
Abstract
Age-related macular degeneration (AMD) is a leading cause of irreversible vision loss among older adults, with both genetic and modifiable risk factors contributing to disease progression. Robust prospective evidence demonstrates that dietary patterns rich in lutein, zeaxanthin, and omega-3 fatty acids—particularly through green leafy vegetables, fatty fish, and Mediterranean diet adherence—reduce AMD progression risk by 20-56% across disease stages. Lifestyle factors including smoking cessation, weight management, and regular physical activity also confer protective benefits. Despite ample evidence, counseling about the benefits of these dietary and lifestyle behaviors remains underutilized in ophthalmic practice, largely due to inadequate medical education in preventive medicine and perceived barriers to implementation of such recommendations. This perspective examines the current evidence, highlights the gap between scientific evidence and clinical implementation, and proposes a framework for systematic reform. Recommendations include embedding nutrition education into medical school and residency training, establishing ocular nutrition as a continuing education requirement, and equipping clinicians with tools for incorporating these guidelines into routine AMD clinical care. Aligning ophthalmic practice with the recommended nutritional guidelines and other behavioral changes through the Macular Degeneration Preventive Diet and Lifestyle, represents a timely opportunity to translate evidence into interventions that preserve vision.
Keywords
“Clinician–patient interactions can provide key opportunities to influence macular health through behavior change, and vision preservation should begin far earlier than pharmacologic or surgical intervention.”
Age-related macular degeneration (AMD) is a chronic neurodegenerative disease which remains a leading cause of irreversible vision loss worldwide, particularly in older adults in industrialized nations. 1 While genetic susceptibility contributes significantly to an increased risk of vision loss due to a higher likelihood of progressing to the advanced stages of AMD, recent prospective evidence demonstrates that well-established dietary and lifestyle behaviors can offset a high genetic predisposition. 2 Despite compelling research and supportive national policy, dietary and lifestyle interventions remain underexplored in ophthalmology training programs and underutilized in clinical practice.
What is the Evidence Supporting Diet and Lifestyle in AMD?
The protective association between dietary carotenoids and AMD was first demonstrated in the 1994 JAMA report, where individuals in the highest quintile of lutein–zeaxanthin intake (6 mg/day) showed a 56% lower risk for AMD compared with those in the lowest quintile. 3 Those consuming green leafy vegetables such as spinach and kale (rich in lutein–zeaxanthin carotenoids) 5-6+ times per week experienced substantially reduced risk. Since then, other studies have confirmed this protective association between carotenoid rich foods and reduced progression to advanced AMD.2,4,5 Furthermore, the intake of ≥2.7 servings/week of green leafy vegetables and higher lutein-zeaxanthin intake was shown to reduce transitioning from early or intermediate AMD to higher AMD severity by 25% over 5 years follow-up. 6
Omega-3 fatty acids from fish, olive oil and nuts have similar protective effects. Twin studies and prospective analyses demonstrated that consuming ≥2 servings/week of fatty fish—such as salmon, sardines, or mackerel—reduced AMD progression rates by approximately 20%.6-9 Among individuals with moderate-to-high risk of progression, those with the highest dietary omega-3 intake had a reduced odds of developing either geographic atrophy or neovascular AMD by approximately 35%. 10
Macular pigments such as lutein–zeaxanthin carotenoids function as critical antioxidants in the fovea, while omega-3 fatty acids maintain photoreceptor membrane integrity through anti-inflammatory mechanisms. Because the body cannot synthesize these essential nutrients, dietary intake becomes essential for ocular health. This physiological mechanism underscores why “food is medicine” is particularly relevant for the management of retinal health.
Beyond individual nutrients, dietary patterns such as the Mediterranean diet—incorporating abundant vegetables, fish, nuts, olive oil, and minimally processed foods—show independent protective effects across AMD stages. 11 High adherence to this dietary pattern reduces progression to advanced AMD by 26% and slows drusen progression in intermediate disease.11,12 Oral micronutrient supplementation such as AREDS2 vitamins, which is standard recommendation for intermediate AMD, may also be beneficial for slowing progression of advanced geographic atrophy lesions toward the fovea and preserving central vision. 13
Lifestyle choices such as cigarette smoking, vaping, higher BMI, increased abdominal adiposity and various other anthropomorphic indices are associated with an increased risk for AMD and progression of the disease.14-16 In contrast, higher levels of weekly physical activity and quitting smoking are significantly associated with lower risk of AMD and progression to higher severity stages.2,9,15
Importantly, recommended dietary and lifestyle benefits appear independent of supplement use
2
,
6
,
11
,
12
and extend across the disease continuum through the stages of early, intermediate and advanced disease (Figure 1). Macular Degeneration Preventive Diet and Lifestyle for stages of age-related macular degeneration. AMD = age-related macular degeneration; AREDS2 = Age-Related Eye Disease Study 2; BMI = body mass index; GA = geographic atrophy.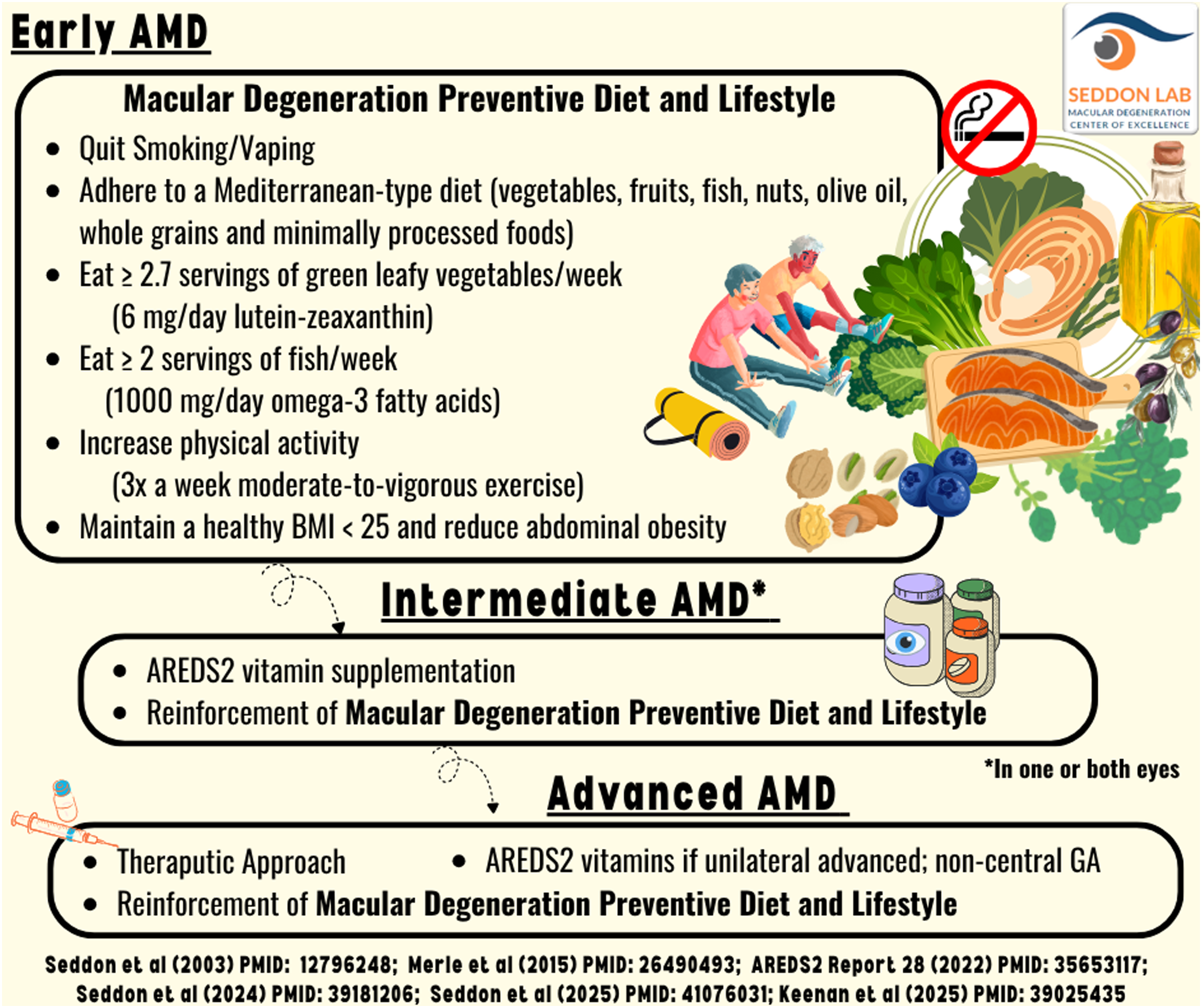
The Implementation Gap
Despite robust evidence, the translation of nutritional evidence into clinical practice is limited. Most patients with early or intermediate AMD may receive little to no AMD-specific dietary and lifestyle guidance beyond general health recommendations. Clinicians may feel inadequately trained in nutritional counseling or view it as outside their scope of practice. Medical schools, on average, provide fewer than 20 hours of nutrition instruction across 4 years, and while few residencies now include formal nutrition and lifestyle curricula, 17 ophthalmology residency programs do not include formal training in dietary or lifestyle counseling.
The American Academy of Ophthalmology’s 2025 Age-Related Macular Degeneration Preferred Practice Pattern® formally supports this approach, recommending that patients with intermediate AMD or advanced disease in one eye be counseled about Mediterranean diet adherence.11,18 The guideline explicitly notes the diet’s association with reduced incidence and progression of AMD, encouraging physicians to emphasize nutrition alongside traditional risk factor modification such as smoking cessation. Given the comparable magnitude of benefit between dietary improvement and quitting smoking, both warrant equivalent clinical emphasis.
Addressing Common Concerns
Some clinicians may question dietary recommendations given that randomized trials of omega-3 supplementation have not shown consistent benefit. However, this apparent contradiction likely reflects differences between whole foods and isolated supplements. Foods provide synergistic combinations of nutrients, fiber, and bioactive compounds that supplements cannot replicate. The consistent protective associations observed across multiple prospective studies, well adjusted for confounders, provide sufficient evidence to guide clinical practice, particularly for interventions with minimal-to-no risk and low cost.
Other clinicians may note that dietary counseling and subsequent behavior change take time. Yet brief, focused conversations can be highly effective. A simple one-page handout listing beneficial foods and practical examples of small, incremental changes can start the process, with reinforcement at follow-up visits. The Mediterranean diet is flexible and can be adapted to local, seasonal, cultural, and budgetary preferences, making it sustainable and non-restrictive to implement. Structured referral pathways to registered dietitians or board-certified lifestyle medicine specialists can further individualize guidance for all patients with AMD at a higher risk of progression or family members with higher susceptibility.
A Call to Action
The cumulative evidence establishes that modifiable lifestyle behaviors—specifically smoking, higher BMI and abdominal adiposity, greater caloric intake, and lower consumption of lutein–zeaxanthin and omega-3–rich foods—are important predictors for progression to advanced AMD. In genetically high-risk individuals, more than half of advanced AMD incidence is attributable to these modifiable factors. 2 If clinicians consistently discuss nutrition and lifestyle behaviors throughout the chronic disease continuum including AMD, vast public health benefits may be achieved at minimal cost. This intervention also offers benefits extending beyond eye health to cardiovascular disease, cognitive function, and overall well-being.
Addressing this deficit between evidence and implementation requires systematic reform: 1) Academic institutions should embed nutrition and lifestyle medicine into medical education, allocating curricular time for diet–disease mechanisms, counseling techniques, and behavior change strategies. Ophthalmology residency programs can include brief, hands-on modules that model how to integrate nutrition and lifestyle discussions into standard AMD care. 2) Professional organizations should establish ocular nutrition as a core competency within continuing education requirements. Continuing medical education programs should emphasize skills of delivering dietary and lifestyle guidance within time-constrained clinical interactions. A brief but focused discussion which reinforces key lifestyle and dietary principles with written resources, digital materials, and consistent follow-up, can meaningfully influence behavior. 3) Clinician–patient interactions can provide key opportunities to influence macular health through behavior change, and vision preservation should begin far earlier than pharmacologic or surgical intervention. If ophthalmologists treat diet and lifestyle as integral clinical tools rather than adjunct topics, they can educate patients and their family members to make evidence-based, modifiable choices that meaningfully reduce burden of a highly heritable disease across generations. 4) Clear, consistent, evidence-aligned messages from trained practitioners during routine clinical care could help counter nutrition misinformation, reduce health-related anxiety, and limit dissemination of non-evidence based wellness fads. Ophthalmologists and other eye-care practitioners can promote the Macular Degeneration Preventive Diet and Lifestyle (Figure 2) as part of a unified, evidence-based strategy. Emphasizing eating dark leafy greens, fatty fish and the Mediterranean diet for eye health, as well as not smoking, maintaining overall and abdominal weight, getting more exercise, echoes the guidance they receive for cardiovascular, metabolic, and cognitive health.
The release of the 2025-2030 Dietary Guidelines for Americans in January 2026 provides a timely moment to reinforce nutritional counseling for AMD.
19
These updated guidelines emphasize whole, nutrient-dense foods—consuming a variety of colorful vegetables, fruits and omega-3-rich seafood as a key protein source while limiting alcohol, highly processed foods and refined carbohydrates. These are precisely the dietary components shown to reduce risk of AMD progression. While the guidelines also include red meat, it should be limited for AMD prevention due to its relatively high saturated fat content compared with most plant proteins and many types of fish and poultry. Macular Degeneration Preventive Diet and Lifestyle. AMD = age-related macular degeneration; BMI = body mass index; kcal = kilocalorie.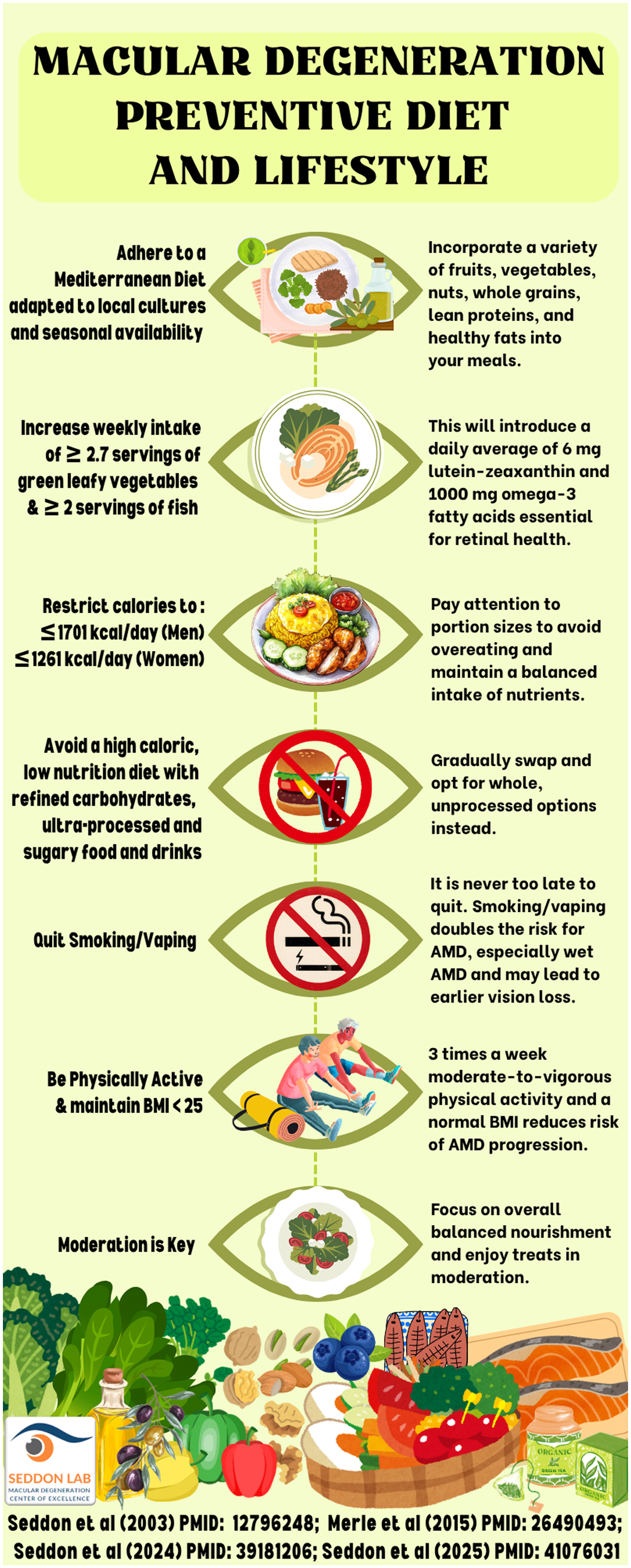
The phrase “you are what you eat” is an old but very relevant saying for prevention of eye diseases, as stated in the introduction of the book, Eat Right for Your Sight, a science-based cookbook for eye health. 20 For ophthalmologists and other eye-care professionals, closing the gap between evidence and clinical practice is both an opportunity and a responsibility. Each patient encounter offers a chance to show that vision preservation begins on the plate. As the population ages, integrating age-appropriate dietary and lifestyle guidance into routine ophthalmic care is essential for a chronic eye disease that disproportionately affects older adults. Implementation must also address common barriers in older adults, including limited access and affordability of healthy foods compared with ultra-processed options, drug–nutrition interactions, limited strength training and fall prevention, and insufficient access to nutrition counseling and oral health care. Aligning ophthalmic care with nutrition policy and healthy lifestyles can help turn existing evidence into everyday actions that support healthy aging and preserve vision.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health National Eye Institute Grants R01-EY011309 and R01-EY028602, Bethesda, Maryland; American Macular Degeneration Foundation, Northampton, Massachusetts; Macular Degeneration Center of Excellence, University of Massachusetts Chan Medical School, Department of Ophthalmology and Visual Sciences, Worcester, Massachusetts.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.