
Abstract
Polypharmacy, commonly described as the use of five or more prescribed medications, is a prevalent health issue among seniors because of the potential adverse side effects due to medication interactions. The main purpose of this study was to investigate the association between dietary patterns and number of medications used. We hypothesized that a plant-based diet and healthy lifestyle choices decreases morbidities and number of medications taken. Data on 328 participants, aged 60 years or older, were collected through questionnaires and measurements at the Loma Linda University Drayson Center in Loma Linda, CA, between 2015 and 2016. The dependent variable was the number of pills taken, used as counts, and the main exposure was the type of diet adopted. Negative binomial regression was used for analysis. Results suggest that a vegan diet reduces the number of pills by 58% compared to non-vegetarian (IRR=.42 [95% CI: .25-.70]), even after adjusting for covariates. Increases in age, body mass index (BMI), and presence of disease suggest an increased number of pills taken. A vegan diet showed the lowest amount of pills in this sample. Body mass index also had a significant positive association with the number of pills.
“... vegan diet showed the lowest amount of pills taken in this sample...”
Introduction
Polypharmacy is a public health dilemma where multiple medications are prescribed to one individual. There are multiple definitions of what polypharmacy is, and this remains to be debated and universally defined to decrease confusion among researchers and clinicians. Nevertheless, polypharmacy does refer to the use of a large number of medications, wherein certain fields the criteria is considered to be the use of five or more medications. 1 It is initially essential to identify unnecessary drug prescriptions and then improve disease management with lifestyle modification to see if it is possible to diminish other medication when diseases are better controlled. However, we understand that this depends on each individual and that healthcare providers must have tight control over their medications and have prescription compliance. Disease complications can be minimized by better disease management with medication, lifestyle modification, or both. Individuals who take more than 5 medications daily have 88% higher risk of adverse drug events. 2 In consequence, patients with adverse drug events stay longer in the hospital, cost more, and have higher mortality rates. 3 Among homecare patients, this number can be much higher as it was observed in the ONEHOME study, with 51.5% of homecare patients in the polypharmacy group. 4
The improvement in life expectancy is one of the main reasons there is a higher use in medications. People are living longer, and the proportion of people aged 65 years and older is expected to be 23% by 2060. 5 The population growth is related to the baby boomer’s generation with increasing life expectancy as a result of improved healthcare services worldwide. 6 Due to the increase in life expectancy, the prevalence of chronic conditions associated with aging such as arthritis, osteoporosis, cardiovascular disease (CVD), diabetes, and cancer has risen. One issue that arises with multiple medication prescriptions is the potential adverse effects due to drug interactions. In older adults, polypharmacy increases the risk of fall injuries, hyperkalemia, hypokalemia, blood pressure issues, and heart failure. 7
It is imperative to assess what can lower the rate of polypharmacy among older adults. There have been inverse trends of healthier lifestyle choices and the rate of polypharmacy. In a study based in Spain, adherence to a healthier lifestyle was linked to a reduction of all-cause and CVD mortality associated with polypharmacy. Beneficial lifestyle behaviors included not smoking, a healthy diet, being physically active, and moderate or no alcohol consumption. 8 A case study described a treatment plan for a patient with a history of polypharmacy. The treatment included a plant-based diet and moderate physical activity, and the results led to the discontinuation of statins, antihypertensives, and the use of beta-blockers. 9
It was hypothesized that a plant-based diet is related to a reduction in the number of medications taken and the main purpose of the polypharma study was to analyze if there is an association between dietary patterns and the number of pills used.
Methods
Study Sample
This was a cross-sectional analysis of data collected by the Loma Linda University Drayson Center Office of Preventative Care in Loma Linda, California. A 40-item questionnaire was designed using selected questions extracted from the Adventist Health Study. 10 The questionnaire and the height/weight measures were administered and collected at the Drayson Center between September 2015 and October 2016. The number of participants recruited was 328 individuals. The inclusion criteria included speaking English and being 60 years and older. Exclusion criteria included incomplete surveys and participants who were younger than 60 years old.
Measures (Outcome and Exposure Variables)
The outcome of interest was the number of pills (prescribed and over the counter) taken by the participants. The research question asked of participants was “how many prescribed or over-the-counter medications do you take per day (please include your totals even if you take two or more of the same)?”
The main exposure variable consisted of the different types of diet the participants follow. Participants were asked the following question: “What type of diet do you follow?” The possible answers included vegan (no dairy, eggs, fish, or meat); lacto-ovo vegetarian (do not eat pork, beef, poultry, fish, or animal flesh of any kind, but do consume eggs and dairy products); pesco-vegetarian (fish, but no meat); lacto vegetarian (do not eat any type of animal meat or even poultry and eggs but consume milk); non-vegetarian (eat meat and/or fish at least once a week). Lacto vegetarian was added to the lacto-ovo vegetarian group due to the lower number of participants in this lacto group.
Other lifestyle factors investigated were physical activity, diagnosed chronic conditions, BMI, and sociodemographic variables such as age, gender, marital status, and education level. BMI index measured as kg/m2 was calculated after the collection of height and weight measurements.
The presence of cardiovascular disease (i.e., ischemic heart disease, peripheral artery disease, angina pectoris, and stroke) and risk factors for cardiovascular disease (e.g., diabetes mellitus, hyperlipidemia, and hypertension) were recorded. The information on the number of pills and the presence of diseases was acquired through the questionnaire.
Ethical Considerations
At enrollment, all participants were informed about the nature of the study and signed the informed consent to participate. The questionnaire was anonymous to protect participant privacy. The survey and measurements collected had the approval from the Loma Linda University Institutional Review Board (IRB# 5 150 344), and the study was conducted with all the ethics and safety concerns required by IRB.
Statistical Analysis
All data were analyzed with SPSS (version 25, IBM SPSS, Inc, Armonk, NY). Descriptive statistics were assessed for lifestyle and sociodemographic factors. Percentages were calculated for categorical variables and continuous variables are presented as means and standard deviations (SD). Univariable analysis was performed to determine the association between the dietary pattern and individual predictors, using one-way ANOVA or chi-square where appropriate.
To determine the relationship between the outcome and exposure variables, we used a negative binomial regression model. Negative binomial regression is for modeling count variables, usually for over-dispersed count outcome variables. Two models were run. The variables included in the first model include the type of diet as the main exposure variable, adjusted for age, gender, and BMI. For the second model, we further adjusted for exercise, education, and the presence of diseases. The diseases included were CVD (ischemic heart disease, peripheral artery disease, angina pectoris, and stroke) and risk factors for cardiovascular disease (diabetes mellitus, hyperlipidemia, and hypertension).
Multiple imputations were performed to deal with missing variables, and five new datasets were produced which were then summarized into averages. The percentage of missing answers per variable ranged from 1% to 9.4%. Variables that were imputed include gender, age, BMI, exercise, and education levels. Observations with missing information on dietary patterns and the number of pills taken or variables missing more than 30% of the answers after imputation were excluded from the analysis.
Results
The Polypharma Study: Characteristics of Participants of the Polypharmacy Study by Type of Diet.
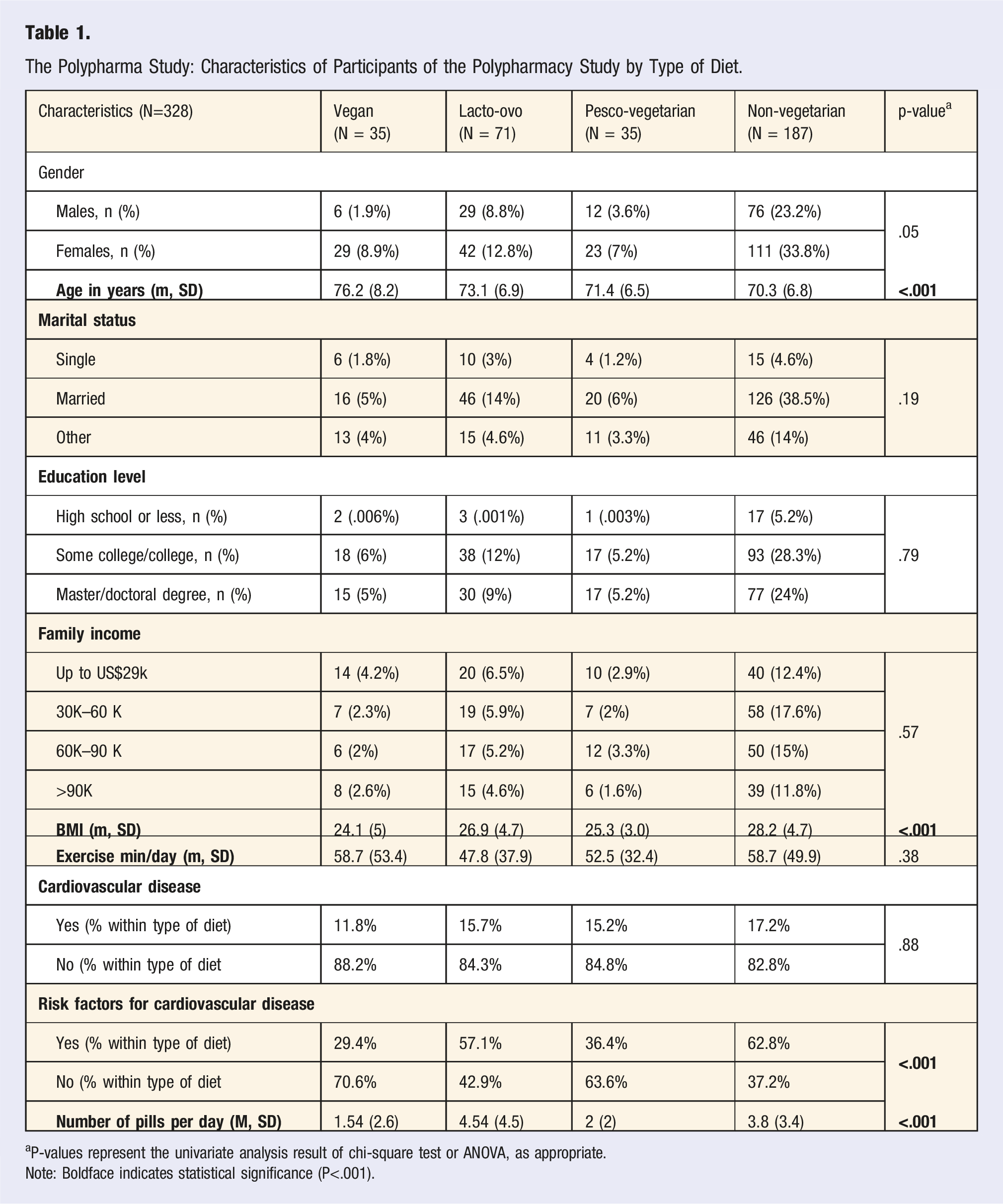
aP-values represent the univariate analysis result of chi-square test or ANOVA, as appropriate.
Note: Boldface indicates statistical significance (P<.001).
The association between diet and number of pills, adjusted for gender, age, and BMI (n=328).
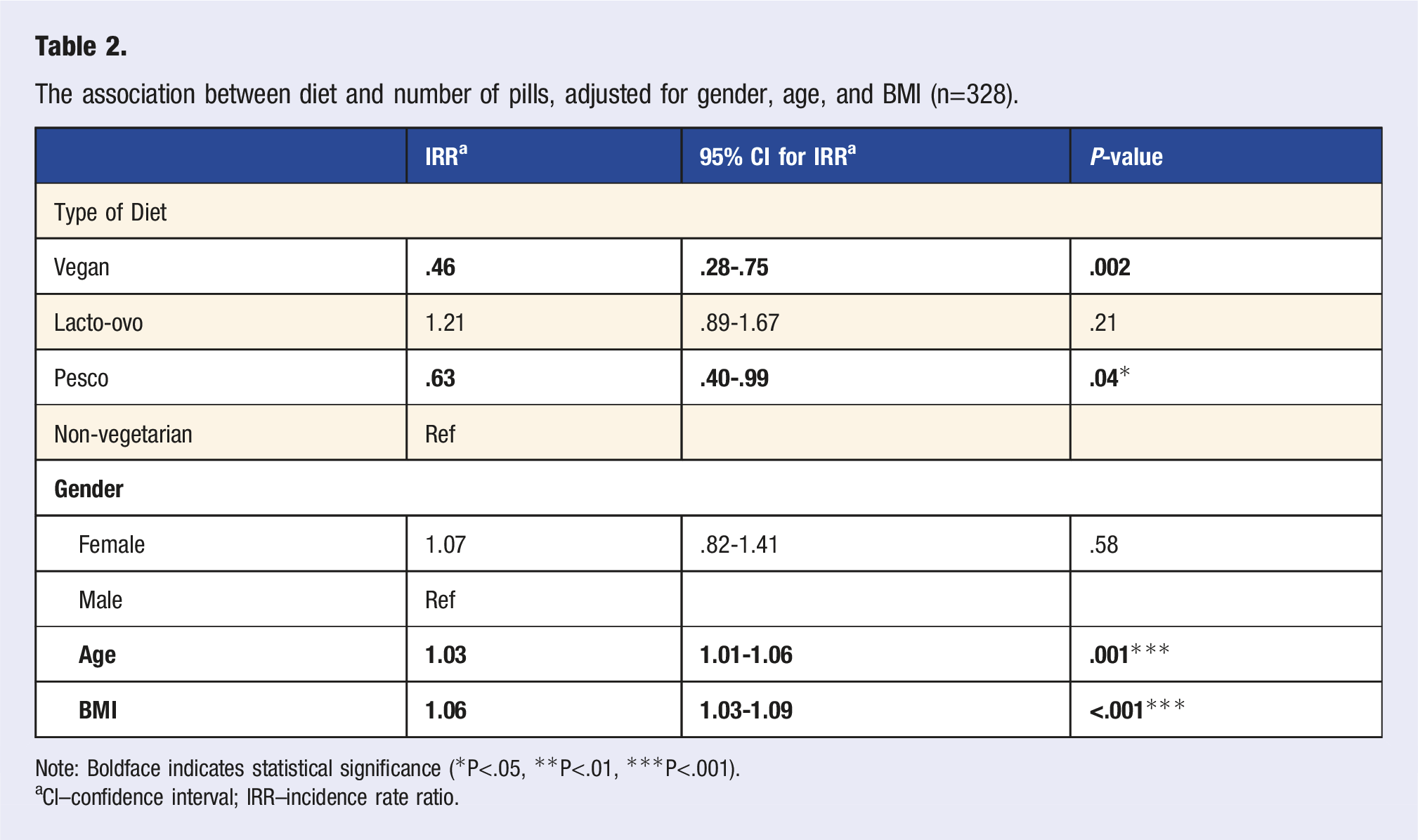
Note: Boldface indicates statistical significance (*P<.05, **P<.01, ***P<.001).
aCI–confidence interval; IRR–incidence rate ratio.
The association between diet and number of pills, adjusted for gender, age, BMI, other covariates (n=328).
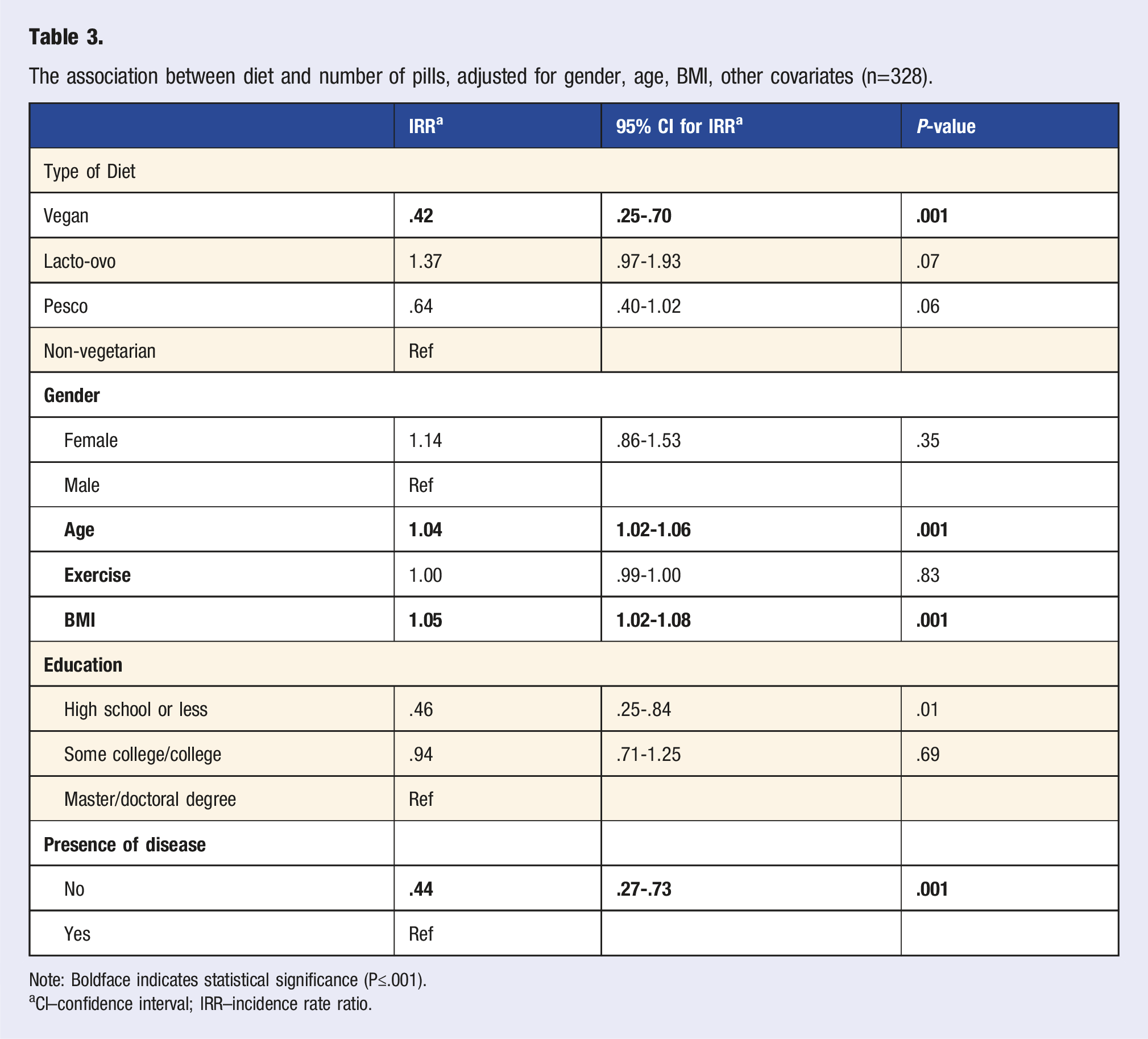
Note: Boldface indicates statistical significance (P≤.001).
aCI–confidence interval; IRR–incidence rate ratio.
Discussion
The purpose of the polypharma study was to assess whether lifestyle behaviors (including diet patterns) were associated with the amount of medications used by either increasing or decreasing the risk of polypharmacy. Moreover, polypharmacy was found to be commonly associated with chronic lifestyle diseases such as hypertension, diabetes mellitus, kidney, and cardiovascular diseases. 11
A vegan diet showed a decrease rate of the number of pills when compared to non-vegetarians. In general, a vegan diet presents with lower ingestion of total calories. Vegans eat less saturated fatty acids, have a higher intake of fiber, and low glycemic index foods, which leads to fewer calories. A vegan diet may also present with a lower BMI, blood pressure, HbA1C, and cholesterol levels as well.12,13 Due to this characteristic, vegetarians and vegans have a lower risk of obesity, which improves glycemic levels and prevents diabetes. Moreover, foods with lower glycemic index and fiber such as vegetables, also ameliorates the glucose levels and reduces blood glucose among patients with diabetes.14,15 Finally, the lower intake of saturated fats prevents insulin resistance, even if there are no changes in body weight. 16
One interesting result was that in our sample the lacto-ovo vegetarians presented with similar results as non-vegetarians for the number of pills taken. Results from the Adventist Health Study cohort found that vegan diets, compared to lacto-ovo vegetarians, offered additional protection for obesity, hypertension, type-2 diabetes, as well as cardiovascular mortality risk. 17 The mechanism involved in such results may be due to a lower BMI among vegans.
We examined the impact of lifestyle factors such as type of diet, BMI, presence of disease, and exercise, as well as demographics (age, education, and gender) with
Although vegetarianism has been linked to a multitude of health benefits, such as lower BMI and less likelihood of chronic conditions, it is not a sustainable diet without proper planning.
Higher BMI presented the increased likelihood of polypharmacy as a one-point increase in BMI leads to an increase in the number of pills by 5%. Reasons for this have been documented in a study done by Johanna Jyrkkä, who found that an increase in BMI is associated with polypharmacy. 18 Moreover, in a Swedish cross-sectional study, older adults who had a BMI of 30.0 kg/m2 or more had over the two-fold risk of polypharmacy compared to those with lower BMI. 19 Another similar finding presented in a US study showed that the older adults who are taking seven or more prescription drugs have higher BMI than those taking fewer drugs. This suggests that increasing BMI leads to polypharmacy. 20 A potential mechanism for this finding is that medications are related to high BMI among the older adults which makes them have greater comorbidity burden such as type 2 diabetes, CVD, etc.18,19
Certain situations of polypharmacy are inevitable and have proper justification; a proper and expected protocol for a post-myocardial infarction can include an angiotensin-converting enzyme (ACE) inhibitor, a beta-blocker, aspirin, paracetamol, etc. 21 Chronic conditions that are not properly regulated can lead to other issues thereby increasing prescription use and causing the potential for other health issues. For example, patients with type 2 diabetes have a higher likelihood of developing or living with hypertension, hyperlipidemia, as well as inflammatory osteoarthritis, which via pharmaceutical intervention leads to more medications such as oral hypoglycemic, antihypertensive agents, statins, analgesics, anti-inflammatory drugs, etc. 22
The presence of cardiovascular diseases and risk factors for cardiovascular diseases were found significantly associated with the number of pills taken in our model. Moreover, higher BMI and older age is associated with an increased rate of the number of medications.
No matter what the income was for the participants, it does not influence the outcome of the study. Family income was not related to the major independent variable which is diet. The most prevalent income for this group was US$30k–US$60k (27.8%).
Some previous studies have assessed different types of diet in relation to polypharmacy risk. 9,23 In this study, it has been proven that a fully plant-based diet has a significant impact on lower usage of pills in older adults’ cohort.
Limitations
A contributing factor is a lack of follow-up post-survey. This study was a self-reported cross-sectional study and thus was not possible to assess the cause and effect relationship. This questionnaire did not address potential confounding factors such as race, ethnicity, religion, and cultural preferences. Regarding the number of pills mentioned in the introduction, we did not reach those numbers in our study—probably because of the healthier nature of our population. Future studies will need to assess diet quality index, as well as cultural preferences, race, and ethnicity. The population we analyzed are middle to high income (more than $30k annually), educated, and most have health insurance; we cannot generalize this to the population of the whole country.
Conclusion
A vegan diet showed the lowest amount of pills taken in this sample. Using a negative binomial model, even after adjusting for covariates, vegans had the lowest rate of number of pills when compared to non-vegetarians. This is a pilot project to understand the polypharmacy situation in our population. Future research is needed to better understand the association with pills and lifestyle for specific diseases such as diabetes and hypertension and ultimately design interventions to assess the effects of lifestyle on polypharmacy.
Footnotes
Acknowledgments
The research presented in this paper is that of the authors and does not reflect the official policy of the NIH. The data collected had the approval from the Loma Linda University Institutional Review Board (IRB# 5150344), and the study was conducted with all the ethics and safety concerns.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.