
Abstract
There is growing interest in the role of sedentary behavior as a risk factor for poor health, independent of physical activity (PA). To guide the spectrum of descriptive, analytic, and intervention studies on sedentary behavior, the authors advocate a behavioral epidemiology framework. This 5-phase framework is useful because it outlines a series of sequential stages important for developing, evaluating, and diffusing interventions to reduce sedentary behavior and improve population health. Studies of sedentary behavior and health outcomes (phase I) have found consistent evidence that excessive use of screen-based media is linked to overweight and obesity in children, and there is some evidence among adults that overall sedentary time is associated with risk factors for cardiometabolic disease, some cancers, and mortality. Biological mechanisms to explain possible relationships have started to emerge but are mostly based on animal models. Obtaining valid and reliable measurements of sedentary behavior (phase II) remains a research priority because self-reports are prone to recall bias, and it appears that sedentary habits do not appear to be well represented by measures of individual behaviors such as TV viewing. Studies have identified few modifiable correlates of sedentary behavior (phase III), although research appears to be limited to studies of TV viewing or to scenarios in which sedentary behavior is defined as an absence of PA. Rigorous intervention research (phase IV) has focused almost exclusively on reducing self-reported TV viewing among children and adolescents, and there is consistent evidence that these interventions are efficacious. There appear to be no interventions focused exclusively on reducing sedentary behavior of adults. Translation studies (phase V) are absent because the underlying evidence is still emerging. Future research should focus on examining causal associations between sedentary behavior and health, developing objective measures of domain-specific sitting time, and identifying modifiable correlates of sedentary behavior that can be used as leverage points for behavioral interventions.
Keywords
For example, animal models of sedentary behavior have demonstrated that prolonged inactivity quickly engages biological signals that suppress levels of lipoprotein lipase (LPL), an enzyme essential for lipid metabolism.
Introduction
Randomized controlled trials and prospective epidemiological data provide strong and consistent evidence that moderate-to-vigorous physical activity (MVPA) reduces the risk of cardiovascular disease, type 2 diabetes, the metabolic syndrome, and some cancers.1,2 The magnitude of the health benefits of physical activity (PA) is inversely associated with baseline activity levels, with the greatest benefits occurring for inactive individuals who become moderately active (see Figure 1). 1
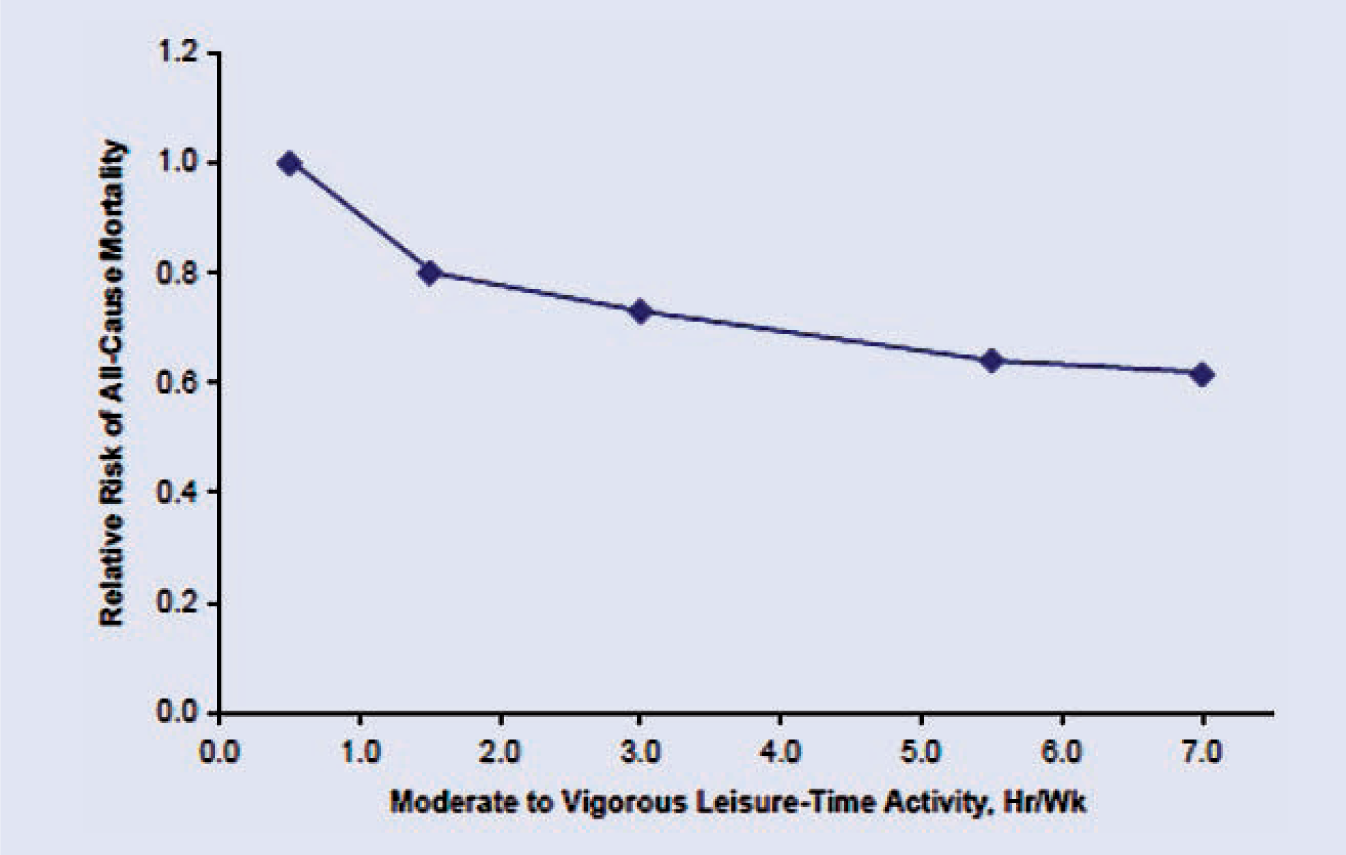
Median Shape of the Dose–Response Curve: Relative Risks of All-Cause Mortality by Physical Activity Level.a
Based on the combined evidence, the national public health guideline for children and adolescents is to accumulate 60 minutes or more of PA daily, with most activity at a moderate or vigorous intensity. For adults, the recommendation is to accumulate at least 150 minutes per week of moderate-intensity PA or 75 minutes per week of vigorous intensity PA. 3 Until recently, the health risks associated with a sedentary lifestyle were thought to be a result of insufficient MVPA, leading many to inaccurately assume that sedentary behavior and MVPA were opposite ends of the same continuum. 2 This assumption was first challenged by Owen and colleagues 4 who reported that the determinants of sedentary behavior and PA might be distinct. In the past 10 years, more than 300 studies have been published that have measured sedentary behavior as a concept distinct from PA, and there is now widespread conceptual and empirical support that the two appear to exert independent and interdependent influences on health.5-8
Building on this evidence, Hamilton and colleagues 9 proposed 4 tenets of a new research paradigm they refer to as “inactivity physiology.” Inactivity physiology posits that prolonged sitting influences disease risk via pathogenic processes that are sometimes different from the molecular and physiological responses associated with PA and exercise. These are discussed in more detail later. The 4 tenets of inactivity physiology state that (1) sitting and limiting nonexercise activity may independently increase disease risk; (2) sedentary behavior is a distinct class of behavior with specific determinants and effects on disease risk, separate from the behavior of leisure time exercise; (3) the molecular and physiological responses in the human body of too much sitting are not always the same as the responses that follow a bout of additional physical exercise; and (4) people already insufficiently physically active will increase their risk even further by prolonged sitting time. 9
The purpose of this review article is to present (1) a systematic research framework to guide the spectrum of descriptive, analytic, and intervention studies related to sedentary behavior; (2) a summary of the evidence from each phase of the systematic framework applied to sedentary behavior; and (3) implications and recommendations for future research.
Defining Sedentary Behavior
Although the scientific study of sedentary behavior is gaining momentum, there remain conceptual and definitional ambiguity about what it actually is. For example, national surveillance systems and expert organizations sometimes classify individuals as inactive or sedentary if they do not meet public health recommendations for MVPA. 10 The American College of Sports Medicine (2006) defines a sedentary lifestyle as “not participating in a regular exercise program or not meeting the minimal PA recommendations from the US Surgeon General” (p. 22). 11 Concluding that individuals are physically inactive is erroneous if data only support a conclusion that individuals are not active enough. Although physical inactivity is an increasingly common term, a more appropriate label is sedentary behavior because it avoids the tendency to treat MVPA and inactivity as antonymic and permits a unique class of behavioral topographies (what the behavior looks like) to be defined. Along with others, 8 we have argued 12 that sedentary behavior is best defined as a distinct class of behaviors that involve sitting and low levels of energy expenditure, typically less than 1.5 metabolic equivalents (METs). Because it is impractical to measure energy expenditure in most studies and there are so few behaviors that involve both sitting and energy expenditure >1.5 METs, sedentary behavior is best operationalized as sitting. Of note is that the word sedentary derives from the Latin verb sedere, meaning to sit. It is also important to focus on sitting because PA and sedentary behavior interventions rarely attempt to change the time spent lying down (usually sleeping and napping), and there are important health-related metabolic processes that occur when individuals change posture from sitting to standing. 13 Even light-intensity activity is thought to convey health benefits.14,15 It is important to note that the most commonly studied sedentary behavior, TV viewing, should not be used as a measure of overall sedentary behavior because the two are largely uncorrelated in samples of children 16 and adults. 17 The limitations of measuring TV viewing are discussed later in the article.
A Research Framework for Studying and Understanding Sedentary Behavior
Because the scientific study of sedentary behavior is relatively new, it is useful to identify a research framework to help conceptualize how this growing knowledge base can be used for health promotion and disease prevention. Research frameworks are particularly useful in public health because they help outline a systematic approach to developing, evaluating, and diffusing behavior change interventions designed to improve population health. Sallis et al 18 advocated the use of a behavioral epidemiology framework to help guide the sequence and spectrum of descriptive, analytic, and intervention studies related to population health. Behavioral epidemiology is the scientific study of the etiology and distribution of behaviors that affect health and disease. More important, behavioral epidemiology has the explicit purpose of understanding health behaviors so that they can be influenced as part of a population-wide effort to prevent disease and promote health. We recently modified this framework for use with sedentary behavior research. 12
The sedentary behavior epidemiology framework specifies 5 main research phases in a rationally ordered sequence. Figure 2 summarizes these research phases. Each phase of research is intended to build on previous phases, and for this reason, the framework provides a nice road map of how best to prioritize and sequence our research efforts as well as identify existing gaps in the knowledge base. For example, using the behavioral epidemiology framework, it is clear why the development of valid and reliable measures of sedentary behavior is an important research priority: accurate assessment tools (phase II) help us better understand the determinants or correlates of sedentary behavior (phase III), which in turn help us focus our intervention efforts on factors most likely to bring about behavior change (phase IV). There is also the possibility for reverse sequencing in the research phases. For example, as more valid and reliable measures of sedentary behavior are developed, we are better able to clarify relationships between sedentary behavior and health (phase I). We have structured the remainder of this review using the research phases specified in the behavioral epidemiology framework.
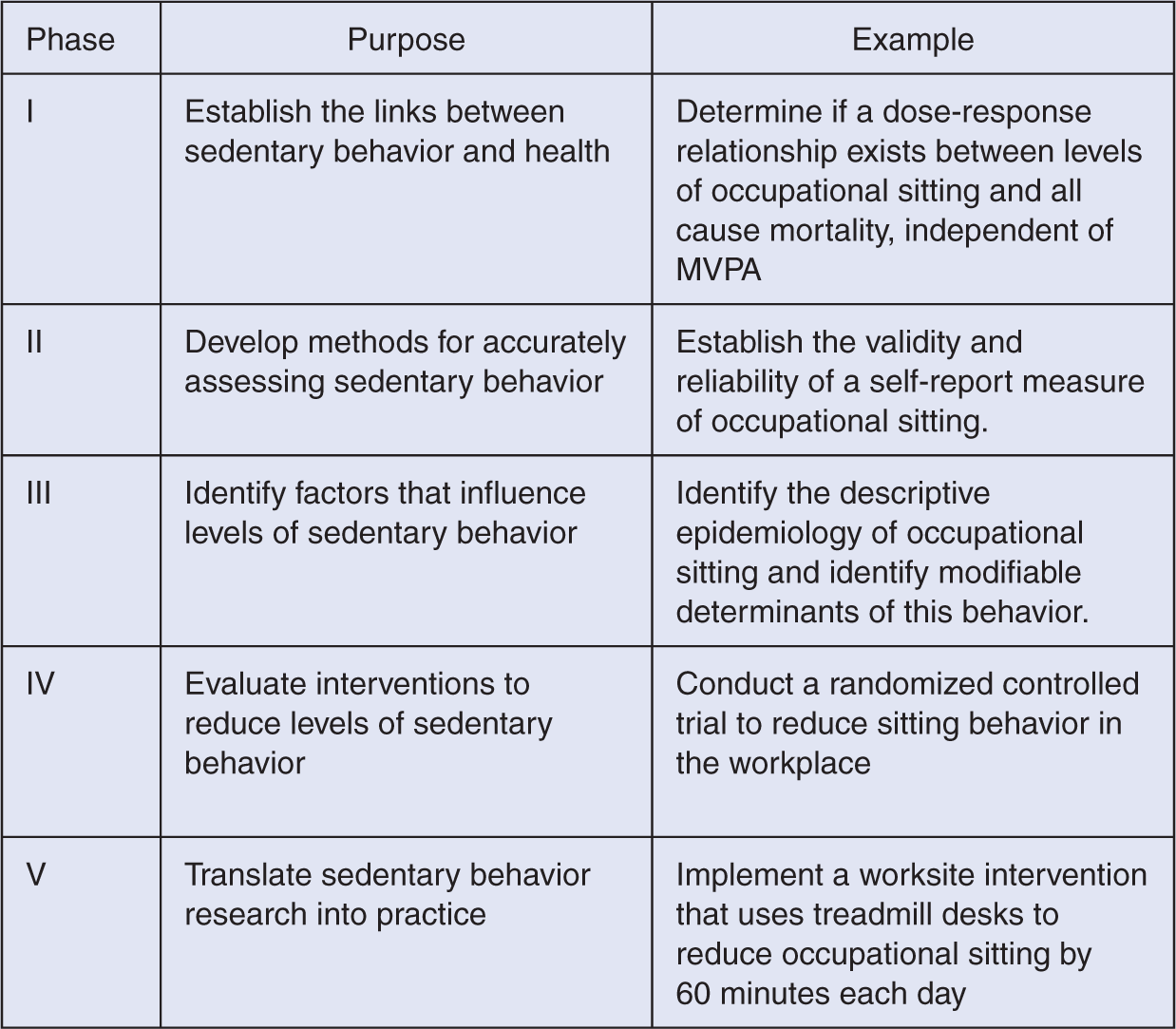
The Sedentary Behavior Epidemiology Research Framework.
Biological and Behavioral Evidence Linking Sedentary Behavior to Health (Phase I Research)
Although there has been recent research interest in the study of sedentary behavior, the evidence linking sitting to cardiovascular health dates back to the pioneering work of Dr Jerry Morris in the 1950s. 16 In a seminal epidemiological study, Morris and colleagues found that seated workers (London bus drivers and mail sorters) had higher rates of cardiovascular events than employees who stood and walked while working (ticket collectors and postal workers). However, it was not until the mid-1990s that researchers began to focus attention on outcomes associated with sedentary behavior that were independent of the time spent in PA.
The most commonly reported health outcome associated with sedentary behavior is obesity.17,19 The biological mechanism underlying this relationship is most likely related to energy balance since sedentary behavior is related to total daily energy expenditure, which, in turn, is related to weight gain. However, exact mechanisms are likely complex because although obese individuals appear to spend 2.5 hours more per day in a sitting position compared with lean individuals, this postural “habit” remains even after weight loss. 20 Similarly, when lean individuals were experimentally induced to gain weight, their sitting time did not change. 20 Regardless, the effect of measured sedentary time on obesity, independent of PA, has been reported in numerous studies across the age spectrum,17,19,21 although there is some evidence to the contrary.22,23 What is important is that meta-analytic evidence 24 of relationships between TV viewing and obesity among children and adolescents found that many studies either did not statistically correct for known confounders such as diet and PA or failed to report what covariates were included in the statistical models. Television viewing is the most commonly studied sedentary behavior in children and adolescents, and meta-analytic evidence suggests that it is related to body fatness. 24 Behavioral mechanisms underlying this relationship are also likely to be complex because energy intake has been shown to be related to TV viewing, 25 which, in turn, is related to between-meal snacking26,27 and food choices that are prompted by TV advertisements. 28 There are also deleterious psychosocial effects of excessive TV viewing on child health, which have been reviewed in more detail elsewhere. 29
Among adults, overall sedentary behavior has been associated with an increased risk of cardiovascular disease, 30 metabolic syndrome, 31 incident hypertension, 32 type 2 diabetes, 23 ovarian cancer,33,34 colon cancer, 35 and endometrial cancer. 36 New research has also indicated that sedentary behavior is associated with markers of cardiovascular disease risk in adolescents. 37 However, it should be noted that many studies of both adults and adolescents have also reported null findings.38-42 TV viewing in particular appears to be related to obesity.23,43-45 It is important to note that many of the associations between sedentary behavior and health are independent of the time spent in MVPA, suggesting that sedentary behavior carries a unique and independent risk to health that may not be reduced simply by becoming more physically active. 46 Large prospective studies of adults have also indicated that time spent sitting and viewing TV in particular is significantly associated with risk of all-cause mortality, cardiovascular disease mortality, and other cause mortality47,48 (see Figure 3). These findings are important because observed associations are independent of demographic factors (age, sex), negative health behaviors (smoking, alcohol consumption), and positive health behaviors (leisure time PA).
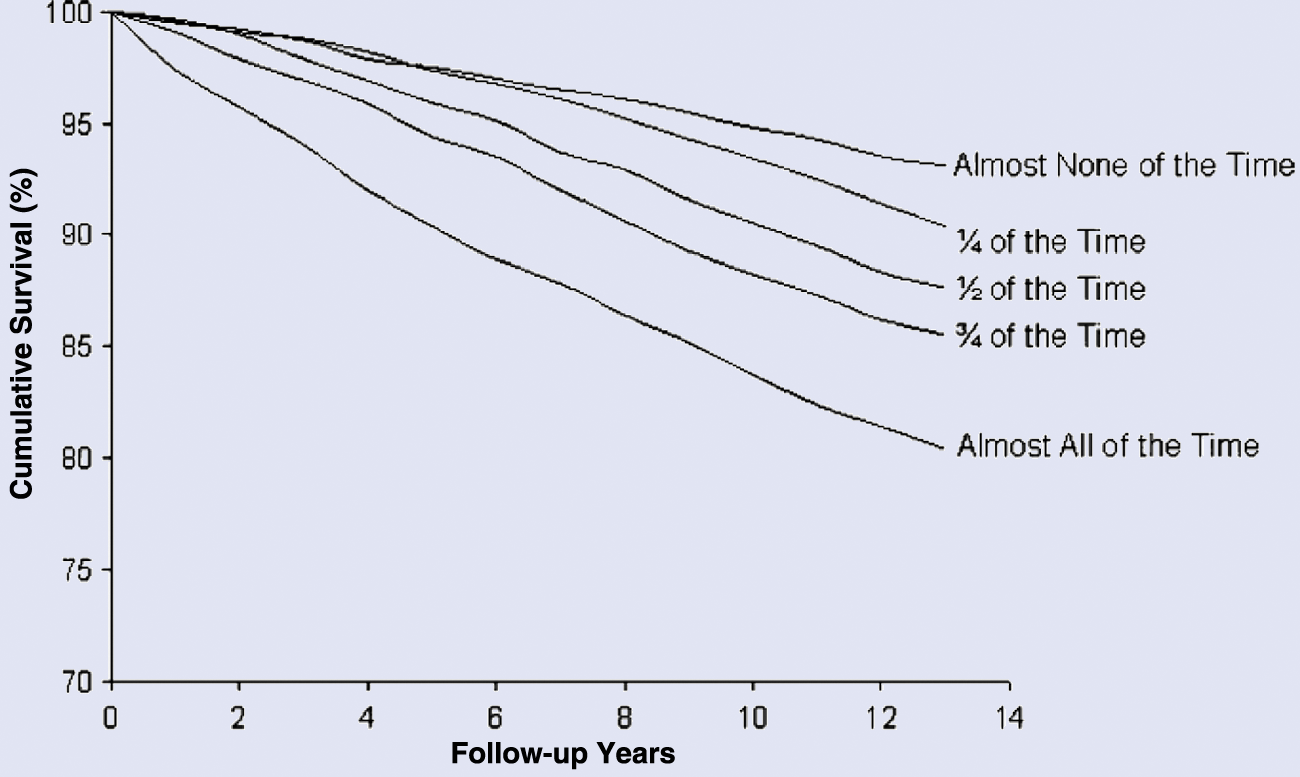
Kaplan–Meier Survival Curve for All-Cause Mortality Across Categories of Daily Sitting Time in 17 013 Men and Women 18 to 90 Years of Age, in the Canada Fitness Survey, 1981–1993.a
New laboratory and observational studies have begun to elucidate the potential biological mechanisms that underlie the relationship between sedentary behavior and cardiometabolic risk. For example, animal models of sedentary behavior have demonstrated that prolonged inactivity quickly engages biological signals that suppress levels of lipoprotein lipase (LPL), an enzyme essential for lipid metabolism. 13 When levels of LPL drop in the lining of blood vessels, rapid and clinically relevant decreases in HDL cholesterol have been observed, and the risk of metabolic and cardiovascular disease increases. 6 Of note is that the mechanism of LPL regulation appears to be different when sitting than standing or when exercising, and the magnitude of change in LPL when seated is much larger than the change in response to exercise. 49 Figure 4 summarizes the difference in cellular events thought to occur during periods of inactivity compared with exercise training. 9 The different mechanisms provide one with the rationale for why the physiology of sedentary behavior might sometimes be distinct from the physiology of PA and exercise. 13
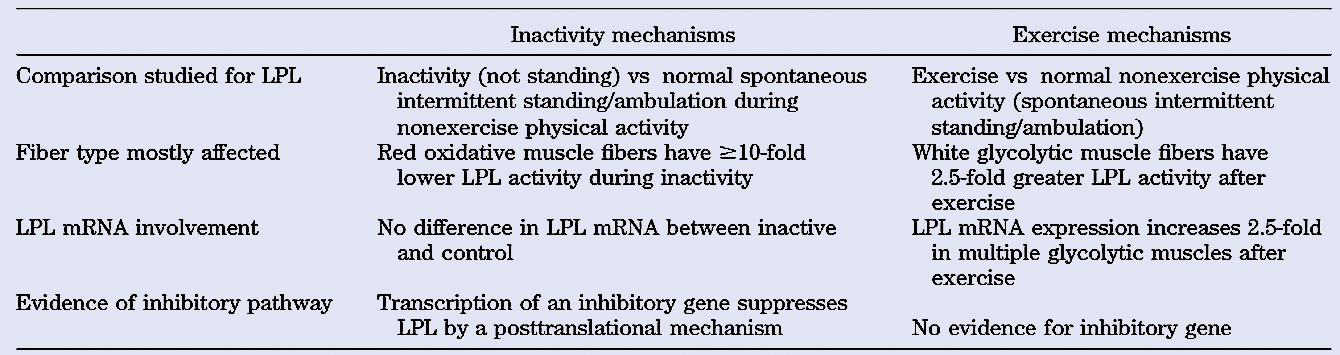
Lipoprotein Lipase Studies Indicate That the Underlying Cellular Events During Inactivity (Nonexercise Activity Thermogenesis Deficiency) Are Distinct From the Cellular Events After Exercise Training.a
New evidence has identified myokines (circulating cytokines associated with skeletal muscle contraction) as being related to overall- and location-specific adiposity. The authors suggest that physical inactivity reduces circulating hormone-like biological mechanisms and thereby disrupts normal metabolic functions such as lipid metabolism and insulin production. 50 These findings also support observational studies14,51 that show significant inverse associations between markers of metabolic risk and the frequency of short (4-5 minute) breaks in sitting time. Experimental studies show that insulin sensitivity of the whole body, skeletal muscle, and the vascular system is dramatically reduced after just 10 days of forced bed rest. 52 For individuals with a family history of type 2 diabetes, hepatic insulin resistance is augmented even further. 53 Combined, these studies suggest that intervention studies designed to get people out of a sedentary position could be of clinical importance, particularly for those already at risk for metabolic abnormality.
Much of the phase I research to date has focused on sedentary behavior in relation to cardiometabolic health, and other health outcomes have been studied only sporadically. For example, occupational sitting has been associated with musculoskeletal health, especially lower back pain 54 and low bone mineral density, 55 but these are rarely reported in the PA and health literatures. In addition, a positive association between sedentary behavior and depression has been reported, albeit in cross-sectional studies.56-59
What We Know
Evidence linking sedentary behavior to poor health is still emerging. The majority of findings relate to distal health outcomes such as obesity 60 and other risk factors for cardiometabolic disease. The majority of evidence also comes from cross-sectional studies based on self-reports of sedentary behavior. Experimental evidence comes predominantly from animal models of hind limb unloading and human studies involving forced bed rest. However, available evidence does support the conclusion that sedentary behavior carries a health risk that is both interdependent and independent of the level of MVPA.
What We Need to Know
More empirical research is needed across the proximal–distal continuum of risks associated with sedentary behavior. More experimental evidence on humans is needed to better understand biological pathways linking prolonged sitting to health, especially in populations who may be at greater risk (such as older adults) because of their prolonged sitting time. In addition, researchers are encouraged to intensify their research on cardiometabolic outcomes of sitting but also broaden their focus to assess a wider spectrum of deleterious consequences, including musculoskeletal ill health.
Methods for Accurately Assessing Sedentary Behavior (Phase II Research)
Assessments of sedentary behavior among children and adolescents focus almost exclusively on TV viewing because it is the most prevalent sedentary behavior reported by young people, 61 and there is a statistically significant relationship between TV viewing and body fatness. 24 However, recent evidence from a study of ~1500 British teenagers found that TV viewing is a poor marker of overall sedentary behavior. 62 Objective measures of TV watching have been reported in a few small studies,63-65 but this method is costly, time-consuming, and prone to behavioral reactivity. Time use diaries, questionnaires, and checklists are more commonly used, but few published data are available to support the validity and reliability of these reports, whether they are based on specific activities (eg, TV viewing) or groups of activities (eg, screen-based media). A recent review of 88 studies measuring TV viewing in children and adolescents 65 found that only 15% of studies used measures that had been psychometrically tested. Only 7% of studies presented validity and reliability data, and correlations between self-reports and direct observation ranged from r = 0.07 to 0.37. In addition, previous research66-69 demonstrates that parent and child estimates of TV viewing are often poorly correlated (typically r = 0.2-0.3), suggesting either that considerable error exists or that different constructs are being measured. Asking children younger than 14 years to recall the number of minutes or hours per day spent watching television may not yield reliable estimates of behavior. Evidence suggests that younger children (<14 years) think about their viewing time not in terms of minutes or hours but according to the programs watched and the time of day when viewing occurred as well as the time spent completing homework and participating in sports. 70 For children younger than 10 years, it is recommended that proxy reports from a parent or older sibling be used in place of the child’s self-report. However, further research is needed to establish reporting guidelines for using proxy reports.
Among adults, TV viewing is also the most commonly assessed sedentary behavior. In a systematic review of 60 studies measuring nonoccupational sedentary behavior in adults, Clark et al 71 found that 65% of studies measured only TV viewing, 12% measured leisure time sitting, with the remainder measuring other media use or multiple behaviors. Only a handful of studies presented psychometric properties of the instruments. Although the reliability of assessments was generally acceptable (test-retest r = 0.32 to 0.93), validity coefficients were highly variable (ranging from −0.19 to 0.80), and TV viewing time was generally underreported when compared with an objective assessment. Measures of domain-specific sitting (such as in the workplace or during travel) are needed, and PA surveillance instruments have now started to include items about sitting.72-74 However, it is unclear if these yield valid and reliable estimates of sedentary behavior. In one of the few studies to validate a surveillance-based measure of self-reported sitting, Rosenberg et al 75 reported correlations between total sitting time from the International Physical Activity Questionnaire (IPAQ) and minutes of ActiGraph accelerometer counts <100 (a commonly used cutoff point to define sedentary behavior) in a sample of 289 adults from 3 countries. Correlations were significant for both the long (r = .33) and short forms of the IPAQ (r = .34) even though the sensitivity and specificity of the 100-count-per-minute cutoff point as a measure of sedentary behavior remains largely unknown. Marshall et al 76 used detailed logs to validate single-item self-reports of sitting across 5 different domains among 253 Australian adults, aged 51 to 63 years. Reliability coefficients were high for week-day occupational sitting, watching television, and using a computer at home (r = 0.84-0.78) but lower for weekend days across all domains (r = 0.23-0.74).
What We Know
Measuring sedentary behavior as an absence of PA is inappropriate. Self-reports of TV viewing dominate the measurement literature in sedentary behavior although the validity of these measures remains questionable, and TV viewing does not appear to be a valid proxy for total sedentary time. Hip-mounted accelerometers appear to be the most common criterion method for validating self-reports of total sitting, but the sensitivity and specificity of the 100-count-per-minute point is unknown, and estimates of domain-specific sitting are not possible.
What We Need to Know
Validity and reliability data are needed for surveillance-based self-reports of total- and domain-specific sitting behaviors. We also need valid objective measures of sitting that are feasible for use with large samples. For accelerometer-based measures, cutoff points with acceptable sensitivity and specificity for detecting posture allocation (ie, lying vs sitting vs standing) should be validated, and clearer thresholds should be identified that can differentiate sedentary behavior from accelerometer nonwear time.
Factors That Influence Levels of Sedentary Behavior (Phase III Research)
Research in phase III of the behavioral epidemiology framework aims to establish determinants and correlates of sedentary behavior so that interventions can better target factors known to cause, or at least influence, sedentary behavior. In samples of children and adolescents, 3 systematic reviews have been published that summarize empirical correlates of youth sedentary behavior 77 and TV viewing in particular.27,78 Available data are often difficult to interpret, but consistent correlates of TV viewing appear to be nonwhite ethnicity (positive), parent income and education (negative), the number of parents in the home (negative), body mass (positive), parental viewing behavior (positive), between-meal snacking (positive), weekend day (positive), and having a television set in the bedroom (positive). Many studies have selected correlates based on a priori associations with PA, which may be inappropriate, given that PA and sedentary behavior should not be treated as behavioral analogs. 7 Although television viewing is the most prevalent sedentary behavior among youth, its value as a marker of overall sedentary time is questionable, 62 largely because empirical associations between TV viewing and PA are null or very small. 24 Within individual studies, the amount of sedentary behavior is rarely associated with age and sex of the child, which contrasts with the findings for PA. 79 However, a cross-study descriptive epidemiology of screen-based media use found that TV viewing tends to peak between 7 and 12 years for both boys and girls, and boys appeared to watch more TV at all ages. 61
In one of the only longitudinal studies of correlates of television viewing among children, Saelens and colleagues 80 reported that the number of meals eaten while watching television and having a television set in the bedroom were significantly associated with television viewing time at ages 6 and 12 years as well as with increases in television viewing time at these ages. These data are important because they suggest that having a television in the bedroom may serve to increase viewing behavior over and above increases that might be associated with age. Other correlates such as depression, dietary fat, and features of the physical environment have been reported, but the systematic review evidence suggests that the data are equivocal, partly because of small sample sizes, the reliance on cross-sectional study designs, lack of theory-driven hypotheses, and measurement error. Recent interest has focused on tripartite relationships between sedentary behavior, sleep, and obesity because cross-sectional and longitudinal evidence suggests a link between short sleep duration and weight, for which screen time may be an effect modifier. 81 This is an area worthy of further research because a consistent correlate of child TV viewing is the presence of a TV set in the child’s bedroom.
Relatively few studies on correlates of sedentary behavior among adults have been conducted. Of the studies that have focused on TV viewing, age (>60 years), being female, and low socioeconomic status emerge as consistent predictors among Australian and European adults.21,82,83 In 2008, Matthews and colleagues 84 published the first study to estimate the national prevalence of sedentary behavior in US adults based on objective measurements. Figure 5 presents the mean hours per day of sedentary time for US adults, by age and gender. From ages 6 to 29 years, girls and women appear to be more sedentary than boys and men of the same age, although this trend is reversed when adults reach 60 years of age. In a recent analysis of the American Time Use Survey, watching TV/movies was the second most prevalent (80.1%) daily activity reported by adults. 85
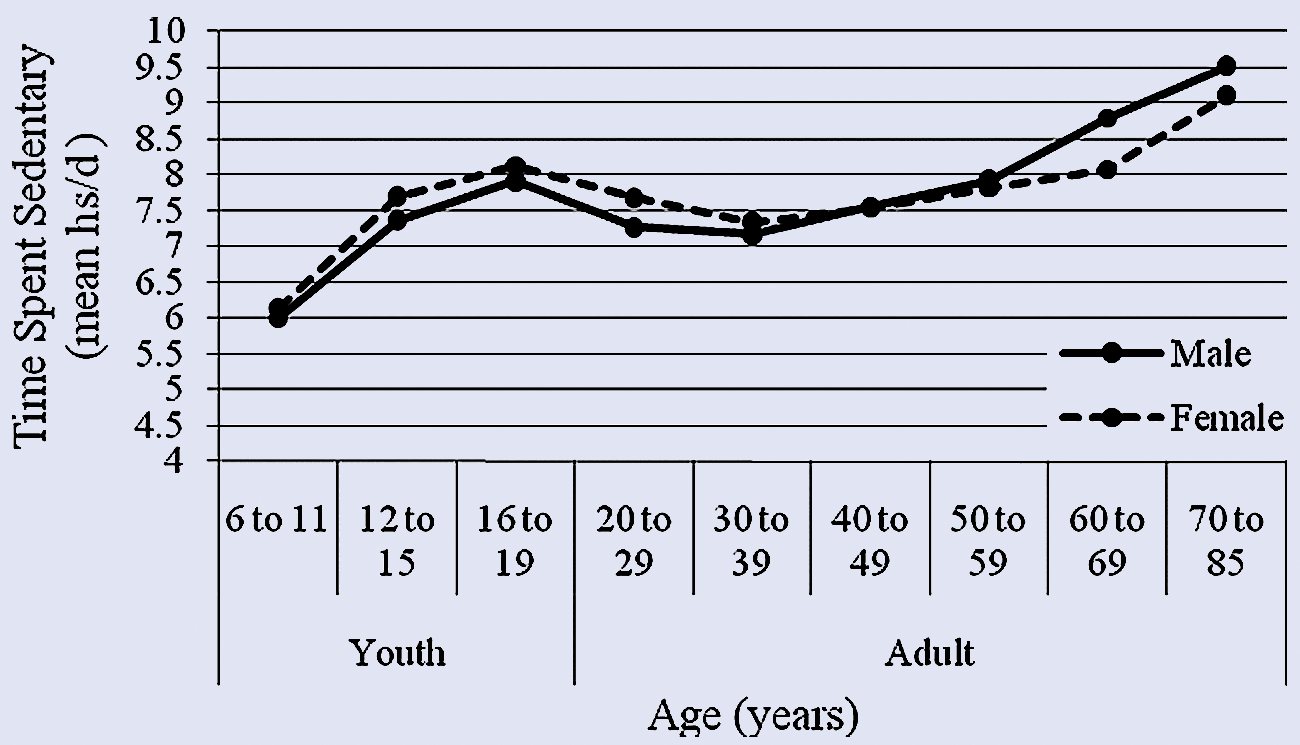
Amount of Time Spent Sedentary in the United States (NHANES 2003-2004).a
Relationships between TV viewing and MVPA appear equivocal in samples of adults, although there is more consistent evidence that associations might be negative for women. 86 Stronger objective evidence exists that sedentary behavior and light-intensity activity are inversely related in both men and women.46,87 A systematic review by Wendel-Vos and colleagues 88 examined physical and sociocultural determinants of a sedentary lifestyle during adulthood and found few significant relationships. The few significant associations were indicated by single studies, which prevented meaningful conclusions being drawn. However, it should be noted that many studies operationalized “sedentary lifestyle” as a lack of PA, and potential correlates were selected based on hypothesized relationships with PA rather than sedentary behavior. Of the few studies that assessed sitting behavior, only one 89 reported consistent associations with features of the physical environment (satisfaction with neighborhood, accessibility of facilities, land use mix, and safety from crime), but the directions of influence are conflicting and hard to interpret. Conference abstracts examining correlates of sitting time have started to emerge, which may indicate that peer-reviewed publications are on the way; however, at present, few published data are available.
What We Know
There exists an extensive literature on correlates of TV viewing among children and adolescents. Research is emerging on uses of other screen-based media such as computer use and video games, and initial relationships appear similar to that found for TV viewing. Health professionals should target modifiable correlates of children’s TV viewing, particularly reducing parental viewing and recommending that TV sets be removed from children’s bedrooms.
What We Need to Know
Although TV viewing remains the commonly studied sedentary behavior in children and adults, more data are needed about correlates of domain-specific sitting time (eg, transportation, leisure, occupation), particularly for adults. Despite the growing phase I evidence base of the deleterious effects of prolonged sitting time on health, data on modifiable correlates of sitting time among adults are virtually nonexistent. More prospective studies are needed to examine how changes in hypothesized correlates of sedentary behavior are related to actual behavior change.
Interventions to Reduce Sedentary Behavior (Phase IV Research)
Recent reviews of interventions designed to reduce sedentary behavior in children and adolescents have focused almost exclusively on screen-based media use.90,91 DeMattia and colleagues 90 reviewed 12 controlled intervention studies published between 1966 and 2005 that attempted to reduce recreational screen time and/or body weight in children and adolescents. Of these studies, 6 were clinic-based interventions, and 6 were population-based prevention studies. Although the length of the interventions varied as well as the setting and type of behavior change strategies used, studies report consistent reductions in self-reported hours of TV/video viewing. Concomitant changes in weight outcomes are usually modest, although interpretations are often confounded by natural age-related increases in BMI.
Summerbell and colleagues 91 reviewed 22 randomized controlled trials as part of a Cochrane review of the effectiveness of interventions for preventing childhood obesity. Only 2 studies92,93 reported significant decreases in sedentary behavior, and both were school-based programs. School-based interventions appear to be the most effective at reducing self-reported screen use during leisure time, which provides support for a public health approach to reducing youth sedentary behavior. 90 Two other theory-driven school-based randomized controlled trials to reduce recreational screen time of 10- to 12-year-old children have since been published, with one finding a reduction in screen use 94 and the other reporting no change. 95 Intervention strategies that appear to be efficacious for reducing screen time include behavioral contracting, offering rewards contingent on meeting screen reduction goals, time budgeting, and using TV turn-off challenges. 90 Education-only strategies appear to be largely ineffective. Thus, behavioral interventions for reducing screen time in children and adolescents are now recommended by the Centers for Disease Control and Prevention’s Task Force for Community Preventive Services. 91 It is important to note that very few interventions are designed to compare targeted reductions in sedentary behavior with attempts to increase PA, and thus, it is difficult to know whether reductions in screen time can occur in the absence of strategies to increase PA. In addition, virtually no interventions use objective measures of either sedentary behavior or of screen use.
To the best of our knowledge, there are no intervention studies in adults that focus exclusively on reducing sedentary behavior. Moreover, there are no intervention studies in adults that have targeted reductions in TV viewing despite the known association between TV viewing and obesity in adults23,43-45 and previous recommendations that these interventions be tried.97,98
A few studies have examined changes in sitting time, but these have involved secondary analyses of data from PA interventions.99,100 As part of a 12-month pedometer-based intervention in Belgium (10 000 steps Ghent), De Cocker and colleagues 99 found that self-reported sitting time (measured using the IPAQ) declined by 12 minutes per day for participants in the intervention condition, compared with an 18-minute increase among participants in a comparison community. Sitting time decreased more in participants who increased their step counts. However, a recent study 100 found no changes in occupational sitting following a workplace walking intervention, despite observed increases in PA. Workplace interventions that target sitting may have the potential to improve employee health because a recent observational study 51 found that workers who took short frequent breaks (2-3 minutes) from sitting had more favorable cardiometabolic risk profiles than workers who did not take breaks. These data are particularly important because an objective measure of sitting time was used, and findings remained after adjusting for levels of MVPA.
What We Know
Behavioral interventions to reduce self-reported sedentary behavior, and screen-based media use in particular, appear efficacious for children and adolescents. Evidence-based strategies for reducing screen time derive mostly from behavioral learning theory and include behavioral contracting, offering rewards contingent on meeting screen reduction goals, time budgeting, and using TV turn-off challenges. These strategies should be used by health professionals. Simply educating children and parents about excessive TV viewing appears ineffective as a stand-alone strategy to reduce the behavior.
What We Need to Know
There is need for randomized controlled trials that exclusively target reductions in sedentary behavior. Available data are based on interventions that combine strategies to increase PA and reduce sedentary behavior, making it difficult to tease apart their individual efficacy. The effects of reducing screen-based media use in adults remain unknown. Interventions to reduce domain-specific sitting time (eg, leisure, occupation, transportation) in adults are also needed, and studies targeting increases in MVPA should report how this affects sitting time or other measures of sedentary behavior. Intervention studies should use objective measures of sedentary behavior where possible.
Translate Sedentary Behavior Research Into Practice (Phase V Research)
Translational research constitutes the final phase in the sedentary behavior epidemiology framework. When interventions are shown to be effective in controlled trials (phase IV), they need to be translated for use in diverse settings such as schools, work sites, and primary care in order to have a public health impact. When evidence linking sedentary behavior to poor health (phase I) is considered strong, consistent, and causal, translational research also involves the development and adoption of public health guidelines and recommendations on appropriate levels of sedentary behavior for children, adolescents, and adults. Phase V research also includes descriptive research on methods of dissemination, adoption, implementation, and maintenance of sedentary behavior change programs to better understand factors that lead to institutionalization. 18 Because the scientific study of sedentary behavior is relatively new, there are few efficacious programs that are ready for translation to public health settings. To date, the majority of studies have focused on the health risks, etiology, measurement, and correlates of sedentary behavior. As the subfield matures it can be expected that a greater number of translation studies become available.
One of the few translation attempts in sedentary behavior research has been the development and adoption of national recommendations for youth sedentary behavior. Although very few published reports present specific guidelines for the amount of sedentary behavior that is recommended for young people, most experts agree that young people, especially those in elementary or primary school, should avoid prolonged periods of inactivity altogether, especially during daylight hours. 101 The most widely cited recommendation is from the American Academy of Pediatrics (AAP), 102 which recommends that parents limit children’s total entertainment media time to no more than 1 to 2 hours of quality programming per day; discourage television viewing for children younger than 2 years, and encourage more interactive activities that will promote proper brain development, such as talking, playing, singing, and reading together. To date, only Australia and Canada have formally adopted and published guidelines about the time young people should spend engaged in sedentary behavior. The Australian government 103 have adopted the AAP recommendations, and Health Canada recommend incremental decreases in screen-based media for physically inactive children. 104
What We Know
There have been few translation studies of sedentary behavior because research studies have focused largely on building the phase I, II, and III evidence base. Based on the strength of the evidence linking screen-based media use to childhood obesity, some countries have started to adopt public health recommendations for youth sedentary behavior. Until more phase I research evidence emerges, it is recommended that health professionals use AAP guidelines, which recommend that parents limit children’s total entertainment media (TV, video games) during leisure time to no more than 1 to 2 hours per day. Although this guideline was intended for children and adolescents, it can also be recommended for adults. This guideline should be accomplished using the behavioral strategies discussed earlier. However, this will require parents to undergo basic behavioral skills training, which could be offered by schools and health professionals. If health professionals simply prescribe this guideline in a didactic fashion, it is likely to be ineffective. Children younger than 2 years of age should be discouraged from watching television altogether and encouraged to participate in more interactive activities such as talking, playing, singing, and reading together.
What We Need to Know
Until research evidence builds on phases I to IV of the sedentary behavior epidemiology framework, translational studies of program effectiveness are likely to have little public health impact. However, as countries begin to adopt national guidelines about appropriate levels of sedentary behavior, research evidence is needed to evaluate their public health impact. It is recommended that a validated evaluation model, such as the RE-AIM framework, 105 be used to guide public health impact assessment. The RE-AIM framework provides metrics of public health reach, effectiveness, adoption, implementation, and maintenance of programs to help decision making.
New Directions in Sedentary Behavior Research
It is generally accepted that interventions to reduce sedentary behavior should target both reductions in sitting time and increases in PA. A growing area of research is now focusing on increasing levels of PA at the low end of the intensity spectrum. 106 These activities include the small incidental movements associated with daily life such as postural control (transitions from lying to sitting to standing), slight movements (eg, fidgeting, talking, and typing), and light-intensity ambulation (eg, walking, doing chores, etc). The cumulative energy expended during these “subthreshold” activities has been termed nonexercise activity thermogenesis (NEAT). Observational and laboratory studies have indicated that time spent in NEAT is predictive of resistance to fat gain following overfeeding. 15 Reducing sitting time by 2.5 hours per day and replacing it with NEAT activities (ie, standing, light ambulation) could result in an additional 350 kcal of daily energy expenditure. 20
Levine and colleagues 107 have conducted novel intervention trials attempting to replace occupational sitting time with light ambulation, all while continuing to engage in office work. For example, in a study of 15 obese participants, it was reported that walking at 1.1 mph while working at a modified “treadmill desk” increased calorie expenditure by 119 kcalh −1. It subsequently hypothesized that using a treadmill workstation for 2 to 3 hours per day could lead to a 20- to 30-kg weight loss over a typical work year (assuming that all other facets of energy balance are kept constant). 107 Additional research with small samples has indicated that treadmill workstations are feasible and enjoyed by users 108 and do not appear to hinder cognitive tasks, attention, or reading comprehension.109,110 Thus, an interesting future direction for sedentary behavior research is to evaluate well-designed interventions that attempt to reduce sitting time among children and adults by using similar NEAT-enhanced activities. At present, there are no randomized controlled trials of NEAT-based interventions designed to reduce sitting time.
In addition to novel interventions targeting occupational sitting, there exists immense potential for ubiquitous wireless technology (eg, cell phones) to act as persuasive tools to change health behaviors. 111 For example, many newer cell phones have triaxial accelerometers embedded into the hardware, which appear capable of harvesting data about PA. 112 No study has attempted to use cell phones to capture data about sitting time. Real-time continuous monitoring of sedentary behavior could be used to develop prompts to reduce sitting that are delivered via cell phones in an unobtrusive manner just at the right time (eg, following 30 minutes of continuous sitting). Although cell phone–based programs (often referred to as applications or “apps”) designed to monitor activity habits in real time have enormous potential, they are currently limited because of inconsistencies in the position of the phone when carried as well as the high energy demand on batteries when devices are required to sample data continuously. Assuming that these technical limitations can be overcome, field-based sensing of sedentary behavior could provide real-time feedback about postural habits and offer unobtrusive prompts of when and how to change. Context-aware sensing about the physical and social environment in which behavior occurs is also a rapidly emerging field, and this has exciting potential for understanding environments that promote prolonged sitting. To date, only short message service (SMS; often referred to as text messaging) interventions that “push” and “pull” information from participants have been used to change health behavior, 113 although even these have yet to be used to reduce sitting time. Passive or “calm” technologies (ie, those that require minimal input from the participant) have perhaps the most potential for reducing sedentary behavior. For example, cell-phone based accelerometers could use pattern recognition algorithms to detect specific behaviors and deliver context-aware just-in-time personalized feedback in a variety of subtle ways (eg, messages, vibrations, auditory signals).
Summary and Conclusions
The study of sedentary behavior as a concept distinct from PA presents a new paradigm in the science of PA promotion. Because emerging evidence suggests that sedentary behavior and PA have interdependent and independent effects on health, health promotion specialists should target reductions in sitting time, not just increases in MVPA. The most consistent evidence supports reductions in screen-based media use for overweight and obese children and beneficial strategies include removing the television from a child’s bedroom, behavioral contracting, offering rewards contingent on meeting screen reduction goals, use of screen time budgeting, using TV turn-off challenges, and reducing parental viewing.
Among adults, there is a growing literature that discusses how prolonged sitting at work may be related to deleterious health, but most studies have focused on distal health outcomes (eg, cardiovascular disease, mortality). Research on musculoskeletal consequences of occupational sitting (eg, musculoskeletal health) may yield additional evidence that sedentary behavior conveys a negative health risk. However, this will require more interdisciplinary and transdisciplinary collaborations with experts in health ergonomics, occupational health and safety, and the rehabilitation sciences. This approach, often referred to as team science, 114 is important if we are to avoid the silo-based model of knowledge accumulation that has dominated much of our field to date.
There is evidence that light-intensity PA conveys a health benefit, and simply encouraging frequent breaks in sitting time at work may prove beneficial. As new social and mobile technology emerges, devices and applications that are grounded in theoretical principles of health behavior change are likely to provide physicians and health care workers with greater ability to monitor and intervene in the sedentary habits of their patients and clients. Reducing sedentary behavior, not just increasing MVPA, should be an important strategy in the intervention repertoire of health promotion experts seeking to improve the health and well-being of their patients and clients.