
Abstract
“Fewer responses for evidence-based strategies and more responses for strategies with limited evidence suggest older adults, in particular, lack awareness of effective fall prevention strategies.”
Introduction
In 2018, there were about 36 million falls reported among older adults (ages 65 and older) with over 8 million fall-related injuries. 1 Older adult falls can result in serious injuries such as hip fracture or traumatic brain injury, often requiring hospitalization and resulting in nursing home placement.2-4 Falls in older adults, while common, are not a normal part of aging. There are known modifiable risk factors that place older adults at a higher risk of falling or sustaining an injury from a fall. 5 Some of the major modifiable risk factors identified include gait and balance disorders, medication use, vision impairment, and problems with feet or footwear.5,6
Effective strategies targeting modifiable risk factors can reduce falls and fall-related injuries in older adults.6,7 Multifactorial interventions encourage providers to select from multiple evidence-based strategies to create a tailored prevention plan unique to the older adult’s modifiable risk factors. Multifactorial approaches have been shown to reduce falls by about 24%. 8 Despite effective fall prevention strategies, healthcare providers face barriers to screening their patients that have resulted in low uptake. 8 These barriers include a lack of time during office visits and a lack of knowledge and training in effective fall prevention strategies.9,10 Similarly, barriers for older adults stem from misconceptions about fall risk. These include older adults either reporting not being at risk for a fall or thinking that they would not sustain a serious injury from a fall, thereby limiting their engagement in fall prevention strategies.11-13 Older adults frequently report being more careful and slowing down to prevent falling. Though such actions may reduce fall risk to some extent, more proactive, evidence-based strategies that address modifiable risk factors can resolve the underlying problem and are potentially more effective in reducing falls.14,15
The Centers for Disease Control and Prevention (CDC) developed the Stopping Elderly Accidents, Deaths, and Injuries (STEADI) initiative (www.cdc.gov/STEADI) to provide tools and resources to assist healthcare providers with fall prevention efforts. The initiative is based on the American and British Geriatrics Societies’ clinical practice guideline and incorporates healthcare provider feedback.16,17 The STEADI initiative recommends evidence-based strategies to reduce fall risk such as referral to physical therapy, making home modifications, addressing visual impairments, and assessing and modifying medications likely to increase fall risk.
Older adults and healthcare providers can take actions to reduce fall risk and prevent injury with advancing age. Understanding their fall prevention beliefs is necessary to develop effective programs to increase awareness about fall risks and evidence-based strategies to reduce this risk. The aim of this study is to describe and compare older adults’ and healthcare providers’ knowledge of fall prevention strategies. These include both evidence-based strategies and those with limited evidence supporting their effectiveness.
Methods
Surveys
The data for this analysis came from the 2019 Porter Novelli ConsumerStyles and DocStyles surveys. In 2019, ConsumerStyles was conducted via Ipsos’ KnowledgePanel®. KnowledgePanel® is an online panel that is representative of the non-institutionalized U.S. population. 18 Panel members are randomly recruited by mail using probability-based sampling by address to reach respondents with or without a landline phone and internet access. If needed, households were provided with a device and access to the internet. Respondents receive cash-equivalent reward points for their participation which can be redeemed online for gift cards and prizes. Participants are invited to participate in three surveys during the year (spring, fall, and winter).
Data for this study used the fall wave or FallStyles. FallStyles was fielded from 10/8/2019 to 10/22/2019. The survey was sent to a sample of 4677 adult panelists. Email reminders were sent to non-responders on days 3, 7, and 11 of the field period. The median survey completion time was approximately 33 minutes. Respondents were not required to answer any of the questions and could exit the survey at any time. Respondents who did not answer at least half of the questions or completed the survey in 5 minutes or less were removed from the data as incomplete (n = 12). A total of 3624 adults completed the survey for a response rate of 77.5%. The data were weighted to match the U.S. Current Population Survey proportions using eight factors: gender, age, household income, race/ethnicity, household size, education, census region, and whether or not they lived in a metropolitan area. For our study, we limited analysis to older adults of ages 65–74 and ages 75 and older.
DocStyles, a web-based survey of healthcare providers, was fielded from 10/03/2019 to 11/04/2019. Quotas were set to reach 1000 primary care physicians, 250 OB/GYNs, 250 pediatricians, and 250 nurse practitioners/physician assistants. Respondents were paid an honorarium of $40–$85 for completing the survey based on the number of questions they were asked to complete.
The DocStyles survey was conducted by SERMO, a physician-focused platform used for market research. 19 SERMO’s Global Medical panelists have their identity and employment verified using a double opt-in sign up process with telephone confirmation at place of work. SERMO invited its currently active panel members based on how active they have been on previous surveys, where responders who answer more than 75% of a previous survey are invited first, followed by medium-active and less active respondents. All invitations included a link to the web-based survey.
Respondents were screened to include only providers who practice in the United States; actively see patients in an individual, group, or hospital practice; and who have been practicing for at least three years. Respondents were not required to participate and could exit the survey at any time. To protect respondent confidentiality, no personal identifiers were recorded.
The survey was sent to a total of 2696 providers with a response rate of 65% (PCP: 67%, NP/PA: 60%). For our study, we limited respondents to primary care physicians (PCP), nurse practitioners (NP), and physician assistants (PA). We grouped NP and PA to ensure sufficient sample size. Providers who practiced in an inpatient setting, and providers who did not have any older adult patients were excluded from this analysis, resulting in a final sample of 1022 respondents: PCP n = 829 and NP/PA n = 193.
Study Variables
Demographic characteristics were recorded for survey respondents. For FallStyles, demographics included age, gender, race/ethnicity, and household region. For DocStyles, demographics included age, gender, race/ethnicity, practice region, years in practice, and percent of older patients (age 65 and older) seen.
Two questions were used to gauge beliefs about fall prevention (Figure 1). The first question asked, “Older people fall and there is nothing that can be done about it,” and responses were dichotomized into agree/strongly agree and disagree/strongly disagree. The second question asked respondents to select all activities that help older people prevent falls. Activities that address specific fall risk factors and are supported by research showing a significant reduction of fall risk were categorized as evidence-based strategies.20-31 All others were categorized as strategies with limited evidence. Responses of “don’t know/not sure” (n = 9 older adults, n = 2 providers) or “nothing can be done to prevent falls” (n = 6 older adults, n = 1 provider) were excluded from the analysis. Fall-related survey questions used to gauge older adults’ and healthcare providers’ beliefs about fall prevention.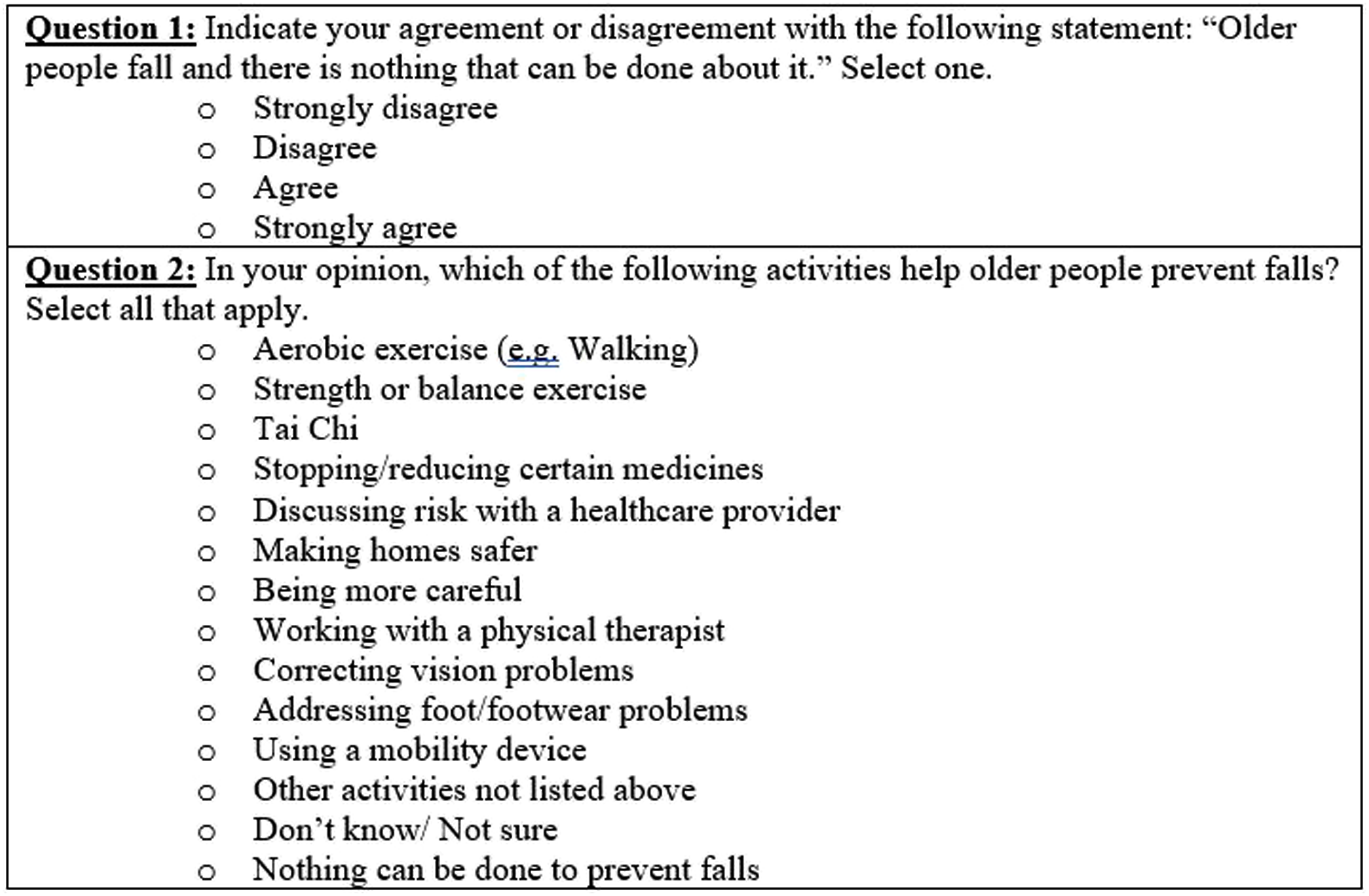
Frequencies and percentages, weighted for FallStyles and unweighted for DocStyles, were reported for all demographic variables. Chi-square tests were conducted to compare PCP and NP/PA responses for each demographic variable. Percentages, confidence intervals, and standard errors were obtained for all fall prevention–related variables using SAS 9.4. The estimates and standard errors were then used in Microsoft Excel to conduct two-way t-tests to make overall comparisons of providers and older adults. 32 A P-value less than .05 was used for significance.
Results
Demographics and Provider Characteristics of Healthcare Providers and Older Adults, DocStyles and ConsumerStyles, 2019.
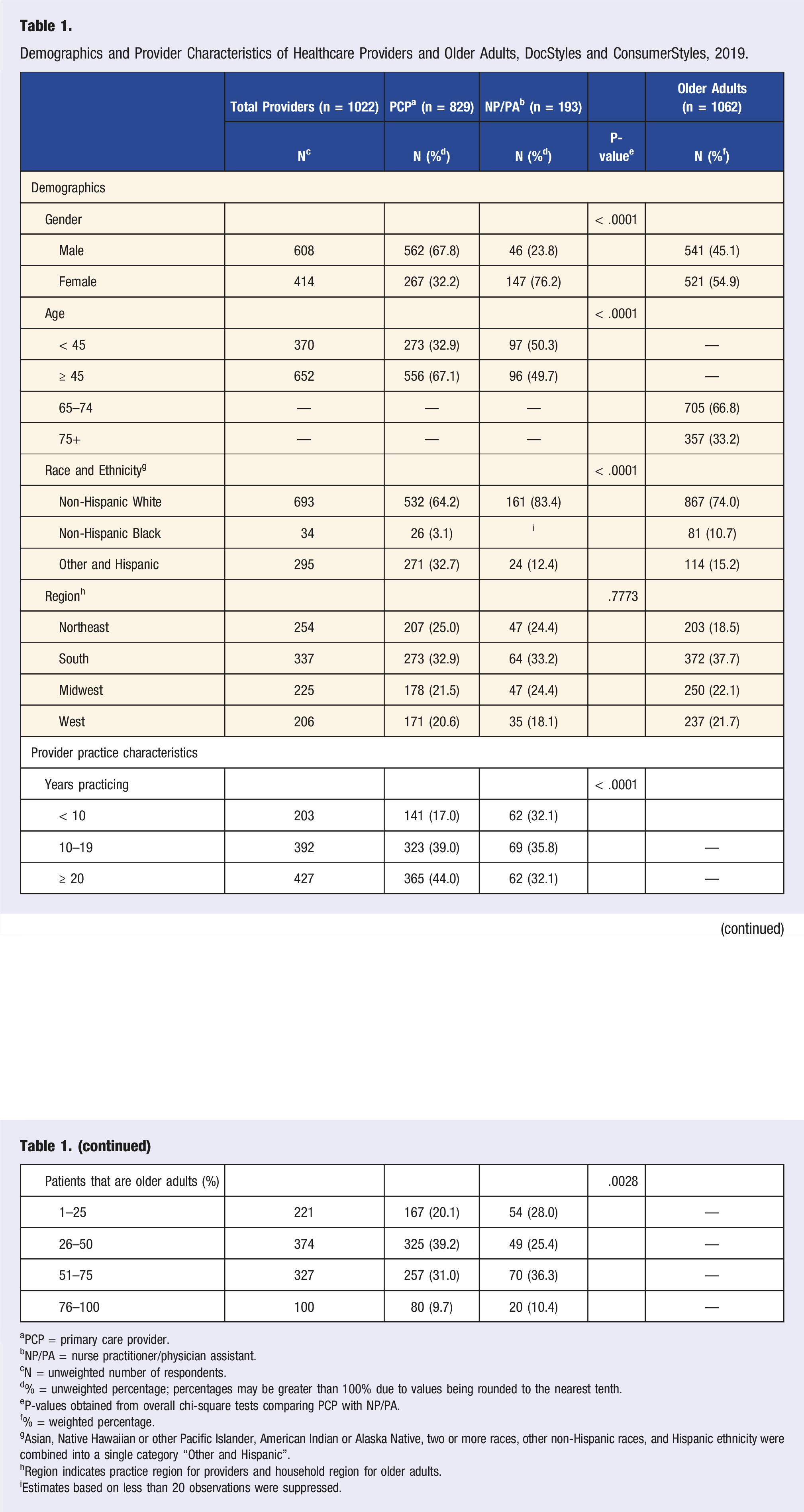
aPCP = primary care provider.
bNP/PA = nurse practitioner/physician assistant.
cN = unweighted number of respondents.
d% = unweighted percentage; percentages may be greater than 100% due to values being rounded to the nearest tenth.
eP-values obtained from overall chi-square tests comparing PCP with NP/PA.
f% = weighted percentage.
gAsian, Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, two or more races, other non-Hispanic races, and Hispanic ethnicity were combined into a single category “Other and Hispanic”.
hRegion indicates practice region for providers and household region for older adults.
iEstimates based on less than 20 observations were suppressed.
Beliefs About Fall Prevention Among Healthcare Providers and Older Adults, DocStyles and ConsumerStyles, 2019.
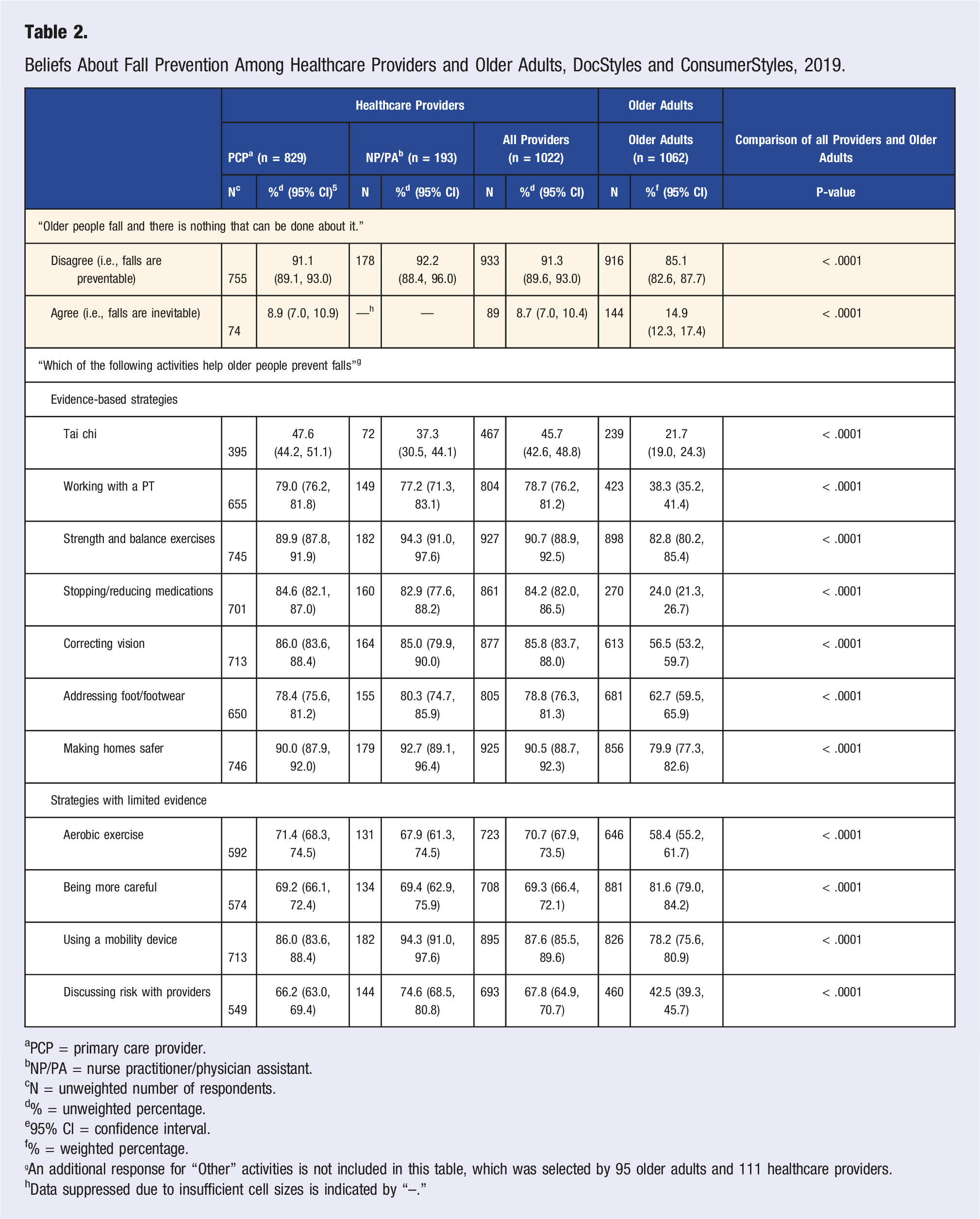
aPCP = primary care provider.
bNP/PA = nurse practitioner/physician assistant.
cN = unweighted number of respondents.
d% = unweighted percentage.
e95% CI = confidence interval.
f% = weighted percentage.
An additional response for “Other” activities is not included in this table, which was selected by 95 older adults and 111 healthcare providers.
hData suppressed due to insufficient cell sizes is indicated by “--.”
Older adults were most likely to recognize strength and balance exercises (82.8%) and making homes safer (79.9%) as ways to prevent falls. Less than half recognized working with a physical therapist (38.3%), stopping and reducing medications (24.0%), and tai chi (21.7%) as helping to prevent falls. When compared to older adults, there were significant differences in the proportion of providers who recognized the strategy across all evidence-based strategies (P < .05), with more providers indicating the strategy as helpful to prevent falls (Table 2). For tai chi, 45.7% of providers indicated tai chi as a strategy to help prevent falls compared to 21.7% of older adults (P < .0001). Compared with older adults, providers were more likely to consider physical therapy (78.7% vs 38.3%; P < .0001), strength and balance exercises (90.7% vs 82.8%; P < .0001), and modifying medications (84.2% vs 24.0%; P < .0001) as effective fall prevention strategies. For strategies with limited evidence, 58.4% of older adults thought aerobic exercise was effective for fall prevention. More older adults indicated that being more careful can help prevent falls (81.6%) compared to providers (69.3%; P < .0001).
Discussion
In this study, we described and compared fall prevention beliefs among healthcare providers and older adults. In general, both providers and older adults believed falls can be prevented, but older adults had lower recognition of several evidence-based strategies that could prevent falls. For most strategies, more healthcare providers than older adults selected evidence-based strategies as preventive against falls. More than twice as many healthcare providers as older adults indicated medication management can help prevent falls and less than half of both providers and older adults indicated tai chi can help prevent falls. These results suggest that while there is general understanding of the preventable nature of falls, both providers and older adults believe certain strategies with limited evidence (e.g., being more careful) can help prevent falls. However, older adults may be less aware of evidence-based strategies. Training and education material for healthcare providers can highlight specific ways to educate their older patients on the effectiveness of these strategies.
While the majority of providers and older adults indicated that strength and balance exercises can prevent falls in older adults, they are less knowledgeable about specific strategies such as tai chi and physical therapy. Similar findings have been reported in other analyses for healthcare providers.9,33 Tai chi, a martial art originating in China, addresses balance and stability through low-impact continuous weight-shifting movements and synchronized breathing. 34 These exercises have been found to be effective in preventing falls among older adults compared to regular exercise.35-37 However, our results suggest that few healthcare providers and even fewer older adults are aware of these benefits. Less than one-third of older adults in our analysis indicated that working with a physical therapist can prevent falls. While physical therapy is an effective strategy to address gait and balance issues in older adults, gaps in understanding the scope of the physical therapist’s role as part of the healthcare team can be a barrier to adherence. 38 An evaluation of a home-based fall prevention program reported that general practitioners and home care nurses were reluctant to implement the physical therapist’s recommendations for their patients, suggesting gaps in interdisciplinary cooperation. 39
About 80% of older adults and 90% of providers endorsed making homes safer as an effective strategy for preventing falls, and this analysis considered this an evidence-based strategy. The evidence supporting the effectiveness of home modifications in reducing fall risk is limited to assessments and modifications conducted by an occupational therapist.31,40-42 Further research is needed to fully determine the effectiveness of home assessments and modifications made without an occupational therapist.
Medication modification was a popular strategy indicated by providers, with approximately 9 in 10 providers selecting it as a fall prevention strategy. Medication management and regimen modification allows for routine evaluation of current medications for potentially inappropriate medications or polypharmacy and optimizing medications to reduce risk of adverse events. 43 While there is uncertainty that deprescribing or discontinuing fall risk–increasing medications as a stand-alone intervention is effective in reducing falls, it is an important component of multifactorial fall risk assessment and intervention.44,45 However, only a quarter of older adults noted that medication modification can reduce their risk of falls. This is consistent with previous findings that most older adults are not aware that their medications increase their fall risk. 46 In the Strategies to Reduce Injuries and Develop Confidence in Elders (STRIDE) clinical trial to determine effectiveness of evidence-based strategies to reduce falls, older adults who were assessed as needing medication management were much less likely to both prioritize it as an intervention (52.4%) and agree to address it (28.6%) compared with other strategies including strength and balance exercises (95.7% and 91.0%, respectively), addressing home safety hazards (80.6% and 50.1%, respectively), correcting vision impairment (87.8% and 67.3%, respectively), and addressing foot problems (82.9% and 50.7%, respectively). The unwillingness to address medication management may result from the low recognition of it as a strategy for reducing fall risk. 8
Both healthcare providers and older adults indicated that strategies with limited evidence could be helpful in preventing falls. Of note, 82% of older adults and 69% of providers indicated that being more careful can prevent falls. As adults age, they may be advised to slow down and take more care, sometimes understood to be common sense habits as the body becomes more frail. 47 It may also be a way to justify doing high-risk activities by being more mindful of how their own behavior can prevent them from falling. 48 Furthermore, over half of older adults and providers thought that aerobic exercise was helpful in preventing falls. The most recent Cochrane Collaboration systematic review of exercise to prevent falls found inconclusive evidence for programs that involved only aerobic activities such as dance or walking, whereas programs that included balance and functional exercises were effective. 49 Proposed exercise programs that combine aerobic with strength and balance training may reduce fall risk but have not been evaluated to show effectiveness at reducing falls. 50 The high proportions of healthcare providers and older adults who selected these strategies with limited evidence suggest a need for greater awareness to counter misconceptions about fall prevention.
The healthcare team can play a significant role in communicating with older adults about the importance of early and effective fall prevention. 51 Older adults trust their doctors; they report being open to discussions and view counseling as a chance to learn about their own fall risk.52,53 In fact, a previous cohort of DocStyles data reported 89.3% of providers discussed fall prevention with their patients. 33 Despite this, another analysis found that only 57% of older adults reported following through with a recommendation and none of the participants were able to recall recommendations other than exercise and home modifications. 53 Conclusive research is needed on the best ways to counsel older adults in a way that will encourage them to adhere to recommendations. 54 For tools and education materials, CDC’s STEADI initiative guides providers to interventions that address specific risk factors found in the screening and assessment of their older patient’s fall risk (www.cdc.gov/steadi/). For older adults, CDC’s Still Going Strong awareness campaign offers information on how to prevent common injuries, including from falls, as they age. 55
There are at least four limitations with this analysis. The survey for healthcare providers is not weighted and therefore cannot be generalized beyond the sample of this study. In this analysis, we compared the frequencies of two datasets that were not created with this specific study in mind. Due to the limited sample size, provider types were combined, which may have made subtle differences between the four provider types undetectable. Lastly, this analysis does not reflect beliefs around multifactorial approaches to fall prevention because we did not test combinations or interactions of strategies. Still, the results of this study provide insightful information on provider’s and older adult’s beliefs about fall prevention.
Conclusion
This study describes healthcare provider’s and older adult’s beliefs around fall prevention, highlighting differences and similarities in approaches to fall prevention. Both healthcare providers and older adults believe falls can be prevented. However, lower levels of response for evidence-based strategies (e.g., tai chi, working with a physical therapist, and medication management) coupled with higher levels of response for strategies with limited evidence (e.g., being careful and aerobic exercise) suggest older adults, in particular, lack awareness of effective fall prevention strategies. Because awareness is an important step toward behavior change, these results demonstrate where fall prevention can be improved. Members of the healthcare team, including lifestyle practitioners, can play a key role in advocating for fall prevention among older adults. Provider and patient communication can address knowledge gaps and work to integrate fall prevention into various clinical practice settings.
Footnotes
Acknowledgments
The authors would like to thank Rose Rudd, MPH and Laurie Beck, MPH for their collaborative work on this project.
Author Contributions
AH had full access to all of the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Study concept and design: AH, YH, and GB
Analysis of data/ Statistical analysis: AH
Interpretation of data: AH, YH, and GH
Drafting of the manuscript: AH and YH
Critical revision of the manuscript for important intellectual content: AH, YH, and GB
Final review and approval of manuscript: AH, YH, and GB
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Previous Presentation of the work
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.