
Abstract
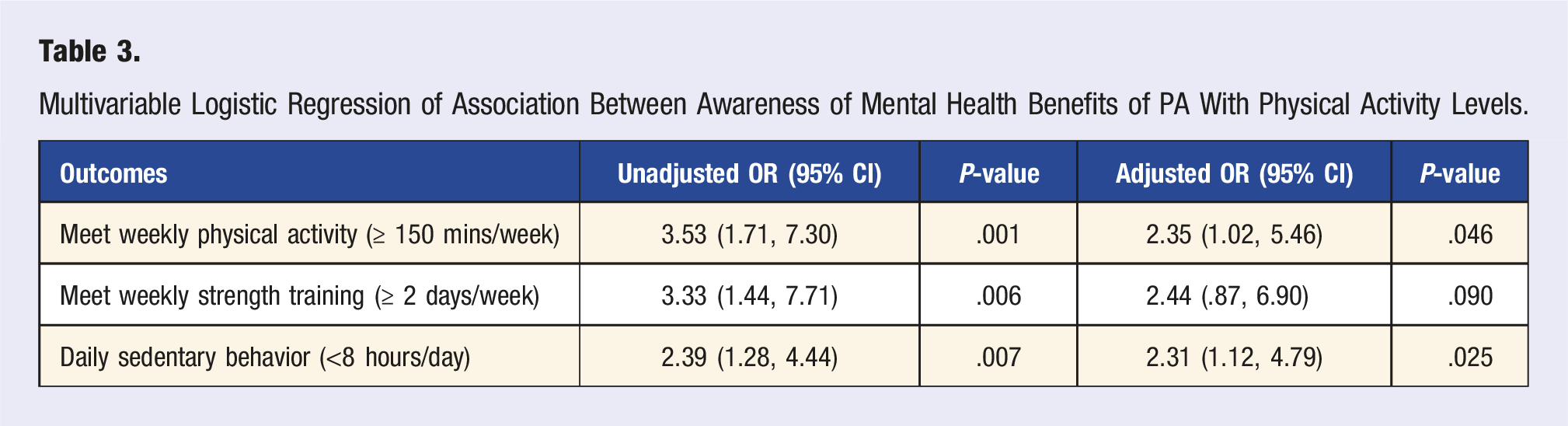
Objective: To examine the prevalence of awareness of PA (physical activity) benefits among those with mental disorders and explore how this is related to actual PA levels in this population. Methods: We queried data from the Health Information National Trends Survey 2019. A sample of 1,139 adults with self-reported depression and anxiety (61% female; mean age of 52.5 years) was analyzed. Multivariable logistic regression was employed to investigate the association between awareness that PA benefits mental health and respondents’ levels of PA. Results: Of the entire sample, a total of 904 individuals (80.9%) endorsed awareness that PA helps reduce symptoms of depression and anxiety. In multivariable analysis, awareness that PA improves mental health was significantly associated with greater odds of being less sedentary (OR 2.31; P = 0.025) and meeting national recommendations for weekly physical activity (OR 2.35; P = 0.046). Conclusion: Overall, findings from this nationally representative survey data indicates that about 4 in 5 adults living with depression and anxiety in the United States endorsed awareness of the mental health benefits of PA. Furthermore, we found that the awareness of these benefits is related to PA engagement.
People who experience more severe SDOH, including being of lower socioeconomic status, may experience fewer opportunities to be active due to lack of green space, poor neighborhood safety, and lack of time due to work and family obligations.
Introduction
Mental health conditions remain a leading cause of morbidity and mortality worldwide. In the United States, the burden of mental illness continues to grow. Data from the National Institute of Mental Health NIMH estimated that in 2020, about 1 in 5 U.S. adults live with a mental illness (52.9 million people). 1
People living with mental illness have substantially higher mortality rates than the general population. 2 Despite elevated unnatural causes of death (i.e.,, suicide), physical diseases account for more than two-thirds of deaths among people with mental disorders. 2 More so, it appears that this group is not experiencing the improved life expectancy seen in the general population over the last several decades. 2 This differential mortality has been attributed to several causes including social determinants of health, access to quality of healthcare, adverse effects of medications, as well as behavioral and lifestyle factors that increase the risk of obesity and cardiovascular diseases among this vulnerable population. 3
Physical activity (PA) has been widely recognized as a protective factor against obesity and cardiovascular risk factors in the general population. 4 More recently, systematic reviews and meta-analyses suggest that it also confers protection against the onset of mental disorders, and reduces psychiatric symptoms in those living with such conditions.5,6 Physical activity is thought to confer mental health benefits through neuroplasticity, reduced inflammation and oxidative stress, modulations of the endocrine system, and increase in social interactions and self-efficacy. 7 Physical activity has been extensively studied across the spectra of mental disorders, and is promising as a feasible intervention to reduce morbidity and mortality, and to improve quality of life. 8 Based on this evidence, some leading healthcare organizations have included lifestyle interventions such as physical activity as a critical component in the care of people with common mental disorders such as depression and anxiety. 9
Despite the widely acknowledged benefits of PA for mental health, those with mental illness are at higher risk of sedentary behavior and physical inactivity than the general population.10,11 People living with mental illness face many barriers to engaging in physical activity, including low mood and other symptoms of psychiatric illness (i.e.,, low energy, anhedonia), lack of confidence, physical health problems, and lack of support. 12 Additionally, promoting adoption and maintenance of PA among those with mental illness is a challenge influenced by social determinants of mental health such as demographic, social, cultural, and physical environmental factors. 12
Studies in the general population have found that knowledge about the benefits of PA is an important predictor of PA adoption.13-15 However, there is scant data regarding the awareness of PA benefits among those living with mental illness. More so, little is known about the relationship between awareness of the mental health benefits of PA and engagement in regular PA among those with mental illness. Understanding these associations may help guide future interventions aimed at improving PA adoption among individuals with mental illness.
Therefore, using a nationally representative sample, this study sought to examine the prevalence of awareness of PA benefits among those with mental illness (specifically those with depression and anxiety), and explore how this knowledge is related to actual PA levels in this population.
Methods
Overview of the Health Information National Trends Survey
For this study, we examined data from the 2019 Health Information National Trends Survey HINTS 5, Cycle 3 (H5c3). The HINTS is a nationally representative survey administered in multiple iterations by the National Cancer Institute (NCI). As with all previous iterations of HINTS, the target sample for H5c3 was non-institutionalized, civilian adults (aged ≥18 years) living in the United States (U.S). Data collection for H5C3 began in January 2019 and concluded in May 2019.
The HINTS collects data from the general population related to health information communication technology, and health behaviors. Unlike previous iterations of HINTS 5 (cycles 1 and 2), H5c3 included a self-administered mailed questionnaire, as well as two experimental web options. In addition, there was a greater emphasis on behavioral health and lifestyle factors (e.g.,, diet, physical activity, tobacco smoking) as compared to previous HINTS versions. 16
The sample frame for H5c3 was derived using the Marketing Systems Group database of addresses and included all nonvacant residential addresses in the United States. This was then grouped into two specific sampling strata: high concentrations of minority populations (from areas with at least 34% population proportion of Hispanics or African Americans), and low-concentration minority populations (from areas with less than 34% population proportion of Hispanics or African Americans). H5c3 utilized the next-birthday method for respondent selection. In this method, households from residential addresses across the U.S. are first selected using an equal-probability method, then one adult within each household is selected to participate in the survey. Written informed consent for H5c3 was obtained from study participants. The Westat institutional review board approved H5c3, and it was classified exempt from review by the US National Institutes of Health Office of Human Subjects Research Protections. As this secondary analysis involves a de-identified, publicly available dataset, institutional review board approval was not required. Full details about the HINTS methodology and data collection have been published elsewhere.16,17
Study Design and Participants
A cross-sectional design was used to examine participant responses from H5c3. The total number of targeted households for the H5C3 sample was 23 430 and data were obtained from 5438 respondents who completed at least 50% of the survey (with 5247 of these completing 80% or more). This sample was then weighted to adjust for between-respondent differences in within-household probability of selection and post-stratified to adjust for discrepancies between the sample and the population with respect to age, sex, educational attainment, race, ethnicity, and census region.
The overall household response rate was 30.3% and was comparable to previous cycles of HINTS. 18 For the purposes of this study, respondents were separated into two groups: (i) depression and anxiety group and (ii) control group. The groups were determined from responses to the survey item on depression/anxiety diagnosis, as noted in the measures section below. As in previous studies, participants who responded “Yes” were classified as having depression or anxiety. 19 Of the complete sample, approximately 1169 participants self-reported a history of depression and or anxiety disorder (23.6% weighted prevalence) and were used in the final analysis. Also, 2.41% (131/5438) of observations were with missing data for depression/anxiety status and these were omitted in the final analysis.
Measures
The primary objective of this study was to investigate the relationship between awareness that PA helps reduce depression and anxiety and levels of physical activity among those with depression and anxiety. To answer this, we used information derived from survey items within H5c3, as follows.
Sample Population: Self-Reported Diagnosis of Depression or Anxiety
Individuals with depression and anxiety were determined using the answer of the participant to the question, “Has a doctor or other health professional ever told you that you had depression or anxiety disorder (yes/no)?”
Exposure: Awareness of Mental Health Benefits of Physical Activity
Awareness that physical activity helps reduce depression and anxiety was determined from the following survey question “As far as you know, does physical activity help reduce depression and anxiety?” Response options were “Yes,” “No,” and “I don’t know.” Those who answered yes were classified as having awareness that physical activity reduces depression and anxiety, and others were classified as not having awareness.
Outcome: Physical Activity Parameters
We examined the association between awareness that physical activity helps reduce depression and anxiety and whether participants reported achieving the national recommended levels of (i) general physical activity (≥150 minutes per week), (ii) weekly strength exercise training, and (iii) weekly level of sedentary behavior, as described below.
Physical Activity
Physical activity level was derived using the following two questions: (i) in a typical week how many days do you do any physical activity or exercise of at least moderate intensity, such as brisk walking, bicycling at a regular pace, and swimming at a regular pace? (8 response options ranging from none to 7 days per week) and (ii) on the days that you do any physical activity or exercise of at least moderate intensity how long do you do these activities? (2 response options for minutes and hours). Based on the World Health Organization’s recommendation on physical activity for adults, 4 we reclassified the response options into a single dichotomous outcome variable for physical activity, that is, whether the subject (i) met physical activity recommendations (≥150 minutes per week) or did not meet the physical activity recommendations (<150 minutes per week).
Sedentary Behavior
Participants weekly levels of sedentary behavior was determined from the survey question “During the past 7 days, how much time do you spend sitting on a typical day?” Based on previous literature regarding recommendations on sedentary for adults,20,21 we reclassified the response options into a single dichotomous outcome variable for sedentary behavior, that is, whether the subject (i) met criteria for sedentary behavior (if they spent 8 or more hours of time sitting in a day) or (ii) did not meet criteria for sedentary behavior (spent less than 8 hours of time sitting in a day) in the preceding week.
Strength/Resistance Training
Respondents’ level of strength training was ascertained from the survey question “In a typical week, outside of your job or work around the house, how many days do you do leisure-time physical activities specifically designed to strengthen your muscles?” Based on CDC recommendation of 2 or more days a week of muscle strengthening activities that work all major muscle groups, we reclassified the response options into a single dichotomous outcome variable for resistance strength training, that is, whether the subject (i) met resistance strength muscle training recommendations (≥2 days a week) or (ii) did not meet the resistance strength muscle training recommendations (<2 days a week)
Sociodemographic and Health-Related Variables
We included available sociodemographic and health-related variables to examine their associations with the study outcomes such as age (18–34, 35–49, 50−64, and 65+ years old), gender (male/female), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and other), education level (less than college and college or above), annual household income (less than $20k, $20k to less than 35k, $35k to less than 50k, $50k to less than 75k, $75k or above), census region, urban/rural, body mass index (BMI, less than 30, 30 or above), and marital status. The health-related factors included access to a healthcare provider and number of medical comorbidities.
Statistical Analyses
Statistical analyses were performed using the “svy” command in Stata 17.0 statistical software (StataCorp LP, College Station, Texas, USA). Final person weights and jack-knife replicate weights provided within the H5c3 dataset were used to estimate national level values and standard errors of estimates, respectively. Descriptive statistics were conducted for the entire study sample and for individuals with and without awareness of the mental health benefits of physical activity. Both unweighted frequencies and weighted percentages were also calculated. Differences in meeting recommended guidelines for daily sedentary behavior, weekly strength exercise training, and weekly minutes of physical activity between individuals with depression/anxiety who had knowledge of the mental health benefits of physical activity and those who did not were assessed using chi-squared tests. To evaluate the relationship between awareness of physical activity’s mental health benefits and respondents’ levels of physical activity, we performed multivariable logistic regression analysis, adjusting for sociodemographic variables of age, gender, race, marital status, household income, access to a health provider, education, geographical residence, census region, and body mass index. Statistical significance was set at P < .05.
Results
Sample Characteristics
Sample Population Demographic Characteristics: Sample N = 1139.
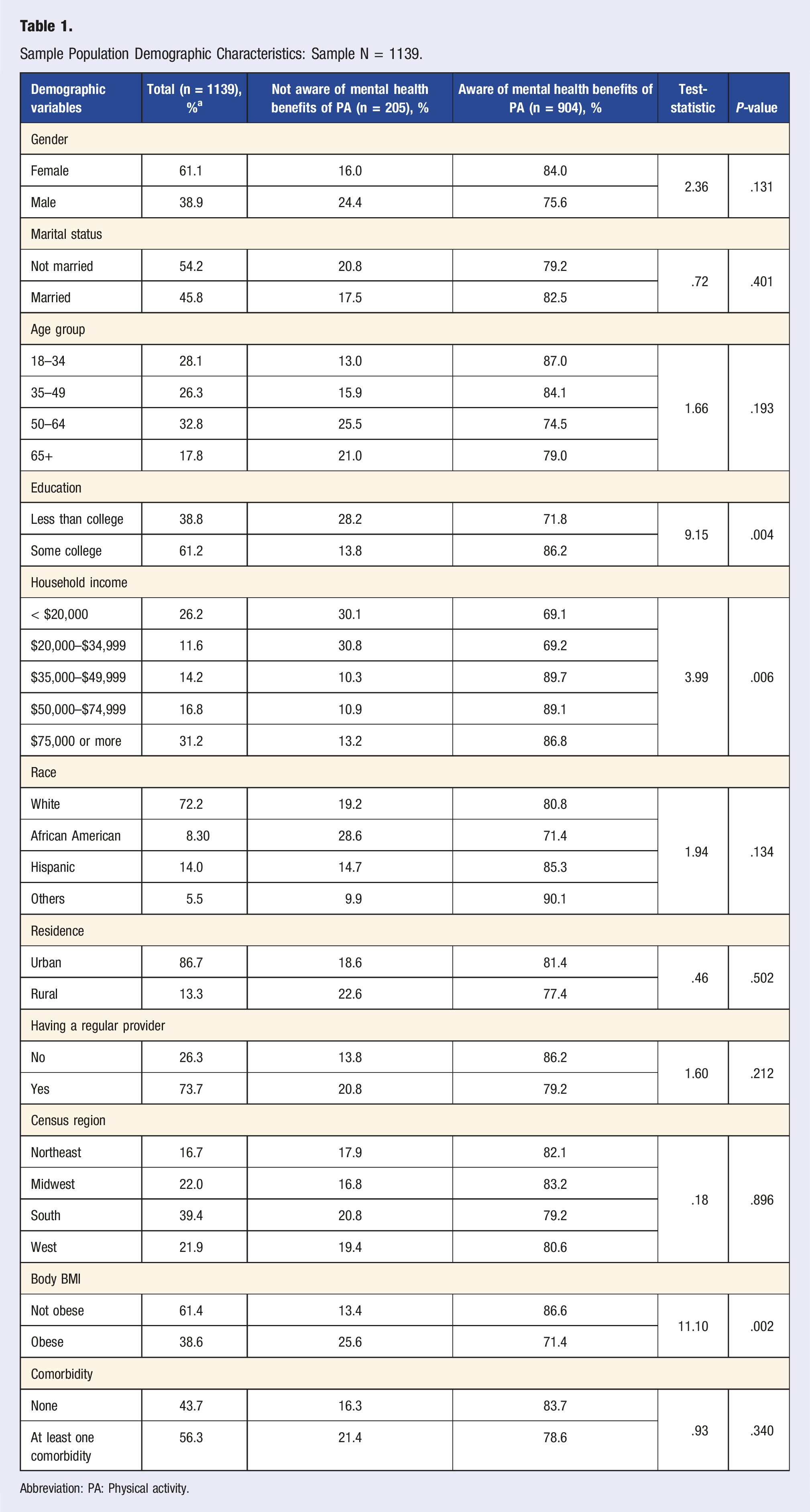
Abbreviation: PA: Physical activity.
In bivariate analysis (Table 1), among individuals with depression and/or anxiety, those who endorsed awareness that PA has mental health benefits were more likely to be college graduates or more (86.2%) vs people with less than a college education (71.8%), and people with high income (86.8% were from households with annual income ≥US$75,000) vs people with lower income (69.1%) were from households with annual income ≤ US $20,000). Regarding race, 85.3% of Hispanics, 80.8% of Whites, and 71.4% of Blacks reported awareness that PA helps reduce symptoms of depression and anxiety.
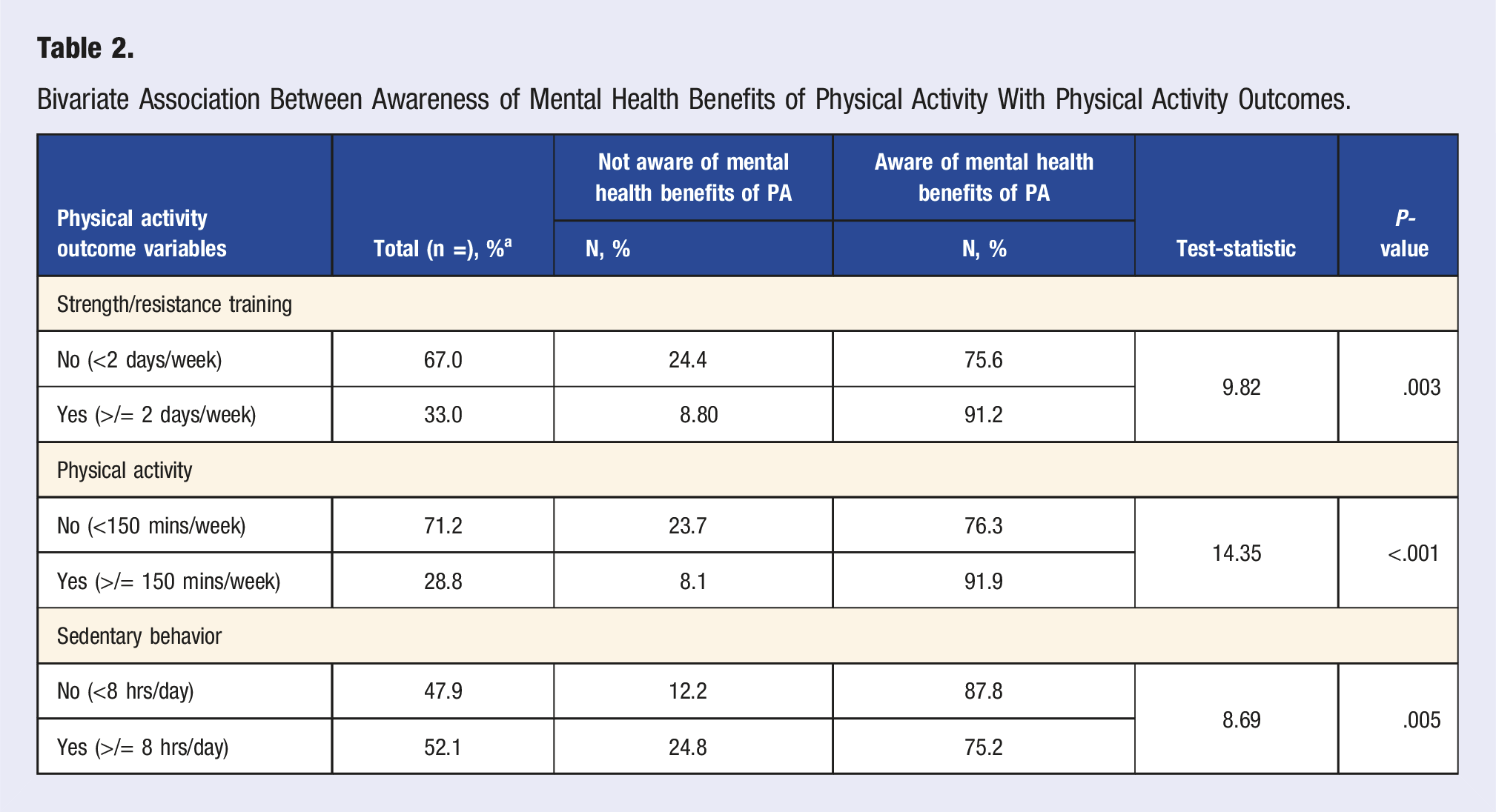
Bivariate Association Between Awareness of Mental Health Benefits of Physical Activity With Physical Activity Outcomes.
Multivariable Logistic Regression of Association Between Awareness of Mental Health Benefits of PA With Physical Activity Levels.
Discussion
The primary objective of this study was to examine the levels of awareness of mental health benefits of PA, as well as evaluate the association between awareness of the mental health benefits of PA and actual physical activity engagement among individuals with mental disorders. Specifically, we examined the associations with weekly physical activity, weekly resistance exercise, and sedentary behavior, among individuals with self-reported diagnosis of depression and anxiety, drawing from a nationally representative sample of the adults in the United States.
We found evidence that large proportions of individuals with depression and anxiety have knowledge of the mental health benefits of PA, and furthermore that these individuals are significantly more likely to meet weekly recommended levels of PA, and to be less sedentary than their peers. These findings are encouraging, as they suggest that many adults with depression and anxiety are aware of the benefits of PA for their condition and feel able to engage in sufficient levels of activity, perhaps on the basis of this. Alongside this, the results could further indicate that increasing the awareness of the mental health benefits of PA among individuals with depression and anxiety who are currently inactive may be a beneficial strategy for enhancing PA uptake and adherence.
An alternative interpretation of our results could be said to demonstrate that “awareness of PA benefits” is driven by individuals’ personal experience of mental health benefits (or lack thereof) from physical activity—whereby those with depression and anxiety who do not feel noticeably different from exercising are thus less likely to engage in PA in future. This could be driven by individual differences in mental health etiology/pathology, the types of PA engaged with, or physical limitations towards engaging and benefitting from PA (as participants in our sample who did not report awareness were more likely to be obese). 22 People who experience more severe SDOH, including being of lower socioeconomic status, may experience fewer opportunities to be active due to lack of green space, poor neighborhood safety, and lack of time due to work and family obligations. To attempt to overcome these factors, it would be worthwhile for primary care and mental health providers to incorporate the assistance of physical activity professionals in conceptualizing personalized and creative ways to motivate and help individuals living with mental disorders to integrate suitable forms of physical activity into their daily lives, which are well-aligned with their own goals, preferences and capabilities.
Our findings also highlight that (SDOH) social determinant of health (specifically income and level of education) may play significant roles in having awareness of the mental health benefits of PA. Such information and awareness may be less accessible to groups who experience higher levels of social deprivation, 23 and health professionals should consider innovative and lower-cost ways to disseminate health information to persons with mental health needs. For example, research suggests that digital tools (e.g.,, smartphones, apps, and wearables) are an increasingly popular option for individuals with mental health needs to receive relevant health information, 24 especially as literacy in technology becomes more common 25 and more free and low-cost tools become regularly available. Future research may explore how individuals across diverse populations with mental health needs currently access and prefer to receive physical health information.
Limitations of the study are noted. Findings are restricted to cross-sectional data and cannot inform trends of knowledge of the benefits of PA for mental health or the impact on PA behaviors over time. The cross-sectional nature of our study also limits our ability to infer causal relationships. Data are also restricted to persons living in households and who were able to respond to the survey. Sample population consisted of individuals with depression and anxiety and findings cannot be generalized to a broader mental health population such as those with psychotic illness. Additionally, the sample relied on individuals self-reporting of either current or previous diagnoses of depression/anxiety, and this could not be validated against health record data. However, self-reported physician/health provider diagnosis of depression/anxiety has been used in several studies 17 across different national US population level surveys26,27 and this measure has also been found to have strong psychometric properties. 28 Another limitation is that it was not possible to ascertain the current status of the diagnosis and whether those who responded affirmatively to depression or anxiety had already received treatment and were no longer impacted by their disease. Also, the survey questions in the HINT dataset precludes any ability to examine other theoretically relevant factors such as neighborhood characteristics, severity of mental illness, and receipt of mental health treatment which may have confounded our findings. Lastly, since PA data were captured by self-report, the possibility of recall bias, and social desirability bias cannot be excluded. Although self-reported PA measures often over-estimate PA levels when compared to device-based PA measurements, 29 they remain a cost-effective means of collecting PA data for population surveillance and continue to be utilized in multiple public health intervention studies. 30
Therefore, future research may include longitudinal data sets, utilize objective PA measures, examine the experiences of persons with mental disorders in context of those currently receiving psychiatric treatment, and examine how knowledge of other psychosocial and cardiovascular benefits of PA may influence PA engagement.
Conclusion
Overall, the findings from this nationally representative survey study data show that the mental health benefits of PA are widely acknowledged among individuals with depression and anxiety, and furthermore that the awareness of these benefits is related to PA engagement. However, disparities in awareness of PA benefits exists, especially for those with low SDOH. Future large-scale studies should focus on PA and exercise program tailored to reach mental health populations that experience poorer social determinants of health as well as eliminating barriers to PA engagement among such groups.
Footnotes
Acknowledgments
JF is supported by a University of Manchester Presidential Fellowship (P123958) and a UK Research and Innovation Future Leaders Fellowship (MR/T021780/1) and has received honoraria/consultancy fees from Atheneum, ParachuteBH and Nirakara, independent of this work. JT is supported by a research fellowship from the American Psychiatric Association Foundation and the American Psychiatric Association. CC has received research support from BioXcel Pharmaceuticals and honoraria from Sunovion Pharmaceuticals independent of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Time for analysis and article preparation was funded by the National Heart, Lung, and Blood Institute through grant R01HL155301 (C.C.) and grant R01HL133149 (J.H.).