
Abstract
Lifestyle medicine commenced in Australia in response to the rise in chronic diseases following the epidemiological transition that began in the 1980s. Today, it is flourishing with an annual conference, a variety of multidisciplinary members, and a developed pedagogy for the “art-science.”
Keywords
And although obesity may or may not have a causal link with other chronic diseases, it can be seen as a canary in the coal mine . . .
Background
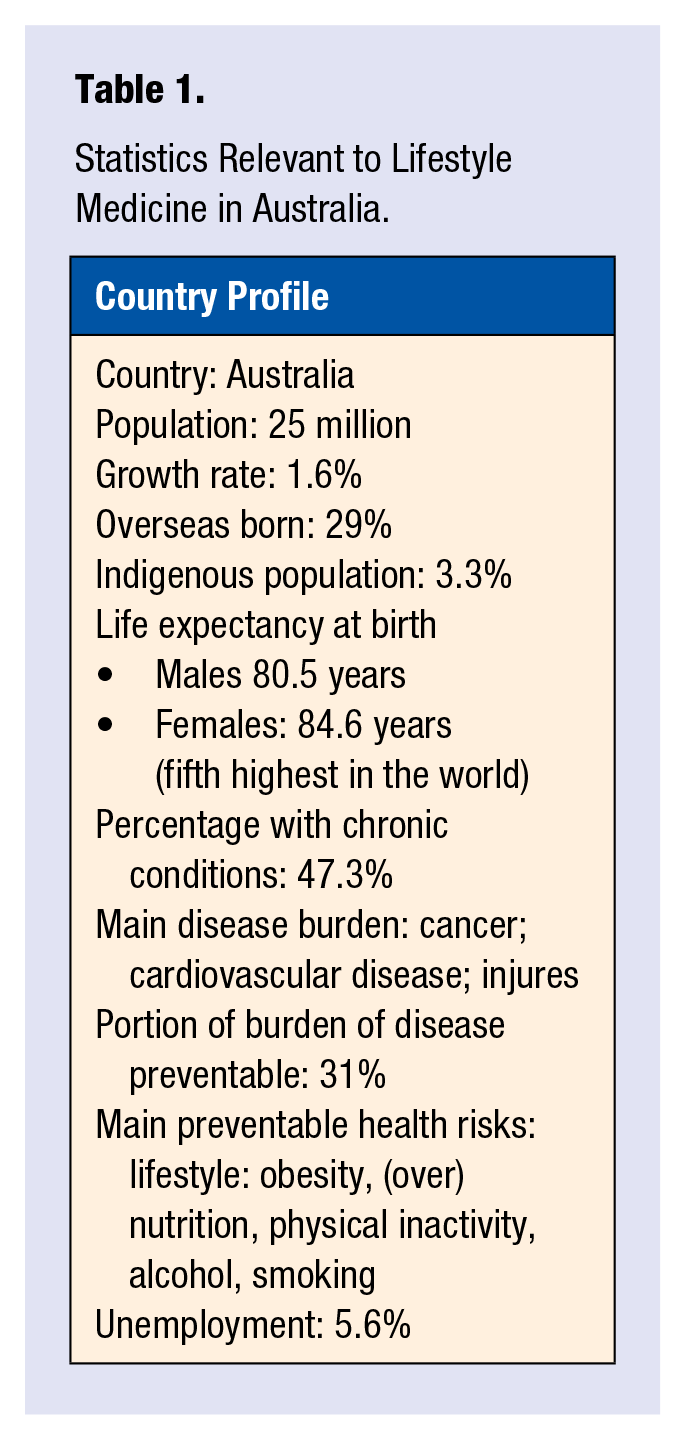
The discipline of lifestyle medicine in Australia developed as a consequence of the “epidemiological transition,” 1 when, around 1980, chronic diseases began to overtake infectious diseases in prevalence (Table 1). This coincided with the beginnings of the obesity epidemic and, not coincidentally, a neoliberal revolution in world events, including an increase in market deregulation, social inequity, environmental pollution, and the availability of low-cost, highly processed, low-nutrient-value foods. And although obesity may or may not have a causal link with other chronic diseases, it can be seen as a canary in the coal mine, warning of other problems in society in general. 2
Statistics Relevant to Lifestyle Medicine in Australia.
Yet obesity failed initially to stir the public imagination. It was not until the early 1990s that obesity (and related chronic diseases) came to be seen as a public health issue. Clinicians were not enthused, however, by the nonclinical taxonomy of health promotion in dealing with this new problem. It was not until the term lifestyle medicine emerged with the first text in this area in 1999 3 that an interest in a new approach to chronic disease emerged.
The Lifestyle Medicine Movement in Australia
To our knowledge, Australia was the second country (after the United States) to formalize a discipline of lifestyle medicine. It did so in 2006 (Table 2)with the election of a steering committee and registration of the Australian Lifestyle Medicine Association (ALMA). A consultant’s report was commissioned in 2007 to consider key issues in the establishment and effective operation of such an association and to confer with other medical associations and stakeholders to ascertain the need for, and positioning of, the new organization.
A Chronology of Events in Lifestyle Medicine (LM), Australia.
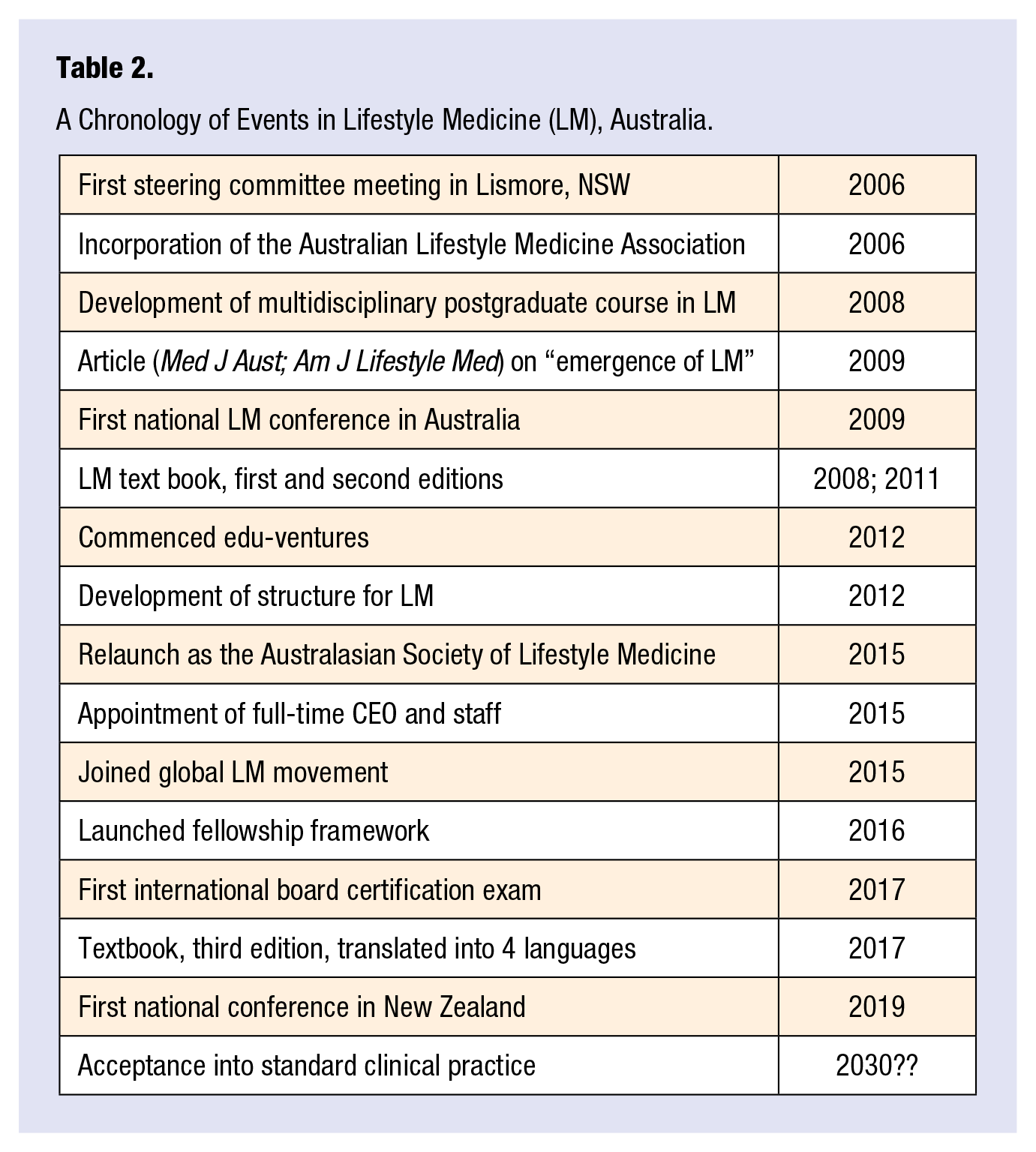
ALMA was formally incorporated in 2008. The organization later changed its name (and branding) to become the Australasian Society of Lifestyle Medicine (ASLM) to include New Zealand. A text book was published in 2008, reprinted in 2011, and a third, international edition published in 4 languages in 2017. 4
The first national conference was held in Sydney in 2009, attracting around 120 delegates. In 2018, attendance at the annual conference had grown to 550, with the event being acknowledged as a world-class medical and scientific meeting. Importantly, by this time, ASLM was seen as a stakeholder to be included in consultations on the national stage, including as a member of the Australian Obesity Policy Coalition and the Health Coalition Aotearoa in New Zealand in 2018.
Membership and Structure
Since inception, ASLM has been both interdisciplinary and multidisciplinary. This has been an important ingredient in the rapid growth of the society. ASLM’s current membership is made up of 45% to 50% physicians and 30% allied health practitioners (mostly dietitians, nutritionists, psychologists, exercise physiologists, nurses, and diabetes educators), with the remainder being public health professionals, health researchers, scientists, and educators. Nonregistered health disciplines have associate status.
Education and Training
A postgraduate master’s degree in lifestyle medicine was offered through a regional university in 2008 followed by another in 2010. More recently, ASLM has designed a plan to develop a suite of practical, practitioner-focused modules of online education and training in lifestyle medicine. This has now received philanthropic funding and will result in therapeutic guidelines, tools, and resources for clinicians to put lifestyle medicine into practice.
Board Certification and Fellowship
In 2016, ASLM introduced a fellowship framework, essentially a points system of recognition of education and training in the domains of lifestyle medicine. This allowed health professionals with prior education to gain recognition toward fellowship of the society. The framework was designed to incorporate the board certification exam (representing one-third of the points required for fellowship). Following the inaugural certification exam in Tucson, Arizona, in October 2017, ASLM held the second exam in Sydney in November 2017, and then in Brisbane in August 2018. At the time of writing, ASLM has 62 graduates of the board certification exam and 60 fellows of the society.
Contribution to Theory and Pedagogy
Whereas the rationale behind the need for a “whole system” approach to health and lifestyle-related disease is unquestioned, it remains for lifestyle medicine to establish a uniqueness and practical application in the field. We have attempted to make a contribution to this in a number of ways:
First, by introducing the concept of anthropogens or “man-made environments, their by-products and/or lifestyles encouraged by those environments,”4(p.40) we have developed a monocausal focus for action against chronic diseases with an underpinning biological basis of metaflammation. This has an analogy to the germ theory, which worked well against infectious diseases. 5
Second, we have developed a framework for the clinical practice of LM. This has 4 principles: (1) knowledge (the science); (2) skills (the art); (3) tools (the materials); and (4) procedures (the actions). Among the former (science), we include the monocausal theory discussed above. Among the latter (actions), we have included new processes such as shared medical appointments (SMAs), adapted from Noffsinger’s original work in the United States, 6 and now “programmed” SMAs, 7 social prescription, telephone triaging, and a range of other newly developing procedures. 8
Third, we have concentrated on points of distinction that can differentiate LM from other adjunct clinical disciplines. We are keen, for example, to never lose sight of the link between the modern environment and lifestyle and how health behavior cannot be divorced from its socioeconomic context. This involves not just looking at the “cause” of a disease, but the cause of the cause, and the cause of the cause of the cause, and so on. 8 In this sense, the immediate determinants of modern chronic diseases and conditions such as smoking, poor nutrition, inactivity, and so on are the equivalent of mosquitos in an infectious disease analogy. Swatting a mosquito or developing a repellent without draining the swamp in which mosquitoes breed (ie, the distal determinants) is a less than total solution.
Funding Limitations
Australian health care is funded by the Medical Benefits Scheme or Medicare. This was developed in the 1970s, an era dominated by infectious diseases and acute care. The system reimburses doctors a fee per “service,” thus constraining preventive and health promoting services and resulting in short, “one appointment/one issue” consultations and inadvertently stifling innovation in clinical practice.
The system is not suited to lifestyle-related illnesses and chronic disease and has been an obstacle to more comprehensive and innovative approaches to chronic disease management. Governments understand this but, in attempting to constrain health spending, are slow to change the current model to better support a new era of disease. A capitation model of imbursement, currently being trialled, offers some promise of correcting this.
Summary
Lifestyle medicine is alive and well in Australia and New Zealand. But with the panoply of medical associations (in nutrition, exercise, environment, etc), it will have to stay ahead of the game to remain relevant. Whereas the knowledge base will remain constant, new developments in clinical skills and diagnostic, prescriptive, and monitoring tools and new processes such as SMAs, with special significance to lifestyle-related problems, should continue to be the goal of LM around the world.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.