
Abstract
The American College of Lifestyle Medicine (ACLM) is forming a Lifestyle Medicine Provider Network (LMPN). The goal of this network is 2-fold: (1) to provide significant benefits to patients by focusing on the adoption of intensive evidence-based lifestyle medicine (LM) therapies to treat and reverse chronic disease and (2) to benefit LM providers by supporting their practice operations and optimizing contracting and reimbursement opportunities. The 2 phases of the network development will include (1) network formation and practice standardization and (2) deployment for group contracting. LMPN will be organized as a special project of the ACLM, with leadership provided through the ACLM LMPN Task Force. As part of this first phase, ACLM will devote the necessary resources to establish the network and promote LM training, certification, and sharing of best practices across the network. The second phase will necessitate the establishment of a separate corporate entity, enabling the acquisition of the required capital and expertise to fully realize the potential of LMPN deployment. Strategic direction will be provided by a LMPN Board of Advisors, consisting of select network members as well as select members of ACLM’s Board of Directors. The first priority of the LMPN will be to recruit interested and qualifying LM practitioners and standardize the LM approach and process of care delivery, starting with high-value services, such as chronic care management. The focus on maximizing existing provider program incentives avails the LMPN the fastest and most efficient path to demonstrating value to its members and to its client base.
‘Clinical trials and cost analyses of LM interventions have repeatedly shown a significant reduction in the total cost of health care.’
Background
One of the greatest challenges facing the practice of lifestyle medicine (LM) is the uncertainty of financial stability. There is a growing recognition that to achieve the economic promise of LM, a new paradigm of medicine must be practiced. LM practices and their staff may look and feel very different from a typical physician practice. 1 The effective practice of LM requires different ways of assessing and measuring patients as well as a unique skill set to achieve lasting behavior change. 2 Incorporating group visits, intensive therapeutic lifestyle behavior change programs, and proactive approaches to health are also important in the practice of LM. These are not superficial adjustments; rather, they are changing health care delivery at its core. To accommodate the required change will require a change to how providers are routinely rewarded and reimbursed for the services they provide. The question is how can LM practitioners receive adequate reimbursement for delivering evidence-based therapeutic lifestyle treatments that reverse disease, decrease drug use, and reduce overall medical cost?
Whereas the financial stability of LM practices is in question, the value that these practices can offer to society is robust and urgently needed. Clinical trials and cost analyses of LM interventions have repeatedly shown a significant reduction in the total cost of health care.3-6 This value proposition has not been lost on various stakeholders eager for a solution to ever-rising health care prices.
Purpose and Goals of the Network
To facilitate the adoption of LM best practices by providers across the country, the American College of Lifestyle Medicine (ACLM) is forming a Lifestyle Medicine Provider Network (LMPN; Figure 1). This network seeks to meet the needs of any stakeholder who wishes to reduce the burden and associated cost of chronic disease. These stakeholders include the following:
Self-funded employers
Unions
Professional organizations
Medicare Advantage plans
Health plans
State or local governments
Centers for Medicare and Medicaid Services (CMS)
Health care cost share cooperatives
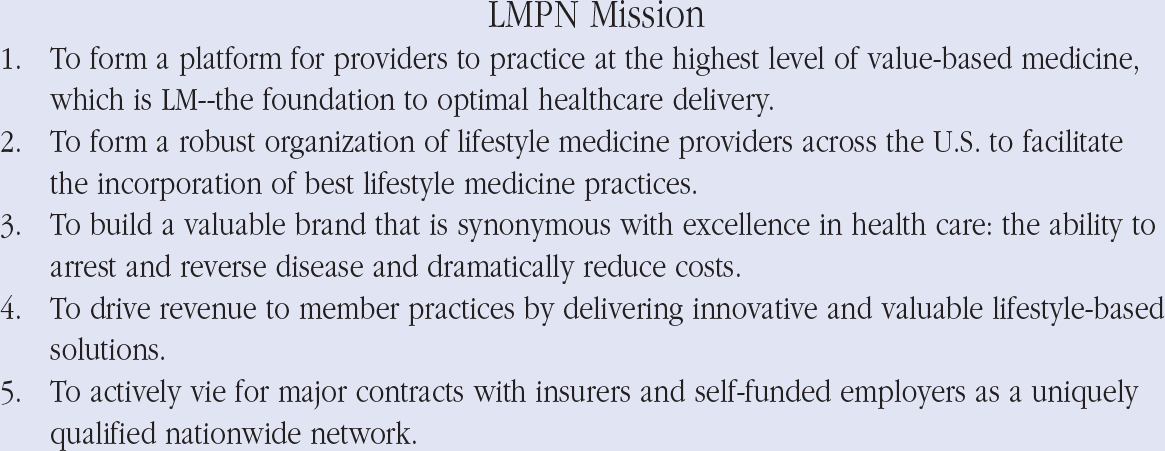
The mission of the Lifestyle Medicine Provider Network (LMPN).
Provider Network Member Criteria
Philosophically, the LMPN will be structured to be as inclusive as possible. Any clinical health care professional who is a member of the ACLM, who is in active clinical practice, who commits to continuous improvement with respect to LM, and who is committed to the adoption of LMPN best practices for its provider education is eligible to join. Certification in the field of LM will be recognized by all network members as the gold standard in regard to network provider credentialing, preparing to the fullest extent possible to ensure that network deployment, in phase 2, meets or exceeds any and all performance guarantees. Preparation and standardization of the network to ensure exceptional outcomes will be vital.
The LMPN will consist of physicians, nurse practitioners, physician assistants, and other health professionals. Although no dues will be required during the first phase of the LMPN, which is projected to last 12 to 18 months, it is anticipated that membership dues will be required during the second phase and will vary based on the size of the practice, with member entities ranging from individuals and clinics to regional health networks. Moreover, it is anticipated that American Board of Lifestyle Medicine (ABLM) board exam eligibility and/or board certification may be a requirement of active network participation. To facilitate communication, the network will rely on large-format web meetings, surveys, self-audits, self-directed training materials, and automation. These and other activities will be coordinated, beginning in the first phase, by an ACLM-employed practice transformation specialist.
One of the main tasks of the LMPN will be to move its members through a pipeline of continuously improving LM practices according to the latest standards. Utilizing a “stone soup” collaborative spirit, members with more expertise will train other members and help them adopt new clinical approaches.
Services
When it is ready to deliver high-quality LM with robust outcomes, the LMPN will seek pilot opportunities as demonstration projects. Beginning in the second phase, the LMPN will expand these offerings based on market demand. These services may be procured from the LMPN through national and regional contracts. It is anticipated that the LMPN will act as a storefront for employers, professional organizations, health plans, or other groups seeking lower-cost and higher-performance health care.
LM consultation. Some member entities may function in a LM consultancy role. Consultation may take the form of one-on-one counseling for disease reversal or dietary advice. It may also take the form of group programs, such as disease reversal programs directed at diabetes, heart disease, obesity, mental health, and so on.
Primary care. The LMPN will function as a top tier network. Customers will pay a per-member-per-month (PMPM) fee to the LMPN for the privilege of enrolling their employees or clients as patients in the network. Primary Care First is a new payment model proposed by CMS for Medicare, anticipated to expand to privately insured beneficiaries, 7 and should be considered a high priority. The LMPN could assist its members in entering into such contracts and in delivering the high-value care that Primary Care First incentivizes.
Telehealth. LM consultation and primary care delivery can be provided through telehealth platforms. This allows LM practices to reach geographically dispersed employees and patients. Customers will pay the LMPN a PMPM fee for the right to use this network as well as additional fees for each consultation. It is anticipated that the LMPN will offer group-based disease reversal programs through a telehealth platform.
Chronic care management (CCM). CCM has been an active Medicare provision since January 1, 2015. It reimburses medical offices to provide strategic and preventive care to Medicare beneficiaries. Many private insurers have followed suit and also reimburse for this. LMPN can provide its primary care–based members with training and coaching to set up their own CCM operations.
Remote patient monitoring. This is a program from CMS that rewards a practice substantial revenue for the use of patient monitoring devices or software. 8 LMPN can deliver a LM-focused monitoring technology, capable of helping patients make healthier lifestyle choices.
Cardiac, weight loss, and diabetes reversal programs. Customers will contract with the LMPN to provide a variety of programs aimed at high-cost diseases. Select LMPN entities will be credentialed by the LMPN as Cardiac, Weight Loss, or Diabetes Reversal Centers.
Accountable Care Organization (ACO). A subset of practitioners who meet the criteria for an ACO may form a national or regional ACO. This provision of the Affordable Care Act 9 rewards primary care practices for reducing total health costs.
Direct contracting entity (DCE). DCEs are a new provision of the Primary Cares Initiative through CMS. 7 As a DCE, the LMPN could provide direct contracting between CMS and a group of LMPN primary care practices.
Organizational Structure of the Network
During the initial phase, the LMPN will operate as a special project of ACLM, led by ACLM’s LMPN Task Force, chaired by David Donohue, MD. The need for the establishment of a separate corporate entity is anticipated, in preparation of phase 2 network marketing and deployment. LMPN members will have a strong voice, with select members comprising an advisory board. The board will guide policies and priorities for the LMPN and vote on key strategic decisions.
During the initial phase, a full-time, dedicated practice transformation specialist will be hired to facilitate the following:
capture aggregate practice-related data through surveys and audits from each member to track progress;
identify training needs from the LMPN members;
coordinate with experts inside and outside of the LMPN who have volunteered to provide training;
facilitate the training of the LMPN members and their clinical staff to ensure that the LMPN standards are being maintained in actual practice;
serve as lead in coordination of pilots and demonstration projects; and
support the development of a business plan and identification of preferred capital sources.
A priority, in preparation for second phase deployment of the LMPN, will be to procure the necessary capital and expert team to interface with external authorities to win contracts and establish partnerships for the benefit of the network, all member practices, and patients served.
Metrics
The LMPN will rely heavily on tracking numerous metrics to gauge progress, determine savings to payers, and identify ongoing operational needs. In phase 1, member surveys and self-audits will be used to track key information. Examples of information that will be tracked include gross revenue, personnel and other costs, number of CCM encounters, and numbers of telehealth encounters. Random chart self-audits will permit tracking of lifestyle workflows of the practice/provider, outcomes data, and aggregate patient population data, such as number of individuals with diabetes. With robust information, the practice transformation specialist will be well equipped to measure progress toward goals and to benchmark members against more successful providers within the network.
Revenue of the Network
Beginning in the second phase, the LMPN will generate revenue through network member dues while also capturing a percentage of contracts negotiated on behalf of its membership (ie, for telehealth, LM consultation). These funds will cover the network’s operational costs and ensure that members are personally invested and committed to the network’s success.
Example Priority: Increase CCM Delivery
An early opportunity that the LMPN plans to pursue is CCM. CCM allows LM providers (whether primary care or consultative) to collect scalable revenue for providing strategic care and LM. A CCM care manager is typically a nurse, medical assistant, or health coach. A medical practice can generally enroll the vast majority of Medicare patients and can bill each month for more than half of CCM enrollees. For example, a practice with 1392 Medicare beneficiaries can generate approximately $18 000 per month in additional net revenue, with little additional time required from providers (Figure 2). A practice can provide extensive lifestyle and preventive medicine counseling in its CCM clinical calls, resulting in measurably improved outcomes. Furthermore, because CCM enables clinical staff to cater to the individual needs of patients, it will likely be valued by patients.
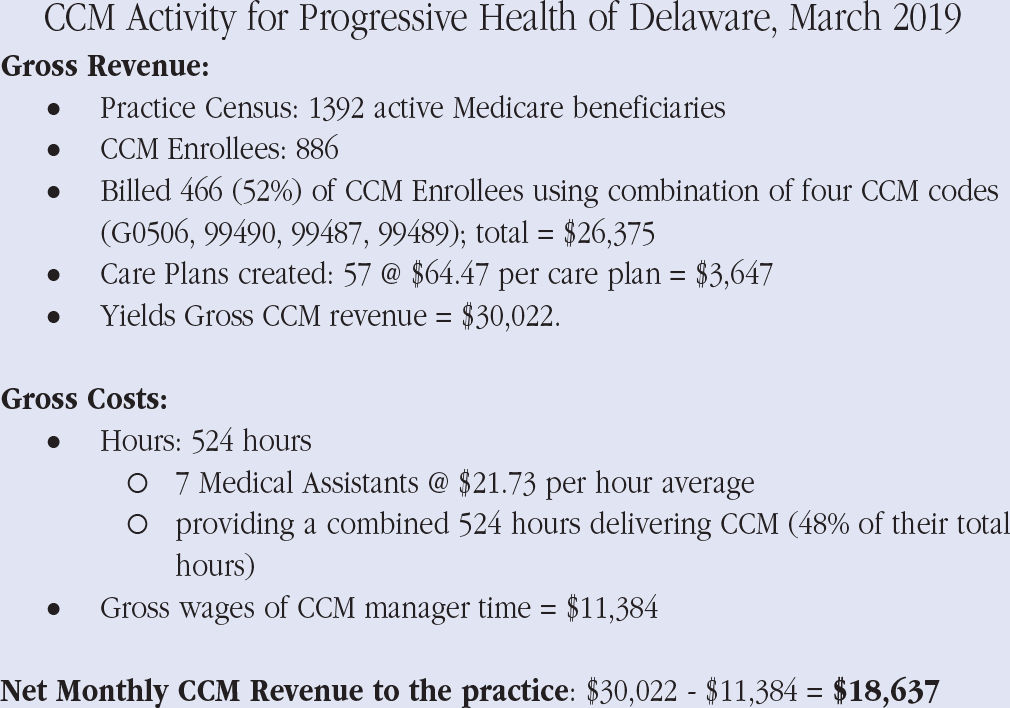
Chronic care management (CCM) balance sheet for a Delaware practice, March 2019.
Conclusion
The ACLM is forming a LMPN to help ensure the financial and clinical success of ACLM member LM practitioners throughout the United States. While initially operating as a special project of ACLM during the first phase of network formation and standardization, the plan is to establish the LMPN as a separate corporate entity in preparation for phase 2 network commercial deployment, actively vying for contracts with insurance companies, self-insured employers, and so on.
The LMPN must meet the core challenges of developing a set of best practices that can be standardized across LM practitioners while simultaneously developing effective means to collect and share data that demonstrate LM’s strong economic business case. The LMPN’s ability to adapt quickly and learn from leading experts will enable effective evidence-based care to be disseminated rapidly to member practices across the nation. The initial focus will be on increasing CCM delivery within practices. It is anticipated that the network will offer additional services, including telehealth and consultation. The financial success of the network will result in the growth of LM and reduction in the cost and pain burden of chronic disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.