some cases, improved over the follow-up period. This is in contrast to the findings of the Dejonge et al systematic review of randomized controlled studies of the long-term effectiveness of health and wellness coaching which demonstrated maintenance of gains in only 6 of 14 studies examined (42.86%). 13 The Dejonge et al review differed from the current review in several ways. Dejonge et al included: 1) RCTs published up to June, 2015; 2) only studies with a post-intervention follow-up at 6 months or later, as a time-frame consistent with the “maintenance” stage of change in the TTM 7 ; and 3) they did not use as specific a definition of coaching as was used in our review. Likely due to differing inclusion criteria and databases used, there was no overlap of the studies in the Dejonge et al systematic review and the current review. The current review, including varied study designs contributes a new and broader perspective to the literature, expanding our understanding of maintenance of gains with HWC.
Ten of the studies we reviewed reported that some of the gains achieved by the end of the coaching period were not sustained over time while other outcomes were partially sustained, sustained, or improved (see Table 3). This raises a question of whether certain outcomes might be more challenging to sustain than others. If this were true, these outcomes might need additional attention in the coaching process and might also benefit from 1 or more of the following: 1) offering a maintenance period of coaching at a reduced intensity or frequency; 2) offering specific maintenance (non-coaching) activities; and/or 3) assuring specific attention to planning with a client how to maintain gains before ending the coaching engagement.
Fifteen of the 28 studies we reviewed reported that all gains achieved at the immediate post-intervention period were sustained, to some degree, or improved upon at the later follow-up (see Table 3). This is an encouraging finding and suggests the value of continued exploration of sustained or maintained gains in coaching, perhaps exploring specific factors related to these outcomes.
While we had not anticipated this finding, 9 studies we reviewed reported improvements in at least 1 outcome from post-intervention to a later follow-up (see Table 3). Improvements were documented in physiological, psychological, behavioral, and health risk assessment outcomes, though not necessarily all in the same study. A pilot study of ten weeks of leadership coaching found that some clients needed time to consolidate new learning before it was demonstrated as new behaviors. 62 The authors suggest that theories of transformational learning may explain the time needed for clients to digest new awareness and implement behavioral changes. A systematic review of coaching within organizations also found that, when studied, transformation among coaching clients continued to evolve beyond the duration of active coaching. 63 Longitudinal research, including 6-12 months of follow-up, may yield greater understanding of not only gains sustained for some period of time, or maintained for at least 6 months, but also possible delayed effects of coaching.
We were surprised to note that only 3 of the 28 studies analyzed in this review found no gains at all sustained from the post-intervention period to a later follow-up.45,54,57 These studies varied in the duration of coaching (6 months54,57 and 16 months 45 ), and the duration of follow-up (3 months, 54 6 months, 57 and 28.8 months 45 ). Of note, it was primarily improvements in physiological variables that were not sustained during the follow-up in these studies, though 2 behavioral variables were not sustained in 1 study. 57
Categories of Outcomes
Examining Table 4, it appears that, while physiological variables were sustained in some instances, and even improved, they were more likely to not be sustained (44.74%) than psychological (13.89%), behavioral (14.29%), or HRA variables (0%). At the same time, physiological variables were more often improved from post-intervention to follow-up than psychological and behavioral: 18.42% of physiological variables examined from post-intervention to follow-up improved over time as compared to 8.33% of psychological variables and 7.14% of behavioral variables. One in 4 (25%) of health risk assessments improved from post-intervention to follow-up. Also, across all studies, it appears that, proportionally, psychological and health risk assessment variables were most likely to be sustained (69.44% and 75%, respectively). This raises interesting considerations for future research. For example: What types of variables yield most useful information on lasting change? Might psychological changes (e.g., in readiness to change) precede or predict behavioral changes? Might behavioral changes precede or predict improved physiological outcomes? What factors could contribute to a change in overall health risk status? Are certain variables more relevant for measuring meaningful change for specific conditions?
The Lin et al study, 29 not included in our analysis here, raises another question about interpretation of findings. In this study, numerous nutrition behaviors (intake in varied categories), and several physiological parameters, improved as a result of the intervention including coaching, and some of these improvements were at least partially sustained at the follow-up. However, while the changes identified at the immediate post-intervention period did meaningfully impact weight and blood pressure, and did demonstrate an improvement in the DASH score, they “did not meet the DASH nutrients targets or food group guidelines.”29(p8) This raises the important question of what might be considered a clinically meaningful change. While beyond the scope of the current review, for any study of health and wellness coaching finding improvements, including sustained improvements, a close look should be taken to explore the clinical significance of these changes. Future research would beneficially report not only improvements on outcome measures but also report effect sizes, and discuss clinical significance.
Maintenance Period
Twenty-five of the 28 studies examined in this review reported 1 or more outcome(s) sustained to some degree or improved, excluding only 345,54,57 (see Table 3). Sixteen of the studies analyzed in this review examined follow-up outcomes at 6 months or longer after the end of the coaching interventions, a period equal to the “maintenance” stage of the TTM, 7 and 14 of these found 1 or more outcome(s) sustained to some degree or improved, excluding only 2.45,57 Janssen et al suggest that after a coaching intervention, clients “may need ongoing attention and guidance, for example, in the form of (Internet) booster sessions, as long-term consolidation of changes is arduous.”44(p308) However, other research reports that transitional support did not impact maintenance of gains.36(p7) Four studies28-31 we initially identified for inclusion—but did not include in our analysis—included a formal “maintenance” period or “post-core” period in which a reduced amount of coaching or different ongoing approach to client support was provided (the Sforzo et al study 32 also included an arm with this configuration). This phenomenon suggests that some health and wellness coaching interventions may be devised to provide an initial intensive intervention, followed by some lesser support over a longer period of time, perhaps until maintenance of gains may have occurred. As an example, the highly successful Diabetes Prevention Program (DPP), a multi-pronged intervention that includes coaching, does factor in support for a period of time to encourage maintenance of gains. 11 An explicit and more detailed look at studies providing this two-stage approach to support clients in reaching a maintenance stage of change would be interesting and might have useful implications for HWC in practice.
Although a somewhat different question, we wonder whether, prior to terminating a coaching intervention, coaches might purposely assist clients in identifying strategies and supports they can make use of in order to promote sustaining and eventual maintenance of gains made during the intervention. In fact, the NBHWC coaching competencies (specifically competency 1.5.2) states that the coach will: “Assist in developing sustainable pathway forward and/or maintenance/relapse prevention plan including available support and resources.”8(p5) While a common, and expected, aspect of HWC, we do not have any way of knowing with certainty whether maintenance plans were explicitly discussed in the coaching provided in the studies reviewed. This might be valuable to explore in future research.
Summary of Findings
Only 3 of the 28 studies examined in this review found no sustained gains in any outcome.45,54,57 In nearly all (25 of 28) of the studies examined in this review, some gains made as a result of the coaching intervention were sustained (whether partially or fully). This was the case for 11 studies with follow-up periods of less than, as well as 14 with follow-up at greater than or equal to, 6 months, the period considered “maintenance” in the TTM. 7 In an interesting pattern, in nearly one-third of the studies (n = 9), some gains achieved by the end of the coaching period were not sustained over time, while other outcomes were partially sustained, sustained, or improved. In over half of the studies (n = 15), all gains reported at the end of the coaching intervention were either partially or fully sustained or improved upon at follow-up. And in approximately one-third of the studies (n = 9), improvement was demonstrated at follow-up in at least 1 outcome explored. Many (20 of 28) studies examined multiple outcomes, including outcome variables in varied categories: physiological, psychological, behavioral, and health risk assessment. Of note is that gains were sustained, and in some cases improved, across all categories of outcomes. While physiological variables were the most likely to not be sustained, physiological variables were also the most likely to improve from post-intervention to follow-up.
Strengths and Limitations
To our knowledge, this is only the second review to explore sustained or maintenance of gains for outcomes of HWC. One strength of this review was the use of the Sforzo et al.5,6 Compendia of health and wellness coaching literature as a database, providing some consistency in the definition of HWC 15 across the studies reviewed. A systematic approach was utilized in the review process and every stage of the coding and data extraction process was completed by 2 independent reviewers with disagreements resolved by a third reviewer or by consensus of the 2 reviewers extracting data.
The literature reported on in this review is notable for wide variety in outcome variables explored, length of the coaching intervention, length of the follow-up period, and type of analysis. Unlike Dejohnge et al, 13 which only explored RCTs, we included all primary study designs, from a case study to RCTs in this review.
As described in the methods section, because of widely varied study designs, statistical analyses, and reporting approaches, and since we were not doing a meta-analysis, in reporting results at follow-up, we chose to extract information reported primarily in the text of each article and its abstract; we specifically chose not to interpret tabular material ourselves. While this may in some measure impact the thoroughness of results reported here, we intended to minimize the risk of interpretation on our part as we extracted data from each reviewed study. At the same time, in our choice to use the author’s own characterization of findings whenever possible, we recognize several limitations: we may have introduced some bias as well as some differing interpretation of terminology regarding sustained gains.
Numerous studies reported on in this review had 1 or more control group(s); some of these had active controls. In this situation, because the control group is receiving an intervention that is also expected to provide some benefit, it can be especially challenging to realize comparative improvement in an intervention group. Where comparative improvement was evidenced, it provides particularly strong support for our positive findings of sustained gains related to HWC.
While our use of the Sforzo et al5,6 Compendia is in some ways a strength of this study—as described above—it also poses a limitation. Because the literature included was from 2019 and before, the included literature is not fully up-to-date. An updated compendium project is in process and is expected to report data on sustained gains (G. Sforzo, personal communication to K. Smith, January 14, 2022). While there is no reason to expect that a review of more recent research would lead to opposite findings from this review, an exploration of sustained gains in the updated database will be of value.
While a number of studies we reviewed demonstrated sustained gains, and some demonstrated improvement on select outcomes from immediate post-intervention to follow-up data collection, the clinical significance of each finding cannot be assured. For example, 1 study found an improvement in scores on a patient activation measure from post-intervention to later follow-up, but also reports that this change, while real, translated to a small effect size (Cohen’s D = .19) which “may not be clinically significant.”50(p1492) Many studies did not report effect sizes nor surmise regarding clinical significance of changes reported. Interpretation of the clinical significance of results would be enhanced if future research on HWC, and on sustained gains, included exploration of effect sizes for outcomes reported.
Conclusions
This rapid systematic literature review offers a valuable contribution to the field of HWC, offering evidence of the efficacy of HWC in sustaining gains beyond the active period of coaching. In many instances, and across physiological, behavioral, psychological, and HRA variables, studies reviewed found sustained effects, and in some cases improvements, over a follow-up period. This is particularly notable because with various other interventions—medication treatments for chronic conditions being a key example—beneficial effects are often not retained when an intervention is discontinued. This review suggests that HWC can support lasting behavior change and improved outcomes, sustained over time, even after the cessation of the intervention. This key finding suggests the unique value and important contribution HWC can make, for varied health conditions, as an emerging field in the healthcare arena.
Most of the studies reported here were not designed to focus specifically on whether gains were sustained. Consequently, interpreting data related to these outcomes was challenging. The field is sorely in need of future research designed to specifically examine the long-term effects of HWC. We offer several recommendations to this end. First, designing studies using a clear, widely accepted definition of coaching (such as the definition found in the Sforzo et al5,6 Compendia) will provide consistency in what is being researched (intervention) and may help explain why certain outcomes are found. Additionally, while we did not identify an impact related to duration of the coaching intervention on sustained or maintained gains, this question could be explored in future research to establish specific recommendations. Further, designing studies to explicitly explore sustained or maintained gains, specifically at a 6-month timeframe per the TTM 7 would be useful. Assuring that studies are powered for detection of sustained gains at a long-term follow-up would also be useful. Perhaps providing incentives to participants for completing a follow-up data collection should be considered as well. In these regards, funding agencies should provide support to incorporate follow-up data collection measures into study design, and should encourage explicit analysis of such. Finally, researchers might also carefully consider whether changes in psychological variables (e.g., readiness to change) would be expected to precede behavioral outcomes and, subsequently, physiological variables. Perhaps future studies could be designed to not only explore behavioral change or targeted physiological parameters but to explicitly explore the impact of coaching on all 3 levels of outcomes: readiness to change, health behaviors, and targeted physical or physiologic outcomes.
This study has implications for coaching practice as well. According to the Wolever et al definition, HWC should support “sustainable change for improved health and wellbeing.”15(p52) Similarly, NBHWC suggests that the goal of HWC is to support “lasting” changes in health behavior and outcomes. 64 To this end, coaches should assure that plans for termination of coaching include attention to supports, strategies, and resources that will promote maintenance of gains and relapse prevention. These can be individualized to each client, but might include the following: plans to innovate on new behaviors; plans to support others as a way to strengthen a commitment to a new behavior; plans to periodically set new goals; and plans for how to reinstitute new behaviors if a lapse occurs. 9
To encourage coaches to address support for maintenance of gains, coach training programs should emphasize the importance of maintenance/relapse prevention planning, a key coaching competency. 8 (NBHWC competency 1.5.2. States: “Assist in developing sustainable pathway forward and/or maintenance/relapse prevention plan including available support and resources.”8(p5)) Additionally, the programmatic design of any coaching intervention program might thoughtfully integrate some specific type(s) of support during the 6 months immediately post-coaching to support maintenance of gains. These approaches could include coaching at a gradually decreasing frequency; a transition from individual to group coaching support; email or text reminders; or other approaches designed to ease the transition from intensive coaching support to the independent maintenance of new health behaviors. A review of the literature to explicitly explore the structure of current coaching programs with a specific maintenance phase might provide fruitful suggestions for this process (see, for example, the Diabetes Prevention Program research 11 and several studies not meeting the inclusion for this review due to offering a formal maintenance phase intervention28-31).
With growing rates of chronic disease, and an ever increasing push towards lowering healthcare costs, exploring the effectiveness of emerging interventions such as HWC is critical. Numerous stakeholders—consumers, employers, program designers, investors, payers, health care providers, coaches, coach trainers, and more—will benefit from continued accumulation of evidence related to the impact of HWC on individual well-being, health risk reduction, and chronic disease management. Exploring optimal approaches for the role of HWC in assuring not only improvements in health behaviors and outcomes, but the maintenance or further improvement in these outcomes over time is essential.
Supplemental Material
Supplemental Material - Health and Wellness Coaching and Sustained Gains: A Rapid Systematic Review
Supplemental Material for Health and Wellness Coaching and Sustained Gains: A Rapid Systematic Review by Elizabeth Ahmann, Micah Saviet, Lisa Conboy, Katherine Smith, Barbara Iachini, Ron DeMartin in American Journal of Lifestyle Medicine
Supplemental Material
Supplemental Material - Health and Wellness Coaching and Sustained Gains: A Rapid Systematic Review
Supplemental Material for Health and Wellness Coaching and Sustained Gains: A Rapid Systematic Review by Elizabeth Ahmann, Micah Saviet, Lisa Conboy, Katherine Smith, Barbara Iachini, Ron DeMartin in American Journal of Lifestyle Medicine
Footnotes
Acknowledgments
Duston Morris, PhD assisted with the acquisition of articles in the early portion of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Protocol and Data Availability Statement
This study was not based on a registered protocol. The data for this study is available as supplemental material (see below).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.