
Abstract
Lifestyle medicine holds great promise to transform health during the period from preconception to early childhood. Genetic, epigenetic, nutritional, and environmental factors have lifetime impact on the newborn and family. Little is known about the full potential of lifestyle medicine to improve maternal, child, and family health. Additionally, health care providers face limits in time and may have gaps in knowledge, that preclude discussion of the impact lifestyle medicine can the mother, newborn, and family. Greater understanding of the potential impact of lifestyle medicine provides opportunities to identify current deficiencies in care and areas for improvement and highlights the need for further research. This article reviews current evidence supporting the 6 pillars of lifestyle medicine: nutrition, physical activity, sleep, avoiding risky substance use, stress management and social connectedness as applied to maternal child care from preconception to early childhood, examines the current state of practice, and identifies opportunities for both practice change and further research. Rather than view each component of care in isolation, viewing care as a continuum from preconception to childhood can best establish healthy habits and optimize outcomes for the entire family.
‘Effective preconception care affords the opportunity to provide health benefits of equal magnitude to comprehensive prenatal care.”’
Preconception care is “a set of interventions that aim to identify and modify biomedical, behavioral and social risks to the woman’s health or pregnancy outcome through prevention and management.” 1 Effective preconception care affords the opportunity to provide health benefits of equal magnitude to comprehensive prenatal care.
Improved access to and effective provision of preconception care is critical for improving perinatal outcomes. Despite the Healthy People 2000 objective for 60% of primary care physicians to provide age-appropriate preconception care, 2 only 1 in 6 prenatal care physicians provided preconception care to the majority of their patients. 3 Multidisciplinary teams, including lifestyle medicine practitioners, are ideally suited to optimize preconception health.
In 2016, 77% of women who gave birth initiated prenatal care in the first trimester. 4 Given the high rates of utilization, prenatal care may be the only opportunity to address the importance of lifestyle in pregnancy. Although the postpartum period offers numerous opportunities to positively affect health outcomes for the mother, her child, and family, and nearly half of maternal mortality occurs in the postpartum period, 40% of patients fail to complete even 1 postpartum visit. 5 The care provided is often fragmented and does not result in a transition to comprehensive follow up. Increasing the frequency and quality of postpartum visits is a Healthy People 2020 goal. 6
At the time of delivery, the medical team’s focus is early identification and prevention of complications. Recognizing that birth also has a powerful, positive impact on the future health of the infant is a step toward optimizing health and improving long-term outcomes. Bonding is key, and inpatient “rooming in” of mother and baby encourages collaboration by providers to create a positive start. Optimal care involves reviewing the 6 core pillars of lifestyle medicine and helping to meet these needs from the first moments of the child’s life. The message should be “Congratulations, you have given birth to a beautiful baby and we are going to do everything we can to ensure you, your child, and your family have a healthy, successful future.”
Nutrition
Most patients of reproductive age follow the Standard American Diet (SAD), with caloric excess and simultaneous nutritional shortfalls. Addressing patients’ nutritional habits is essential before conception. Male and female fertility are affected by diet: Ovulation improves by transitioning to plant-based protein sources 7 and saturated fat consumption negatively affects both sperm counts and sperm concentration. 8 Greater intake of plant-based foods also provides folate 9 and antioxidants, which improve semen quality in men 10 as well as greater success at in vitro fertilization (IVF) for women. 11
Preparing for a newborn is an opportunity to change eating patterns for the entire family. Maternal diet during pregnancy 12 and breastfeeding 13 affects food preferences of the newborn. Family meals with more fruits and vegetables, fiber and micronutrients 14 expands the food palate and positively influences the child’s future diet. As the infant moves beyond exclusive breastfeeding and as complementary foods are introduced at age 4 to 6 months, choosing a variety of healthy foods which expands beyond traditional manufactured bottled foods introduces a wide array of tastes and textures to the early palate. Exposure to new foods often needs to be repeated many times before the infant accepts them. Initial exposure to nonbitter vegetables like cauliflower may be sufficient to encourage intake, whereas bitter vegetables like brussels sprouts can be paired with foods the infant already likes to encourage intake. 15 Lifelong patterns are established early, and healthy eating is encouraged through scheduled family mealtimes and positive parental role modeling in food choice.
The Dietary Guidelines for Americans for 2015-2020 promote some of the whole food plant-based (WFPB) concepts. Key recommendations encourage 16
healthy eating patterns across the life span;
increased variety and nutrient density of foods;
limiting calories from sugar, salt, and fat;
alternating usual foods to make healthier choices; and
supporting healthy eating at home, school, and work: everyone has a role.
The US Department of Agriculture Guidelines were developed for clinicians, but MyPlate was created to show patients how these guidelines can be implemented. Many of the recommendations are congruent with a WFPB diet, which encourages a wide variety of fruits and vegetables, whole grains, and a variety of plant-based protein sources such as vegetables, nuts, legumes and seeds.
The American College of Lifestyle Medicine ( ACLM) has a WFPB Plates for children (Figure 1) and adults (Figure 2) to simplify choices and illustrate plant-based options to encourage healthy food variety. Knowledge about foods and skills regarding cooking and food preparation are needed to encourage healthy habits. Community referrals such as cooking classes, nutritionists, dietitians and WIC (Women, Infants, Children) visits can foster healthy habits. Strong community advocacy helps ensure widespread access to healthy foods to build healthy communities, school lunch programs, and workplace environments.
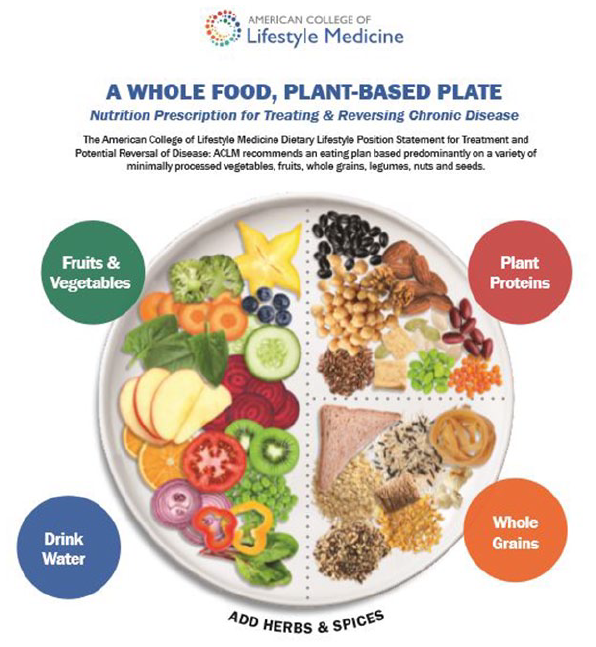
ACLM Whole Food Plant Based Plate for Adults.
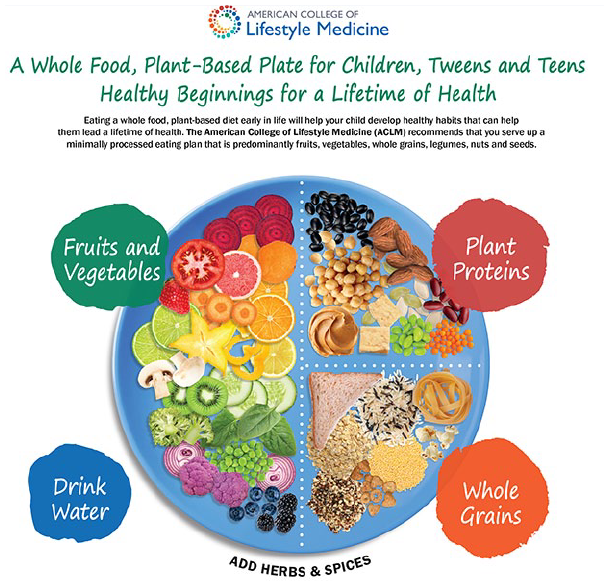
ACLM Whole Foods Plant Based Plate for Children, Tweens and Teens.
Prenatal and postpartum patients are often told to follow MyPlate, Mediterranean, and DASH (Dietary Approaches to Stop Hypertension) diets, but a WFPB diet is appropriate. The Academy of Nutrition and Dietetics states that carefully planned vegetarian diets are appropriate in pregnancy and lactation. When following a WFPB diet, patients need education to ensure adequate consumption of vitamin B12 as it is important for neonatal and fetal neurocognitive development. 17 Most pregnant women do not have adequate dietary intake of omega-3 fatty acids important for development of baby’s brain, eyes, and central nervous system 18 such as docosahexaenoic acid (DHA). Women consuming a WFPB diet seeking alternatives to traditional recommendations such as fish and eggs, should know that alternative sources such as algal oil show great promise. 19 Expectant mothers will be happy to know that neonates born to vegetarians are well within birth weight norms for gestational age. 20
Potential nutritional shortfalls during pregnancy may also include folic acid, iron, calcium, and fiber. Two-thirds of women of childbearing age do not consume enough folic acid, and supplementation prior to conception should be encouraged. 21 Adequate iron stores are critical for the expanded maternal blood supply, the developing fetus, and to replace blood loss at delivery. In published dietary guidelines, pregnant women are encouraged to consume heme iron from animal foods such as red meat, poultry, and fish, due to higher absorption, and take oral iron supplements. 22 Further research is needed on the adequacy of nonheme plant-based sources in pregnant patients with iron-deficiency anemia.
Calcium is needed for both maternal and fetal development. Dairy and meat sources are commonly recommended as the “best sources of calcium” along with oral tablet supplementation. Plant-based sources are often mentioned as an alternative only for those having trouble digesting milk products. 22 Further research is needed to establish plant-based whole food sources as the primary source of calcium in pregnancy.
Ninety-seven percent of women do not consume the recommended 25 g of daily fiber, even though fiber is a factor indicated for the primary prevention for stroke, a leading cause of perinatal mortality. WFPB diets are high in fiber, which improves glycemic control and may also prevent preeclampsia. 23
Two-thirds of women are overweight or obese at the time of pregnancy, increasing obstetric risks. 24 Even modest reductions in weight prior to conception may have a beneficial effect on perinatal outcome. 25 Women are much more likely to be able to return to their prepregnancy weight if they remain within the Institute of Medicine (IOM) weight gain guidelines. During pregnancy, weight loss is not advised but counseling concerning appropriate weight gain is advisable. The goal should be to develop lasting habits to maintain a healthy weight. 26
Screening for and treating undiagnosed diabetes decreases the risk of fetal developmental defects and intrapartum complications. Preconception glycemic control among women with pre-gestational diabetes reduces the risk of congenital anomalies. 27 Postpartum counseling is critical as women have a 30% to 70% chance of recurrent gestational diabetes and 50% of patients with gestational diabetes develop type 2 diabetes within 5 years. 28 Intensive lifestyle intervention in the Diabetes Prevention Program showed a 35% decrease in the onset of type 2 diabetes among gestational diabetics, 29 and could prevent one-sixth of all female diabetics. 30 Women diagnosed with gestational diabetes should be screened with an oral glucose tolerance test 4 to 12 weeks postpartum, followed by annual screening. Despite this recommendation, less than half receive any postpartum screening. 31
After birth, breastfeeding helps the newborn establish a healthy microbiome 32 while helping the mother return to a healthy weight. Through skin to skin contact, breastfeeding promotes bonding and positive feeding practices as well as increased responsiveness of mothers to infant cues. 33 Breast milk uniquely provides vital nutrients and reduces the risk of many diseases such as ear and respiratory infections, asthma, obesity, diabetes mellitus, and childhood leukemia. For mothers, breastfeeding decreases the risk of type 2 diabetes, and breast and ovarian cancer. 34 Breastfeeding may optimize neurodevelopmental outcomes and prevent depression, anxiety, and somatic complaints. 35
The American Academy of Pediatrics recommends exclusive breastfeeding for 6 months with continuation for 1 year or longer, yet at least one-third of mothers in the United States may experience barriers to initiate breastfeeding. Of those who do, 1 in 5 will stop nursing by 1 month, and two-thirds will discontinue by 6 months. 28 Health care providers should initiate a discussion of the benefits of lactation at preconception visits and ensure that mothers considering breastfeeding are fully supported and educated during prenatal care as well as after delivery. Follow-up by a lactation consultant and continued advocacy of breastfeeding by the pediatric provider can support and increase the length of breastfeeding. The WHO (World Health Organization) recommends support for exclusive breastfeeding via baby-friendly hospital initiatives and customized community-based strategies such as peer to peer support and group counseling. 36 The American College of Obstetricians and Gynecologists’ (ACOG) “Physician Conversation Guide on Support for Breastfeeding” encourages postpartum discussion, engaging the mother’s partner and family to provide maternal support. 37 It truly takes a village to optimally raise and support a child and family.
Physical Activity
Women planning to conceive should exercise 30 minutes or more at least 5 days a week. Once pregnant, women should continue this exercise, yet only 15% do. Moderate-intensity exercise during pregnancy does not increase the risk of low birth weight, preterm delivery, or early pregnancy loss. Pregnant women should avoid exercises that involve lying on their back after the first trimester as this could restrict blood flow to the placenta and fetus. They should also avoid sports with high risk of falling or abdominal trauma. 38
After delivery, exercise recommendations should be adjusted if needed for recovery from cesarean section or a complicated vaginal delivery, but most patients can resume moderate intensity activity when they feel able. Postpartum exercise increases a woman’s cardiorespiratory fitness and improves mood, does not impair lactation, and can help her return to her prepregnancy body weight. Maternal exercise may influence her child’s future metabolic and cardiovascular health, including a reduced risk of type 2 diabetes. 39
For the infant, physical activity should be encouraged in the first year. Parents modeling healthy behaviors with routine physical activity increases children’s physical activity. Sedentary parents encourage sedentary activities, such as TV viewing. 40 Daily TV viewing from birth to 2 years averages 1.2 hours, and parental background TV use discourages movement and parent-child interactions. When discussing media with parents, limits on children’s and parents’ daily screen time and encouraging more interactive play should be stressed. When watching TV, colors, shapes, and other learning points can be pointed out to encourage development. Children between 18 and 24 months should have less than 1 hour of high-quality programs viewed with parents, and from ages 2 to 5, less than 1 hour a day of screen time. 41 Tech-free time during meals and before sleep promotes interaction and movement should be encouraged. Encouraging play increases physical activity, results in increased resilience, and decreases the influence of toxic stress, while encouraging physical and socioemotional development. 42
By 4 to 6 months of age, physical activities such as “tummy time” are routinely recommended. 43 Toys that encourage jumping and weight bearing can be used starting at 4 months if the infant is developmentally on track. Taking infants and toddlers on daily walks develops the senses and calms kids; walks also allow parents to be active while still caring for their child. Playgrounds that include slides and play objects encourage movement and sensory integration. As children approach preschool, 180 minutes of play should be encouraged with at least 60 minutes of energetic play. 44 The Centers for Disease Control and Prevention (CDC) released guidelines recommending physical activity throughout the day with caretakers engaged in active play with preschoolers aged 3 to 5 years. 45
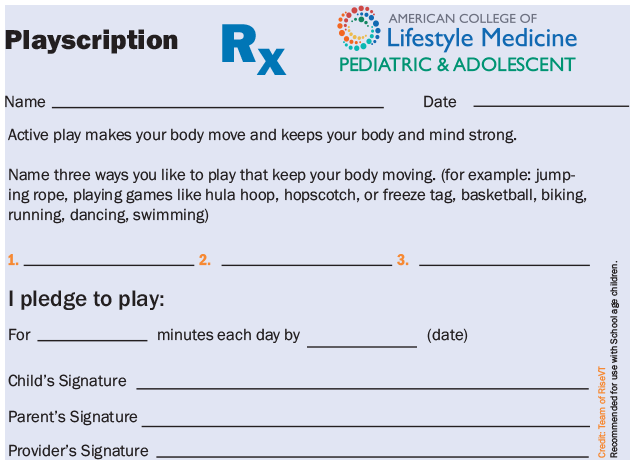
A play prescription, originally recommended by the American Academy of Pediatrics to encourage early childhood development, may also encourage regular play. 42 A “Playscription” was first developed by the RiseVT campaign and adopted by ACLM and can be (Figure 3) given at well-child visits to encourage regular play. Mentioning specific indoor or outdoor activities that are accessible and affordable will help the family get started. Families and health care providers can engage in community initiatives. Advocating for sidewalks, open use school playgrounds, and community centers benefits everyone and leads to increased movement opportunities for lifelong health. 46
Avoiding Risky Substance Use
About 17.5% of women of childbearing age smoke regularly, and 12.5% are frequent drinkers. 47 Smoke-free vaping has risen recently with up to 7% of patients vaping during pregnancy. 48 Patients often enter with or initiate use of prescription and nonprescription substances during pregnancy and postpartum, and providers must recognize and screen for these risks. It is important to recognize the myriad of reasons for substance use, including established addiction, stress relief, and social connection. Exploring the root cause can direct counseling toward education about self-harm, potential harm to offspring, and stress management techniques.
The effects of smoking in pregnancy are significant. Up to 8% of preterm deliveries, 19% of term low birth weight, 34% of cases of sudden infant death syndrome, and 7% of preterm-related infant deaths 49 as well as developmental defects such as orofacial clefts and congenital heart disease are attributable to smoking.50-52 Second- and third-hand smoke exposure during infancy increases the risks of bronchitis, pneumonia, and other respiratory and ear infections. 53
Maternal use of alcohol has a wide range of effects, including dysmorphic facial features, height restriction, microcephaly, birth defects of vital organs, and issues with memory, cognition, behavior, and learning disabilities, 54 summarized as fetal alcohol spectrum disorders. Without preconception interventions, alcohol use would affect approximately 577 000 births per year. 1 There is no acceptable lower limit for alcohol use in pregnancy; less than 1 drink per week in pregnancy has been associated with later behavior problems in girls. 55
Pregnancy is a time of increased motivation; ideally, initiation of screening, counseling, and referral during the preconception period with follow up at subsequent visits will empower abstinence. Almost 25% of pregnant women who used tobacco quit during pregnancy, and preterm birth is reduced the earlier the mother quits tobacco use. 56 Because two-thirds of smokers relapse during pregnancy or postpartum, 28 providers should continue screening even if patients had reported quitting.
A brief counseling session performed by trained health care providers is effective with pregnant or postpartum women who smoke, consume alcohol, or use other substances. The 5 As (Ask, Advise, Assess, Assist, and Arrange) are appropriate for use during routine prenatal office visits. Motivational interviewing techniques can be employed successfully by (1) acknowledging the provider and the parent’s interest in the infant’s health, (2) avoiding placing blame or evoking guilt, (3) asking the parent to offer a plan for behavioral change (eg, an agreement to ban any smoking indoors or in vehicles), (4) referring the parent/family to additional resources (state Quitline, information on nicotine replacement products, their primary care provider), and (5) revisiting the topic at the next scheduled visit or sooner by telephone or other type of brief visit.
As substances of abuse and their metabolites may pass into breast milk, breastfeeding is often contraindicated. In addition to direct effects on the neonate, mothers under the influence may have altered judgment and emotional effects that could interfere with neonatal care. Therapeutic drugs have varying levels of evidence to determine their safety during breastfeeding. The Drugs and Lactation Database, LactMed, is a comprehensive resource for drug selection and suggestions for alternative medications. 57
Preventative screening at all well-child visits includes asking about environmental exposure to smoke. The provider needs to ask about all caregivers including partners, other family members, visitors, and daycare providers. Remind parents that even those who smoke in another room, in the car, or only when the child is away still expose the child to the negative effects of smoke.
For pediatricians, broaching the subject of substance use screening for the parent when the infant/child is their patient may seem challenging. Rapport established with the family through a warm hand-off from mother’s obstetrics/gynecology provider can assist in this transition. Parents often fear shame, judgment, and legal consequences for themselves and the guardianship of their children if alcohol or drug use is admitted. Even after explaining the nature and limits of confidentiality, many will be reluctant to reveal such habits. Careful attention to the child-parent interaction can help detect concerns. Subtle signs during the visit identified by these observations might be the key to early identification of parental substance use.
As children progress from neonatal and early infancy periods to early childhood, additional concerns arise. Infants begin to imitate behavior before 12 months, progressing to pretend play at 24 months, increased imitation at 3 years, and role-playing activities by age 4. Smoking, or any substance abuse, in the child’s presence can lead to early experimentation and habit development. 58
Sleep
The impact of the quantity and quality of sleep on both fertility and pregnancy outcomes is neither routinely addressed nor well understood. Whether impaired sleep causes infertility or is correlated to a common issue (eg, obesity and sleep apnea) is not understood. 59 Up to one-third of pregnant women suffer from restless leg syndrome which, in addition to the discomforts of pregnancy, can cause significant sleep impairment. 60 Given concerns over pharmaceutical sleep aids in pregnancy, there is a clear need for both further research on the prevalence of disordered sleep in pregnancy, the impact on the mother and fetus, and the potential for nonpharmaceutical treatment of sleep disorders. Current postpartum guidelines recommend a review of sleep habits, including coping strategies for fatigue and sleep deprivation. Family and friends can help alleviate some of the burden by assuming greater responsibility for providing care. 5
Despite the challenges of a newborn, developing strategic sleep routines early in life encourages optimal sleep as kids grow older and may prevent obesity, attention problems, depression, anxiety, and other chronic diseases. For optimal health, the American Academy of Sleep Medicine recommends the following amounts of sleep (including naps) on a regular basis every 24 hours 61 :
Infants 4 to 12 months: 12 to 16 hours
Children 1 to 2 years: 11 to 14 hours
Children 3 to 5 years: 10 to 13 hours
Achieving optimal sleep is challenging if the caretaker does not have healthy sleep patterns. 62 Four key steps to foster adequate sleep are encouraged. First, establish a consistent bedtime routine, which can improve mood, decrease fatigue, and reduce depression while encouraging healthy sleep habits. By 6 months, most infants have established their circadian rhythm and are able to sleep through the night. Routines such as “Brush, Book, Bed” 63 or regularly scheduled bedtimes encourage healthy sleep. When nighttime awakenings occur, caretakers should respond briefly without stimulation to prevent sleep disruption. The second step is to minimize caffeine intake. If children have poor sleep patterns, parents often combat daytime fatigue with caffeine leading to poor parental nighttime sleep. Kids age 2 and up are often exposed to caffeine through soda, coffee, tea, flavored dairy, and sweetened grains, which can encourage arousal and impair sleep. 64
The third step is minimizing light exposure prior to bedtime, including screens, televisions, and ambient light. Dimmed room lights encourage the natural stimulation of melatonin allowing for natural sleep induction. The fourth and final step is having a calm and quiet sleep environment with a comfortable room temperature and reduced noise. White noise may encourage sleep for some infants and toddlers.
Stress Management
Pregnancy and childbirth are inherently times of joy as well as stress for both the mother and family, with potential for lasting implications. Looking at health care providers’ ability to identify and treat stress in a continuum across prenatal and pediatric visits offers the best opportunity to create a lifelong impact.
Depression, trauma, and even physical abuse are common in the perinatal period, and 10% of women postpartum meet criteria for major depressive disorder. 65 The incidence of physical abuse during pregnancy and the postpartum period is estimated to be 20%. 28 The birth experience itself is viewed by some as trauma, and up to 16% of patients experience posttraumatic stress disorder in the postpartum period. 5 In addition, up to 50% of fathers meet criteria for depression when the mother experiences postpartum depression. 66
Early identification of these concerns with the use of validated screening tools is an important part of perinatal and well-child visits. Brief screening instruments, such as the 4-item Hurt Insulted Threatened or Screamed at (HITS), the 3-item Partner Violence Screen (PVS), and a 3-item Abuse Assessment Screen (AAS), can be effectively used to screen, intervene, and refer patients at risk or encountering physical abuse. 28 The Edinburgh Postnatal Depression Scale (EPDS) has been validated for perinatal use and even for screening fathers for depression. 66
Seventy-two percent of women reported discussing perinatal depression with their prenatal care provider. 67 Screening alone can offer some limited benefit, but optimal care includes initiation of treatment and referral. 65 National Institute for Health guidelines recommend screening all women for resolution of the “Baby Blues” 10 to 14 days after birth to facilitate early identification of and treatment for postpartum depression as psychosocial support for pregnant and postpartum women decreases depressive symptoms. 65
The newborn to infancy period is critical as physical, emotional, and social factors affect present and future health. However, given the difficulty of assessment of long-term effects of stress, it is often overlooked. Exposure to high levels of stress in early childhood, particularly adverse childhood experiences (ACEs) have been linked to chronic disease, including heart disease, cancer, asthma, heightened risk of infection, depression, as well as later behavioral problems and decision making in adulthood.68,69 Early recognition of these stressors, and targeted intervention has the potential to prevent significant disease later in life.
Reviewing the history of the mother is the beginning of the newborn’s history. Asking about family structure and stability, respite for parents, and community support helps identify potential sources of stress. Screening for social determinants of health will provide additional structure to a newborn care plan. Barriers, including health, finance, insurance, and transportation may affect parents’ compliance for well child visits and consequently routine vaccinations. Referral to care team members, including a social worker, addresses some of these concerns. Red flags should prompt further questioning focused on the safety of the child: unsafe sleeping positions, possible parental substance use, concerns for shaken baby/physical abuse, and other forms of neglect.
Recognizing that some level of environmental stress is universal, we are better poised to approach well-child visits in infancy and early childhood with the goal of supporting parents and providing children the tools to develop resiliency. The 7 Cs of resilience (competence, confidence, connectedness, character, contribution, coping, and control) are skills that can be discussed throughout early childhood wellness visits. 70 Early infancy conversations should be centered around establishing effective routines that provide comfort for the infant and structure for parents. These patterns serve the family well and create a sense of safety for the growing child. Providing anticipatory guidance on developmental stages and effective limit setting provides the foundation for discipline needed in all aspects of their health.
Social Connectedness
Little research exists on the impact of social connectedness on pregnancy outcomes. One promising study enrolled patients with poor psychosocial health markers into group prenatal visits via the Centering Pregnancy program, and compared their outcomes with patients in routine prenatal care. The Centering Pregnancy program allows for more frequent, patient-led group prenatal visits; participating patients report an improved social support. At 4 months postpartum, by addressing the need for connection during a time of increased psychosocial stress, Centering Pregnancy participants were more likely to have improved psychosocial health. 71 Additional research is needed to more fully determine the impact of stress and connectedness on pregnancy outcomes, as well as health care providers’ ability to effectively address this pillar of lifestyle medicine before, during, and after pregnancy.
The most important aspect of the first few days after birth is allowing the child to bond with parents and reducing the mother’s stress. The infant develops its earliest relationships with immediate caregivers: learning to recognize scent, voice, and appearance. Infant and mother, indeed, have a connection that precedes birth. Rooming in and early initiation of breastfeeding can promote child-mother bonding. 72 In time, the infant will learn to distinguish immediate family as well by voice and facial recognition. Encouraging family and friends’ involvement in infant’s care allows those relationships to develop and provides support throughout childhood. Establishing the importance of social connection early on is key to the success of families.
Interactions with older siblings and peers at childcare or preschool provides further space for interaction and modeling. Children will model peers and follow cues based on their environment. These early relationships teach children important skills such as self-regulation, turn-taking, and early conflict resolution.
Encouraging parents to provide a safe space for their toddler to develop these early relationships will support their behavioral development. As the young child likely spends a significant portion of time at home, it is important to discuss how to model good behavior and healthy relationships. As children watch parents interact with others, they learn the value of trust, respect, and empath needed in their own self-preservation and engagement with their world.
Approaching school-age brings on its own set of unique rewards and challenges. For some, social anxiety and separation from primary caregivers may make this transition difficult. When possible, beginning with shorter periods of separation can help develop a sense of security for children. Establishing a trusting relationship with a child, through mutual respect and a non-judgmental approach, will create a safe space for them in times of confusion or stress. Teaching them about healthy relationships is vital for children to better navigate situations where they might be at danger, including bullying and abuse. A network of close family and friends may serve as valuable mentors in these situations. This in turn helps develop resilience in all aspects of their lives. 73
Summary
As providers, we see care as being delivered to the patient presenting to us, yet our patients often face the challenge of integrating our advice into a complex family dynamic involving the newborn, their partner, and other family members. Families that embrace and reinforce healthy habits are more likely to sustain these changes. Providers benefit from exploring the complexity of family dynamics as well as viewing the transition from preconception visits to delivery and infancy as an opportunity to establish and promote healthy habits for the entire family.
Perinatal care is not without challenges and is often a patchwork of services without the introduction of the key lifestyle medicine practices. In addition, the challenges faced in addressing some of the determinants of adverse childhood experiences (ACEs) scores, drivers of the toxic stress so many of our patients face, are deep rooted and may span generations. Nevertheless, interventions such as the Centering Pregnancy program hold promise for the most vulnerable patients. Practitioners benefit from understanding lifestyle medicine interventions such as improving nutrition, sleep hygiene, physical activity, stress management, and building social networks. Many intervention programs are readily available, often inexpensive, and would be utilized more with discussion and referral each visit. In addition, broadening the scope of screening to the entire family could improve outcomes not only for patients but for the family and the population as a whole.
Further research regarding the impact of lifestyle medicine on perinatal outcomes is warranted including the impact of lifestyle changes on epigenetic “imprinting” of the newborn. As most lifestyle medicine interventions do not translate into profitable products, private sector funding may be negligible. Publicly funded research is required, yet overall public funding for major research is limited, and rarely focused on either maternal child health or such subjective interventions as sleep, exercise, and nutrition.
In closing, we encourage maternal and child health practitioners to continue learning, applying, and questioning current standards of care, and to work toward integration of the 6 pillars of lifestyle medicine into perinatal care. Integrating healthy habits into the daily life of the entire family can optimize health for all.
Footnotes
Authors’ Note
Portions of this information were presented at Lifestyle Medicine 2019: The Foundations of Health Care in Orlando, Florida, October 27-30, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.