
Abstract
Patients with chronic conditions are at higher risk of complications and mortality if they get COVID-19. Approximately half of American adults have at least 1 condition that increases their risk of complications if they become infected. The medical and public health communities need to send a clear message about the impact of lifestyle on health, particularly in the time of this pandemic. We need to communicate with patients and the public, to let them know how rapidly major lifestyle changes can improve health. This communication is urgent; the timeline for self-care and lifestyle medicine interventions has been telescoped, so that chronic diseases are now acute risk factors.
An optimally resilient host may be less likely to contract COVID-19 and, if infection occurs, may experience fewer and less severe complications from the disease.
Patients with chronic conditions are at higher risk of morbidity and mortality from COVID-19. Diabetes, chronic lung disease, coronary artery disease, obesity, and several other conditions have been identified as risk factors for severe illness. 1 Approximately half of American adults have at least 1 condition that increases their risk of complications if they become infected, 2 and even among young adults, the risk of severe illness is 1 in 3. 3 Reducing the burden of chronic illness is, therefore, a rational strategy for reducing adverse outcomes of coronavirus infections.
Reducing risk from COVID-19 requires a multitiered approach. Incorporating currently available and potential tools, this effort can be conceptualized as a 4-tiered pyramid (Figure 1), in which the foundation involves strengthening the host with lifestyle interventions. An optimally resilient host may be less likely to contract COVID-19 and, if infection occurs, may experience fewer and less severe complications from the disease.
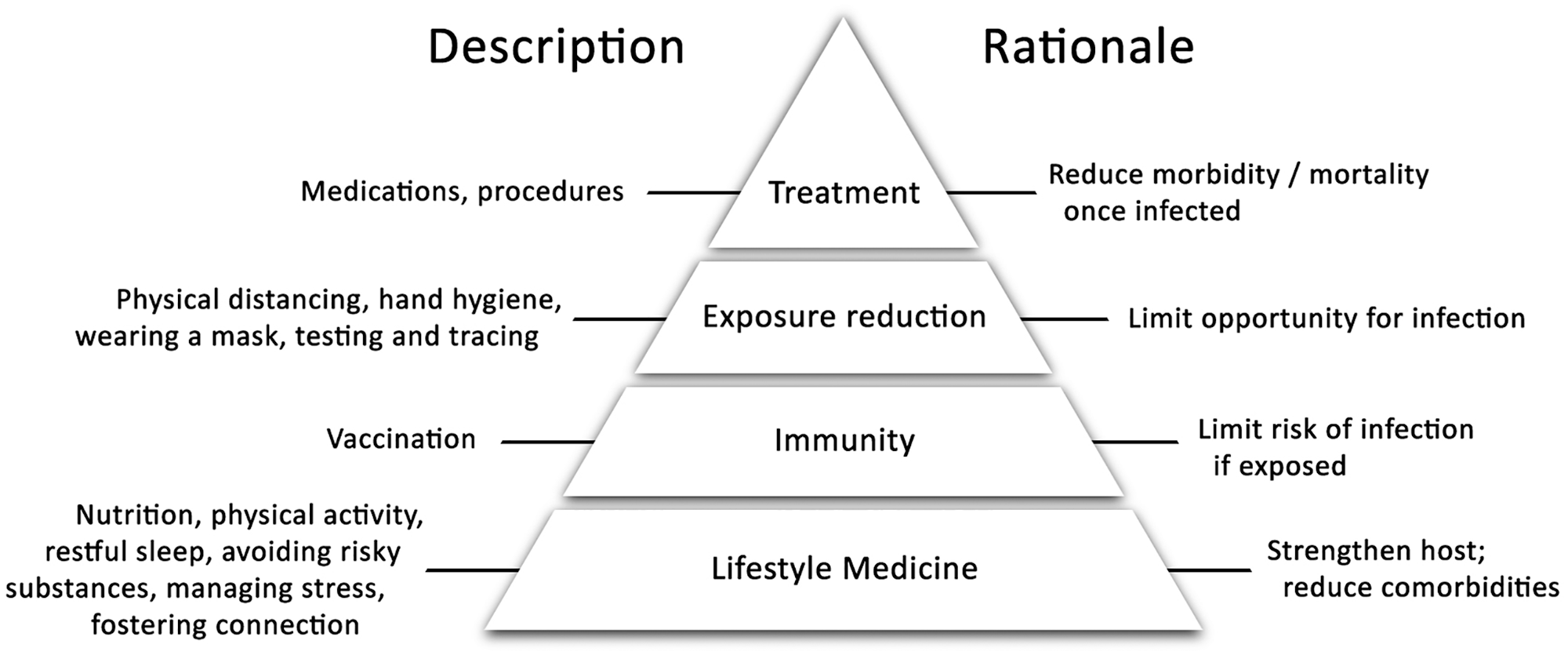
Four-tiered framework for reducing risk from COVID-19.
The second tier—not currently available—is vaccination, to reduce the risk of being infected. The third tier represents the next level of defense: reducing the risk of disease exposure, through physical distancing, frequent handwashing, covering one’s mouth and nose, and testing and tracing. The fourth and uppermost tier represents treatment with medications and procedures, once a patient has been infected, to reduce morbidity and mortality.
Whereas a great deal of attention has been focused on the top 3 tiers of this pyramid, less has been given to the foundation, despite observational evidence that lifestyle contributes to the risk of serious disease 4 and theoretical evidence that lifestyle could be protective. 5 The lack of concerted messaging about strengthening the host has hampered our ability to reduce complications at a time when prevention techniques and therapies are limited and less than completely effective.
In the traditional Levels of Prevention model developed more than 60 years ago, 6 primary prevention is aimed at reducing the risk of developing a target condition through efforts such as vaccination. Secondary prevention aims to reduce progression of a disease. In a pandemic, this can be accomplished through reducing the communicability of an infectious disease with public health efforts such as wearing masks. Tertiary prevention limits morbidity by treating established illness.
However, it has more recently been recognized that there is a more basic level of prevention—namely, primordial prevention. Primordial prevention reduces a population’s risk from the target illness and builds resilience against disease 7 by addressing the development of risk factors in the first place. 8 By preventing and treating the chronic illnesses that increase the risk of morbidity and mortality from coronavirus, lifestyle medicine provides a foundational approach for reducing risk from this pandemic.
Lifestyle medicine is the evidence-based practice of helping individuals and families adopt and sustain behaviors that improve health and quality of life. 9 It uses 6 pillars to reduce chronic illness: a whole-food, plant-predominant eating pattern; regular physical activity; restorative sleep; managing stress; avoiding risky substances; and fostering positive social connection. The chronic diseases that put patients at risk for complications from COVID-19 can be attenuated by these lifestyle medicine interventions.
It has been estimated that 80% of chronic conditions could be avoided through the adoption of recommendations for a healthy lifestyle. 10 However, multiple barriers prevent people from making changes that will help their health. These barriers involve patients, clinicians, and the health care system at large. Patients may be confused about the approaches that will reduce risk or may lack the skills that they need to implement changes. They may lack time and resources and may be faced with stresses that reduce the desire and ability to make lifestyle changes. Clinicians may lack education about the impact of lifestyle and may lack skills in coaching. They may not be practicing healthy habits themselves, making it less likely that they will recommend changes to their patients. Ineffective goal setting with patients may lead to their failure to make the recommended changes; practitioners then get discouraged, thereby setting in place a negative feedback loop. Finally, the health care system is not currently designed to address the root causes of disease; lack of time and reimbursement make it less likely that practitioners will work with patients to address the pillars of lifestyle medicine.
Behavior change is not easy. Practitioners who work with patients to help them change long-standing lifestyle patterns need not only to be well versed on the evidence supporting the impact of lifestyle on target chronic conditions, but also to be able to work with patients to help them make and sustain changes. They need to be able to understand and address patients’ beliefs, stresses, support systems, and community resources; assess readiness to change; establish effective relationships with patients; and collaborate with them over time during the successes and challenges of sustaining a lifestyle change. 9
The medical community needs to send a loud, clear message about the impact of lifestyle on health, particularly in the time of COVID-19. Two messages are particularly important. The first is that chronic disease does not necessarily have to be an inexorable progression of disease severity, complications, and morbidity. There is copious literature demonstrating that lifestyle medicine programs, such as the Complete Health Improvement Program, 11 the Barnard Program for Reversing Diabetes, 12 the Ornish Reversal Program, 13 and Esselstyn’s program to prevent and reverse heart disease, 14 can not only prevent the onset of disease, but also slow progression and even reverse established disease.
The second is that major lifestyle changes improve health rapidly. Tobacco cessation improves blood pressure and circulation within days and improves lung function within 6 weeks. 15 Adopting a low-fat, whole-food, plant-based diet leads to clinically significant reductions in blood pressure, weight, cholesterol, and fasting blood glucose within 2 weeks. 16 Daily aerobic activity can improve mood in less than 2 weeks, 17 and instituting a regular exercise regimen, such as jogging 2 miles or riding a bicycle for 45 minutes, can lower blood pressure within 4 weeks. 18
It is true that, as our defense against the coronavirus improves, one or more levels of the pyramid may become less necessary and may be able to be leapfrogged or collapsed. For example, an effective vaccine will reduce the risk of infection and will decrease the dependence on the top 2 tiers. However, even this will not substitute for a robust effort to address COVID-19 risk through using lifestyle medicine approaches.
For one thing, vaccines are not likely to be 100% effective. The stronger the host’s immune system, the more likely there will be an appropriate response to the vaccine and it will be protective. Those who get infected despite being vaccinated will be better able to avoid complications if they have fewer comorbidities or less severe ones. Additionally, not everyone will be vaccinated. Those who cannot or will not get the vaccine will be dependent on their baseline health to reduce morbidity and mortality if they are infected. The primordial prevention level—a state of wellness fostered by healthy habits—will continue to be important because it prevents so many diseases and because it promotes well-being and contentment irrespective of disease prevention.
There has never been a more urgent time to educate the public about the power of lifestyle to rapidly improve health. The timeline for self-care and lifestyle medicine interventions has been telescoped. Diseases that previously led to gradual decrements in health, function, and quality of life can now lead to rapid decline and death when patients with multiple chronic comorbidities are faced with the novel coronavirus. While the scientific community continues to work to find ways to prevent and cure COVID-19 and the public health sector continues to message about risk reduction through limiting opportunities for infection, clinicians must work to alleviate the chronic medical conditions that put our patients at increased risk of death and disability from this disease. Building a foundation on the pillars of lifestyle medicine is a powerful means to that end.
Footnotes
Acknowledgements
The authors would like to thank Robert Franki for his excellent work in preparing the figure for this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Both Susan Friedman and Ted Barnett practice Lifestyle Medicine. All 3 authors are board members of Rochester Lifestyle Medicine Institute, a non-profit organization with a mission to “transform the community and the practice of medicine by empowering patients to take control of their health.”
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.