
Abstract
Disordered eating includes both behaviors and cognitions and can cause many of the same negative health outcomes as clinically diagnosed eating disorders (e.g., growth retardation, nutritional deficiencies, and psychosocial disturbances). Compared to the general population, disordered eating is more common in college-age women. An experiment was conducted to test 8 expressive writing interventions in the context of disordered eating. Interventions were drawn from theory-based prevention programs, which included cognitive behavioral therapy, peer and media risk reduction, and cognitive dissonance theory. Dependent variables included emotions (e.g., sadness and hope), evaluation of the expressive writing interventions (e.g., engagement, clarity, ease, and interest), and re-evaluation of disordered eating behaviors and cognitions. Results show that 62.90% of participants had observed disordered eating in their peers. Sadness, with an action tendency related to increased inward evaluation, was the most typical emotional response upon completion of the expressive writing tasks. Interventions that were based on the principles of cognitive behavioral therapy led to the most positive outcomes including engagement and re-evaluation of current disordered eating behaviors and cognitions. Overall, it was concluded that expressive writing interventions are effective in eliciting emotions and causing a re-evaluation of harmful behaviors and cognitions in the context of disordered eating.
An experiment testing 8 expressive writing interventions for disordered eating shows that sadness was the most typical emotional response after completing the tasks.
Disordered eating (DE) is a mental and physical health concern that includes both behaviors (e.g., skipping meals, self-induced vomiting, and chronic dieting) and cognitions (e.g., guilt after eating, shame, and intrusive thoughts). 1 DE is not a medical diagnosis; rather, it is a term encompassing symptoms experienced by an individual. The most significant difference between DE and eating disorders (EDs) is whether symptoms meet the criteria defined by the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-V). 2 It is common for individuals to experience DE, but fail to meet the diagnostic criteria of an ED. Nevertheless, DE can lead to serious health outcomes including growth retardation, poor bone health, fluctuations in weight, nutritional deficiencies, and psychosocial disturbances. 3 DE can also progress into a clinically diagnosed ED over time. 4 Treatment for EDs is complex and is typically effective for only 40-50% of patients. 5 This is concerning because there is some evidence to suggest that incidence is increasing for some types of EDs and all-cause mortality rates are elevated among individuals with EDs, particularly among those with anorexia nervosa.6,7 Thus, interventions focused on DE and ED prevention should be developed for individuals who are most at risk.8,9 EDs may be prevented with primary interventions targeted to high-risk populations, including college-age women.9,10 This study will test 8 expressive writing interventions, drawn from existing theory-based prevention programs, in a college-age population.
Young-adult women are particularly at risk for DE. Compared to the general population, DE is more prevalent in college-age women. 11 As many as 60% are at high-risk for the onset of EDs, highlighting an opportunity for college-based prevention programs. 12 Compared to their male counterparts, female college students have higher rates of DE.13,14 The emergence of the COVID-19 pandemic has exacerbated female college students’ risk for DE behaviors and cognitions. The pandemic has caused stress, anxiety, decreased social support, food insecurity, panic buying, and trauma which can cause or intensify DE. Now, more than ever, tailored prevention programs that can be disseminated safely during an evolving public health crisis are needed.15,16 By targeting modifiable risk factors for DE such as the cultural thin-ideal, body dissatisfaction, restrictive dieting, and negative affect, DE could be decreased or even prevented. Consequently, clinically diagnosed EDs may not develop. 17 Preventing DE through early intervention is essential.
Interventions to Reduce Disordered Eating
A review of DE and ED prevention programs, published in the peer-reviewed literature, yielded evidence-based programs that fell into 3 categories: Cognitive behavioral therapy, peer and media risk reduction, and cognitive dissonance. First, there is evidence that cognitive behavioral therapy is successful in reducing body image concerns and symptoms of EDs. 18 Cognitive behavioral principles are typical in the treatment of mental illness, and there is evidence that presenting EDs and DE in the context of mental illness may reduce sigma. For example, messages that presented the eating disorder bulimia nervosa as a distressing mental illness, that is physically and mentally damaging, were found to reduce stigmatizing attitudes, compared to messages that omitted the mental illness context. 19 The My Body, My Life intervention addressed body image, eating issues, motivations for change, unhealthy eating patterns, normalizing eating patterns, strategies for change, and negative self-talk. In one writing intervention, participants were asked to make a list of their food rules and reflect upon how the rules create problems in their lives. In a similar study, Gollings and Paxton 20 applied cognitive behavioral therapy principles, focusing on the causes of body dissatisfaction and DE, readiness to change, eating experiences, self-esteem, social pressures to be thin, and problem-solving. Participants completed writing exercises reflecting upon how their lives would be different if body image and eating concerns were no longer a problem. Significant improvements in all cognitive and behavioral outcome variables of interest were reported.
Second, there is a category of risk reduction interventions focused on addressing negative peer and media influence. The media perpetuates a thin-ideal and women may internalize this message and subsequently compare their own bodies to the content presented in the media. To reduce this negative influence, the Happy Being Me intervention included media literacy training, exploration of fat-talk, body comparison, and reduction of the thin-ideal. 21 Participants were asked to write about the pressure to conform to appearance ideals. Compared to the control group, the intervention group (that completed the writing intervention) reported significantly more positive outcomes on body dissatisfaction, body image, dietary restraint, and self-esteem at post-test and follow-up. 21
Finally, cognitive dissonance based prevention aims to create discomfort or confusion when attitudes and behaviors are inconsistent.22,23 Cognitive dissonance theory posits that people are driven by the need for consistency between their attitudes and behaviors because inconsistency generates psychological discomfort. It is this cognitive discomfort that motivates attitudinal or behavioral change, aimed at resolving the unpleasant feelings inconsistency generates. 22 The Body Project was a dissonance-based prevention program for college women. 8 In this intervention, participants were asked to write about what they would rather do than spend time and energy obsessing over body image concerns or engaging in DE. Thin-ideal internalization, body dissatisfaction, dieting, negative affect, and ED symptoms were measured. Compared to a control group, participants in the dissonance condition showed significantly greater decreases in thin-idealization, body dissatisfaction, dieting, and negative affect at post-test and 1-year follow-up. 8 A cognitive dissonance intervention was also used in a randomized control trial with sorority women in 3 groups: Cognitive dissonance, media, or control. 24 Participants completed an expressive writing intervention, listing the costs of engaging in the thin-ideal. Conversely, the media group watched a video on the influence of advertising on body image and the thin-ideal. Both intervention groups experienced reduced dietary restraint, body dissatisfaction, and ED pathology. However, only the dissonance group, who participated in self-reflection writing exercises, reported reduced thin idealization. 24
In the aforementioned studies, expressive writing interventions influenced attitudes and behaviors about DE. However, this previous work is limited in that study designs make it impossible to isolate the unique effect of each expressive writing intervention, and subsequently, make it impossible to identify which theoretical mechanisms are at work. Writing interventions were used alongside other in-person interventions. Understanding which theory-based expressive writing intervention leads to an outcome is essential in the design of future interventions.
The immediate outcomes of expressive writing interventions are hypothesized to be emotional responses and cognitive re-evaluation. Smith and Ellsworth’s 25 formative study of cognitive appraisals of emotion determined that appraisals of attention, pleasantness, certainty, anticipated effort or obstacles, and attributions of agency can reliably discriminate between different emotions. Discrete emotion theorists link the function of specific emotions to action tendencies.26,27 Negative emotions are typically more powerful than positive ones at inducing behavioral responses. 27 Anger and sadness are two notable examples of this. Anger is a reaction to a demeaning offense against “me or mine,” the individual or close others. 28 This emotion is motivating at moderate intensity and can lead to problem-solving behaviors intended to circumvent obstacles.28,29 Sadness is the reaction when an irrevocable loss is endured. This emotion increases inward evaluation, which can lead to problem-solving behaviors intended to recover the loss. 30 There is little research that examines the discrete emotional responses related to cognitive dissonance. 31 However, it is established that cognitive dissonance aims to create psychological discomfort. Cognitive discomfort and potentially negative emotions are necessary to modify thoughts, beliefs, and behaviors.22,32
For the primary prevention of DE, web-based interventions offer advantages compared to the in-person interventions reviewed in the previous section. Web-based interventions can provide anonymity to women who may be reluctant to seek help for DE due to shame or embarrassment.33,34 Anonymity can make it easier for women to disclose personal information and allow them to feel safe exploring their emotions surrounding this sensitive topic. 35 We know that some college students do not seek formal mental health services; thus, a web-based intervention offers assistance to those who may not utilize in-person options. 36 In addition, during the COVID-19 pandemic, web-based formats allow interventions to be safely carried out and remain insulated from disruptions, as public health measures change over time. DE is an excellent fit for a web-based intervention because the health problem is widespread and is often accompanied by shame, which may prevent or delay treatment-seeking behaviors. 37 Due to the presence of this health problem in college-age women and the infrastructure that is already in place on a college campus, a web-based intervention allows for a wide reach and is an appropriate channel for primary prevention at the population level. However, these in-person interventions must first be tested in a web-based format.
Current Study
The purpose of the current research study is to (1) investigate the self-reported and observed DE and ED risk in a sample of college-age women and (2) isolate, test, and compare web-based versions of expressive writing interventions extracted from existing DE prevention programs. Outcomes of interest include clarity, ease of completion, perceived interest, and discrete emotional responses. The following research questions guide this study.
Research Questions
Research Question 1: What is the self-reported and observed DE and ED risk in a sample of college-age women?
Research Question 2: What emotional responses do expressive writing interventions elicit?
Research Question 3: Is there a difference in ease of completion, perceived interest, or completion time between expressive writing interventions?
Method
Participants
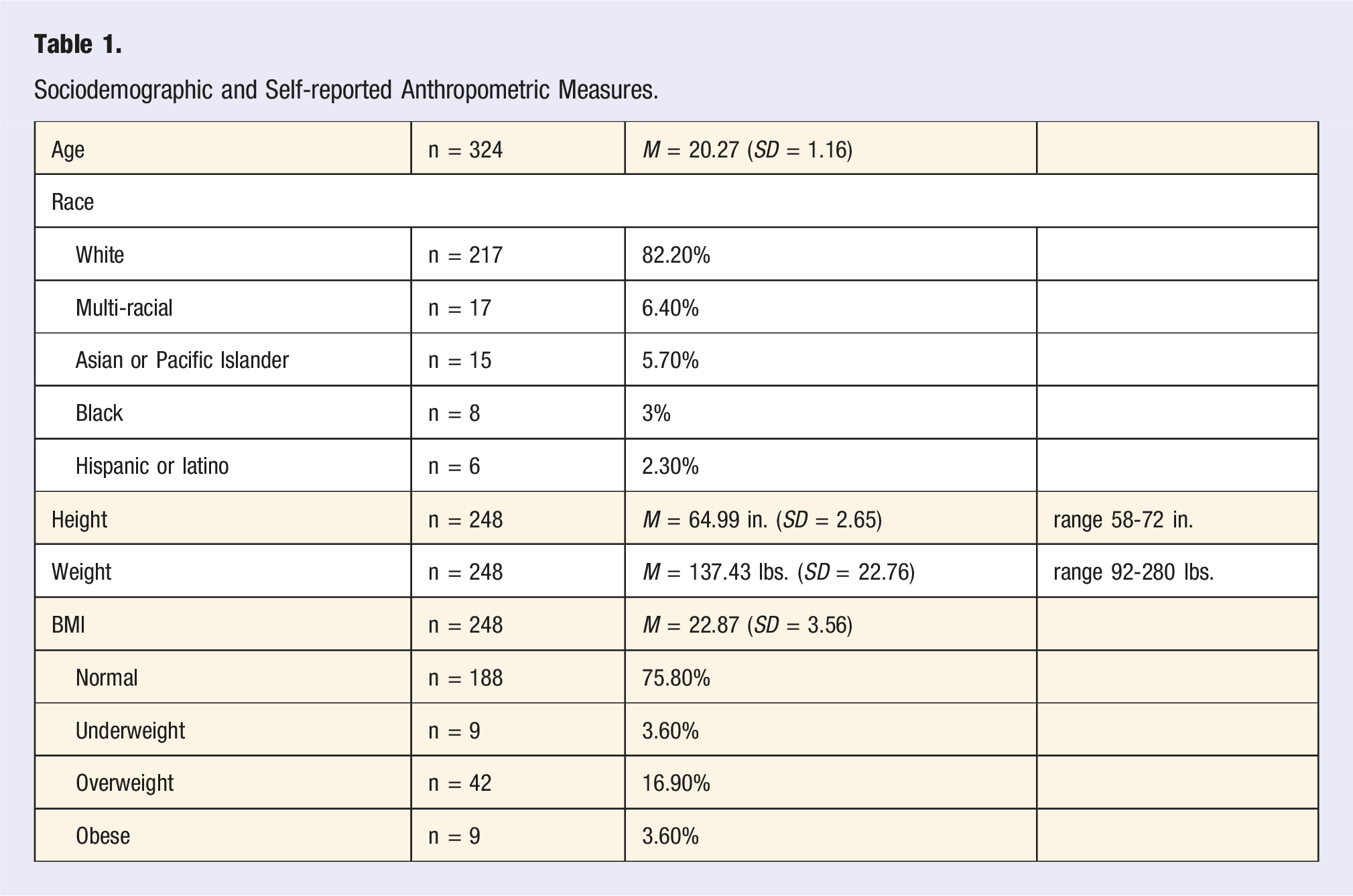
A web-based experiment was conducted with a sample of 326 women (M age = 20.27, SD = 1.16). Participants were 18-25 years old and enrolled at a mid-Atlantic university. Most participants majored in psychology (n = 43), health behavior science (n = 33), or neuroscience (n = 18). Participants were predominantly White (82.20%, n = 217), followed by multi-racial (6.40%, n = 17), Asian or Pacific Islander (5.70%, n = 15), Black (3.00%, n = 8), and Hispanic or Latino (2.30%, n = 6). Height and weight were self-reported and used to calculate body mass index (BMI, weight in pounds divided by height in inches squared multiplied by 703). 38 Most (75.80%, n = 188) had a BMI classified as normal (18.50-24.99 kg/m2), 3.60% (n = 9) had a BMI classified as underweight (less than 18.50 kg/m2), 16.90% (n = 42) as overweight (25-29.99 kg/m2), and 3.60% (n = 9) as obese (30 kg/m2 or higher). The mean BMI was in the normal classification range, 22.87 (SD = 3.56).
Procedure
Participants were recruited using a variety of methods. Instructors in multiple campus departments were asked to forward the web-based study link to their students. A snowball sampling method was then utilized, with participants being asked to forward the study link to other female students at the same institution. Participants were randomly assigned to an experimental or control condition. The experiment consisted of a pre-test questionnaire, 9 study conditions, and a post-test questionnaire. The study conditions were writing interventions that were completed individually and submitted as part of the experiment. Participants could take as much time as they wanted to complete the writing intervention. As an incentive, participants could choose to be entered into a drawing for 1 of ten $50 Amazon gift cards. Approval was obtained from the university’s Institutional Review Board (approval number: 1396364-1). All participants provided informed consent.
Materials
Experimental Conditions: Expressive Writing Interventions
The main independent variable of interest was the expressive writing intervention. Each participant completed the intervention privately, and the data was submitted to the researchers only and was not shared with the other participants. Acquisition of expressive writing interventions began with an extensive literature search. A team of researchers examined the literature for communication-based programs and interventions that aimed to prevent DE behaviors and cognitions. Keywords used in this search were “disordered eating intervention,” “eating disorder intervention,” “disordered eating program,” and “eating disorder prevention program.” The literature search resulted in 31 programs for review. Researchers then systematically examined the interventions for developer, program leader type (peer or professional), materials used, and determined if the intervention could be implemented at a university in a web-based, mediated format, with a female college-age population. Programs were included if the focus was on the reduction of DE. Interventions pertaining to clinically diagnosed psychological disorders were excluded. The authors of each program were contacted to obtain specific program materials (e.g., brochures, PowerPoints, lectures, and exercises). The systematic examination resulted in 8 expressive writing interventions from 4 programs.9,20,21,39 Minor modifications were made to the interventions to control for length and expected completion time. The final 8 expressive writing interventions represented 3 categories: Cognitive behavioral therapy, peer and media risk reduction, and cognitive dissonance. A control condition was included as a comparison group. All interventions were similar in length and applicable to the college-age female population (see the Appendix for the full content of each intervention).
Observed Disordered Eating Behaviors and Cognitions
To assess observed DE behaviors and cognitions in this sample, participants were asked: “What kind of eating behaviors do you observe your peers engaging in? Choose all that apply: Frequent dieting, skipping meals regularly, feelings of guilt related to food consumption, binge eating, self-induced vomiting, misusing laxatives or diuretics, fasting, chronic restrained dieting, something else, or my peers do not engage in any of these behaviors.” Participants were also asked if they observe their peers doing anything to control their weight (yes, plus please describe, or no).
Self-Reported Disordered Eating Behaviors and Cognitions
Participants were asked, “What kind of eating behaviors do you engage in? Choose all that apply: Frequent dieting, skipping meals regularly, feelings of guilt related to food consumption, binge eating, self-induced vomiting, misusing laxatives or diuretics, fasting, chronic restrained dieting, something else, or I do not engage in any of these behaviors.” Participants were also asked how often they talk about body image with their peers using a 4-point scale (often to never).
Eating Disorder Risk Assessment
ED risk was measured using the SCOFF questionnaire. This 5-question screening tool is based on the acronym SCOFF (i.e., Sick, Control, One, Fat, Food). Answering yes in response to 2 or more questions indicates a possible ED with 100% sensitivity and 87.50% specificity. 40
Evaluation of the Expressive Writing Interventions
After completing the expressive writing intervention, participants were asked to rate the ease of completing the task on a 7-point scale (1 = extremely easy, 7 = extremely difficult). They were also asked to rate how interesting the writing task was on a 5-point scale (1 = not interesting at all, 5 = extremely interesting). Completion time in minutes was also collected as a measure of engagement.
Emotional Response
Discrete emotions were measured after the completion of the expressive writing task. Participants were asked: “How did you feel while completing this intervention? Choose all that apply to you: Happiness, anger, worry, surprise, confusion, disgust, guilt, shame, sadness.”
Results
Sociodemographic and Self-reported Anthropometric Measures.
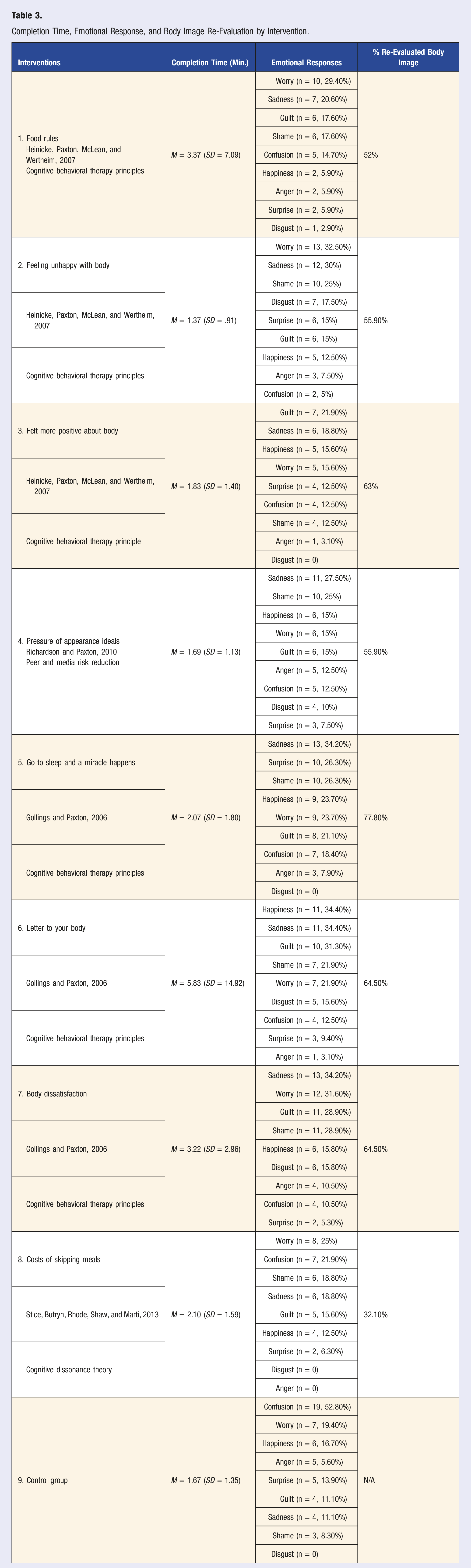
Research Question 2 examined the outcomes of the expressive writing interventions. The full text of each writing prompt is included in the Appendix. Six interventions were based on the principles of cognitive behavioral therapy. For intervention 1 (food rules), 20% wrote that they do not have any food rules for themselves. Among the participants with food rules, feelings of worry (29.40%) and sadness (20.60%) were reported most often. In this condition, 52% said that the writing task made them re-evaluate their own eating and body image. Intervention 2 (feeling unhappy with your body) participants reported feeling worry (32.50%) and sadness (30%) most often. In this condition, 55.90% said completing the writing task led them to re-evaluate their own eating and body image. In intervention 3 (felt more positive about your body), participants reported feeling guilt (21.90%) and sadness (18.80%) most often. In this condition, 63% said that writing made them re-evaluate their own eating and body image. In intervention 5 (go to sleep and a miracle happens), participants reported feeling sadness (34.20%), shame (26.30%), and surprise (26.20%) most often. In this condition, 77.80% said writing made them re-evaluate their own body image and eating. Intervention 6 (letter to your body) participants reported feeling happiness (34.40%) and sadness (34.40%) after completion. In this group, 64.50% said the task made them re-evaluate their own eating and body image. Finally, in intervention 7 (body dissatisfaction), participants felt sadness (34.20%) and worry (31.60%) most often. In this group, 64.50% reported that completing the task made them re-evaluate their own body image and eating. In summary, sadness was an expressed emotional outcome of all 6 cognitive behavioral therapy expressive writing tasks, with 18.80-34.40% of participants reporting this emotional response after writing.
One intervention was focused on peer and media risk reduction (intervention 4, pressure of appearance ideals). Participants reported feeling sadness (27.50%) and shame (25%) most often after completion. In this condition, 55.90% said that writing made them re-evaluate their own eating and body image. And finally, one intervention was cognitive dissonance based (8, costs of skipping meals). The task brought about feelings of worry (25%) and confusion (21.90%) most often. In this experimental group, 32.10% said the writing task made them re-evaluate their own body image and eating.
Examining the data across conditions, the expressive writing interventions were compared on their ability to cause re-evaluation of the participants’ current body image and eating. Intervention 5 led the highest number of participants to cognitively re-evaluate (77.80%). This was followed by 6 and 7 (64.50%), 3 (63%), 2 and 4 (55.90%), 1 (52.00%), and finally 8 (32.10%). In summary, interventions 5 (go to sleep and a miracle happens), 6 (letter to your body), and 7 (body dissatisfaction) had the greatest influence on cognitive re-evaluation.
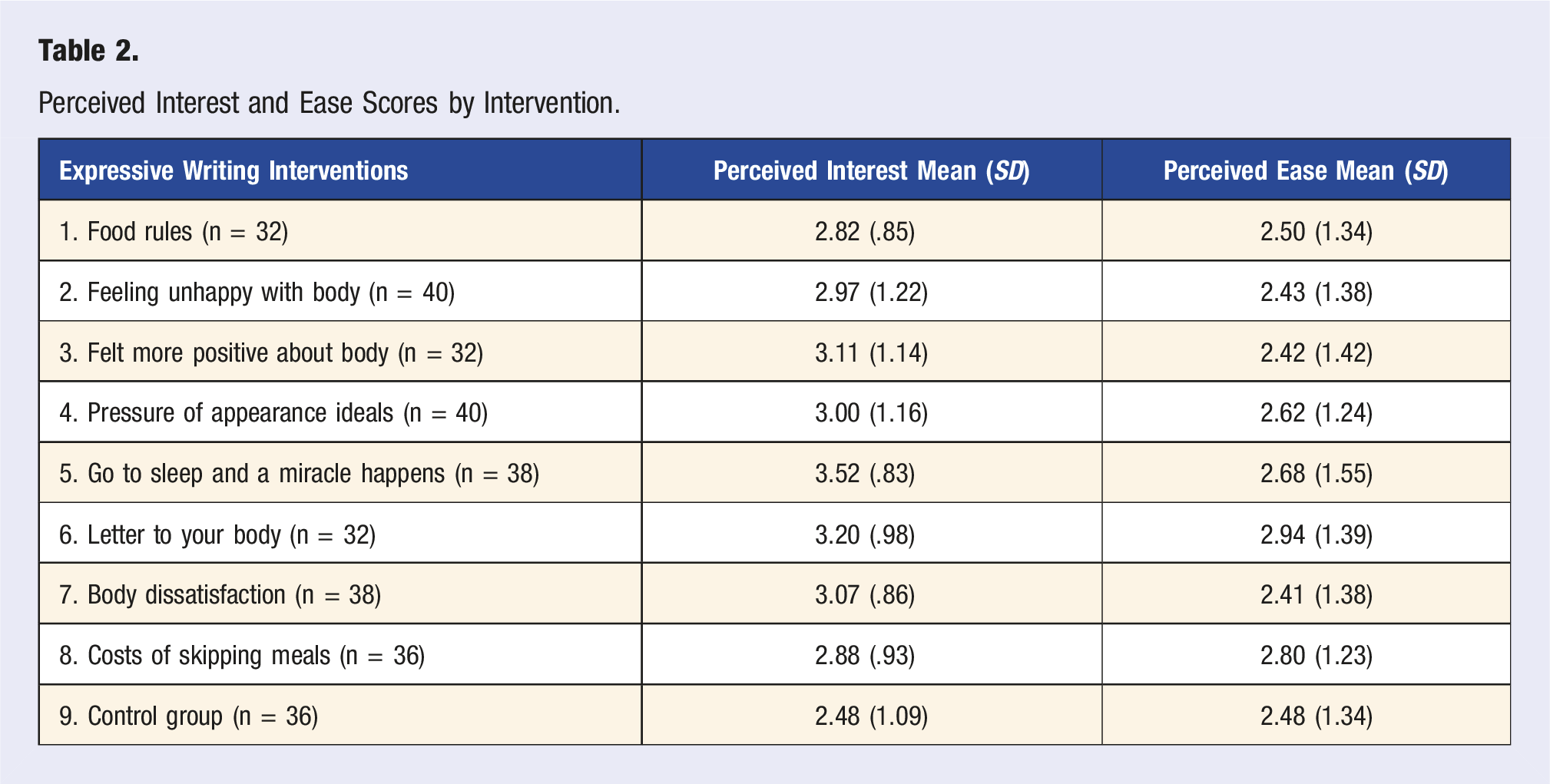
Perceived Interest and Ease Scores by Intervention.
Completion Time, Emotional Response, and Body Image Re-Evaluation by Intervention.
Discussion
This study was designed to (1) measure the observed and self-reported DE and ED risk in a sample of college-age women and (2) test and compare expressive writing interventions. Other outcomes of interest for the expressive writing tasks included engagement, ease of completion, and interest. As the existing literature predicted, DE was present in this population. The majority (62.90%) of women in the study had observed their peers engaging in DE including fad diets, food restriction, or other methods of weight control. Furthermore, 33.50% of women in this sample were personally at risk for an ED, according to the predictive SCOFF risk assessment measure. This is higher than the 21.10% who fit at-risk criteria in the 2020 College Risk Behavior Survey, with data collected from a random sample of both men and women enrolled at the university (University of Delaware Center for Drug and Health Studies, unpublished data, March 2020). Overall, it can be concluded that this population is an appropriate target for a future DE prevention program.
Turning to the heart of this project, the outcomes of the expressive writing tasks, sadness was the most common emotional response. As a discrete emotion, sadness is a reaction when an irrevocable loss has been sustained. Despite the negative cognitions associated with sadness, this outcome can be viewed as a positive one in terms of intervention success. Felt sadness has been shown to increase inward evaluation, which can lead to problem-solving behaviors intended to recover the loss. 30 This action tendency is exactly the outcome that may be necessary for cognitive or behavioral change. The emotional responses that were identified in this work should be examined in future research. Notably, sadness was not a key outcome for the cognitive dissonance based intervention. As previously noted, there is little research on the emotional responses related to cognitive dissonance. 31 While not a discrete emotion, dissonance (intervention 8) did lead to confusion as a reported outcome. This may provide some evidence of felt cognitive dissonance and should be explored in future research on cognitive dissonance messaging in health interventions. This study did not measure the intensity of the reported emotions. At high levels of intensity, emotions can become dysfunctional. Future research should examine the role of intensity on cognitive processing and attitude change in this context.
Based on responses and measured outcomes for all writing interventions, condition 5 (go to sleep and a miracle happens), condition 6 (letter to your body), and condition 7 (body dissatisfaction) were not only perceived as the most interesting but were also most likely to cause participants to re-evaluate of their current body image and DE. Surprisingly, the cognitive dissonance writing task, which theoretically should lead to cognitive re-evaluation to reduce inconsistency, scored lower on this measure (32.10% compared to 77.80% for condition 5, 64.50% for condition 6, and 64.50% for condition 7). Overall, 3 expressive writing tasks, based on the principles of cognitive behavioral therapy, were most effective on all outcomes of interest.
Finally, the limitations of this study should be mentioned. One long-term goal of this study is the development of a web-based intervention in a college campus setting, which is especially important during the current COVID-19 pandemic. The study sample was drawn from the population of interest; however, it is important to note that study participants were predominantly White (82.20%) and all participants were women. Results may be different for other demographic groups and other university populations, and those groups should be studied in future work. It is also worth noting that DE and EDs are not limited to women. Subclinical DE is also present among men. 41 On this campus, the majority of students are female and White. Yet, EDs and DE are not unique to White women and other populations need attention in future work. Conducting message testing research at historically non-white colleges or in areas of the country that are more diverse will be a necessary next step in order to develop unique interventions or to determine whether similar messaging works for individuals who are non-white. Additionally, DE among college students is correlated with a history of trauma. The COVID-19 pandemic has undeniably increased a personal and societal sense of trauma. Interventions aimed at reducing DE should consider a trauma-based perspective in their design.42,43 A final limitation was the use of self-report measures for behaviors and cognitions. This introduces subjectivity in the reporting of personal and observed DE.
Results from this study can be used to develop a DE prevention program for college-age women or to design stand-alone expressive writing interventions in the future. Overall, it was learned that writing interventions caused participants to re-evaluate their body image, DE behaviors, and DE cognitions. Expressive writing interventions are easy to administer in a web-based primary prevention program and this format offers anonymity. Given the secretive nature of DE behaviors and the shame that often accompanies them, this format has many benefits. A web-based primary prevention program could be used as a mechanism to identify those with risk factors for clinical EDs. Once identified, higher risk women could then be offered a secondary prevention program or if warranted, treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for participant incentives was provided by the Department of Behavioral Health and Nutrition at the University of Delaware.