
Abstract
Comprehensive lifestyle medicine programs have begun to show efficacy in patients with cerebrovascular disease. The Veterans Affairs (VA) health care system has a large poststroke population and VA rehabilitation departments have significant expertise and resources for promoting healthy lifestyles. A 12-week clinical lifestyle medicine program was therefore implemented for poststroke patients, along with an optional observational study evaluating cardiovascular fitness, function, body composition, vitals, and quality of life before and after the program. Seventeen of 18 clinical patients elected to participate in the study, and 3 later withdrew. The 14 participants improved VO2 max by 1.94 mL O2/min/kg (P = .001, 95% CI 0.96-2.90). Significant improvements were seen in estimated metabolic equivalents, exercise duration, 6-minute walk test, 30-second sit to stand, grip strength, and balance. Among patients who were hypertensive at baseline, mean decrease in supine systolic blood pressure (SBP) was −9.70 mm Hg (n = 10, P = .005, 95% CI −15.7 to −3.7) and standing SBP was −11.09 mm Hg (n = 11, P = .009, 95% CI −18.7 to −3.48). There were no significant improvements in laboratory measures or body composition. Participant satisfaction was high. These findings corroborate recent literature suggesting that lifestyle programs improve stroke recovery and reduce recurrence risk.
The primary goals of poststroke rehabilitation are functional recovery and recurrence prevention, yet standard physical therapy and medication regimens have limited impact on functional decline and underlying disease processes. 1 Fatigue and musculoskeletal changes, poor diet, social isolation, and stress act to increase morbidity and mortality poststroke, perpetuating a cycle of poor health and increased secondary stroke risk.1-4
Lifestyle medicine programs, including exercise, nutrition, stress management, psychosocial support, and education, have become established models for rehabilitation and secondary prevention of cardiovascular disease.5,6 Traditional cardiac rehabilitation programs reduce mortality and hospital admissions 7 ; more comprehensive intensive cardiac rehabilitation programs demonstrate greater benefits, including fewer cardiac events, reduced costs and procedures, improved symptoms, and reversal of atherosclerosis at 1 and 5 years.8-11 Given the similar etiologies between cerebrovascular and cardiovascular disease and the known role of physical activity, nutrition, and mental health in reducing primary stroke risk,1,12-14 there is growing interest in utilizing comprehensive cardiac rehabilitation models with stroke patients.15,16
Stroke burden among the veteran population is significant with roughly 15 000 veterans treated annually for stroke. 17 Veterans may have higher rates of cardiovascular disease than the general population, 18 and the Veterans Affairs (VA) has recognized the significant opportunity to reduce stroke burden through focusing on prevention. 19 VA rehabilitation departments house a wide array of resources to support healthy lifestyle in disabled populations, including staff expertise, adaptive equipment, and facilities. Utilizing these resources, a 12-week outpatient lifestyle medicine program was established at a large VA hospital for transient ischemic attack (TIA) or mild-moderate stroke patients. An pilot observational research study was conducted to assess the cardiovascular and functional outcomes of the clinical program.
Methods and Materials
Patient Population
Two successive 12-week clinical Wellness in Rehabilitation (WIR) programs were held during fall 2017 and spring 2018. Patients enrolled in the poststroke WIR clinical program at the VA Palo Alto Health Care System (VAPAHCS) were recruited for the observational study, which was approved by the Stanford University Institutional Review Board. Patients were selected for the WIR program based on provider referrals and medical record evaluation. Inclusion criteria for both the WIR program and research study included the following: ischemic or hemorrhagic stroke within 1 year, ambulate ≥10 feet with moderate assistance, and eat with modified independence. Exclusion diagnoses included the following: cerebral aneurysm, terminal illnesses, and moderate-severe dementia.
Patients enrolled in the study provided written informed consent and completed baseline physician screening, exercise stress testing with VO2 max, blood testing, dual-energy x-ray absorptiometry (DXA) scan, psychosocial assessment via questionnaires, and functional evaluation and exercise prescription by a physical therapist. Assessments were repeated postprogram.
Fitness and Function
Resting supine and standing blood pressures were measured twice prior to exercise testing. Blood pressure was also taken at regular intervals during and after testing. A standard cardiopulmonary exercise test (COSMED Omnia system) was performed either on an upright cycle ergometer or treadmill following American Heart Association/American Stroke Association (AHA/ASA) protocols.1,20 Functional assessments included dynamometer grip strength, Berg Balance Test, timed up and go (TUG), 6-minute walk test (6MWT), and 30-second sit to stand (30STS).
Body Composition
DXA total body scan (GE/Lunar iDXA, GE Healthcare) was performed to measure total, lean, and fat mass.
Questionnaires
Survey instruments included Beck Depression Inventory-II, RAND 36-Item Short Form Health Survey (SF-36), Physical Activity Scale for Individuals with Physical Disabilities, and Montreal Cognitive Assessment (MoCA).
Laboratory Measures
Laboratory measures included hemoglobin A1c (HbA1c), fasting glucose, erythrocyte sedimentation rate (ESR), low-density lipoprotein cholesterol (LDL cholesterol), high-density lipoprotein cholesterol (HDL cholesterol), total cholesterol, triglycerides, vitamin D 25-hydroxy, and vitamin B12.
Statistical Analysis
Paired T tests were performed to compare assessments pre- and postintervention. Given the difficulty of assessing the parametric nature of a small dataset, comparisons were also performed using the Wilcoxon signed-rank test. No values lost statistical significance (P > .05) with this test. Analyses were performed using SPSS Statistics software (Version 25.0. IBM Corp.).
Clinical Program
The WIR program consisted of 12 weekly, 5-hour group sessions held at VAPAHCS. Each session included exercise, cooking, mindfulness, education, and group support.
Group exercise focused on light to moderate intensity aerobic training with a secondary focus on strength, flexibility, and balance, and included land and aquatic sessions. Patients were divided by functional ability into groups, which were led by a physical therapist, recreational therapist, or program assistant.
Cooking sessions focused on whole food, plant-based meal preparation and healthy eating habits. Sessions took place in an activity room with a sink, but no kitchen. Cooking was done using portable induction burners and microwaves. During each session, patients were given a brief lesson, such as knife skills or cooking grains, which they applied to prepare a meal.
Mindfulness sessions were largely based on the mindfulness-based stress reduction (MBSR) program, and utilized the freely available Palouse MBSR resources. 21 Exercises included visualizations, mindful eating, breathing techniques, and basic yoga postures.
Lectures were given by clinical staff and topics included nutrition, stress, exercise, sleep and social connection. Group support included both patients and caregivers and was led by a physician or social worker. Each session included individual updates and discussion of a general topic such as purpose or gratitude.
At home, patients were asked to exercise, eat a healthy diet (defined as ≥4 cups of fruits and vegetables daily), practice mindfulness exercises and record daily whether they completed these tasks using paper or Health Storylines software. 22 Therapists and social workers served as health coaches who called each patient weekly for support.
Results
Across fall 2017 and spring 2018 clinical sessions, 155 potential candidates admitted for stroke at the VAPAHCS inpatient facility were screened for the clinical program. A total of 62 met eligibility criteria, and a total 18 enrolled, evenly distributed across the fall and spring cohorts. Seventeen patients further agreed to undergo pre- and postprogram evaluation for research, and 14 of these patients successfully completed research assessments; attrition was due to transportation burden or health issues. Four participants elected to bring a caregiver to weekly sessions, which was encouraged.
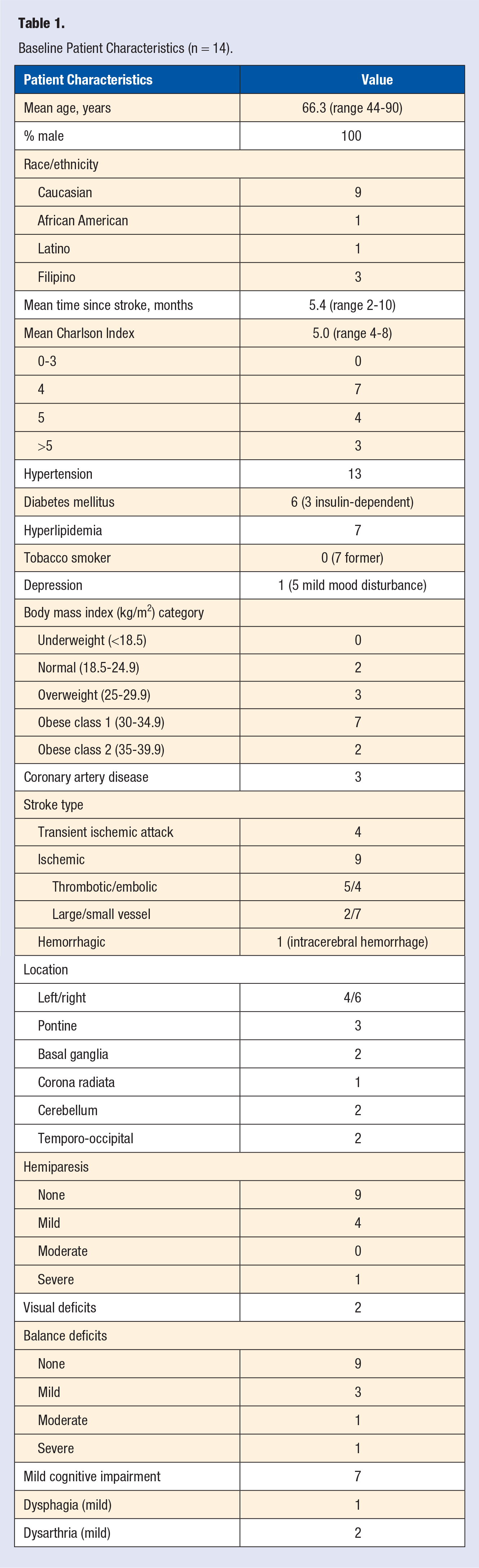
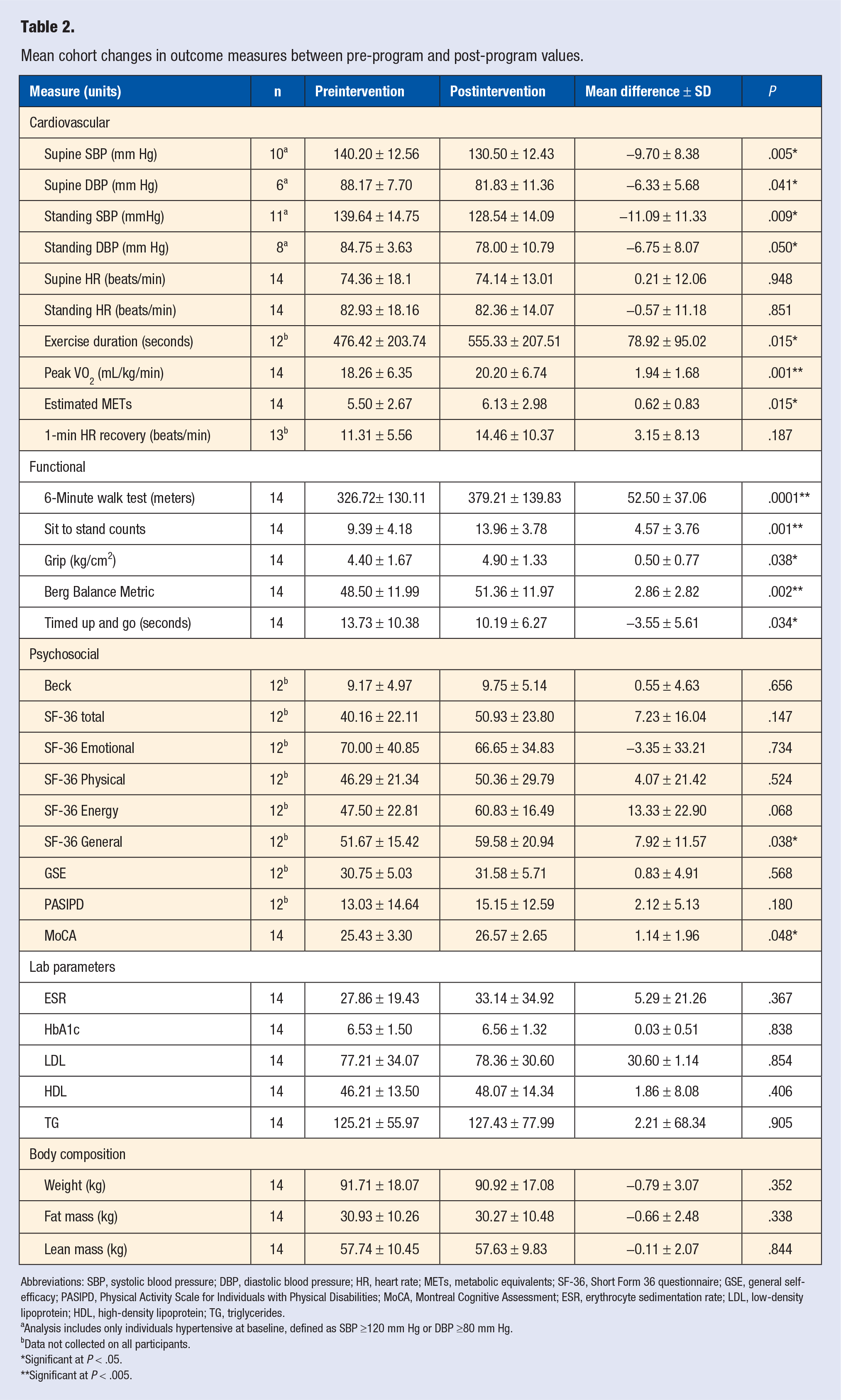
Combined cohort demographics across the 2 sessions are summarized in Table 1, and key cohort outcomes are summarized in Table 2. Among baseline hypertensive participants (systolic blood pressure [SBP] ≥120 mm Hg), a mean improvement of −9.70 mm Hg was demonstrated for supine SBP (n = 10, P = .005, 95% CI −15.70 to −3.7) and −11.09 mm Hg for standing SBP (n = 11, P = .009, 95% CI −18.70 to −3.48). One participant had a blood pressure medication change; if excluded, supine SBP improved −8.33 mm Hg (n = 9, P = .011, 95% CI −14.19 to −2.48) and standing SBP by −9.20 mm Hg (n = 10, P = .016, 95% CI −16.31 to −2.09). While fewer participants had elevated baseline diastolic blood pressure (DBP ≥80 mm Hg), supine DBP improved −6.33 mm Hg (n = 6; P = .041, 95% CI −12.29 to −0.37) and standing DBP by −6.75 mm Hg (n = 8; P = .050, 95% CI −13.49 to −0.01).
Baseline Patient Characteristics (n = 14).
Mean cohort changes in outcome measures between pre-program and post-program values.
Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; METs, metabolic equivalents; SF-36, Short Form 36 questionnaire; GSE, general self-efficacy; PASIPD, Physical Activity Scale for Individuals with Physical Disabilities; MoCA, Montreal Cognitive Assessment; ESR, erythrocyte sedimentation rate; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglycerides.
Analysis includes only individuals hypertensive at baseline, defined as SBP ≥120 mm Hg or DBP ≥80 mm Hg.
Data not collected on all participants.
Significant at P < .05.
Significant at P < .005.
Cardiopulmonary fitness improvements were noted in peak VO2 max (1.94 mL/kg/min, P = .001, 95% CI = 0.96-2.90), estimated metabolic equivalents (METs; 0.62, P = .015, 95% CI = 0.14-1.10), and exercise duration (78.92 seconds, P = .015, 95% CI = 18.54-139.29). There was no significant improvement in post exercise 1-minute heart rate recovery or resting heart rate. Mean improvements were significant across all functional tests, including 6MWT (52.50 m, P = .0001, 95% CI = 31.10-73.90), 30STS (4.57 sit-stands, P = .001, 95% CI = 3.29-6.74), grip strength (8.05 kg/cm2, P = .034, 95% CI = 0.03-0.96), Berg balance test (2.86 points, P = .002, 95% CI = 1.27-4.49), and TUG (−3.55 seconds, P = .034, 95% CI = 0.31-6.78).
No significant changes were noted in body composition or laboratory measures, including weight, HbA1c, fasting glucose, ESR, HDL, LDL, triglycerides, total cholesterol, or vitamins B12 or D.
Two patients did not complete the self-administered surveys postprogram and were excluded from evaluation. While there was improvement in SF-36 General Health (7.92, n = 12, P = .038, 95% CI = 0.56-15.27) and MoCA scores (1.14, P = .048, 95% CI = 0.014-2.27), no other standardized psychosocial measures showed significant improvement.
The combined cohort sustained an average 89.3% (SD = 11%; range 62.5%-100%) weekly attendance over the 12-week program. Anonymously collected patient satisfaction scores assessed on a 10-point scale demonstrated high overall satisfaction, including likelihood to recommend to others (mean ± SD = 9.6 ± 0.96), helpfulness with lifestyle improvements (9.6 ± 0.70), importance to rehabilitation (9.6 ± 0.70), and overall enjoyment (9.9 ± 0.32).
Discussion
In this pilot study, 14 poststroke veterans showed significant improvements in a broad range of fitness and functional measures, as well as SBP and DBP, following participation in a comprehensive lifestyle intervention. These findings corroborate recent literature on the positive impacts of lifestyle changes in stroke rehabilitation.15,16
A primary goal of stroke rehabilitation is functional recovery. This study demonstrated significant improvements in multiple measures of functional ability, including the 6MWT, bilateral grip strength, 30STS, Berg Balance Test, and TUG.
Another primary goal of stroke rehabilitation is prevention of future events, and improvements in cardiovascular fitness and SBP correspond to reduced stroke risk and mortality.23,24 In this study, participants improved in VO2 max, estimated METs, and exercise time. While the long-term impact of these improvements has not been quantified in a poststroke population, a 1 MET increase corresponds with 10% to 40% reductions in mortality25,26 and a 17% reduction in stroke risk 23 in patients with cardiac disease. Study participants also showed significant blood pressure improvements without medication increases, including a mean SBP reduction of 9.7 mm Hg. A meta-analysis of randomized clinical trials has previously shown that a SBP reduction of 10 mm Hg is associated with a 34% relative risk reduction in secondary stroke risk over 3.1 years. 27 The SBP improvements in this study are consistent with those in recent meta-analyses and randomized controlled trials of poststroke interventional lifestyle programs.15,16
No significant improvements were seen in laboratory or body composition measures, which may be due to insufficient dietary and exercise change, existing medication (ie, statin), small sample size, and/or a short follow-up period. Multiple survey measures were used to further assess changes in quality of life, mood, physical activity, self-efficacy, and cognition. Among these, the MoCA and SF-36 General Health measures showed statistically significant improvements; however, the 1.14-point MoCA improvement is below the 4 point minimum detectable change. 28
Strengths of this study include the broad range of outcome measures, as well as participant diversity with regard to age (range 44-90 years) and race/ethnicity. In addition, participants had multiple comorbidities as assessed by the Charlson Index (range 4-8, mean 5.0), which suggests that lifestyle interventions may be successful in more complex, debilitated patients. Nevertheless, this study has several limitations. The small number of participants, short follow-up period, and all-male demographic limit the conclusions. In addition, no control group was used, so natural improvement in outcome measures is unknown. However, Pohl et al 29 followed 92 participants with similar demographics over the same time period and noted mean VO2 max improvement of 0.69 mL/kg/min, compared with 1.94 mL/kg/min in the current study. Last, costs and long-term outcomes were not assessed to determine whether the program adds value (improved outcomes at lower cost) to poststroke rehabilitation.
To the best of our knowledge, this is the first comprehensive lifestyle medicine intervention for poststroke patients to be evaluated at a VA facility. Notably, the program was implemented using staff and resources common to most VA rehabilitation departments. Given these resources and the lack of dependence on fee-for-service insurance reimbursement, VA rehabilitation departments nationwide may have the flexibility to implement similar programs. This aligns with the VA’s strong commitment to wellness and prevention through programs such as the Whole Health Initiative. 30 Furthermore, such programs appear to be well-received by patients. Anonymous surveys demonstrated high levels of satisfaction, and participants indicated that the group-based format provided community and peer support for healthy behavior change.
Conclusion
A comprehensive lifestyle medicine program demonstrated significant improvements in fitness, function, and blood pressure in a cohort of 14 poststroke veterans with significant comorbidities. These improvements are consistent with the primary poststroke rehabilitation goals of functional recovery and recurrence prevention. Participant satisfaction in the program was very high. To our knowledge, this is the first lifestyle medicine program for stroke rehabilitation to be implemented at the VA, which is widely promoting wellness in the veteran population, and it may provide a model for wider VA implementation. Future research with control groups, larger populations, and longer follow-up periods is warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Salary support (JK) was provided by the VA Office of Academic Affiliations. Materials and program supplies were provided by the Department of Neurosurgery, Stanford School of Medicine and VA Rehabilitation R&D Service.
Ethical Approval
Patients enrolled in the poststroke Wellness in Rehabilitation (WIR) clinical program at the VA Palo Alto Health Care System (VAPAHCS) were recruited for the observational study, which was approved by the Stanford University Institutional Review Board.
Informed Consent
Patients enrolled in the study provided written informed consent.
Trial Registration
Not applicable.