
Abstract
A whole-food plant-based (WFPB) diet in combination with healthful lifestyle modifications has been shown to be an effective approach to managing and reversing the progression of coronary artery disease and type 2 diabetes mellitus (T2DM). The Health Achieved Through Lifestyle Transformation Program (HALT) is a 20-week real-world healthful diet and lifestyle intervention program implemented at Kaiser Permanente South Sacramento Medical Center (KPSSC), whose goal is to treat, and where possible, reverse CAD and T2DM. Here, our objective is to describe HALT, including enrollment, the intervention, adherence, and data collection activities during a 2-year period from October 15th, 2016, through October 9th, 2018. There were 204 KPSSC members enrolled, of which, 19 (9.3%) had CAD only, 166 (81.4%) had T2DM only, and 19 (9.3%) had both CAD and T2DM. Among the enrolled, 196 (96.1%) completed self-administered questionnaires, and 88.2 to 97.5% completed blood tests, depending on the test. The enrolled were predominantly female (63.2%), ≥50 years old at program entry (83.3%), and white (32.8%) or black (25.5%). HALT has the potential to become a valuable resource for examining the impact of dietary and lifestyle modifications on patients diagnosed with CAD and/or T2DM.
“The greatest difference is that the HALT program is based within a large, demographically diverse, integrated healthcare system serving over 4.6 million members in Northern California.”
Introduction
Heart disease is the leading cause of death in the United States (US) 1 and coronary artery disease (CAD) accounts for over 350 000 deaths per year. 1 Diabetes has also reached epidemic proportions, with over 34 million people in the US living with the disease, and is itself a risk factor for CAD. 2 According to the Centers for Disease Control and Prevention, the number of adults diagnosed with diabetes has more than doubled over the past 20 years and is now the seventh leading cause of death in the US. 2 Type 2 diabetes (T2DM) accounts for 90–95% of all diabetes cases. 2
Research has shown that following a whole-food plant-based (WFPB) diet can decrease the risk of developing CAD and T2DM, improve disease management and outcomes, and lower disease related mortality.3-8 This may be in part due to evidence suggesting that a WFPB diet facilitates decreases in weight, blood pressure, hemoglobin A1c (HbA1c), and total and LDL cholesterol levels.8,9 Research has also shown that intensive lifestyle changes, which include dietary modifications in combination with physical activity, smoking cessation, and psychosocial counseling can improve the course of CAD10-13 and T2DM. 14
The Health Achieved through Lifestyle Transformation Program (HALT) is a real-world healthy behavior and lifestyle program based at the Kaiser Permanente South Sacramento (KPSSC) facility which is part of a large and diverse integrated healthcare system serving over 4.6 million members in Northern California. HALT uses an education and behavioral management program administered by a team of physicians, pharmacists, behavioral health specialists, and health educators to promote healthful lifestyle changes in patients with CAD and/or T2DM in a primary care setting. The goal of HALT is to help patients live healthier, longer, and higher quality lives, while also reducing the long-term financial burdens on both patients and the health facilities that care for them.
Our objective here is to describe the design and implementation of HALT, including enrollment, the intervention, adherence, and data collection activities during a 2-year period from October 15th, 2016, through October 9th, 2018. We also describe the demographic and clinical characteristics of the program participants as compared to those who elected not to participate after an initial orientation to the program, and to the broader potentially eligible population at KPSSC. As a real-world fully integrated diet and lifestyle intervention program, HALT may be well positioned to inform new strategies for improvement of CAD and T2DM prognosis and be instrumental in contributing to future research to benefit this ever-growing population.
Methods
HALT is a diet and behavioral modification intervention program developed and implemented through the Department of Lifestyle Medicine (DLM), KPSSC, 1 of 21 medical centers in the Kaiser Permanente Northern California (KPNC) integrated healthcare system. The HALT program is delivered over a 20-week period and is focused primarily on patients diagnosed with CAD and/or T2DM. The central goals of the program are to support, manage, treat, and where possible, reverse CAD and T2DM as well as enhance overall health, through sustained diet and lifestyle behavior changes along with continued community support.
This study was approved by the Institutional Review Board of Kaiser Permanente Northern California (KPNC) and written informed consent was obtained from all study participants.
Participant Enrollment
HALT participants were enrolled directly from the DLM’s introductory 1-hour course (PB101) where KPSSC members learned about the benefits of a WFPB diet. Individuals diagnosed with CAD and/or T2DM were typically referred to PB101 by their KPSSC pharmacists, cardiologists, and primary care physicians for management and treatment of their conditions. However, any KPSSC member could have become aware of the class on their own and have decided to attend. At the end of the 1-hour class, attendees were provided more detailed information about the HALT diet and lifestyle intervention program, its expectations and timeline, and were invited to join the program.
Those who were interested in the HALT program were then contacted by phone to assess their level of motivation using a scale from 1 to 10, with 1 being the lowest level of motivation and 10 being the highest. Those who scored <7 on the motivation scale were referred to alternative educational resources and standard chronic condition management. Those who scored ≥7 on the motivation scale had their electronic health records (EHR) reviewed to ensure program eligibility. For those for whom it was determined did not have CAD and/or T2DM or did not meet any of the other program eligibility criteria were referred to an alternative diet and lifestyle program called Plant Strong, whereby participants experienced a less intensive version of HALT programming with no behavioral or medical monitoring.
Those who met program eligibility signed a consent form, were emailed a series of self-administered surveys, had blood tests ordered, and were scheduled for an in-person exam with a program physician. During the in-person physician exam, participatory motivation and program eligibility was reassessed. A series of clinical measures (e.g., height, weight, waist circumference, and blood pressure) were ascertained from those confirmed as eligible, who were then subsequently enrolled into the program.
Participant Eligibility
Eligibility criteria for the HALT program.
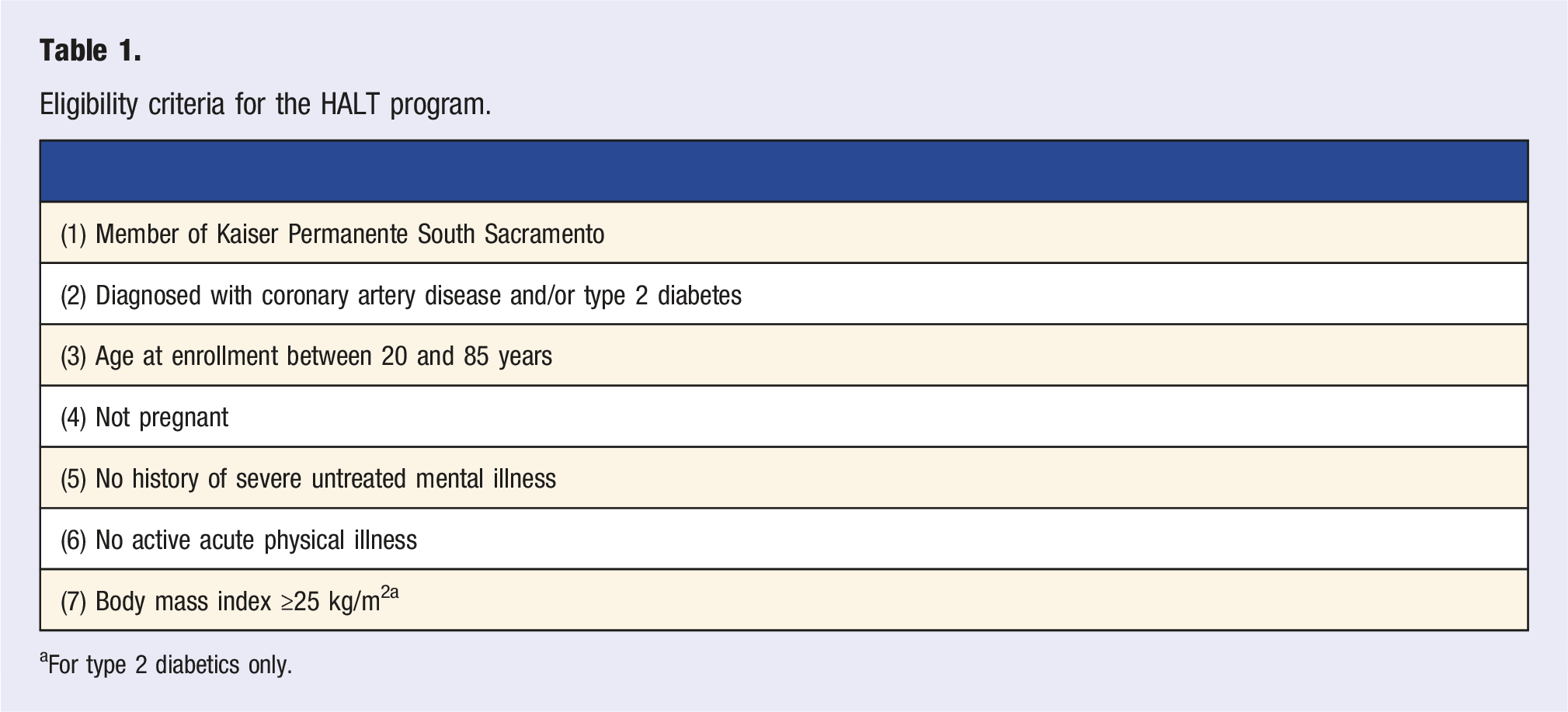
aFor type 2 diabetics only.
Program Intervention
Participants were typically scheduled to begin the diet and lifestyle intervention program within 2–4 weeks after initial enrollment. Maintaining typical lifestyle behaviors until starting the intervention was encouraged and spouses/partners were urged to enroll as a source of support for the participant. HALT pilot programs showed participants to be 3 times more likely to succeed in completing the program with support from a partner. Support participants did not need to meet the eligibility criteria for the program and their data were not included in this study.
Summary description of the HALT program.
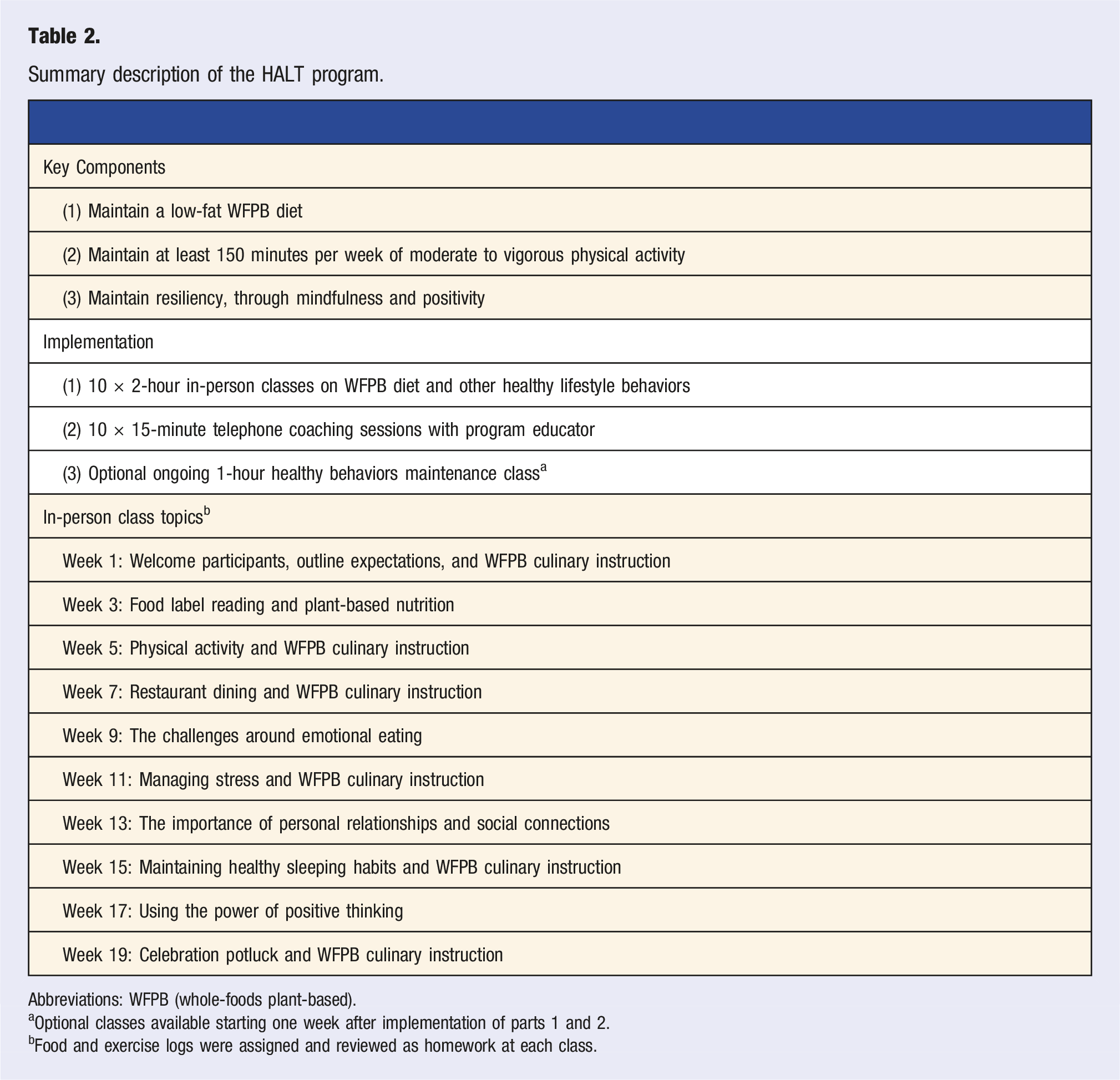
Abbreviations: WFPB (whole-foods plant-based).
aOptional classes available starting one week after implementation of parts 1 and 2.
bFood and exercise logs were assigned and reviewed as homework at each class.
Dietary Intervention
The HALT program encouraged adherence to a low-fat WFPB diet with approximately 10% of total dietary energy obtained from fat. An example of a typical day of eating might have been having oatmeal for breakfast, baked tofu sandwich for lunch and rice with beans for dinner. In addition, eating leafy green vegetables with each meal was encouraged. Dietary behavior changes were implemented through a multi-disciplinary program which included nutritional guidance from instructors, providing recipes of healthy WFPB meals, culinary education on batch meal cooking to increase efficiency, as well as one-on-one consultations with instructors for personalized coaching. Recommendations were also made for vitamin B12 supplementation to prevent deficiency from following a WFPB diet. Participants used daily food logs to keep track of their progress and record their daily food consumption.
Physical Activity Intervention
The HALT program encouraged participants to engage in at least 150 min of moderate to vigorous physical activity per week, as recommended in the Physical Activity Guidelines for Americans set forth by the Centers for Disease Control and Prevention. 15 HALT instructors educated participants on the benefits of physical activity and provided in-person demonstrations on various forms of stretching, yoga, sit-ups, wall push-ups, and other general fitness exercises. Participants tracked their physical activity through provided activity logs, their phones, or other types of physical activity tracking devices.
Resiliency Intervention
Implementing lifestyle modifications in the context of complex life situations and circumstances can be challenging, thus cultivating greater adaptation, or resilience, was integrated into the HALT program. Participants were educated on the adverse health effects of stress and encouraged to engage in daily mindfulness and meditation practices to cope with stress. Instructors encouraged participants to maintain deeper connections with family and their respective communities to increase social support. Participants also learned the importance and healthy impacts of sleep and were provided in-class assignments on the advantages of positive thinking, which has been shown to help sustain healthy behavior changes.21,22
In-Person Courses
The HALT program intervention consisted of 10 in-person 2-hour courses every other week over a 20-week period. Each class began with a 15-minute group check-in, where each participant had an opportunity to discuss their progress and ask questions. This time may have also been accompanied by a meditation or other mindfulness exercise. Each class focused most of its time on a specific topic such as plant-based nutrition or emotional eating (see Table 2 for complete list), while the last 15 min of each class was devoted to goal-setting for the upcoming week. In at least 4 of the 10 classes, a culinary demonstration was provided, whereby participants were shown the specific steps in preparing or cooking a healthy WFPB meal. Several courses were also attended by the program physician who discussed topics covering the benefits of diet, physical activity, and resiliency.
Telephone Coaching Sessions
In addition to the 10 in-person courses, the HALT program provided 10 one-on-one 15-minute telephone coaching sessions every other week when there was no in-person class. Coaching sessions offered encouragement and motivational interviewing 16 to help move participants towards behavior change. It also assessed dietary and lifestyle modification adherence by reviewing participant logs and obtaining feedback on what the participants found challenging.
Lifestyle Maintenance Courses
Upon completion of the 20-week intervention program, each participant was encouraged to participate in ongoing 1-hour maintenance classes to help sustain their modified dietary and lifestyle behaviors. These classes were made available 2–3 times a week over the entire study period and were meant to reinforce healthy behaviors by checking in with participant progress, discussing challenges, and revisiting course materials and practices.
Behavior Change Theory
The HALT program was based on accepted theoretical models of behavior change, including the Health Belief Model, 17 Social Cognitive Theory, 18 and the Transtheoretical (Stages of Change) Model. 19 Commonalities of these models include having adequate motivation and skills, self-efficacy, the right triggers or prompts preceding change, and the ability to overcome barriers. Being ready, willing, and able to change was critical to participant success in the HALT program, as well as recognition of the importance of social support and ability to implement behavioral changes within the context of the domains in which they occur.
Goal-Setting
Evidence has shown that goal-setting can be effective in changing behaviors and meeting long-term goals,20,21 and was therefore a central part of the HALT intervention program. HALT made use of the SMART criteria (Specific, Measurable, Achievable, Realistic, and Timed) for individualized goal-setting, which has shown to be effective in identifying and making specific behavior changes. 21 With instructor oversight, participants developed their own goals at the end of each class which they recorded in their personal logs. Participants were urged to reflect on these goals throughout the week as needed and at the beginning of the following class.
Data Collection and Potential Outcomes
To capture and measure participant progress over the course of the program, several behavioral, clinical, and biometric data collection tools were administered at program entry, and again at 6, 12, 18, and 24 months after enrollment. These tools included a series of self-administered questionnaires, laboratory tests from blood collection, and in-person clinical measurements. These data domains were augmented with data from the KPSSC databases.
Self-administered surveys included an abbreviated food frequency questionnaire (FFQ) to assess food-intake and were accompanied with questions pertaining to the sustainability of a WFPB diet. The Yale Food Addiction Scale assessed eating behaviors, 22 and the Medical Outcomes Study Short-Form 20 (SF-20) evaluated physical, role and social functioning, as well as mental health, current health and pain. 23 The surveys also inquired about physical activity and stress management.
Blood was drawn from each participant at the KPNC laboratory of their choice, from which, the following tests were performed and thus became part of the participant’s clinical record: HbA1c, fructosamine, fasting blood sugar, alanine aminotransferase test (ALT), high-sensitivity C-reactive protein, vitamin B12, and a fasting lipid panel (including total cholesterol, HDL cholesterol, and triglycerides, and estimated LDL cholesterol).
In-person exams were performed by a study clinician who measured blood pressure, body weight, waist circumference, and resting metabolic rate (RMR). Measurements were taken at the initial physician exam and 30 min before each in-person class for a total of up to 11 assessments for each participant during the 20-week intervention period. Full body photos were also taken before, during, and after the intervention to visually illustrate physical changes and for participants to use as a motivational tool.
KPNC clinical databases were used to supplement primary data collection on all study participants. Data of interest included demographics, diagnoses, laboratory tests and results, prescription medications, anthropometry, and vital signs. These were obtained from the KPNC Virtual Data Warehouse (VDW). 24 Healthcare utilization cost data for each participant was also obtained from the KP Cost Management Information System (CMIS).
Comparison Groups
To help describe the demographic and clinical characteristics of HALT participants, two comparison groups were identified: (1) PB101 attendees who were either ineligible or chose not to participate in the HALT program, and (2) the source population of HALT participants; that is, those who were diagnosed with CAD and/or T2DM at KPSSC and were theoretically eligible to enroll in the HALT program. To have been included in the source population, participants were required to meet the central HALT eligibility criteria (KPNC member whose care was received through the KPSSC medical center, diagnosis of CAD and/or T2DM, be 20 to 85 years old, and body mass index ≥25 kg/m2 for T2DM) at any point in time during the study period. The source population was identified using diagnosis codes in conjunction with demographic and clinical characteristics ascertained from KPNC’s EHR.
Statistical Analysis
These analyses provide descriptive data of HALT participants, as well as distributions of program adherence regarding attendance of in-person classes and one-on-one coaching calls. Completion rates for baseline questionnaires, biometric measures, and blood tests are also provided. A demographic and clinical comparison of HALT participants with those who attended PB101 but did not enroll in HALT, and with the KPSSC source population identified through the EHR is also provided. Demographic and clinical characteristics were summarized using tabulations of categorical variables.
Results
Participant Recruitment
Of the 900 KPSSC members who participated in PB101 during the study period, 456 (50.7%) were deemed potentially eligible for the HALT program (Figure 1). The primary reason for ineligibility was that the person did not have a CAD or T2DM diagnosis (n = 422, 95.0% of the 444 not eligible). Other reasons for ineligibility were being aged 85 years or older (n = 3, 1.0%), and having had a T2DM diagnosis with a BMI <25 kg/m2 (n = 19, 4.5%). Of the remaining 456 eligible PB101 attendees, 234 (51.3% of 456) were not interested in participating in the HALT program, and 222 (48.7%) went on to be examined by a HALT program physician to confirm eligibility and willingness to participate in the program. Of those examined by the physician, 18 (8.1%) were determined to be ineligible: 9 for lack of motivation, 2 for having an active acute physical illness, 1 for having a history of untreated mental illness, and 6 for other reasons, including unsubstantiated diagnosis of CAD or T2DM, enrollment in another lifestyle intervention program, and living outside the KPSSC region hence making attendance at HALT in-person sessions difficult. A total of 204 PB101 attendees were therefore enrolled into the program (Figure 1). HALT program recruitment and exclusion process.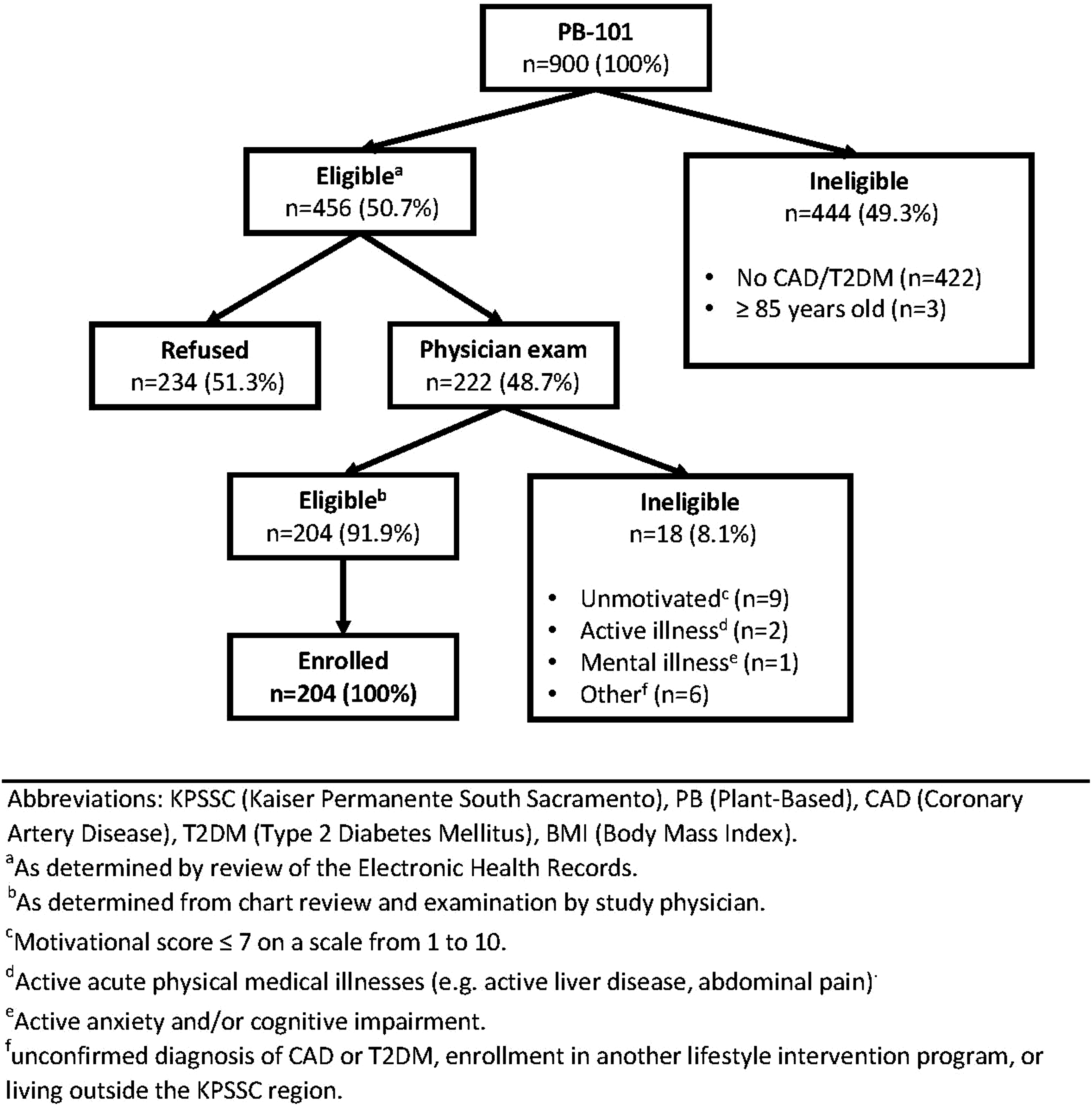
Program Participation
HALT program attendance (n = 204).
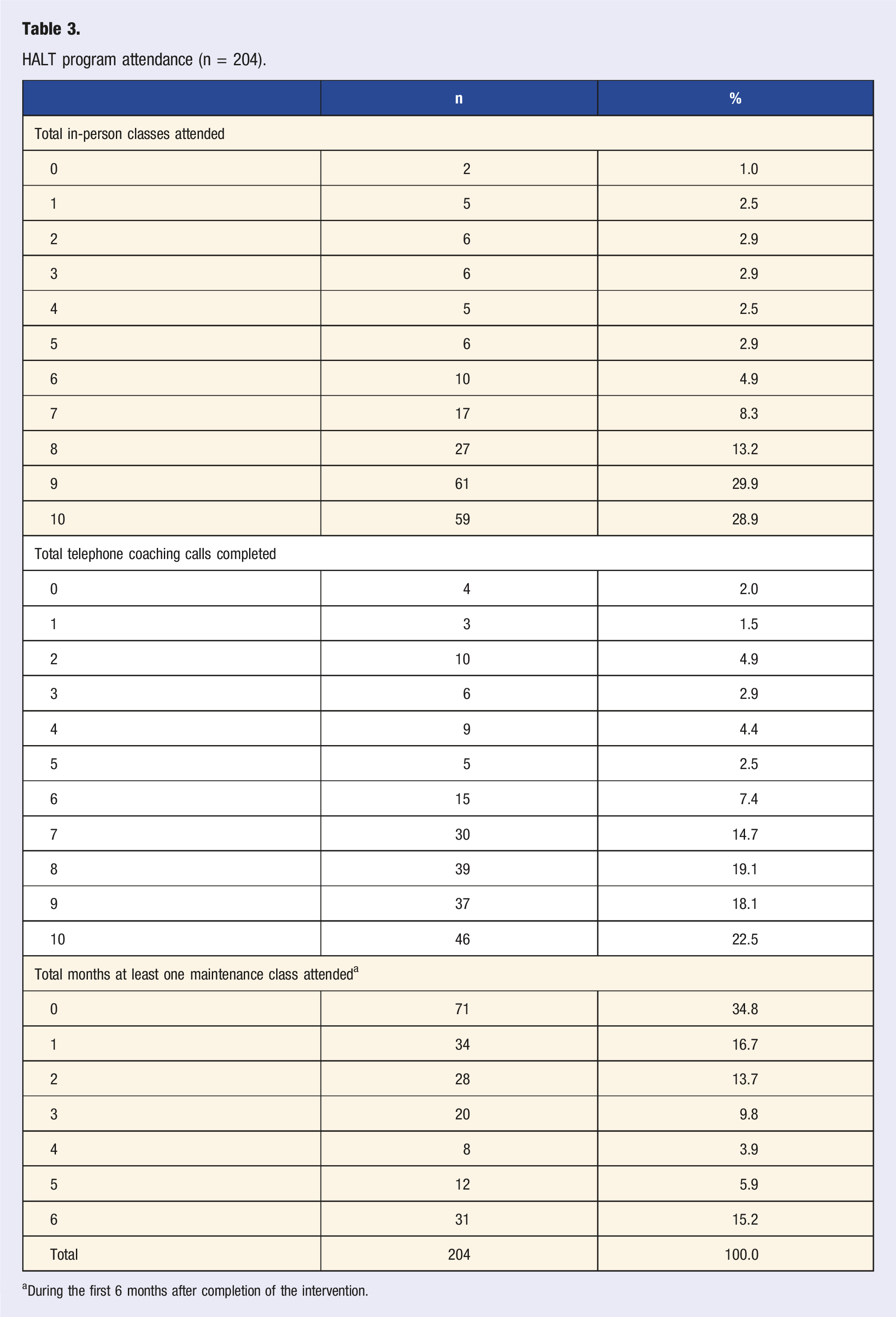
aDuring the first 6 months after completion of the intervention.
HALT program questionnaires, blood tests, and biometric measures collected at baseline (n = 204).
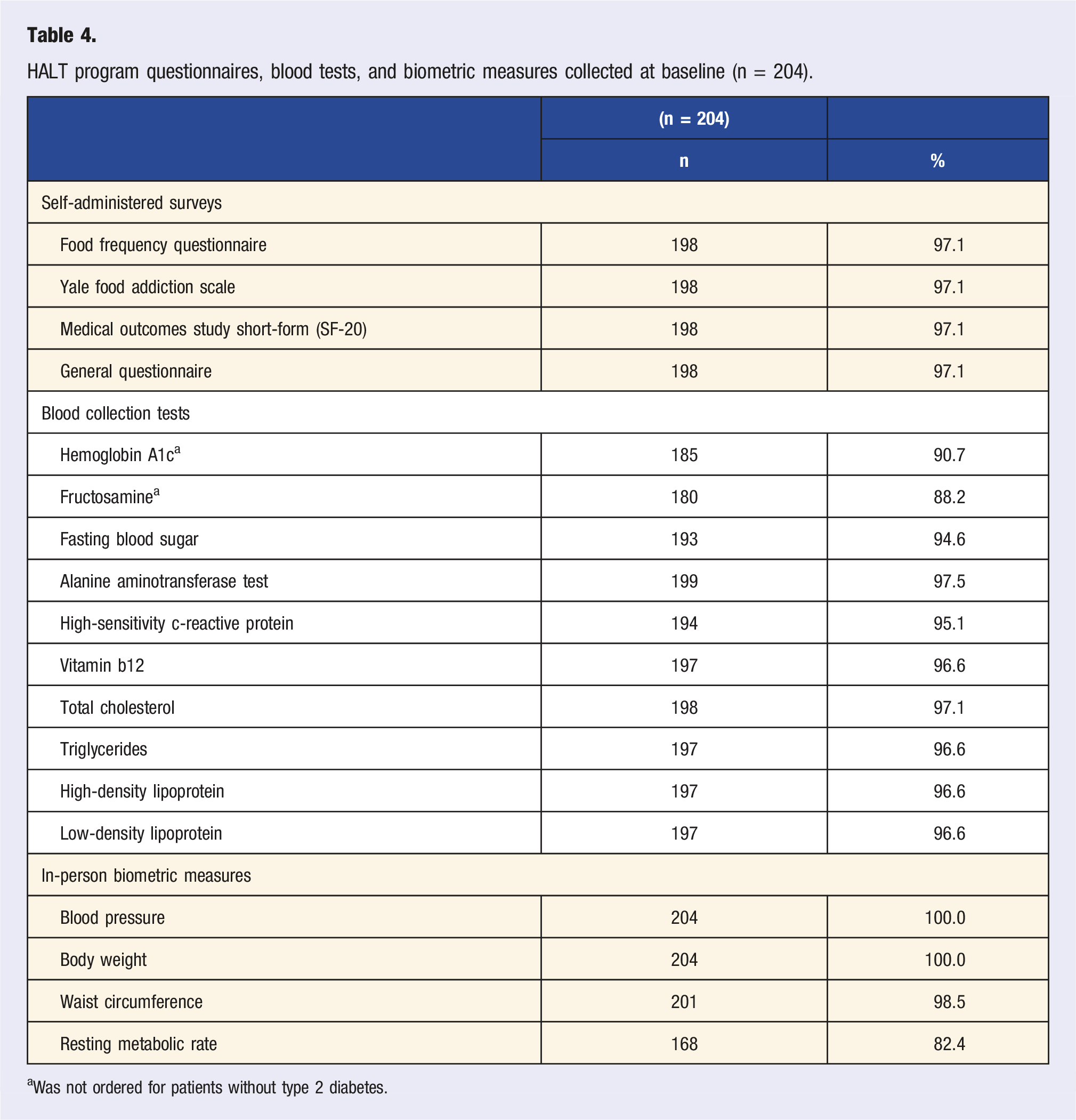
aWas not ordered for patients without type 2 diabetes.
Demographic and Clinical Characteristics
Baseline characteristics, comparing HALT participants to plant-based 101 attendees and the Kaiser Permanente source population.
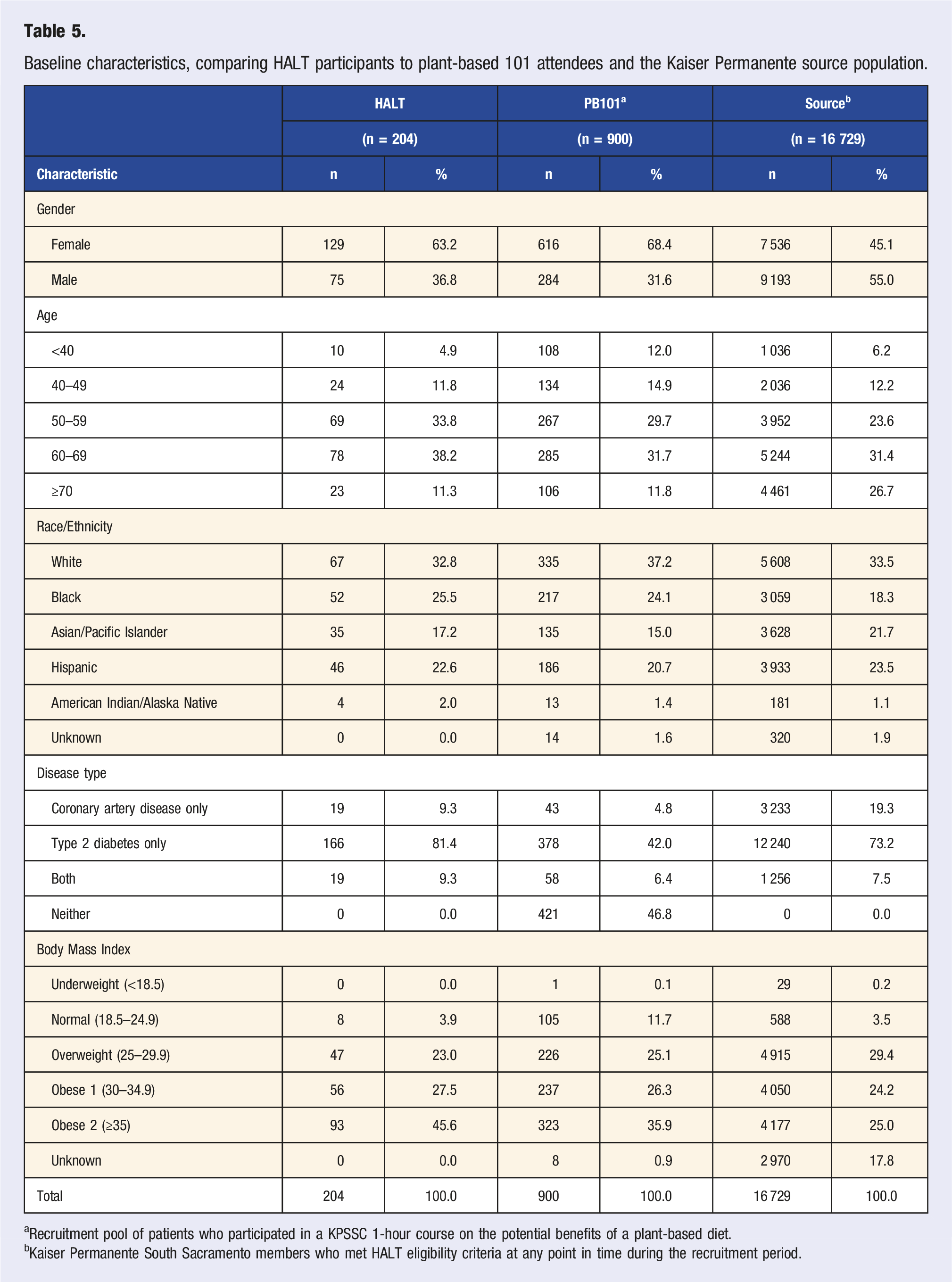
aRecruitment pool of patients who participated in a KPSSC 1-hour course on the potential benefits of a plant-based diet.
bKaiser Permanente South Sacramento members who met HALT eligibility criteria at any point in time during the recruitment period.
The KPSSC source population who were theoretically eligible for the HALT program had a lower proportion of females (45.1% vs 63.2%) compared to HALT program participants, were older (26.7% vs 11.3% for ≥70 years old) and had a slightly lower proportion of blacks (18.3% vs 25.5%). The KPSSC source population also had a higher proportion of people diagnosed with CAD only (19.3% vs 9.3%), a lower proportion of people diagnosed with T2DM only (73.2% vs 81.4%) and lower proportion of participants with BMI ≥30 kg/m2 (49.2% vs 73.1%). However, 17.8% of the KPSSC source population were missing their BMI value.
Discussion
HALT is an ongoing real-world diet and lifestyle intervention program organized by the Department of Lifestyle Medicine at KPSSC. It focuses on a low-fat WFPB diet, physical exercise, and resiliency to support, manage, treat, and where possible reverse CAD and T2DM. The overall goal of the program is to improve patient outcomes related to CAD and T2DM and to lower hospital costs. The purpose of this study was to describe the HALT program and its participants, and in part, compare them to both the cohort of PB101 class attendees and the KPSSC source population. Though there may been some slight differences, HALT participants were a demographically and clinically diverse population that were representative of the larger population of CAD and T2DM members at KPSSC. With thorough dietary and lifestyle measures, efficient follow-up, and linkages to KPNC clinical and financial data sources, HALT holds promise for future research and could provide important insights for people diagnosed with CAD and/or T2DM, as well as the health facilities that care for them.
Other programs have intervened on diet and lifestyle behaviors to improve heart disease related outcomes.25,26 The Lifestyle Heart Trial (LHT), a randomized clinical trial (RCT) conducted between 1986 and 1992, 27 was among the first RCTs to report on the benefits of comprehensive lifestyle changes (including low-fat vegetarian diet, increased moderate exercise, smoking cessation, and stress management) on coronary atherosclerosis. 13 After 1 year of follow-up, the study reported 82% of participants in the intervention group having had a change towards coronary disease regression. 13 The LHT has since developed into an ongoing independent diet and lifestyle intervention program referred to as undo it with ornish (UIWO), 28 which employs similar interventions that were examined during the LHT. 28 While UIWO is covered by Medicare and some health insurance companies, it is not well integrated into any specific medical system. 28
The HALT program has several important differences in comparison to UIWO, the greatest difference is that the HALT program is based within a large, demographically diverse, integrated healthcare system serving over 4.6 million members in Northern California. Although the HALT program is currently offered only at the KPSSC medical center (serving roughly over 200 000 members), there are efforts underway to evaluate the program for potential expansion into other KPNC medical centers. As an integrated healthcare setting, members are identified and directly encouraged by their own physicians and pharmacists to participate in the program, enrollment and access is efficient and relatively straight forward, and health histories via EHR are easily accessed by program administrators. This may be especially important for increasing motivation and participation by individuals who might otherwise not seek out such a program on their own.
The existing KPNC infrastructure also allows for use of standing resources which may reduce costs and increase efficiency. For example, KPSSC mental health resources are incorporated directly into the HALT program for participants who are struggling with behavior change and need extra attention. Also, an interdisciplinary team of KPSSC physicians, psychologists, pharmacists, health coaches, and program assistants come together on a weekly basis to discuss specific participant needs and determine how to best help them be successful. Additionally, the integrated healthcare system provides a feedback loop from the program administrators back to the healthcare physicians and pharmacists, allowing for participant clinical treatments and medications to be adjusted when necessary.
Regarding specifics of the program, while UIWO is comprised of 18 4-hour sessions over a 9-week period, 28 HALT has 10 2-hour sessions in conjunction with 10 15-minute one-on-one counseling sessions over a 5-month period. Additionally, HALT provides participants with optional 1-hour healthy lifestyle maintenance classes for as long as the participant desires. This extended version of the intervention was made by design to provide the participant with longer exposure to the intervention and increase the possibility of long-term adherence. Both UIWO and HALT encourage a healthy diet with 10–15% of calories derived from fat, however, while the UIWO diet allows for egg-whites and some non-fat dairy consumption, 27 the HALT program encourages consuming a diet completely free from any animal-based foods. It has been shown that adhering to a vegan diet allows for more consumption of overall nutrients, such as magnesium, potassium, iron, thiamin, riboflavin, folate and vitamins, and less total fat. 29
Another diet and lifestyle intervention program for the treatment of heart disease was The Coronary Health Improvement Project which began in 1988. 25 In 2012, it became known as the Complete Health Improvement Program (CHIP) as it expanded its focus onto other chronic diseases such as T2DM, depression and sleep disorders. 25 Much like UIWO, CHIP is a third-party program and not formally integrated into any larger healthcare system. 30 A Canadian study of 1003 CHIP participants between the years of 2005 and 2011, showed significant overall reductions in BMI (−3.1%), systolic blood pressure (−7.3%), diastolic blood pressure (−4.3%), total cholesterol (−11.3%), low-density lipoprotein cholesterol (−12.9%), triglycerides (−8.2%), and fasting blood sugar (−7.0%) after adhering to the program for a 30-day period. 31 Other studies of the CHIP program have reported similar findings.32-34
Like both UIWO and HALT, CHIP provides a dietary, lifestyle and stress management intervention program with the goal of treating and reversing chronic diseases. 25 While UIWO focusses on heart disease and HALT on CAD and T2DM, CHIP seeks to treat an array of chronic conditions including heart disease, diabetes, cancer, osteoporosis, depression, and sleep disorders.25,30 CHIP delivers 18 group sessions over a 6- to 12-week period (depending on the specific program), with each session being 1 to 1.5 h long as compared to 4 hours for UIWO and 2 h for HALT. 25 Like UIWO, CHIP does not provide any one-on-one coaching sessions, nor does it provide optional follow-up maintenance classes. CHIPS’s dietary intervention is similar to that of the HALT program in that it encourages a diet completely free of animal-based foods; however, one major difference is that approximately half of each CHIP class involves the viewing of a prerecorded educational video. 25
Underlying both the CHIP and HALT programs are elements from behavioral change theories. While CHIP uses the Theory of Planned Behavior to assert that behavior is driven by intention which can be ultimately changed by influencing attitudes, 29 HALT draws upon an integrated approach across several behavioral change models (Health Belief Model, Social Cognitive Theory, and Transtheoretical Model) to facilitate behavior change that goes beyond set intentions and mindset. It does so, by focusing on evidence-based strategies and teaching skills to problem-solve and overcome challenges. HALT also incorporates goal-setting using SMART criteria to set short-term achievable goals, which is important for increasing self-efficacy, 21 and supports long-term change through ongoing group support sessions and resilience training.
Unlike UIWO and CHIP, the HALT program specifically highlights the treatment of T2DM. Though CHIP also targets the treatment of T2DM, it does so as one of several chronic diseases that it addresses. The HALT program emphasizes the treatment of T2DM due to the abundance of research in recent years which supports a WFPB diet and lifestyle behavior modifications for the treatment of T2DM. A recent meta-analysis of 14 studies showed a 75% lower risk of incident diabetes for those considered to have followed the healthiest lifestyle compared to those that had the least healthiest lifestyle. 35 The same study also demonstrated a 56% lower risk of all-cause mortality among individuals with T2DM when comparing the healthiest lifestyle with the least healthy lifestyle. 35 In a 74-week randomized control trial, a low-fat vegan diet appeared to improve blood sugars, insulin sensitivity, and plasma lipids more than a conventional diabetic diet. 6 In another meta-analysis of 28 studies, healthy lifestyle modifications significantly lowered HbA1c levels among type 2 diabetics in the intervention group as compared to those receiving usual care. 36 The authors of this study concluded that “lifestyle intervention is more effective than the standard care regarding the glycemic control of type 2 diabetic patients, particularly when there is weight loss. It is time to translate this evidence to the primary healthcare practice.” 36
Conclusion
CAD is the leading cause of death in the US and T2DM has reached epidemic proportions. Both diseases incur direct costs of hundreds of billions of dollars and are major public health concerns while also leading to increased suffering and disability. Evidence has shown that comprehensive diet and lifestyle interventions can greatly reduce the health and financial burdens of both diseases.
Here, our intention was to describe the HALT program, its participants, as well as program adherence and data collection activities. HALT is an ongoing diet and lifestyle intervention program provided to a large and demographically diverse integrated health system, which utilizes a low-fat WFPB diet, physical exercise, and resiliency to improve patient outcomes related to CAD and T2DM and to lower hospital costs. While there are eligibility requirements to join HALT, participants are generally representative of the larger KPSSC population of members with CAD and/or T2DM. With exceptionally well characterized diet, lifestyle and clinical data from both self-administered questionnaires and electronic health records, the HALT program is poised to inform new strategies for improvement of CAD and T2DM prognosis and can help contribute to future research to benefit this large and ever-growing population.
Footnotes
Acknowledgments
We gratefully acknowledge the HALT program participants for their vital contributions to this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by funding from The Permanente Medical Group (TPMG). Funders were not involved in the study design, collection, analysis, and interpretation of the data and have no restriction regarding publication.
Data Sharing
Data described in this manuscript will be made available upon request.