
Abstract
Dietary fiber are non-digestible carbohydrates that are diverse, have varied functions, and are acquired by consuming plant-based foods. Some forms of fiber are digested by the gut microbiota and produce bioactive metabolites called short chain fatty acids—butyrate, acetate, and propionate. Dietary fiber is able to alter human physiology through multiple mechanisms that can result in health benefits. Unfortunately, nearly 19 out of 20 Americans do not consume the minimum recommended amount of fiber each day. This bears profound relevance to public health because at least six of the ten leading causes of death are potentially preventable or clinically improved through dietary means. Additionally, these same conditions share a common underlying pathophysiology-metabolic dysfunction. This can manifest as abdominal obesity, high blood pressure, insulin resistance, dyslipidemia, or collectively as metabolic syndrome. In this review, we will assess the evidence that consumption of dietary fiber undermines these forms of metabolic dysfunction, examine the mechanism of action for these physiologic effects, and consider the potential for dietary fiber to improve human health on a public health level by simply encouraging our patients to consume more plant-based foods in abundance and diversity.
“We find that dietary fiber has metabolic health benefits that are comparable in a general population as well as those with diabetes, hypertension, and cardiovascular disease.”
At least six of the top 10 leading causes of death in the United States are potentially preventable or clinically improved through dietary means. 1 Important advances in our understanding of these diseases implicates metabolic dysfunction as driving forces in their pathogenesis. Heart disease, stroke and diabetes-the number 1, 5, and 8 causes of death-are cardiometabolic diseases. Abdominal obesity, high blood pressure, insulin resistance, and dyslipidemia collectively constitute metabolic syndrome, individually signal a dysfunctional metabolism, and are associated with increased risk for cardiovascular diseases.2,3 Additionally, many forms of cancer, Alzheimer’s disease, and chronic kidney disease-the number 2, 7, and 10 causes of death-are associated with these derangements: metabolic syndrome, obesity, diabetes, hypertension, and hyperlipidemia.4–16
The challenge for healthcare professionals in the 21st century is the overwhelming burden of latent, chronic diseases that gently and covertly develop over years or decades before manifesting, often in an advanced stage and potentially being life threatening. Prevention takes a back seat as we attempt to put out the fires of chronic disease that surround us. New drug and medical device development provides healthcare professionals with novel tools to combat these conditions once present. Unfortunately this reactive strategy requires us to idly wait until the disease has already manifest and caused harm, generally does not address the root cause of metabolic dysfunction, confers risk of adverse events, and adds to rising healthcare costs.
Due to the latent nature of these conditions, there is a window of opportunity for prevention and early intervention using dietary tools available to the general public before the onset of disease. Additionally, it is never too late to use evidence-based tools to prevent disease progression or even promote reversal in some cases. In this review, we will consider the case for dietary fiber as the humble and underappreciated tool that has consistently proven to improve metabolic dysfunction. In an attempt to get an accurate big picture view of the evidence, we will examine the relationship between dietary fiber and metabolic diseases in systematic reviews and meta-analyses of large prospective cohort studies and randomized, controlled interventional trials. We will then explore additional works that provide mechanistic insights to understand the role of fiber in metabolic dysfunction.
With the exception of COVID-19, a new addition in 2020, the top 10 leading causes of death in the United States are the same from year to year and represent a “Who’s Who” of modern disease
1
: 1. Heart disease: 696,962 2. Cancer: 602,350 3. COVID-19: 350,831 4. Unintentional injuries: 200,955 5. Stroke: 160,264 6. Chronic lower respiratory diseases: 152,657 7. Alzheimer disease: 134,242 8. Diabetes: 102,188 9. Influenza and pneumonia: 53,544 10. Chronic kidney disease: 52,547
A Brief Overview of Dietary Fiber
Dietary fiber are naturally occurring plant polysaccharides that cannot be completely broken down by human digestive enzymes. Carbohydrates are classified according to the number of monomeric sugar units as mono-(1), di-(2), oligo-(3-9), or polysaccharides (10 or more). Traditionally, dietary fiber has been recognized exclusively as being polysaccharides, but more recently European Food Safety Authority (EFSA) expanded the definition to include any carbohydrate with 3 or more monomeric sugar units that resists digestion by human enzymes. 17 This includes some oligosaccharides and resistant starches.
Dietary fibers are diverse and complex in their chemical composition. For ease of simplicity, fibers are generally grouped by specific properties, such as solubility, viscosity, and fermentability. Each property affects how the fiber is processed in the body. For example, viscous fibers-such as beta-glucan and psyllium-thicken the fecal mass.
The most common classification for fibers has been according to solubility-soluble and insoluble. Insoluble fiber does not dissolve in water, is often referred to as roughage, and has a bulking effect on stool. Examples of insoluble fiber include wheat bran, cellulose, and lignin. Soluble fiber dissolves in water, is often viscous, and includes inulin, wheat dextrin, beta-glucans, and guar gum, to name a few.
The fermentability of fiber is not perfectly correlated with solubility; however, soluble fibers are generally fermentable fibers while most insoluble fibers have limited fermentability. 18 That said, there are examples of resistant starches that are insoluble and highly fermentable. 19 Fermentability is an important quality in fiber because fermentable fibers are consumed by our gut microbiota, releasing byproducts that include gases but also include short chain fatty acids.
The short chain fatty acids (SCFAs) are the main, and perhaps most important, metabolites produced by the gut microbiota residing in the large intestine. They are fatty acids containing five or less carbon atoms, with acetate (2), propionate (3), and butyrate (4 carbons) being the most common. They have diverse physiological roles in the body and have been connected to numerous measures of human health, some of which we will discuss further. 20 By far, the dominant source of SCFAs is dietary fiber.
The good news is that dietary fiber is not difficult to find. All plants contain dietary fiber. That includes fruits, vegetables, whole grains, seeds, nuts, and legumes. Mushrooms also provide fiber, even though they are fungi and not plants. Every plant will offer a mix of diverse types of fiber that include both soluble and insoluble fiber and have varying degrees of fermentability and viscosity. Although dietary fiber is biochemically complex, the fact that it can be easily sourced by eating more plants is a simple and important message that we need to relay to our patients.
The bad news is that the majority of the United States is inadequate in their fiber consumption. The United States National Academy of Medicine recommends that we consume 14 grams of fiber for every 1000 kilocalories in our diet. 21 This amounts to 30–38 grams of fiber per day for most men and 21–25 grams per day for most women. The most recent data from the National Health and Nutrition Examination Survey (NHANES) indicate that the average adult man and woman consume 18.1 and 15.2 grams of fiber per day. Just 4% of American men and 12% of American women are adequately consuming dietary fiber. 22 The pooled results of all Americans, including children and adults, indicate that just 6% of Americans are meeting their daily fiber requirement. 23
The Health Benefits of Dietary Fiber in the General Population in a Series of Systematic Reviews and Meta-analyses
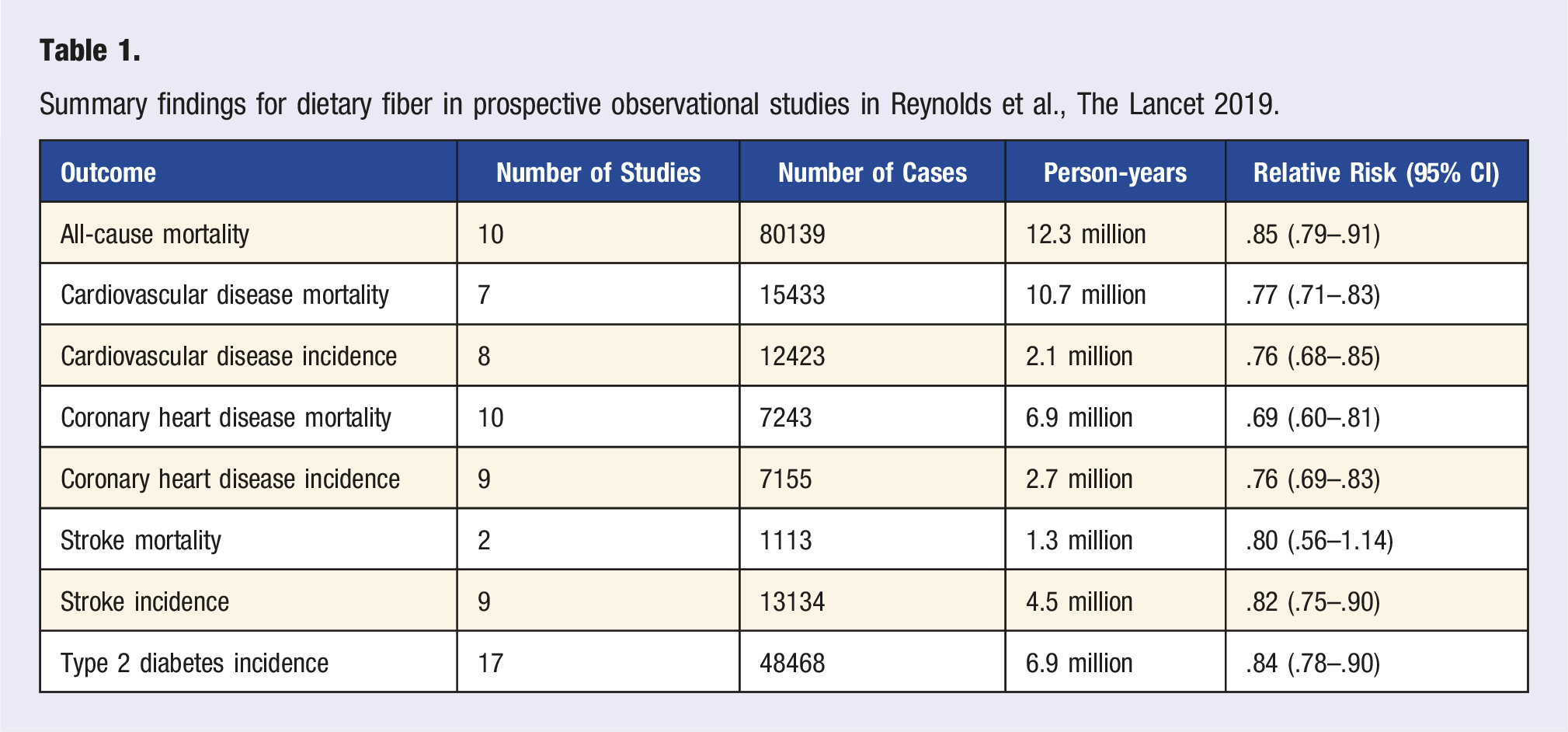
In an effort to update recommendations regarding carbohydrate intake, the World Health Organization commissioned Dr. Andrew Reynolds and a team of nutrition researchers from The University of Otago in New Zealand to perform a series of systematic reviews and meta-analyses seeking to understand the relationship between dietary carbohydrate quality and mortality, the incidence of non-communicable diseases, and their risk factors in the population at large and currently free of disease.
To accomplish this, they performed a series of systematic reviews and meta-analyses of prospective studies published until April 30, 2017, and randomized controlled trials published until February 28, 2018. They excluded adults with acute or chronic disease or in weight loss trials, but did include individuals with prediabetes, mild to moderate hypercholesterolemia, mild to moderate hypertension, or metabolic syndrome. The summary of their findings was published in The Lancet on February 2, 2019 and the complete study findings were detailed in a 316 page supplementary appendix. 24
Summary findings for dietary fiber in prospective observational studies in Reynolds et al., The Lancet 2019.
Considering metabolic outcomes in randomized controlled trials, those who consumed increased fiber lost weight (mean difference −.37 kg, 95% CI −.63 to −.11), lost fat mass (MD −.34 kg [−.59 to −.09]), and reduced their BMI (MD −.17 kg/m^2 [−.33 to −.01]). They also had lower total cholesterol (MD −.15 mmol/L [−.22 to −.07]), lower LDL cholesterol (MD −.09 mmol/L [−.15 to −.04]), lower triglycerides (MD −.06 mmol/L [−.11 to −.01]), and lower systolic blood pressure (MD −1.27 mmHg [−2.50 to −.04]). There was a trend toward improvements in diastolic blood pressure, HbA1c, insulin sensitivity, insulin resistance, and fasting insulin that did not meet statistical significance. It is important to frame these findings within the context that the population studied was free from diabetes, cardiovascular disease, and other major illness.
Taken as a sum, in a series of systematic reviews and meta-analyses among a general population free from major illness the authors found health benefits to dietary fiber that were consistent across both observational studies and randomized trials, and that many of these results had a dose-response relationship. This suggests that dietary fiber intake is more than just a measure of healthy users, and that the fiber is in fact responsible for the disease specific benefits. We will explore this relationship in more detail among these conditions.
A Series of Inpatient Feeding Trials by Dr. Kevin Hall That Provide Insights Into Dietary Fiber and Metabolic Health
Dr. Kevin Hall, a metabolism researcher at the National Institutes of Health, has conducted a series of inpatient feeding trials with subjects to understand the impact of our dietary pattern on our metabolism. In these studies, participants are randomly assigned to spend two weeks on one diet and then crossover to two weeks on the alternative diet. They are instructed to consume as much or as little as desired.
The etiology of obesity and metabolic syndrome is complex. Yet, there is little doubt that the “Western” diet—high in refined carbohydrates, red meat, salt and ultraprocessed foods and low in fiber and minimally processed plant foods-is driving metabolic dysfunction and chronic inflammation. 25 In the first study, an ultra-processed diet was compared to an unprocessed diet. 26 Importantly, meals were matched for calories, energy density, macronutrients, sugar, sodium, and fiber. Fiber supplements had to be added to the ultra-processed diet due to losses of fiber that occurred during processing. The participants ate until they were full on both diets, so measures of hunger, fullness, and satisfaction were similar. Yet, participants consumed 508 more kilocalories per day and gained .9 kg during the two weeks while on the ultra-processed diet.
There are important takeaways from this study. First, to achieve an equal amount of fiber with ultra-processed foods, you have to consume a larger number of calories and add supplemental fiber. Said another way, by consuming the same amount of fiber they achieved equal satiety but the ultra-processed diet added an additional 508 kilocalories per day in doing so. Second, this study suggests a benefit to an intact or minimally disrupted food matrix, the innate structure of food. These are important findings in the context that more than 60% of calories in the United States come from ultra-processed foods. 27
In the second study by Dr. Hall, a plant-based (high carb, low fat) diet was compared to an animal-based (high fat, low carb) ketogenic diet using the same randomized, two week crossover and inpatient design. 28 Both diets were minimally processed (26–32% of energy from ultra-processed foods) and were matched for energy (total calories per day), protein percentage and grams of non-starchy vegetables. The plant-based diet was substantially higher in fiber (31 g vs 9 g per 1000 kcal) and sugars and substantially lower in all fats (including saturated fats). Once again, participants ate until they were full and achieved similar measures of hunger, fullness, and satisfaction.
During the two weeks on each diet, subjects lost more weight on average while on the animal-based low carb diet (1.8 vs 1.1 kg, P = .15). However, most of the weight lost on the ketogenic diet was fat-free mass (1.6 kg, P < .0001 compared to baseline) and just .2 kg of fat loss (P = .35). Fat-free mass includes water and muscle mass. Alternatively, the plant-based diet resulted in significant fat loss (.7 kg, P = .001 compared to baseline) and an insignificant loss of fat-free mass (.2 kg, P = .56). Daily energy intake was consistently lower each day on the plant-based diet when compared to the animal-based ketogenic diet, with an average daily energy deficit of 689 kcal per day on the plant-based diet.
Further, laboratory results revealed a significantly higher total cholesterol, LDL cholesterol, HDL cholesterol, free fatty acids, and high sensitivity C-reactive protein on the animal-based ketogenic diet. The plant-based diet yielded significantly greater fasting triglyceride, as is often seen, but the peak postprandial triglycerides were significantly greater on the low carb ketogenic diet. The low carb ketogenic diet generally favored lower fasting and postprandial blood sugar measures, but insulin sensitivity was superior on the plant-based diet after an oral glucose tolerance test. Finally, the plant-based diet resulted in significantly lower systolic blood pressure, diastolic blood pressure, and pulse rate when compared to the low carb ketogenic diet.
Mechanistic Explanations for Fiber Causing Weight Loss and Reduced Fat Mass
Between the systematic review and meta-analyses by Dr. Reynolds and the metabolic studies done by Dr. Hall we see a compelling picture that dietary fiber undermines metabolic syndrome, including obesity and fat mass. There are a number of mechanistic explanations for the contribution of fiber to metabolic health and lower energy intake.
First, high fiber foods have lower energy density. 29 In the plant-based vs keto study, the energy density was nearly double on the ketogenic diet (2.1 kcal/g vs 1.1 kcal/g). 28 Individuals tend to consume a similar weight of food at each meal, regardless of energy density. 30 If the weight of food consumed is equal, a reduced energy density translates into reduced energy intake.
Second, high fiber foods require more chewing, which slows down eating rate. Previous studies have demonstrated that a 20% change in eating rate can impact energy intake by 10–13%. 31 In the plant-based vs keto study, the ketogenic diet eating rate was 43% greater than the plant-based diet (44.2 vs 30.9 kcal/min). In the ultra-processed vs unprocessed study, the ultra-processed diet eating rate was 17 kcal more per minute (P < .0001). 26
Third, high fiber meals decrease plasma ghrelin (hunger hormone) and increase cholecystokinin (CCK), glucagon-like-peptide-1 (GLP-1), and peptide YY (PYY) compared to energy matched low fiber control diets. 32 Satiety is affected by our gut microbes metabolizing prebiotic fiber. The short chain fatty acids propionate and butyrate bind to G-protein coupled receptors (GPR41 and GPR43) in the colon leading to the production of PYY and GLP-1. 33 SCFAs can also increase leptin secretion, a hormone secreted by adipocytes which regulates food intake, body weight, and energy metabolism. 34 We saw in the plant-based vs keto study that on a plant-based diet the participants achieved equal satiety despite consuming 689 kcal/day less.
There are additional benefits to short chain fatty acids regarding metabolism and weight balance. In animal models, SCFAs enhance lipid oxidation by activating brown adipose tissue, inhibit fatty acid synthesis, induce mitochondrial function, increase energy expenditure, and reduce fat storage.35–37 Butyrate improves intestinal barrier function, reduces serum lipopolysaccharide levels, and reduces free fatty acids, all of which may contribute to healthy weight balance. 38 Additionally, there are cross-over benefits to the effects of SCFAs on insulin sensitivity and lipid metabolism that we discuss below.
Finally, dietary fiber cannot be broken down by human digestive enzymes and as a result acts as a barrier to rapid digestion by slowing digestive enzyme activity and reducing the bioavailability of energy-yielding components.39,40
Systematic reviews and meta-analyses examining the associations of dietary fiber with metabolic health in populations with diabetes.
Building upon the findings from 2019 Lancet paper, Dr. Andrew Reynolds sought to understand the role of dietary fiber in diabetes management as a preamble to updating the European nutrition guidelines for diabetes management. Similar to his prior work, he conducted a systematic review and series of meta-analyses of prospective cohort studies and controlled trials, this time among those with type 1 or type 2 diabetes. The results were published in March 2020 in PLoS Medicine. 41
In total, they identified 2 prospective cohorts including 8300 adults with type 1 or type 2 diabetes residing in 22 countries followed for a mean duration of 8.8 years. When compared to the lowest fiber consumers, those with the highest fiber consumption had significantly reduced all-cause mortality (RR .55 [.35-.86]).
Summary findings for dietary fiber in clinical trials involving type 1 or type 2 diabetes. 41
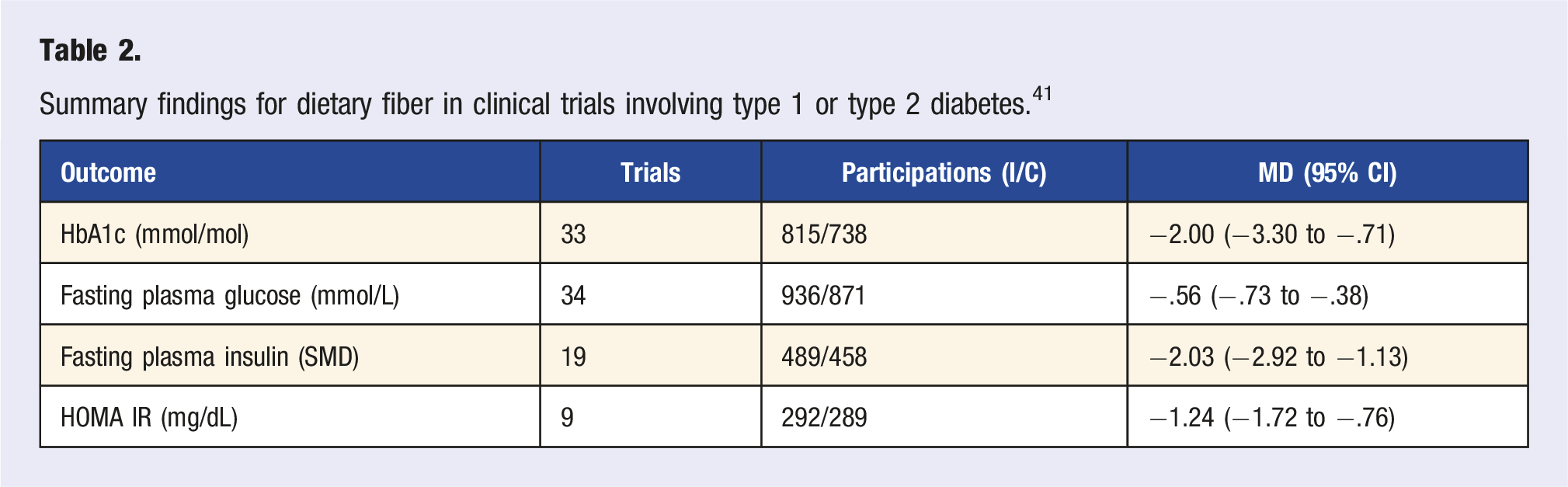
Further, among eligible trials and in those who received increased dietary fiber, they also noted a statistically significant reduction in total cholesterol, LDL cholesterol, and triglycerides. There was also a statistically significant reduction in body weight, body mass index, and waist circumference.
Mechanistic Insights for Fiber Improving Diabetes and Insulin Resistance
Fiber is the carbohydrate that helps you to manage diabetes. There are a number of ways that it manages to accomplish this. First is reducing the glycemic index of foods. Soluble fiber attenuates the speed of carbohydrate absorption. The addition of fiber to carbohydrate containing meals has been shown to flatten the glycemic response in both those with and without diabetes, reduce insulin requirements, lower fasting glucose, and improve glycosylated hemoglobin.42,43 Compared to eating a white biscuit, the addition of 10 grams of a highly viscous fiber blend reduced the glycemic index by 74% in healthy participants and by 63% in participants with diabetes. 44
More importantly, fiber undermines insulin resistance, the root cause of type 2 diabetes and major driver of metabolic dysfunction. In the PREDICT study, gut microbiome characteristics were the second most powerful predictor of post-prandial insulin responses, bested only by serum glucose measures. 45 The microbiome predicted post-prandial insulin levels more accurately than waist circumference or other anthropometric measures, age, sex, genetics, or even meal composition. The likely explanation for this is that the microbiome is responsible for producing short chain fatty acids from dietary fiber.
This was shown in a randomized study of patients with type 2 diabetes who received either a control diet or a macronutrient matched, isoenergetic high fiber diet. 46 Over 28 days, there was a significant change in the gut microbiota on the high fiber diet associated with better clinical outcomes. There was a significant increase in the carbohydrate processing enzymes, indicating that the gut microbiome was adapting its ability to metabolize fiber. This resulted in increased butyrate levels in the high fiber group only. Those receiving the high fiber diet had a significantly greater reduction in glycosylated hemoglobin as well as a greater reduction in body weight and improvements in blood lipids. To demonstrate causality between the gut microbiota and fiber-induced glucose improvements they transplanted the pre- and post-intervention microbiome from the same participants into germ-free mice. Mice that received the post-intervention gut microbiota from the high fiber group had the lowest fasting and postprandial blood glucose levels among the mice.
It was previously mentioned that SCFA’s produced by gut microbes from prebiotic fiber activate the release of GLP-1. The incretin GLP-1 slows gastric emptying and gut transit, enhances glucose-dependent insulin release and promotes early satiety and reduced food intake.47,48 This activity is what led to the development of semaglutide, FDA-approved as Ozempic for diabetes and as Wegovy for weight loss. In the 28 day high fiber diet study, the high fiber group was found to have increased post-prandial levels of GLP-1. They attributed the improvements in glycosylated hemoglobin to the high fiber diet altering the gut microbiome and increasing butyrate production to increase GLP-1 release.
GLP-1 isn’t the only relevant gut hormone for glucose control. SCFAs can stimulate the secretion of PYY, enhancing the absorption of glucose in muscle and adipose tissue while also promoting satiety and reduced food intake. 49 SCFAs also stimulate leptin release, which promotes glucose uptake in brown adipose tissue, the synthesis of liver glycogen, and blood glucose uptake in muscle tissue.50–52
GLUT4 is a protein that allows glucose to enter the cell and is found in both skeletal muscle cells and liver cells. Short chain fatty acids can increase the expression of GLUT4, promoting the increased absorption of glucose by these cells. 53
Systematic reviews and meta-analyses examining the associations of dietary fiber with metabolic health in populations with cardiovascular disease or hypertension.
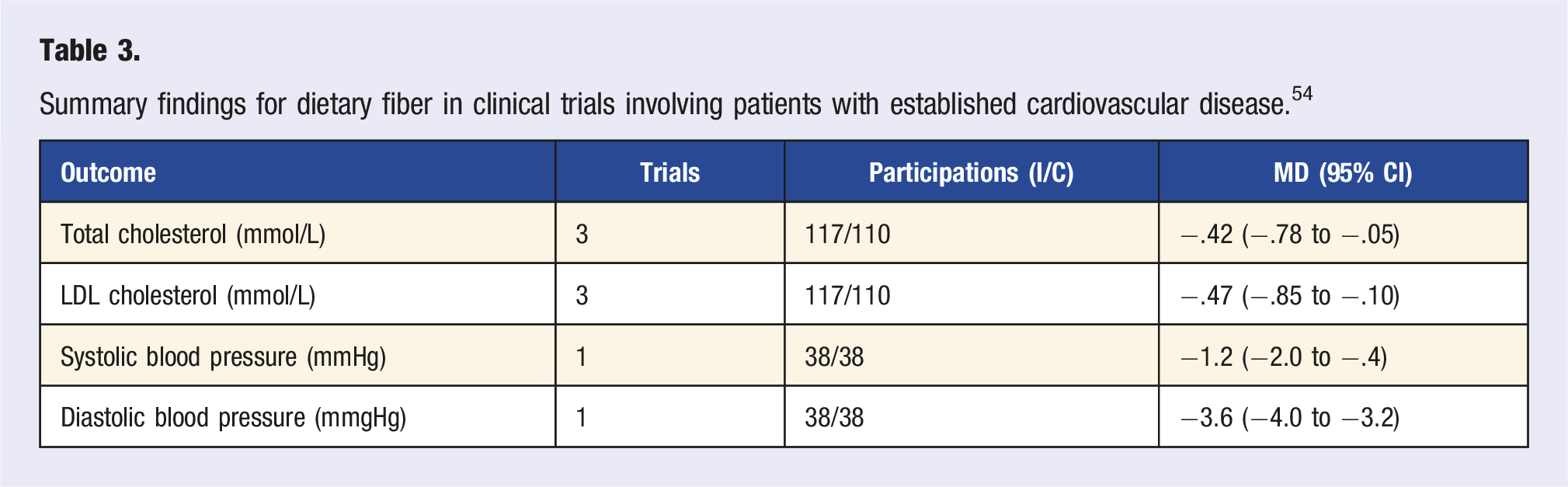
In the 2019 Lancet study on carbohydrate quality and health, Dr. Andrew Reynolds found that high fiber intake was associated with a reduced risk for cardiometabolic events and premature mortality in a generally health population. 24 Then, in his 2020 PLoS Medicine study, he found comparable benefits in adults with type 1 or type 2 diabetes. 41 In a third systematic review and series of meta-analyses, he sought to understand the extent to which dietary fiber can further reduce cardiometabolic risk for those with cardiovascular disease or hypertension. The results were published in April 2022 in BMC Medicine. 54
In total, they identified 4 prospective cohort studies including 7469 adults with cardiovascular disease who were followed for a mean duration of 8.6 years. The studies were conducted in the USA, the UK, and Taiwan. When compared to the lowest fiber consumers, those with the highest fiber consumption had a 25% reduction in all-cause mortality (RR .75 [.58–.97]). This translates into an astonishing 60 fewer deaths per 1000 participants for higher fiber consumers. Additionally, there was a dose response relationship, with every 10 grams of fiber associated with a 14% reduction in all-cause mortality.
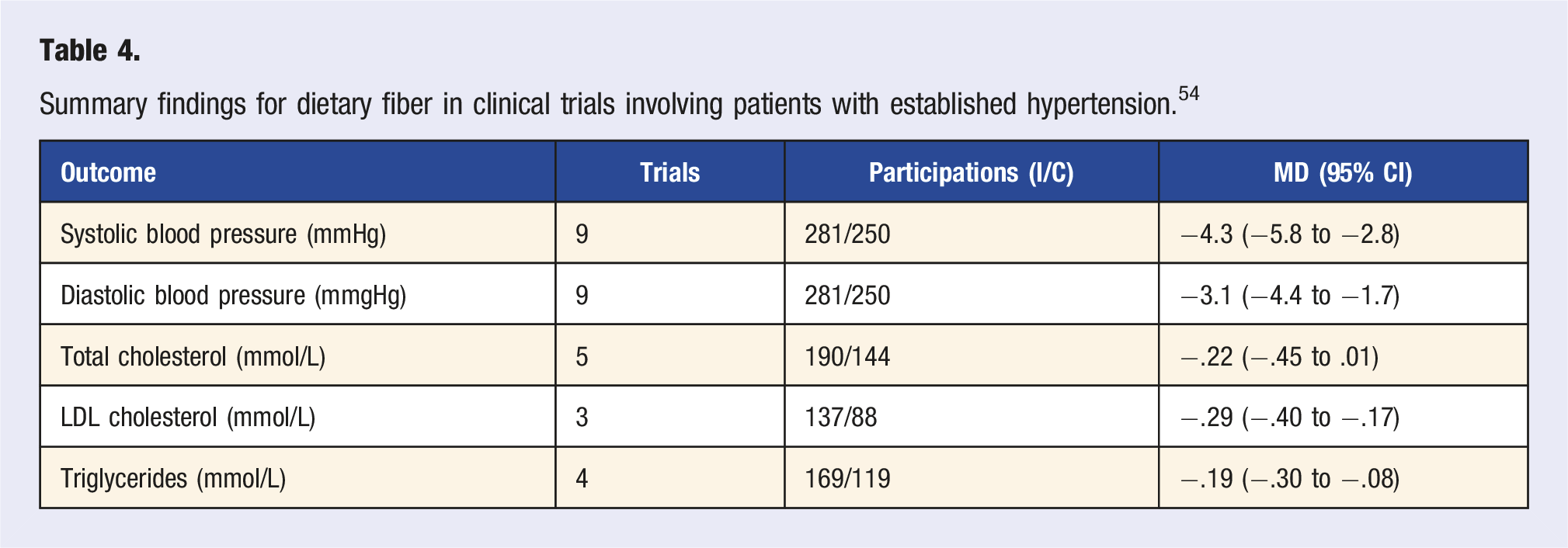
They also analyzed three randomized controlled trials involving 230 participants with cardiovascular disease and nine trials involving 648 participants with hypertension. The increase in fiber intake ranged between just 5.6 and 12 grams per day.
Summary findings for dietary fiber in clinical trials involving patients with established cardiovascular disease. 54
Summary findings for dietary fiber in clinical trials involving patients with established hypertension. 54
Mechanistic Explanations for Fiber Improving Hypercholesterolemia and Hypertension
There are two main ways that fiber helps lower LDL and total cholesterol levels. First, soluble fiber forms a gel-like substance in your intestines that traps cholesterol found in bile acids and prevents your body from reabsorbing them. The trapped cholesterol is ushered out of your body and excreted as a bowel movement.55,56 This is also why bile acid sequestrants lower cholesterol levels. Second, SCFAs that are produced by our gut microbes from prebiotic fiber reduce the hepatic cholesterol synthesis rate. 57 Similarly, patients with hypercholesterolemia have been found to have a distinct gut microbial signature associated with blood lipid patterns. 58
By reducing LDL cholesterol and triglyceride uptake, dietary fiber may improve the elasticity of blood vessel walls, contributing to an antihypertensive effect. 59 Similarly, insulin resistance is believed to play a role in endothelial dysfunction and hypertension. 60 Beyond these cross-correlated mechanisms, SCFAs have been shown to directly reduce hypertension through a number of pathways, including activating receptors in vascular smooth muscle and endothelial cells, altering renin-angiotensin activity in the kidney, and by activating the parasympathetic nervous system. 61 Finally, fiber-rich foods, such as vegetables and fruits, can often be a source of dietary nitrates, which are precursor molecules to nitric oxide that improve blood pressure through vasodilation. 62 While this may not be the direct effect of fiber, it is a benefit of consuming fiber-rich foods and would contribute to associated blood pressure lowering effects.
Conclusion
We find that dietary fiber has metabolic health benefits that are comparable in a general population as well as those with diabetes, hypertension, and cardiovascular disease. Fiber has a number of important and unique qualities including its viscosity, resistance to human digestive enzymes, and fermentability by gut microbes to produce short chain fatty acids that have physiologic effects throughout the body. Across populations and using different study formats, we consistently find that dietary fiber undermines metabolic disease by reducing weight, burning fat, improving insulin sensitivity, and lowering cholesterol and blood pressure. In this context, it comes as little surprise that those who consume more fiber live longer with less risk for cardiovascular diseases. Thus, the current state of fiber deficiency in Western countries is of supreme public health importance. We have a tremendous opportunity to improve human health across populations by simply correcting this fiber deficiency on an individual, person-by-person basis. It starts with the simple message to our patients that they should eat more plants, in diversity and abundance.
Footnotes
Acknowledgments
I am the US Medical Director of ZOE Global Limited, the sponsors of the ZOE PREDICT trials that are cited in this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.