
Abstract
Background. There is a notable lack of education on nutrition and physical activity guidelines in medical schools and postgraduate training. The purpose of this study is to assess the nutrition and exercise knowledge and personal health behaviors of physicians in the Department of Medicine at a large academic center. Methods. We conducted a survey study in the Department of Medicine at the University of Florida in 2018. The survey instrument included questions on demographics, medical comorbidities, baseline perception of health and fitness, and knowledge of nutrition concepts. The Duke Activity Status Index assessed activity/functional capacity and the validated 14-point Mediterranean Diet Survey evaluated dietary preferences. Data were analyzed using descriptive statistics and the χ2 test was used to perform comparisons between groups. Statistical significance was determined at P < .05. Results. Out of 331 eligible physicians, 303 (92%) participated in the study. While all respondents agreed that eating well is important for health, less than a fourth followed facets of a plant-based Mediterranean diet. Only 25% correctly identified the American Heart Association recommended number of fruit and vegetable servings per day and fewer still (20%) were aware of the recommended daily added sugar limit for adults. Forty-six percent knew the American Heart Association physical activity recommendations and 52% reported more than 3 hours of personal weekly exercise. Reported fruit and vegetable consumption correlated with perceived level of importance of nutrition as well as nutrition knowledge. Forty percent of physicians (102/253) who considered nutrition at least somewhat important reported a minimum of 2 vegetable and 3 fruit servings per day, compared with 7% (3/44) of those who considered nutrition less important (“neutral,” “not important,” or “important, but I don’t have the time to focus on it right now”; P < .0001). Conclusions. This study highlights the need for significant improvement in education of physicians about nutrition and physical activity and need for physicians to focus on good personal health behaviors, which may potentially improve with better education.
Keywords
‘Studies show that HCPs [health care professionals] who engage in healthy behaviors are more likely to promote these behaviors and are perceived as more credible and motivating to their patients.’
Background
Declines in mortality rate for coronary heart disease (CHD) have occurred, in large part, due to advances in prevention of risk factors through pharmacotherapies and lifestyle modifications.1,2 Diabetes, hypertension, hyperlipidemia, sedentary lifestyle, and obesity are risk factors associated with increased CHD and mortality. Obesity and overweight rates, which contribute to many risk factors, reached 70% in the United States by 2013. 3 Poor diet quality is considered the top cause of premature mortality in the United States. 4 While plant-based and Mediterranean-style diets, abundant in whole grains, fruits, vegetables, legumes, nuts, and seeds, seem to be effective for primary prevention of major chronic diseases, 5 consumption of processed foods, high in added sodium and refined sugars, has increased.6-8 Despite recommendations for 5 to 7 daily fruit and vegetable servings, the average American only eats 0.6 cups of fruit and 0.8 cups of vegetables per day per 1000 calories consumed. 9 Similarly, the new 2018 Physical Activity Guideline for Americans recommends up to 300 minutes of moderate intensity exercise performed weekly in any increment, plus muscle strengthening and balance training for older adults, including in those with chronic diseases 10 and only 26% of men and 19% of women have met 2008 recommendations by the Department of Health and Human Services for aerobic and muscle strengthening exercise. 10
Health care professionals (HCPs) can be powerful motivators to enhance dietary and physical activity (PA) habits of their patients. Patients perceive HCPs as respected sources of health-related information and “very credible” sources of nutrition facts.11-13 HCPs’ lifestyle advice to their patients is associated with behavior changes that can lead to decline in the incidence and progression rate of various diseases. 14 However, doctors usually miss the opportunity to provide lifestyle advice to patients.15,16 In one study, 4% of cardiologists reported not discussing nutrition and 58% reported spending less than 3 minutes per visit counseling on nutrition in their physician-patient visits. 17 Interestingly, in another study of female physicians, nutrition and weight loss were emphasized more where 43% of female physicians counseled their patients on nutrition and 50% counseled their patients on weight loss. 18
Despite the lack of counseling of patients, HCPs and medical students, in general, feel that they are healthy.19-22 In a Canadian study from 2009, physicians felt that they were generally in good to excellent health (90%) and exercised on average for 4.7 hours per week, which averages to 56 minutes per day. 23 This is significantly higher than the general public where less than 5% of Americans exercise 30 minutes or more per day. 24 In another study, medical students were noted to be more commonly vegetarian. Interestingly, that eating practice declined throughout medical school. 25 Proper nutrition and PA are important components of physician wellness. 26 Poor nutrition can affect HCPs’ physical, emotional, and cognitive functioning 27 and improving physician nutrition is associated with enhanced cognitive testing results. 28 HCPs’ regular PA correlates with their career satisfaction, improved sense of well-being, increased empathy, and decreased burnout.29-32
Studies show that HCPs who engage in healthy behaviors are more likely to promote these behaviors and are perceived as more credible and motivating to their patients.33-38 HCPs with healthy habits are also more likely to counsel. 39 Understanding the personal health care regimens of HCPs at a large academic center and their knowledge of optimal lifestyle practices will aid in targeting future education and help us understand the connection between education of HCPs and patient counseling.
Methods
The institutional review board at the University of Florida in Gainesville, Florida approved this survey study. We developed a 50-item electronic survey, using the Qualtrics web-based system (Qualtrics). The survey instrument included questions on demographics, medical comorbidities, baseline perception of personal health and fitness, and knowledge of nutrition concepts (Tables 1 and 2). The bulk of the questions came from 2 validated surveys: the 14-point Mediterranean Diet Survey 40 (Table 3) and the Duke Activity Status Index (DASI) 41 (Table 4), to assess dietary preferences and activity/functional capacity, respectively. There were a few knowledge-based questions and items about physician stress and happiness levels that were also included (Table 2).
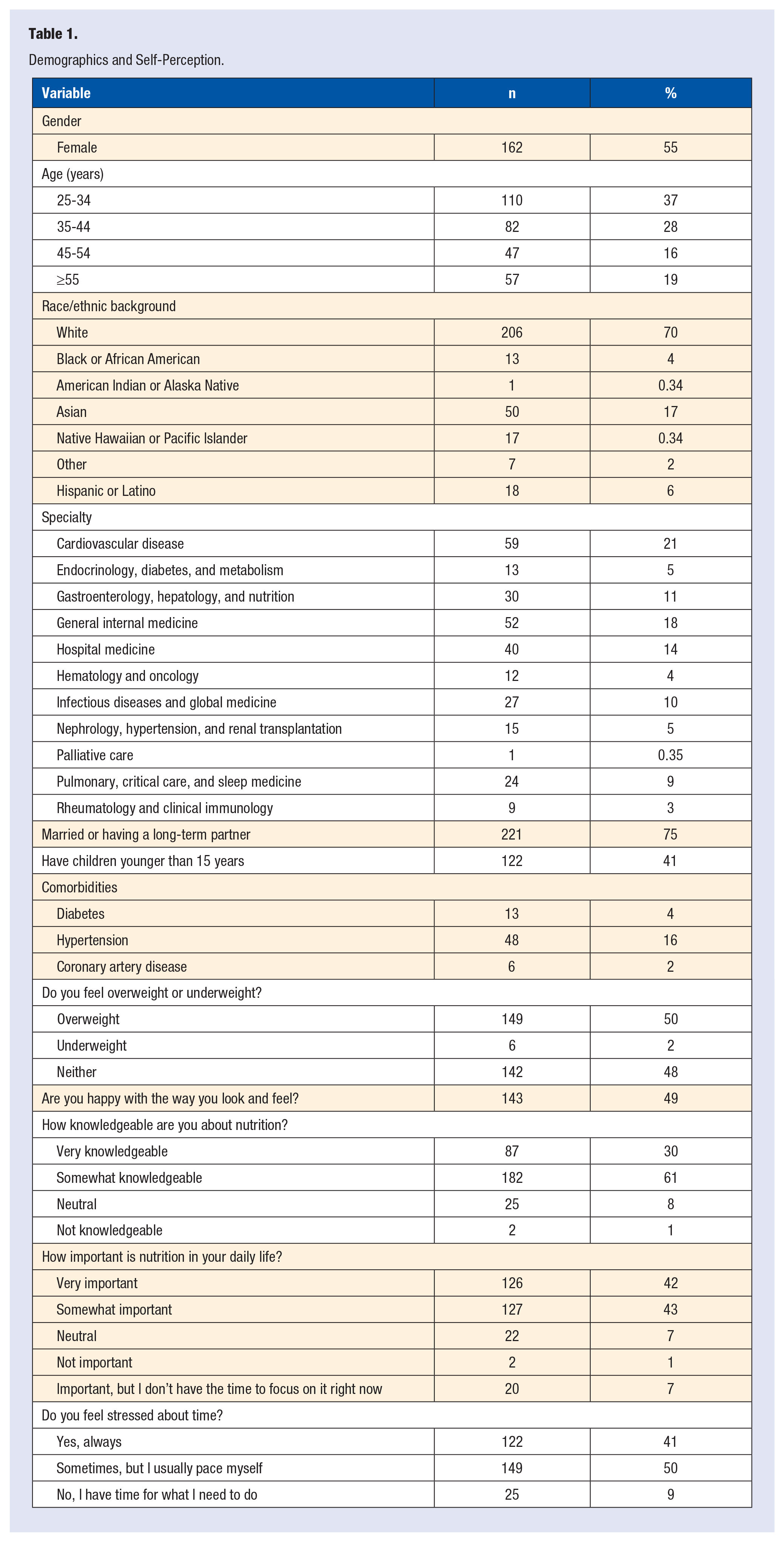
Demographics and Self-Perception.
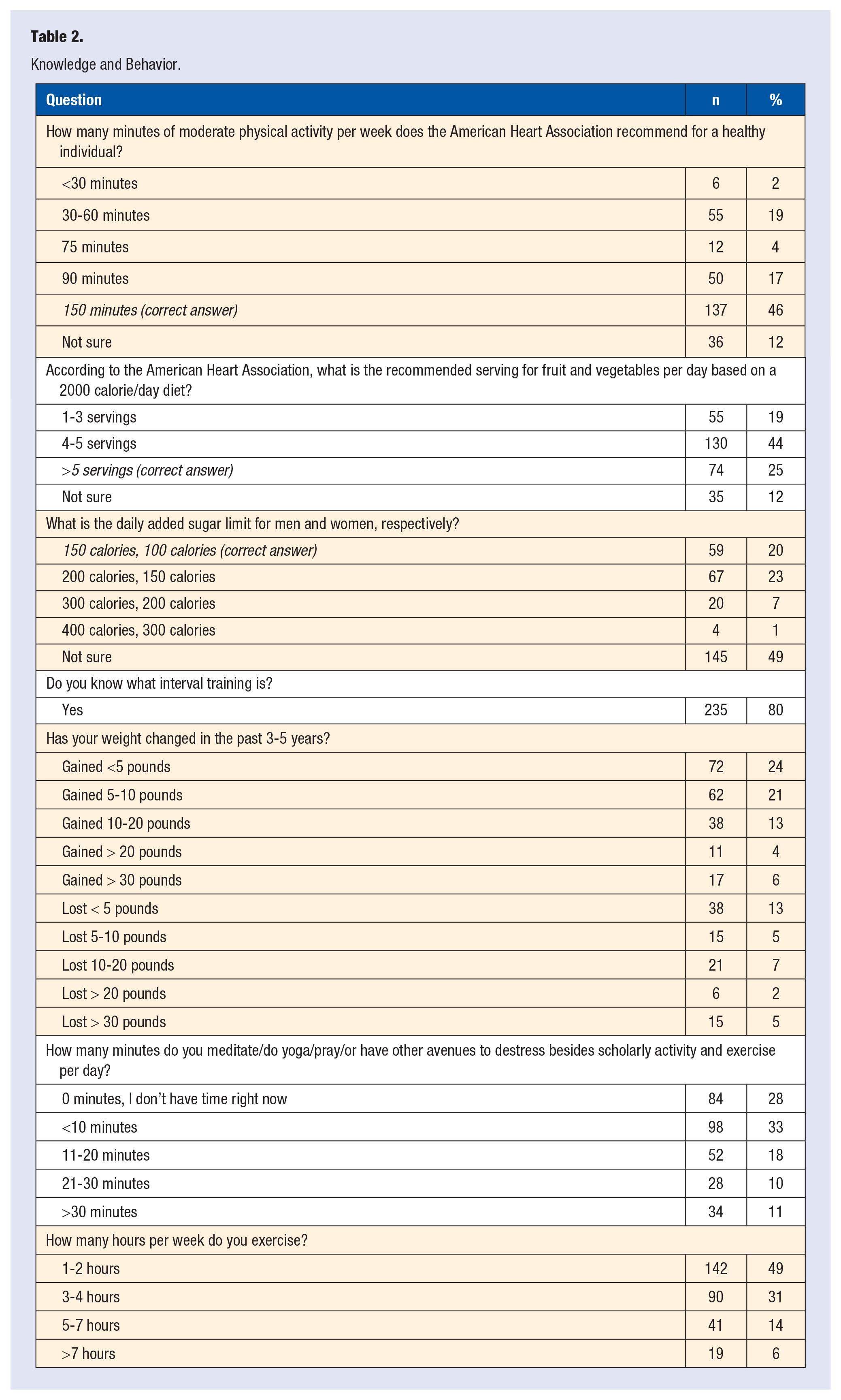
Knowledge and Behavior.
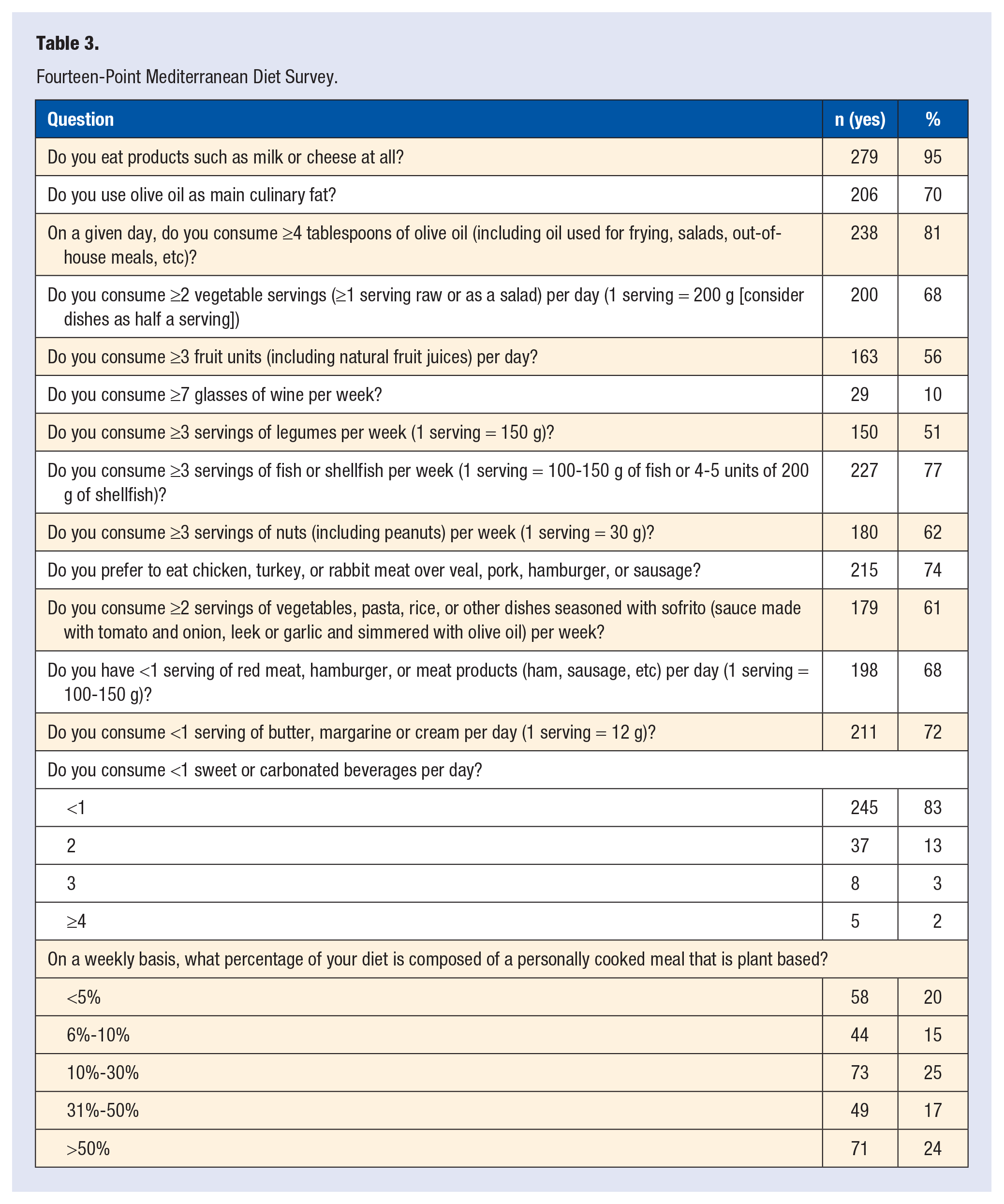
Fourteen-Point Mediterranean Diet Survey.
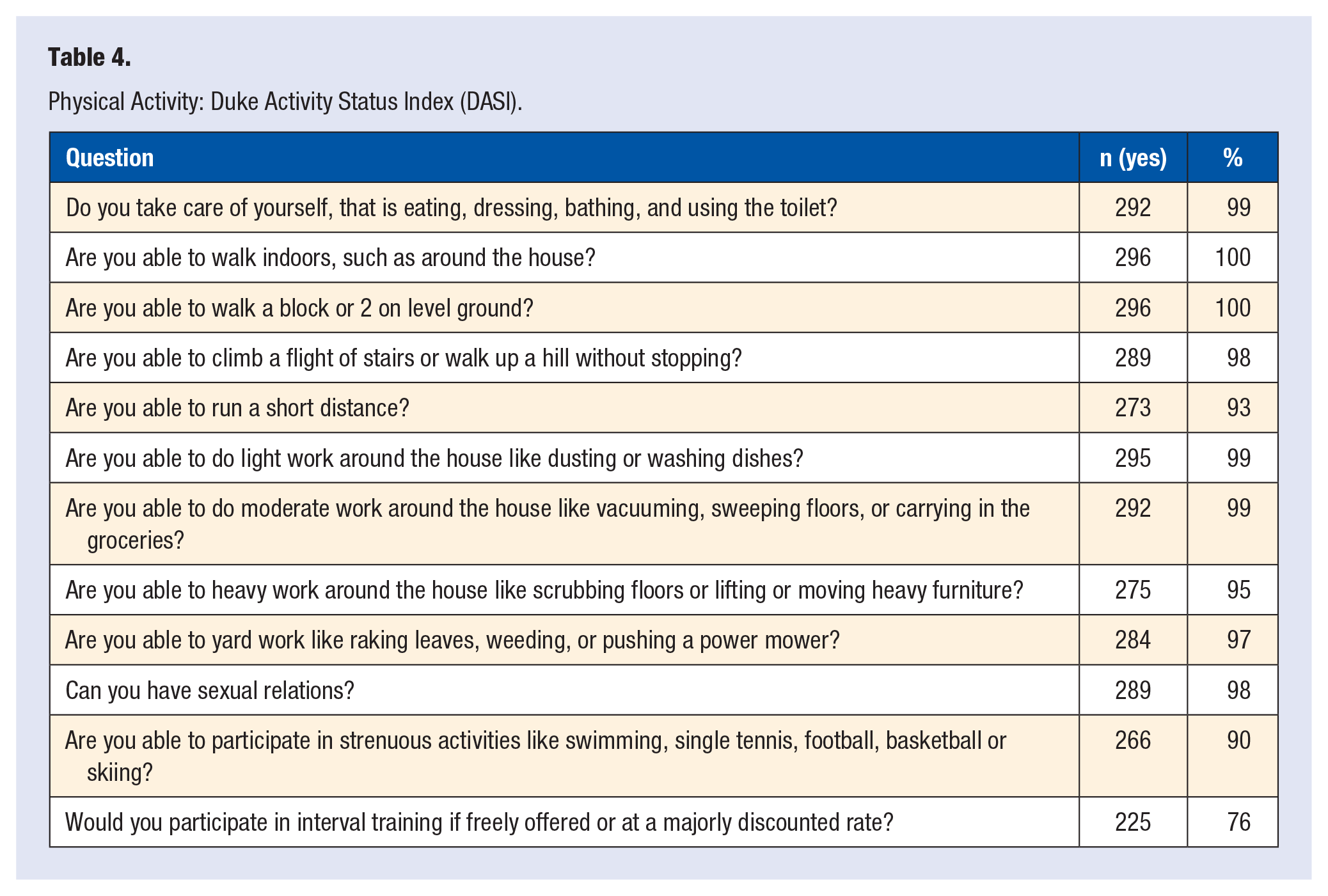
Physical Activity: Duke Activity Status Index (DASI).
An invitation email including the link to the anonymous electronic survey was sent through individual divisions in the Department of Medicine (DOM), followed by a reminder email through an active mailing list for the DOM. The survey was open for 2 weeks in 2018. Data were analyzed using descriptive statistics according to variable type and distribution. Comparisons between groups were analyzed using the χ2 test as appropriate. Statistical significance was determined at P < .05.
Results
Out of 331 eligible physicians, 303 (92%) participated in the study. The number of responses to each survey item ranged from 282 to 297. All participants were from the DOM with a large percentage from divisions of cardiology (21%) and general internal/hospital medicine (32%; Table 1). The majority were women (55%), white (70%), and married (75%).
Dietary Knowledge and Personal Practices
Tables 2 and 3 represent results of responses to knowledge and behavior questions and the validated 14-point Mediterranean Diet survey respectively. While most participants (85%, 253/296) considered nutrition at least somewhat important in their daily life, 77% responded that less than half of their meals are home cooked and plant based (Table 3). The majority reported not consuming at least 3 fruit units per day, 3 legume servings per week, or 3 servings of fish or shellfish per week (Table 3). Sixty-eight percent reported consuming at least 2 daily vegetable servings and 41% at least 3 fruit servings per day (Table 3). Ten percent reported consumption of 7 or more glasses of wine per week (Table 3).
Reported fruit and vegetable consumption correlated with perceived level of importance of nutrition as well as nutrition knowledge. Forty percent of physicians (102/253) who considered nutrition at least somewhat important reported a minimum of 2 vegetable and 3 fruit servings per day, compared with 7% (3/44) of those who considered nutrition less important (“neutral,” “not important,” or “important, but I don’t have the time to focus on it right now”; P < .0001; Figure 1).
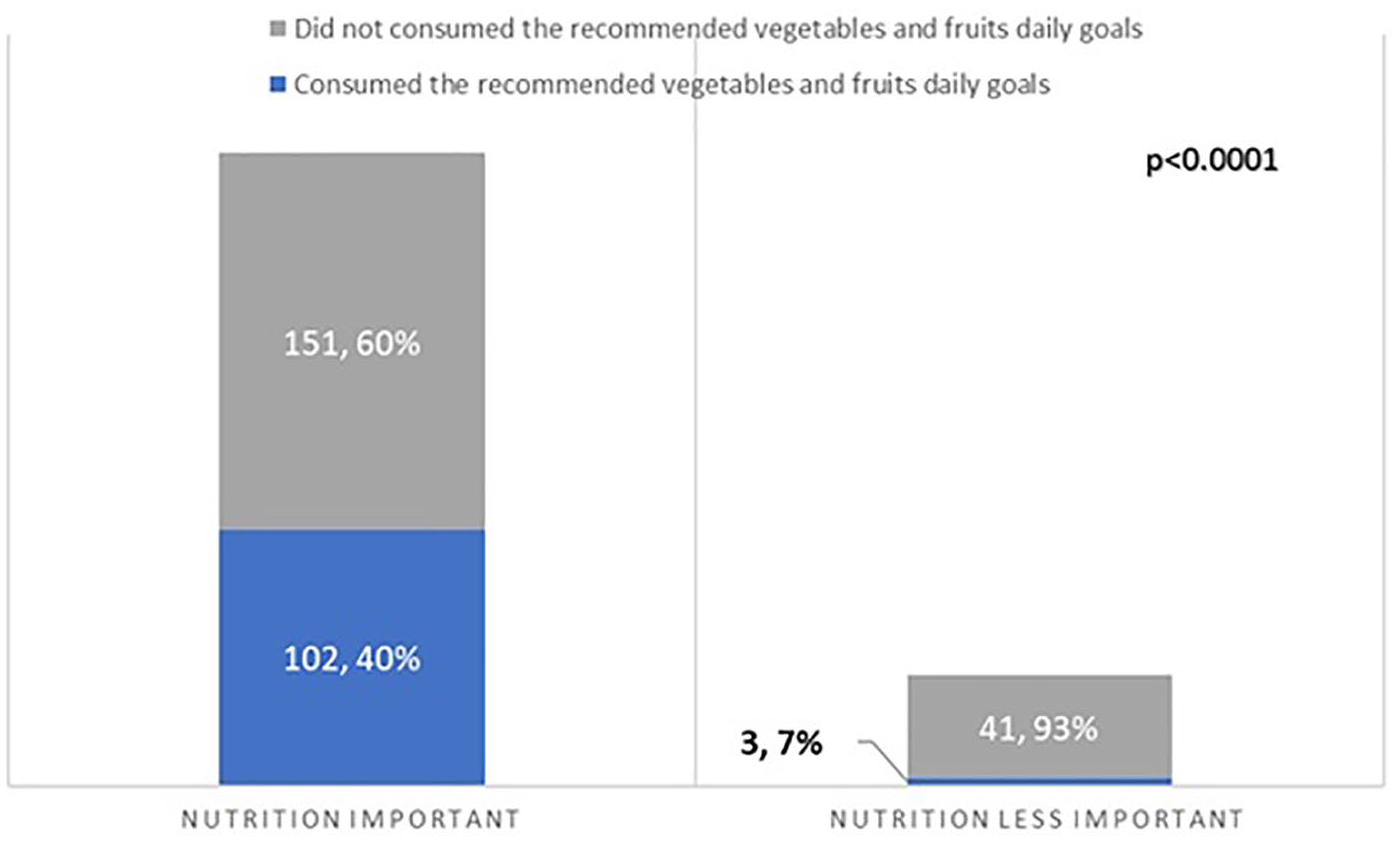
Perceptions of the role of nutrition and personal fruit and vegetable consumption.
Most physicians (91%, 269/296) reported that they were somewhat or very knowledgeable about nutrition (Table 1). However, only 25% of those who felt they were knowledgeable correctly identified the recommended number of fruit and vegetable servings per day per the American Heart Association (AHA) and fewer still (20%) were aware of the recommended daily added sugar limit for men and women. Only 6% (18/297) answered both questions correctly. None of the participants that considered their nutrition knowledge neutral or not knowledgeable answered both questions correctly (P = .3932; Figure 2).
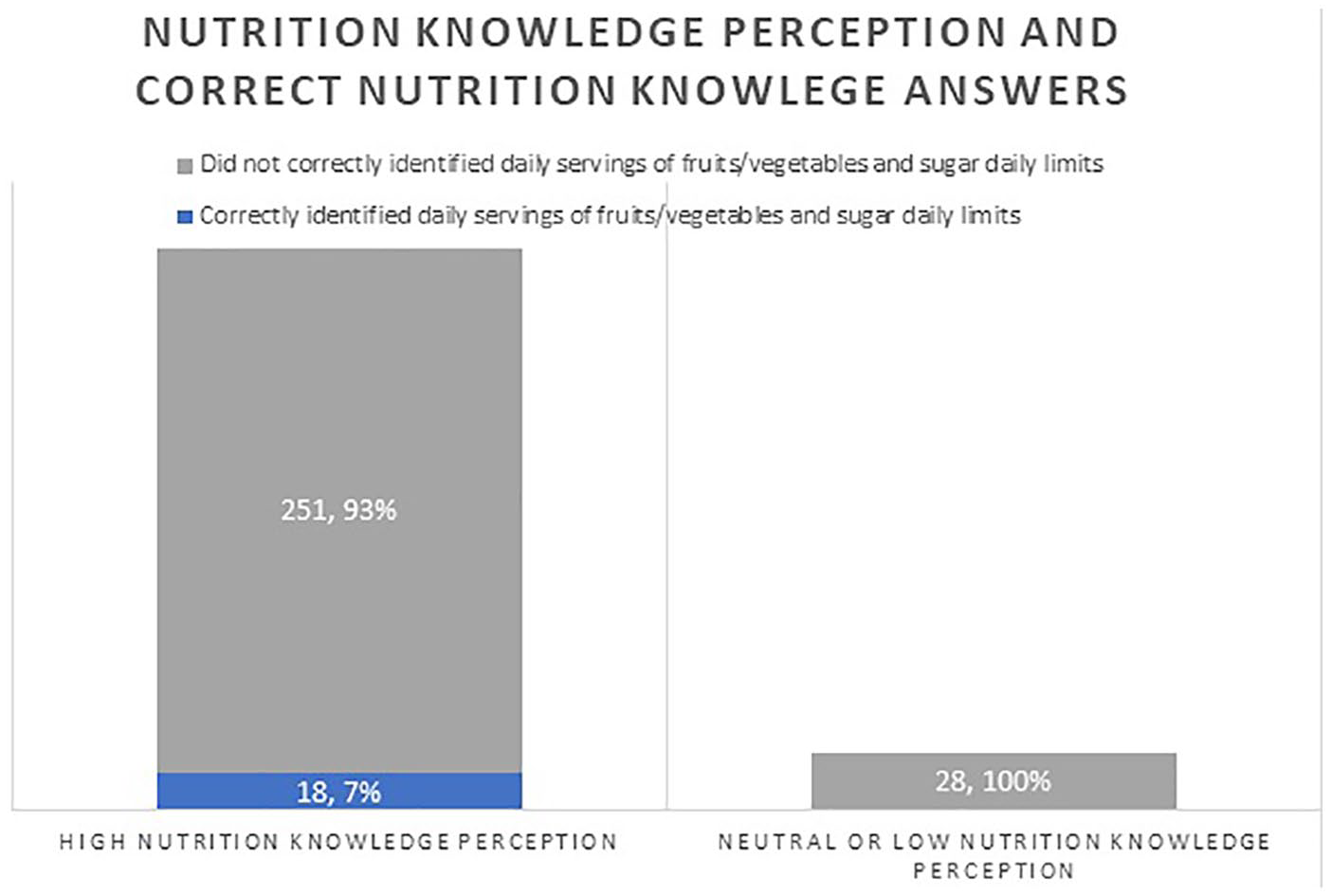
Health care professionals’ perception of nutrition knowledge and accuracy of knowledge-based questions.
Participants who answered both nutrition knowledge questions correctly (11/18, 61%) consumed at least 2 vegetable and 3 fruit servings per day, compared with 34% (94/279) of those who did not answer both questions correctly (P = .023; Figure 3).
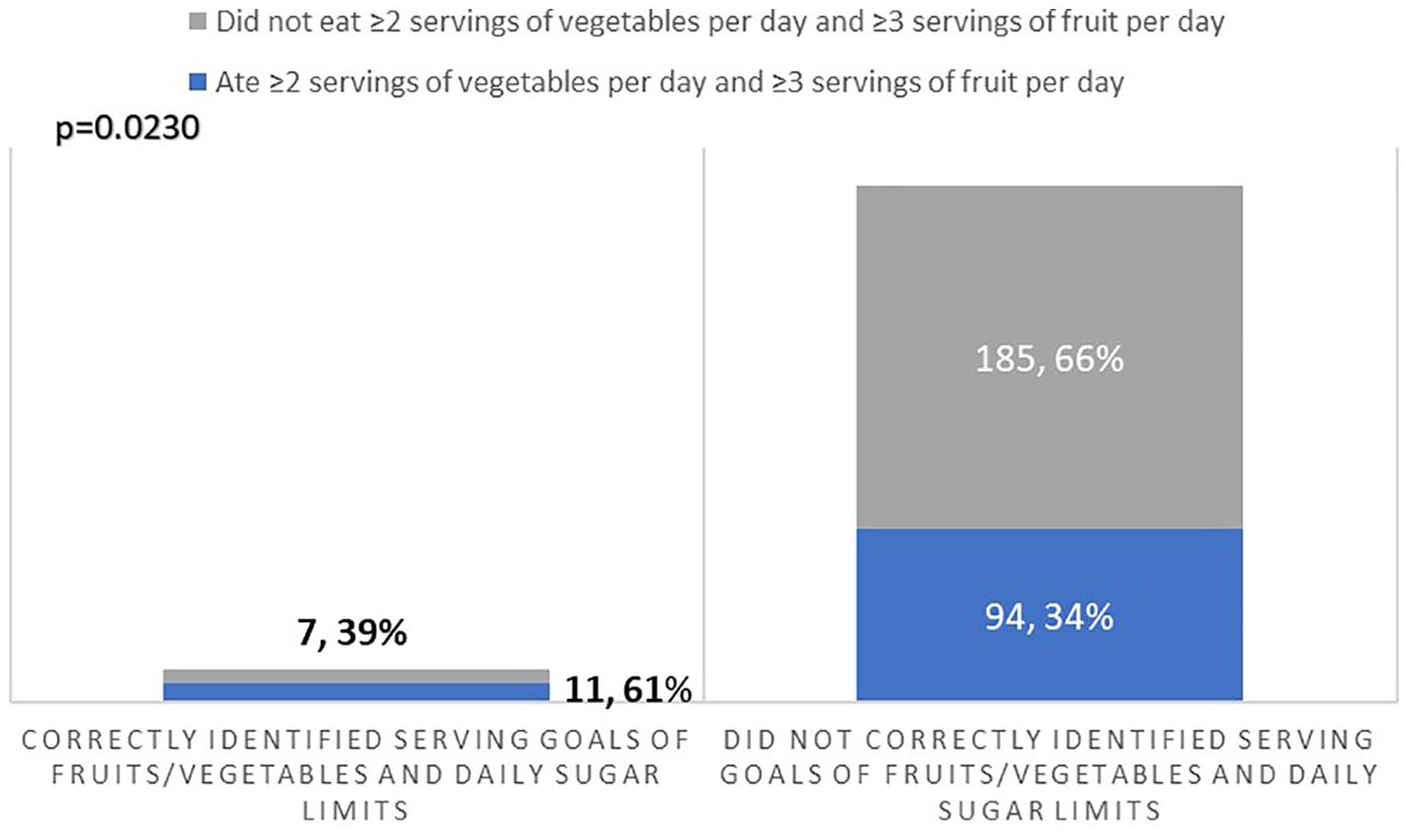
Knowledge of servings of fruits and vegetable goals and personal behavior.
Exercise Knowledge and Personal Practices
Table 4 summarizes the results of responses to the DASI. There were no significant limitations in the respondents’ ability to exercise. The majority of physicians did some level of exercise. However, only 20% of participants reported exercising ≥5 to 7 hours per week (Table 2).
The majority (80%) reported knowing what interval training is. Forty-six percent (137/296) correctly identified the AHA recommendation for 150 minutes of moderate PA per week. Twelve percent were not sure of the AHA physical activity recommendation and the rest (42%) chose a lower target. While not statistically significant, more participants who correctly recognized the exercise goal (57%, 78/137) reported exercising over 3 hours weekly than those who did not identify the exercise goal correctly (48%, 77/160; P = .1298; Figure 4). Only 3.7% (11/296) correctly identified the recommendations for PA, fruit/vegetable servings, and calorie limit from sugar.
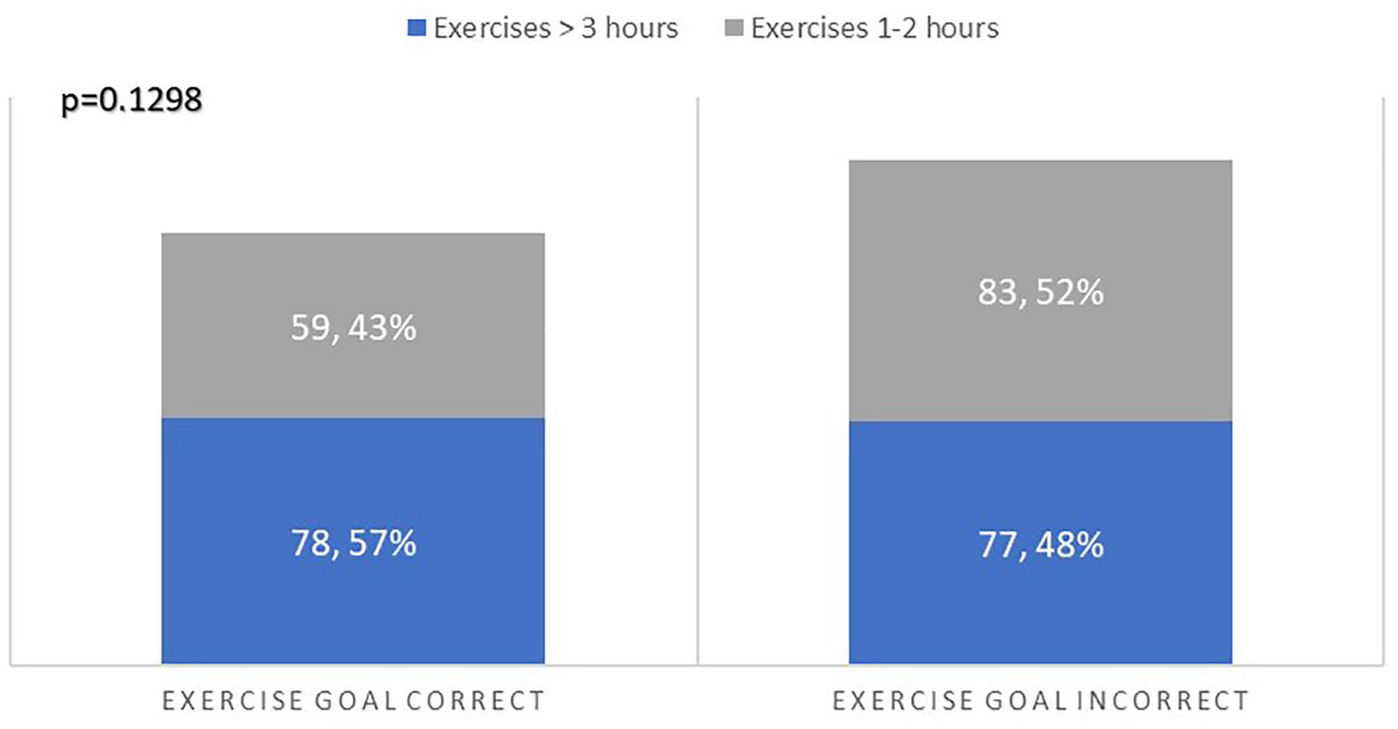
Knowledge of exercise goals and personal behavior.
Physician Self Impression
Most participants did not have diagnosed diabetes, hypertension, or coronary artery disease (Table 1). However, 50% of participants (n = 149) reported feeling overweight. Forty-eight percent (n = 143) reported being happy with the way they looked, corresponding to 78% of participants who reported normal weight (108/139) and 22% (32/148) who reported being overweight. Ninety-one percent of participants reported some level of stress, with 41% of participants reported feeling stress most of the time. Sixty-one percent engaged in no or less than 10 minutes of activity per day to combat stress. Only 11% (n = 34) reported spending more than 30 minutes daily in activities other than scholarly ones and exercise to decrease stress, such as meditation, yoga, or praying.
Discussion
Our results show that HCPs engage in more health promoting behaviors than the general public.9,24 Our study also suggests that physicians do not reach exercise and nutrition standards set out by the AHA.20-22 Insufficient education, knowledge, and training as well as lack of time have been reported as barriers to PA counseling by physicians.42-44 Education of physicians in lifestyle tools is a significant issue where in one study, 59% of cardiologists did not recall nutrition education during their internal medicine training and more than 90% of physicians recall little or no such education in medical school. 17 Other studies report infrequent and inadequate undergraduate and graduate medical education in PA.45-47 A survey of US medical schools found that only 13% of 102 schools included PA and health in the curriculum, and only 6% had a core course or requirement related to exercise. 48 A review of 109 studies found that, in comparison with smoking, nutrition, alcohol, and drug use, PA was the least addressed topic in health behavior counseling curricula for medical trainees. 49 The lack of knowledge of guidelines that we noted in our study, is consistent with other studies as well. A study among general practitioners in the United Kingdom, 80% of the 1013 respondents were unfamiliar with the national PA guidelines. 50 Studies also suggest that the perceived relevance of nutrition education among medical students seem to decrease over their medical school training, which might suggest when initiatives need to be introduced into training. 51 However, studies show that nutrition education in medical school improves counseling related confidence. 52
A number of innovative strategies, both online and in the classroom, have been introduced to reduce the gap in lifestyle education and knowledge. The first nutrition and cooking elective in a medical school was offered at SUNY-Upstate in 2003. The first postgraduate course, Healthy Kitchens Healthy Lives was developed at Harvard in 2007. 53 Brown University has created an elective for years 1 and 2 in the Food & Health curriculum with interactive cooking workshops. The Goldring Center for Culinary Medicine at Tulane University, a dedicated teaching kitchen that offers hands-on training with electives designed for medical students, was developed in 2013. 54 The University of Florida (Gainesville, Florida) offers a nutrition in medicine course for first-year medical students, integrated nutrition content in second year medical school training and a monthly prevention conference that focuses on educating fellows on nutrition and lifestyle. Currently, 10 medical schools offer nutrition courses as electives. 55 Online coursework is also available. Nutrition in Medicine (NIM) is a comprehensive online nutrition curriculum for medical students and practicing physicians, with nearly half of US medical schools utilizing components of the NIM curriculum. 56
Specific physical activity education courses are less well recognized. The Healthy Living Practitioner (HLP) graduate certificate program, a 22-credit interdisciplinary curriculum trademarked by the AHA, was recently proposed to be provided in conjunction with standard training on lifestyle-based practices to supplement standard therapies. The University of Chicago implemented this program in 2017. Other international institutions, such as University of Tasmania in Australia and University of Belgrade in Serbia, are in the process of implementing the program into their curriculum. Students in all health care programs are eligible to participate in the program as an elective. Trademarking by the AHA allows for standardization of education for physicians and is an option that can be considered at organizations around the world with the potential for creating a health care environment capable of providing healthy living medicine. 57 Another education source is a 10-part online course module introduced by the American College of Lifestyle Medicine designed for HCPs that focuses on the role of nutrition, sleep, exercise, and other lifestyle tools and another 10-part online module by NextGenU.org, which is an accredited Lifestyle Medicine course that is available for free and supported by many lifestyle organizations including the European Lifestyle Medicine Organization. 58
One interesting finding from our study were the significant percentages of other unhealthy perception and practices. For example, 51% of respondents felt unhappy with the way they looked, 41% reported feeling stress all of the time, and 10% reported consuming more than 7 glasses of wine per week. While the vast majority of participants reported feeling stress a large percentage of time, less than half devoted at least 10 minutes per day in activities that provide avenues to relieve stress. Conversation about physician burn-out and poor physician self-care is not new and has been noted for decades. 59 Our study shows that despite highlighting these issues in study, there is no trend toward improved physician personal health over time. The implementation of more widespread education of physicians on nutrition and lifestyle and a concrete focus on physician health and stress needs to be emphasized and should start at the institutional level. This has the potential effect of improving physician cognitive and emotional well-being and increasing physician counseling of patients in a “trickle-down” effect from physician wellness. Our study should serve as a “call to action” to make physician education on nutrition and lifestyle and personal well-bring a primary focus in the workplace.
Conclusion
Our study suggests that while many physicians are active and surpass the average nutrition and activity profile for people in the United States, HCPs do not reach national standards for physical activity and healthy eating. This study again highlights the need for improvement in medical education about nutrition and PA. This improvement in education will hopefully increase physicians’ focus on their own health promoting behaviors and arm physicians with tools to then provide lifestyle counseling to their patients. Physician counseling on lifestyle has a role in disease prevention/management as well as a potential role in reducing morbidity, mortality, and medical costs. 60
Strengths and Limitations
Strengths of our study include the use of 2 validated surveys to assess diet and physical activity. We also had a very high response rate to the survey. Limitations include those inherent to a survey study that relies on participants’ self-report of their behavior. Previous studies, however, have shown the validity of food frequency questionnaires. 61 In addition, the knowledge-based questions and stress related questions were nonvalidated questions. In addition, our study was performed at the DOM in a major academic center in southeastern United States and therefore, our results might not be generalizable to all physicians in different demographic regions. It was also noted that there were no family practice doctors included in this study and the percentage of primary care specialties was on the lower side. This survey was primarily hospital based and therefore, a larger percentage of subspecialists responded to the survey. A comparison between primary care doctors and subspecialists would be worthwhile. Future studies involving multiple specialties and various settings would be helpful to provide insight into the behavior and knowledge of physicians beyond internal medicine and in other settings, such as private practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was done with support from the Gatorade Foundation Education Grant and Heavener Family Foundation.
Ethical Approval
The institutional review board at the University of Florida in Gainesville, Florida approved this survey study.
Informed Consent
Not applicable.
Trial Registration
Not applicable.