
Abstract
Introduction
Frequent mental distress (FMD) is poor mental health for ≥14 days in the past month. Prevalence and risk for depression and suicide are higher among US veterans (USV) than US civilians (USC). Limited research has been done among USV regarding FMD. Anyone can experience mental distress without being clinically depressed—examining FMD more broadly captures health burden of poor mental state. This study’s purpose was to examine the association between having a history of heart attack (HHHA) and FMD among USV vs USC.
Methods
This cross-sectional study used the 2019 Behavioral Risk Factor Surveillance System (n = 274 352) data. Weighted and adjusted logistic regression models were conducted overall and by USV/USC status.
Results
HHHA increases weighted adjusted odds (WAO) of FMD. Among insured not obese USV with HHHA, the WAO of FMD were 1.4x significantly greater (P < .05) than among insured not obese USV without HHHA. Among uninsured obese USC with HHHA, the WAO of FMD were 3.2x significantly greater (P < .0001) than among uninsured obese USC without HHHA, and significantly lower among USV.
Conclusions
Study findings suggest a distinction in FMD among USV/USC with HHHA. Understanding this association can inform policy for FMD screening post-heart attack as another potential intervention to prevent/reduce suicide among USV/USC.
“We hypothesize the odds of experiencing FMD will be significantly higher among US adults with HHHA compared to adults without HHHA.”
Introduction
In 2018 in the United States (US) there were approximately 18 million veterans, representing 7% of the US population at that time. 1 The prevalence and risk for post-traumatic stress disorder,2,3 traumatic brain injury,4,5 suicide, 6 and depression7,8 are higher among US veterans (USV) than US civilians (USC). While much needed attention is given to address these public health crises, limited research has been done among USV regarding the general experience of mental distress beyond these specific issues.
Frequent mental distress (FMD) is a health-related quality of life (HRQOL) measure defined as poor mental health—including feeling stressed or depressed—for any 14 or more days in the past month. 9 While depression is projected to be the leading cause of disability in America by 2030, 10 and FMD includes feelings of depression in its construct, anyone can experience stress and problems with emotions without necessarily being clinically depressed. Therefore, examining FMD, over clinical depression alone, more broadly captures the experience and burden of poor mental state on one’s HRQOL.11,12 The use of HRQOL measures like FMD provides a more holistic assessment of self-perceived health and disease burden and is correlated with disease morbidity and mortality.11,13 Good health is a multi-dimensional state, is more than “merely the absence of disease,” 14 and includes functioning and flourishing in all aspects of life 15 including being free of mental distress.
Heart disease, which can result in a heart attack (HA), remains the leading cause of death in the US. 16 While heart disease prevalence among USV remained around 6% between 2014-2019, 17 USV had higher prevalence of having a history of HA (HHHA) (7.1% vs 3.3%, respectively), and over 2 times significantly greater odds (adjusted odds ratio (AOR): 2.26, 95% confidence interval (CI): 1.41, 3.62) of HHHA than USC. 18 The risk factors for having a HA—including race, gender, socioeconomic factors, and health behaviors—are well-established in the general population.19-22 Mental distress is a risk factor for developing chronic diseases, such as coronary heart disease (CHD), and poorer associated outcomes therefrom like having or dying from HA.23,24 Among US adults, the pathways between HA and mental distress—specifically depression—are bidirectional in nature.25,26 This creates a vicious cycle where individuals find themselves struggling with mental distress and adverse health behaviors contributing to poor health outcomes manifesting as increased symptoms and physical and emotional distress.27,28
While the body of literature is growing, risk factors for experiencing FMD are not nearly as well studied as those of heart disease but are similar—including minority race, socioeconomic factors (e.g., lower income), health behaviors (e.g., lack of physical activity), and health conditions including HA 29 —although only investigated among certain states30,31 or specific subgroups of adults.32,33 A population seldom examined for experiencing FMD is USV. While the existing literature is limited, previous studies have found the prevalence and odds of FMD among USV to be higher than national estimates for the general population.24,34,35
Mental distress and its relationship with the heart is complex. Underutilized mental health services,
36
especially among USV,
37
suggest measuring depression alone may inadequately capture the effect of HHHA on mental wellbeing. While previous research has examined risk factors for HA and separately for FMD among USV, to our knowledge, there are no studies to date that explore the association between HHHA and experiencing FMD among USV compared to USC. The purpose of this study is to examine the association between HHHA and FMD among USV vs USC, and to answer 3 research questions: 1. Are US adults with HHHA more likely to experience FMD than adults without HHHA? 2. Does this association differ by US veteran status? 3. Are there any effect modifiers of this association within each of the 2 groups (USV and USC)?
We hypothesize the odds of experiencing FMD will be significantly higher among US adults with HHHA compared to adults without HHHA. We also hypothesize this association will be stronger among USV than USC.
Methods
The 2019 Behavioral Risk Factor Surveillance System (BRFSS) publicly-available and de-identified data was used for this study. The BRFSS is a cross-sectional, US nationally representative, annual telephone survey. 38 All BRFSS questionnaires, data, methods, sample selection, including the weighting procedure and technical information, and reports are available at https://www.cdc.gov/brfss/.
Measures
Veteran Status
Veteran status was based on responses to the 2019 BRFSS question, “Have you ever served on active duty in the United States Armed Forces, either in the regular military or in a National Guard or military reserve unit?” with possible answers “Yes” or No.”
Exposure of Interest: Having a History of Heart Attack (HHHA)
The exposure of interest is HHHA, derived from the 2019 BRFSS Chronic Health Conditions core section question that asks, “Has a doctor, nurse, or other health professional ever told you that you had a heart attack also called a myocardial infarction?” with possible answers “Yes” or “No.” This variable has demonstrated good validity and reliability. 39 In the 2019 BRFSS questionnaire, HHHA is considered a distinct event from CHD diagnosis.
Outcome of Interest: Experiencing Frequent Mental Distress (FMD)
The outcome under investigation is FMD, derived from the 2019 BRFSS Healthy Days core section question that asks respondents to indicate the number of days their mental health was not good in the last 30 days at the time of the survey. A cut-off point of 14 or more days was used to dichotomize FMD based on clinical markers for depression. 40 This threshold to cross-sectionally measure and longitudinally track FMD has been commonly used by the CDC and other researchers for decades,11,12,41 has been validated for use among US adults, 42 and has high test/retest 39 and strong intra-rater reliability. 43 The poor mental health days question has demonstrated good construct and criterion validity.11,44
Identifying Confounders
Confounders of interest were identified based on previous literature and then entered into a directed acyclic graph (DAG).
45
After running the DAG (Figure 1), the independent variables identified as the minimum sufficient adjustment set needed for estimating the total effect of HHHA on FMD include: age (in years; range 18 to 79 years) 1119,20,29; race/ethnicity (white, non-Hispanic; black, non-Hispanic; other, non-Hispanic; and Hispanic) 2220,30,31; sex (male/female) 2220,33; completed education (less than high school graduate; high school graduate; some college or technical school; and college graduate or more) 2221,29; employment (unable to work; out of work; homemaker/student/retired; and employed for wages/self-employed) 2229,33; household income (<$25,000; $25,000 to <$50,000; and ≥$50,000) 2220,32; marital status (never married; separated/divorced/widowed; and married/unmarried couple) 2229,46; CHD (yes/no if ever told by doctor/other health professional they had angina/CHD) 2221,33; high blood pressure (yes/no if ever told by doctor/other health professional they have high blood pressure) 4447,48; diabetes (yes/no; 2019 BRFSS does not distinguish between type 1/type 2 diabetes) 1119,22,33; obesity (Body Mass Index (BMI) ≥ 30 kg/m2) 1119,29; health insurance (yes/no to having any kind of health care coverage: health insurance, prepaid plans e.g., HMOs, or government plans e.g., Medicare, Indian Health Service) 3330,49; heavy drinking (yes/no, adult men having >14 drinks/week, adult women having >7 drinks/week) 2222,33; physical activity for leisure (yes/no to doing leisure physical activity/exercise e.g., running/calisthenics/gardening/walking during the past 30 days at the time of the survey) 2222,30; and smoking status (never smoker; former smoker; current some day smoker; and current every day smoker).19,29 Directed Acyclic Graph (DAG): HHHA and FMD.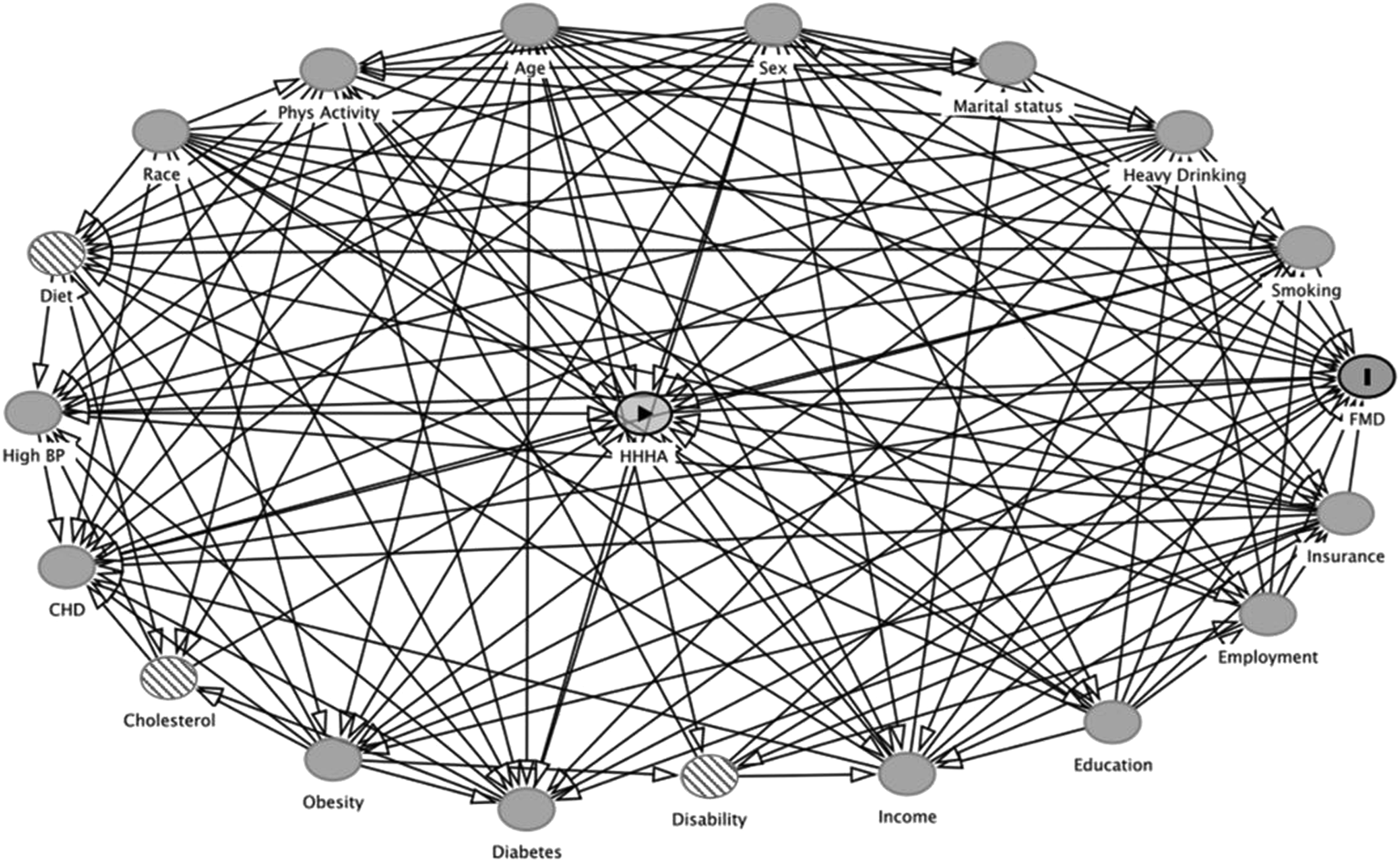
Final Study Sample
The initial sample size from the 2019 BRFSS was 418 268 US adults. Pregnant women (at the time of the survey), individuals ages 80 and above, and individuals with “missing”/“refused”/“don’t know” responses to any variables included in analyses were excluded from this study. Pregnant women were excluded due to the “scientific complexities”
50
and physiological changes experienced during pregnancy that cannot otherwise be controlled for; and respondents ages 80 years and above were excluded due to their ages being imputed to 80 years. The final study sample for this study was 274 352 adult US residents (Figure 2). Consort diagram of final study sample.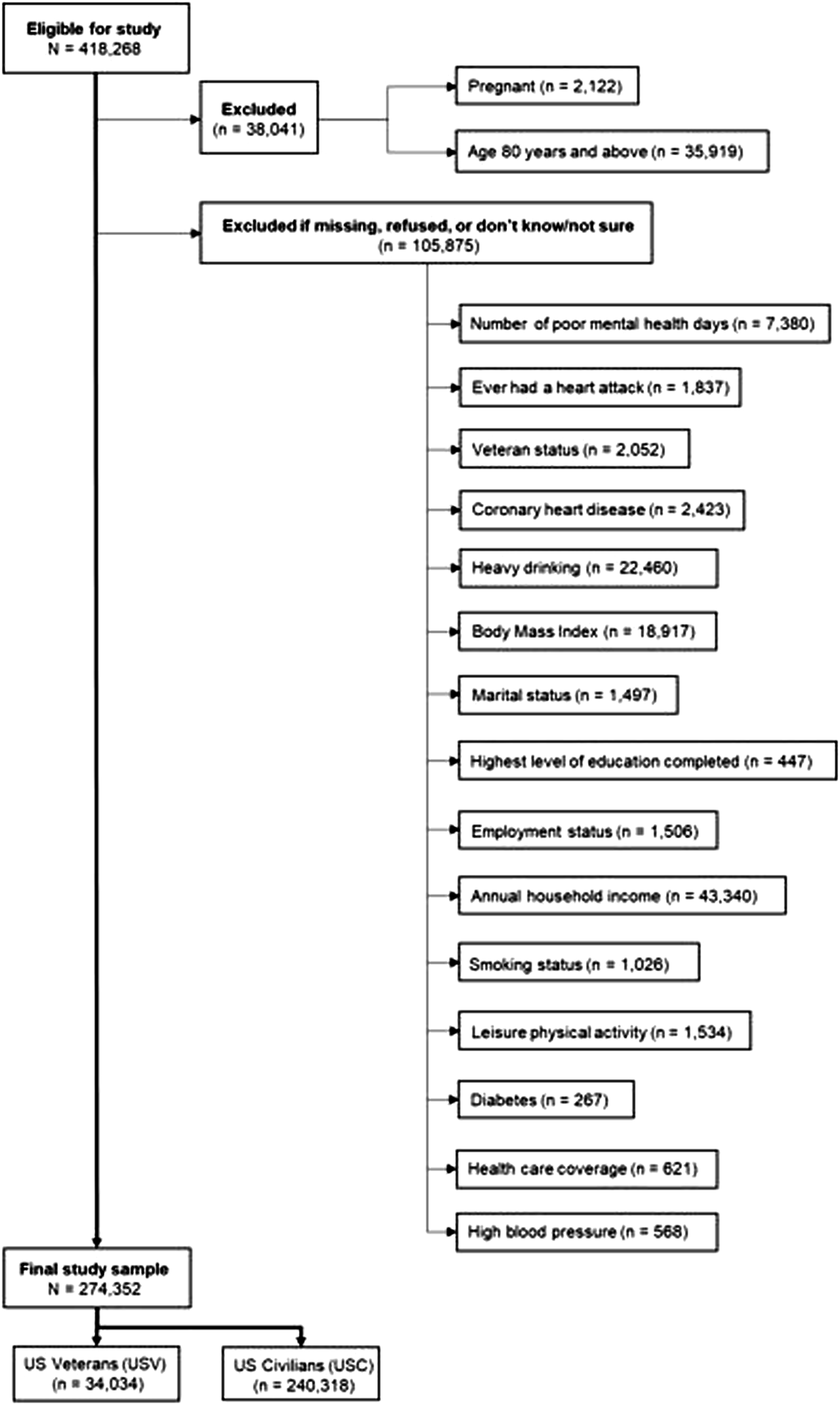
Statistical Analyses
Weighted median and interquartile range are reported for continuous variables; and weighted prevalence and 95% CIs are reported for categorical variables. We evaluated the simple association between each categorical variable and FMD status with Rao-Scott Chi-square tests separately for USV and for USC. To investigate the relationship between HHHA and FMD, weighted adjusted logistic regression models were conducted for the overall final study sample and then by veteran status while adjusting for confounders previously specified. We tested for interaction effects and where significant, corresponding subgroup analyses were performed. All analyses were conducted in 2022 using SAS OnDemand for Academics (SAS Institute Inc., SAS 3.8 (Enterprise Edition), Cary, NC, USA). SAS survey procedures (e.g., PROC SURVEYLOGISTIC) were used to account for the complex sampling design. Differences were considered statistically significant at P < .05 using two-tailed tests.
Results
Characteristics of the Final Study Sample
Descriptive Statistics for US Veterans (USV).
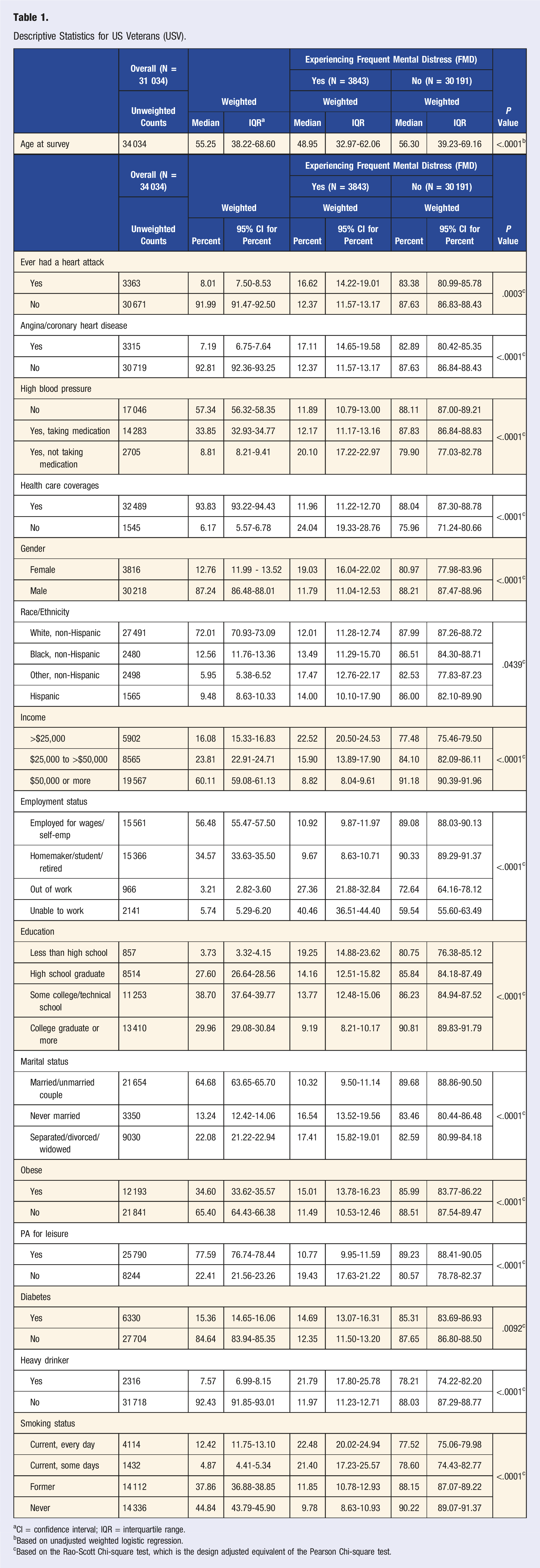
aCI = confidence interval; IQR = interquartile range.
bBased on unadjusted weighted logistic regression.
cBased on the Rao-Scott Chi-square test, which is the design adjusted equivalent of the Pearson Chi-square test.
Descriptive Statistics for US Civilians (USC).
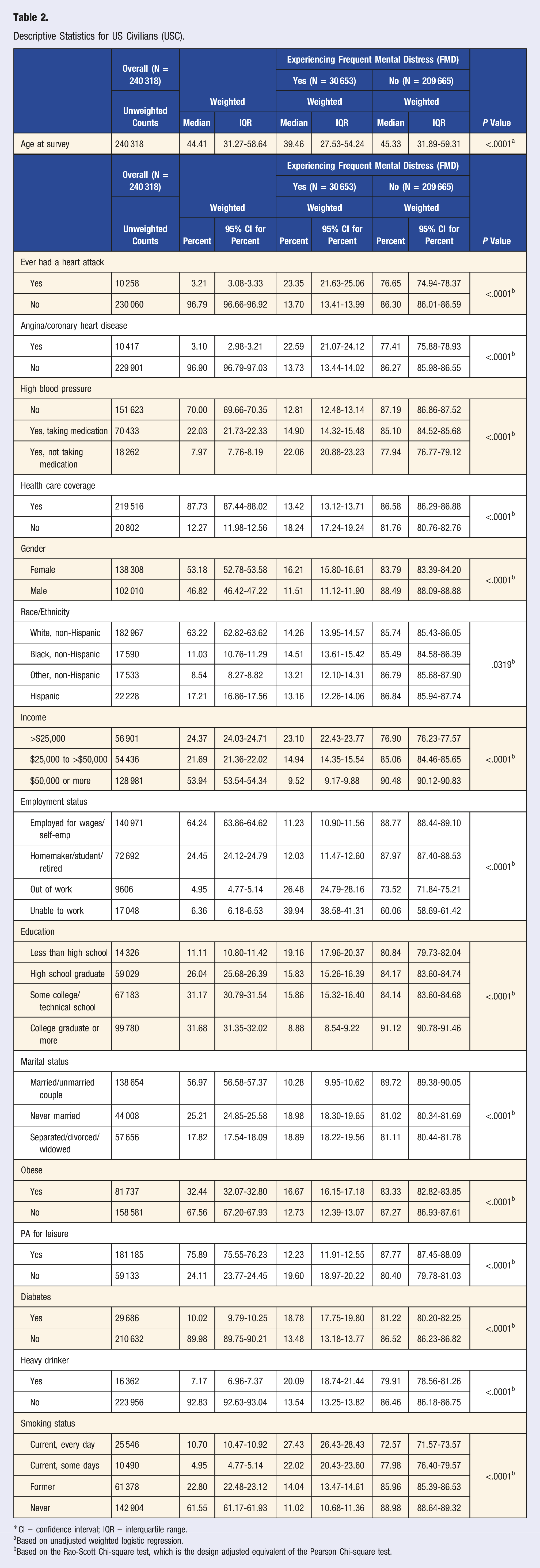
*CI = confidence interval; IQR = interquartile range.
aBased on unadjusted weighted logistic regression.
bBased on the Rao-Scott Chi-square test, which is the design adjusted equivalent of the Pearson Chi-square test.
Weighted and Adjusted Logistic Regression Results
Weighted Unadjusted/Adjusted Logistic Regression results of FMD by HHHA Within Subgroups.
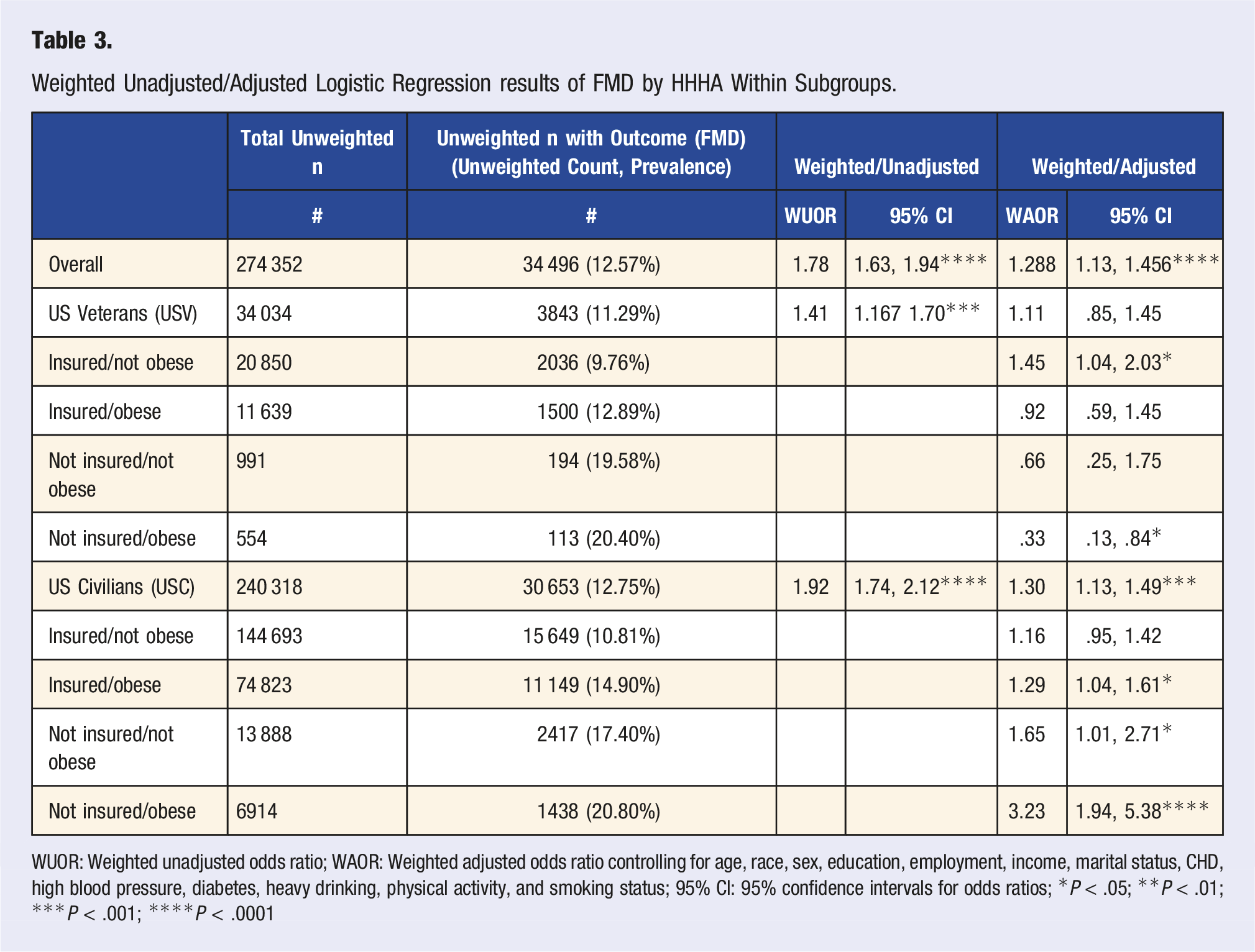
WUOR: Weighted unadjusted odds ratio; WAOR: Weighted adjusted odds ratio controlling for age, race, sex, education, employment, income, marital status, CHD, high blood pressure, diabetes, heavy drinking, physical activity, and smoking status; 95% CI: 95% confidence intervals for odds ratios; *P < .05; **P < .01; ***P < .001; ****P < .0001
The current study found health insurance and obesity status to be effect modifiers (P < .05) of the weighted adjusted association between HHHA and FMD. Table 3 shows results from the weighted, adjusted logistic regression model by veteran, health insurance, and obesity status. Among insured, not obese USV, the WAO of FMD among those with HHHA were 1.45 times significantly greater (95% CI: 1.04, 2.03) than the WAO of FMD among insured, not obese USV without HHHA. Although positive, the WAO of FMD among insured, not obese USC with HHHA were non-significant (WAO = 1.16; 95% CI: .95, 1.42). Among uninsured, obese USC, the WAO of FMD among those with HHHA were 3.23 times significantly greater (95% CI: 1.94, 5.38) than the WAO of FMD among uninsured, obese USC without HHHA. However, among uninsured, obese USV, the WAO of FMD were 67% significantly lower (WAO = .33; 95% CI: .13, .84) among USV with HHHA.
Discussion
To our knowledge, this is the first study to investigate the association between HHHA and FMD among USV and USC using a large, nationally representative sample of US adults. Results indicated HHHA increases the odds of FMD among US adults, providing support for our first hypothesis. Previous literature is limited, but this finding is consistent with one study among Hawaii adults that found HHHA was associated with FMD. 30 We found higher prevalence of HHHA among USV than USC which is consistent with previous literature, 18 but found FMD prevalence to be lower among USV than USC differing from previous literature. 24 Contrary to our second hypothesis, study results indicated the odds of FMD among USV with HHHA were non-significantly greater than the odds of FMD among USV without HHHA. Whereas the odds of FMD among USC with HHHA were significantly greater than the odds of FMD among USC without HHHA (Table 3). We found health insurance and obesity status to be effect modifiers in the weighted adjusted association between HHHA and FMD. The WAO of FMD were nearly one and half times significantly greater among insured, not obese USV with HHHA. Although positive, the WAO of FMD among insured, not obese USC with HHHA were non-significant. The WAO of FMD were over 3 times significantly greater among uninsured obese USC with HHHA. However, among uninsured, obese USV with HHHA, the WAO of FMD were 67% significantly lower.
To better understand the differences in findings between USV and USC, we consider both sociological and psychological interpretations. From a sociological perspective, the military is a distinct institution 51 with a specific set of norms, nomenclature, and social structures that are shared among all its members. 52 There is a shared understanding and application of a warrior ethos embodied in the Soldier’s Creed 53 that always places the mission first and is built on a foundation of self-discipline and mastery, physical and mental toughness, etc., which is instilled in all recruits through basic training, regardless of branch of service (Army, Navy, etc.).53,54 There are key differences between the military institution and the general US culture. The military molds its members into a cohesive unit, minimizing individual differences, 54 which is in juxtaposition with the diverse and multi-cultural55,56 America of civilians who embrace individualism—a core value in American culture. 57 Therefore, the finding that the WAO of FMD were significantly higher among USC than USV with HHHA may be partially explained by the training USV received emphasizing mental toughness, offering protection against the experience of FMD. 58 Conversely, insured not obese USV with HHHA had significantly greater WAO of FMD than USV without HHHA. Based on the values instilled in military personnel (e.g., self-discipline/mastery), HHHA may be especially distressing considering the veteran continued to practice self-discipline and mastery by taking care of their health. Psychologically, this finding echoes the basis for terror management theory (TMT) which asserts individuals utilize both unconscious and conscious methods to cope with the anxiety induced by the awareness of one’s mortality and inevitable death. 59 Unconscious methods are based on one’s view of self as valuable in, and meaningful to, society regarding certain attributes (e.g., bravery/intelligence/beauty) and social roles (e.g., soldier/parent/friend). They provide symbolic protection against the recognition of one’s mortality by establishing the individual as a significant part of “an eternal death-transcending reality.” 59 Conscious methods push away the threat of death as something in the distant future and involve rational efforts to reduce or deny “one’s vulnerability and emphasizing one’s prospects for longevity.” 59 In other words, one eats well, exercises, maintains a healthy weight, sees the doctor, etc. so one can tell themselves they have reasonably done all the right things to push death as far away as possible. This expectation of positive health outcomes stems from the just-world belief hypothesis (JWB) asserting individuals with this belief think people get what they deserve—if they do good, they will be rewarded, and vice versa.60,61
Considering a veteran who has served their country and has practiced self-discipline and mastery to maintain their health (e.g., healthy weight); HHHA breaks through both conscious and unconscious defenses as well as challenges one’s belief in a just world—they did everything right, didn’t they? On the other hand, when viewed through the lens of TMT and JWB, this study’s finding that uninsured obese USV with HHHA had significantly lower WAO of FMD suggest the veteran’s conscious defenses may argue they could have done more to prevent a HA so they may not experience FMD.
Study Limitations and Strengths
Limitations of this study include BRFSS data being cross-sectional, limiting the ability to determine temporality/causation in the association between HHHA and experiencing FMD. Also, FMD is based on self-reported data and is not a clinical diagnosis, and therefore may not accurately reflect the severity or type of mental health condition experienced by the study participants.
Strengths of this study include the large and nationally representative sample of US resident adults. To our knowledge this is the first study to date that assesses the association between HHHA and currently experiencing FMD among USV and USC.
Future Research
Future research should explore the potentially diminishing healthy warrior effect. Shrestha, et al 62 found ideal heart health—including blood pressure and BMI—was less prevalent in active-duty military (Army) personnel than a corresponding subset of noninstitutionalized USC. Hoerster, et al 63 found male USV have poorer short- and long-term health outcomes and behaviors than male USC, specifically a higher prevalence of diabetes, obesity, current smoking, heavy alcohol consumption, and lack of physical activity, which are risk factors for HA. A growing body of literature has demonstrated negative life stressors are risk factors and precipitating circumstances for suicide, which can be a consequence of FMD, 64 and refer to physical health, including HA,65-67 as well as psychosocial factors, such as mental distress.68-70 There is no single cause for suicide, and this public health crisis calls for any and all precipitating circumstances—including HHHA and FMD—to be examined and addressed, especially among USV who have higher suicide rates than USC. 6
Conclusion
Results of this study indicate that HHHA increases the odds of FMD among US adults overall but varies by health insurance and obesity status among USV and USC. This study’s findings contribute new knowledge to the literature about USV. Based on these findings, screening for FMD should be increased among US adults—especially among HA survivors and USV who have a higher HA prevalence than USC. Understanding this association can help inform interventions post-HA to reduce the experience of FMD—including screening and counseling—and may provide another potential area of intervention to prevent and reduce suicide by identifying and preventing FMD post-HA among USV and USC alike.
Footnotes
Acknowledgments
Research reported in this publication was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under Grant no. P20GM103442. IDeA did not have any role in study design; collection, analysis, and interpretation of data; writing the report; and the decision to submit the report for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.