
Abstract
Maternal and infant mortality are fundamental indicators of a society’s health and wellness. These measures depict a health crisis in the United States. Compared with other rich countries, women in the United States more frequently die from pregnancy or childbirth, and infants are less likely to survive to their first birthday. Most of these deaths are preventable; disproportionately affect diverse, low-income groups; and are perpetuated by social and health care inequities and subpar preventive care. Lifestyle medicine (LM) is uniquely positioned to ameliorate this growing crisis. The article presents key prescriptions for LM practitioners to build health and health equity for women. These prescriptions, summarized by the acronym PURER, include action in the areas of (1) practice, (2) understanding/empathy, (3) reform, (4) empowerment, and (5) relationship health. The PURER approach focuses on partnering with diverse female patients to promote resilience, promoting social connection and engagement, facilitating optimal family planning and advocating for culturally responsive, equitable health care systems. Through PURER, LM practitioners can help women and partners resiliently overcome the harmful challenges of discrimination and stress characterizing present-day American life. Over time, the equitable and collective practice of LM can help ameliorate the health care barriers undermining the health of women, families, and society.
Keywords
‘Pregnant women in the United States are more likely to die from childbirth- or pregnancy-related causes than in other developed nations in the world.’
“We should all want to live in a world that supports the power and potential of women,” stated Texas Representative Kay Granger in 2015. 1 Whereas politicians of different stripes can agree on the fundamental need to protect the health of women—society’s mothers, sisters, partners, and daughters—sobering statistics reveal our poor performance in this realm. Worldwide, women are disproportionately affected by inequality, violence, poverty, and preventable health conditions. 2 Pregnancy is a leading global cause of death, consuming about 830 women daily. 3 Many of the deadly complications associated with pregnancy and childbirth could be prevented by skilled, responsive, and prevention-oriented health care over the women’s life span.3,4
In rich and even some middle-income countries, occurrence of maternal and infant deaths are at least partly linked to the usual suspects: preventable lifestyle factors. Several risk factors for pregnancy complications and maternal death include potentially preventable chronic conditions such as hypertension, obesity, preexisting cardiovascular disease, diabetes, and use of tobacco, alcohol, and illicit drugs5-9 Preexisting chronic conditions now explain a third of US maternal deaths, representing the most rapidly increasing cause of maternal mortality in the United States. 9 Preexisting chronic conditions in the mother are also linked to the most common causes of infant death, including congenital birth defects and low birth weight.10,11 In the United States, women of child-bearing age are experiencing the same unhealthy shifts in weight, blood sugar, and blood pressure common to all Americans.7-9 One may superficially conclude that addressing the rising death toll of pregnant mothers and infants is simply a matter of encouraging women to make healthier lifestyle choices in the realm of diet, activity, and substance use.
However, as public health and preventive medicine practitioners have long recognized, the lifestyle behaviors that most powerfully influence health status spring from surrounding culture and society. Markers such as maternal mortality and infant mortality represent a “compelling social mirror” of societal “healthiness,” social justice, and welfare.12,13 In fact, pregnancy-related mortality ratios are explicitly used by the Centers for Disease Control (CDC) as an indicator to “measure the nation’s health.” 13 By this yardstick, the United States is undergoing a worsening societal crisis. Pregnant women in the United States are more likely to die from childbirth- or pregnancy-related causes than in other developed nations in the world. 14 American-born babies are 76% more likely to die before their first birthday compared with babies born in other rich countries. 15 Consistent evidence supports that such subpar maternal and child health outcomes stem at least partly from the high poverty rate in the United States, which ranks highest among all developed countries (second highest for child poverty), and the status of the United States as one of the most unequal developed societies.9,10,12,16-19
Even though the overall US infant mortality rate (IMR) has declined by 15% since 2005, the rate of decline has not kept pace with worldwide declines and appears to have plateaued.20,21 In 1960, the United States ranked 12th among developed countries in infant mortality. 22 With its current (2017) IMR of 5.9 deaths per 1000 infants—or 25 000 infant deaths annually—the US now ranks lowest among the world’s wealthy countries.20-23 Meanwhile, as maternal mortality decreased substantially in most countries around the world, the US maternal mortality rate (MMR) actually increased over the past 2 decades.3,24-28 Some researchers have argued that the upturn in US MMR (currently 26.4 per 10 000 births) reflects changes in national recordkeeping and coding practices; however, controlled and adjusted analysis confirms a persistent increase in MMR of at least 26% in recent years, underscoring the reality that “the U.S. maternal mortality rate is moving in the wrong direction.”24(p.454),28,29 Moreover, an in-depth assessment by 9 maternal mortality review committees in the United States estimated that 63.2% of pregnancy-related deaths were preventable. 28 On top of maternal deaths, there is the significant, highly preventable, and rapidly increasing burden of near-deaths and lifelong health complications—termed severe maternal morbidity—that affect 50 000 delivering women per year. (Table 1 contains a listing of selected, commonly used terms and definitions).4,29-31
Defintions for epidemologic terminology related to infant and maternal mortality.
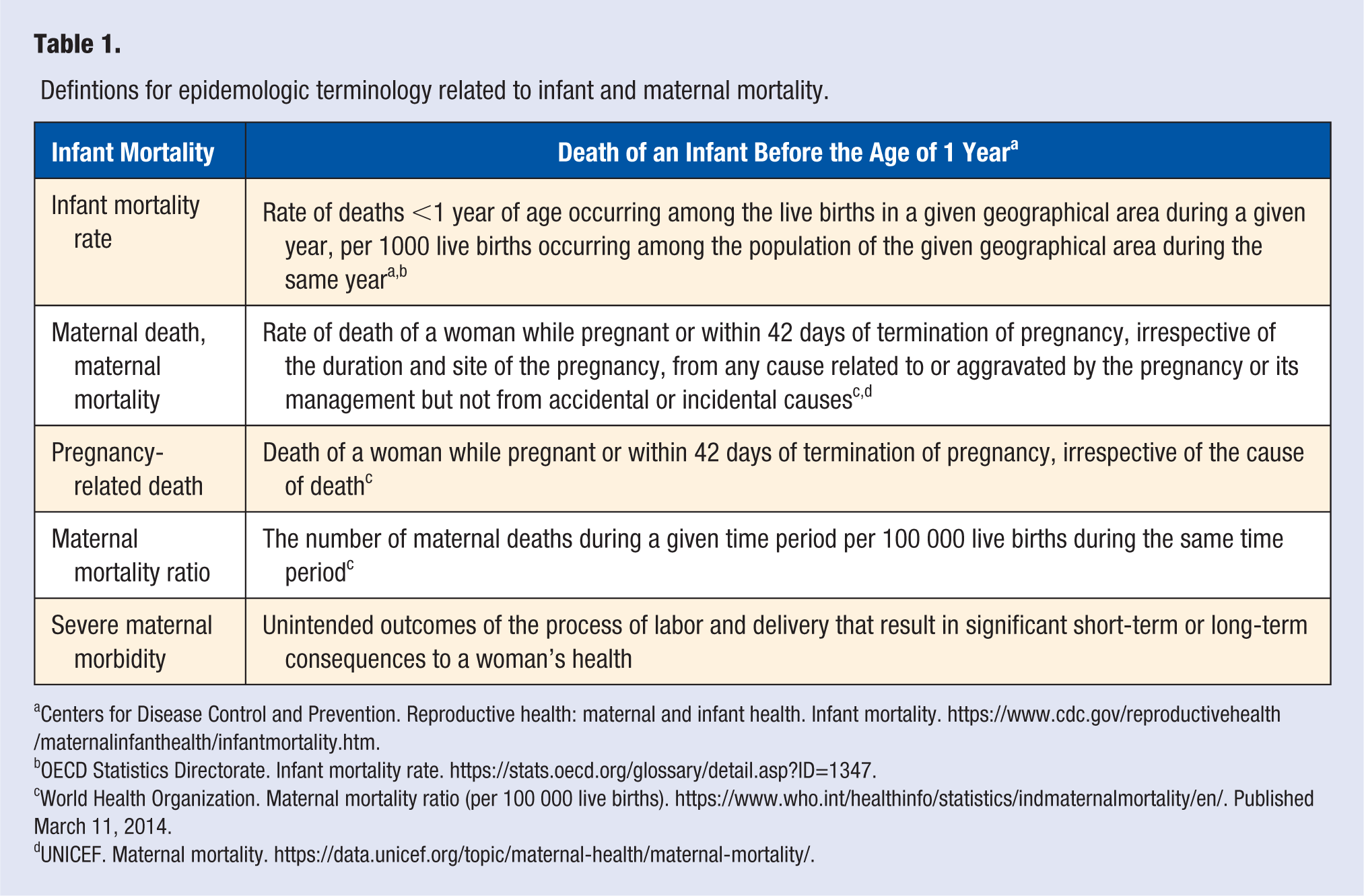
Centers for Disease Control and Prevention. Reproductive health: maternal and infant health. Infant mortality. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/infantmortality.htm.
OECD Statistics Directorate. Infant mortality rate. https://stats.oecd.org/glossary/detail.asp?ID=1347.
World Health Organization. Maternal mortality ratio (per 100 000 live births). https://www.who.int/healthinfo/statistics/indmaternalmortality/en/. Published March 11, 2014.
UNICEF. Maternal mortality. https://data.unicef.org/topic/maternal-health/maternal-mortality/.
A deeper dive into IMR and MMR patterns in the United States reveals the disproportionate burden of death and disability borne by African American and Native American women and babies. Compared with Caucasian counterparts, African American babies are more than twice as likely to die in the first year of life (IMR = 11.4 in 2016), whereas African American mothers are 3 to 4 times as likely to die from pregnancy.30-34 In New York City, African American mothers were 12 times more likely to die during childbirth from 2005 to 2010 compared with Caucasian mothers (an increase from a 7-fold gap in 2000-2005). 30 Even as overall US IMR declined, the gap between African American and Caucasian IMRs and MMRs remained unchanged, possibly worsening in several states.26,33,34
Evidence suggests that the lifestyle and health of pregnant minority women (and survival of their offspring) are uniquely vulnerable to accumulated, subtle exposures of poverty, inequality, and prejudice.15,16,18,33-40 Recognition of this link is imperative for lifestyle medicine (LM) practitioners to begin reforming such disparities at the grassroots health care level. For African American women, lifestyle and behavioral factors of diet, exercise, educational level, and even individual income level each fail to fully explain the disparity between birth and maternal outcome.37-39 In New York, African American mothers with a college education were twice as likely to die—and more likely to suffer severe complications and mortality—from a pregnancy or childbirth compared with white women without a high school education.30,39 Furthermore African American mothers are 71% less likely than their Caucasian counterparts to smoke during pregnancy and 41% less likely to consume alcohol—both behaviors associated with adverse pregnancy and birth outcomes.41,42 African American women are also more likely than their Caucasian counterparts to experience maternal death from preventable, reversible causes. 43
Recent research suggests that time of exposure to US social stresses and biases may serve as major contributing factors.35,37,40,43-46 A study by Collins et al 35 illustrated this phenomenon, countering the viewpoint that the typical immediate causes of infant deaths—low-birth-weight babies, prematurity, and congenital defects—were a result of intrinsic genetic predisposition. 40 The Collins study found that infants of African-born mothers were similar in birth weight outcomes and survival patterns to infants of US-born Caucasian mothers, rather than US-born African American mothers. Within one generation, the protective “African-born” effect disappeared, and adverse birth outcomes and low birth weight prevalence increased. As Collins stated, “There’s something about growing up in a black female in the U.S. that’s not good for your childbearing health. I don’t know how else to summarize it.” 44 (The quote is mentioned in this video documentary, “Unnatural Causes”. Dr. Collins states the quote in the film. There is a transcript of the film that illustrates Dr. Collins’ quote: https://www.unnaturalcauses.org/assets/uploads/file/UC_Transcript_2.pdf). A similar situation is seen for Mexican American births; increased acculturation to the United States appears to worsen risk of adverse birth outcomes.46-49 In a recent study of US pregnant Mexican women living in low-income areas, US-born Mexican mothers experienced worse birth outcomes and low-birth-weight rates of 14%, compared with Mexican-born mothers, who had low-birth-weight rates of only 3%. 50 The concept that time of exposure to life in the United States could act as a significant, independent risk factor harming the health of pregnant women and infants is further supported in studies of other ethnicities.51,52 As reported by the CDC, foreign-born mothers experience improved birth outcomes compared with their US-born racial/ethnic counterparts, despite the former group’s relatively lower socioeconomic status level and later entry into prenatal care. 53
Although the national burden of mortality and morbidity falls most heavily on African American mothers and infants, it is important to recognize that the public health crisis of preventable maternal and infant deaths affects all ethnic groups. Even the Caucasian-specific MMR and IMR in the United States is significantly higher than in OECD counterparts. 25 Moreover, micro-level analysis illustrates that geographic pockets of elevated maternal and infant deaths cross ethnic lines. A study conducted by the University of Texas System Population Health Division analyzed IMR data by zip code and race in various Texas counties. The study found that for all races studied (white, African American, and Hispanic), there existed counties where infant mortality was both significantly lower and higher than the national average (ranging from 1 to greater than 10). 54
Indeed, for all women in the United States, biases occurring within the health care setting exacerbate the infant and maternal mortality crisis for women in the United States. These health care biases, representing low-hanging targets to be addressed by the individual and collective work of LM practitioners, can be categorized as follows: (1) gender bias: lower quality health care for women; (2) infant bias: focus on infant over mother; and (3) treatment bias: preference for procedures over prevention.
Numerous reports suggest that women as a whole are treated as “second class citizens in health care,” a situation that partly explains why patients seeking better care via alternative and nontraditional modalities are predominantly women.55-60 One study found that women were up to 25% less likely than men to receive pain medication in emergency rooms; other reports confirm that women are treated for pain less aggressively.56,59,61 Another study found that women received bystander CPR less frequently compared with men during myocardial infarction. 57 . Many serious reproductive and gynecological conditions in women go undiagnosed; women are more likely to report poor health, yet are more likely to be dismissed or misdiagnosed by health care professionals. 59 In a troubling confirmation of health care system gender biases and their devastating effects, a recent study reported that women treated by male physicians during a myocardial infarction were less likely to survive compared with patients of either gender treated by female physicians or male patients treated by male doctors. 62
During pregnancy, gender bias manifests as lower likelihood of women to participate in their health care decisions and fewer resources dedicated specifically to promoting health in pregnant mothers. 55 The majority of women polled in a recent survey reported that they held back from asking questions of their providers because they feared being perceived as difficult (22%), felt rushed (30%), or desired a different plan of care (22%).60,63 Such fear undermines the woman’s ability to engage in partnership approaches, such as creating birth plans, that increase a woman’s ability to promote desired elements of a pregnancy.
Other experts note the systemic focus on the “baby” to the detriment of the “mother” in health care settings.25,64 The belly of the pregnant mother becomes the focus for the purpose of monitoring the baby; comparatively little monitoring addresses the woman’s own health. Federally, fewer dollars flow to the care and wellness of the pregnant mother compared with the unborn baby; only 6% of federal grants supporting maternal and child health focus on the health of mothers, whereas 78% targeted infant outcomes. Only 1 multidisciplinary hospital care unit has been established to care for high-risk pregnant mothers; 20 such programs exist for high-risk infants. 64 So-called “emergency” Medicaid programs that cover uninsured mothers in many states, such as Texas, cover infants for up to 1 year but cover mothers for only 60 days postpartum. 65 Although there are no data available covering that 60-day span, the maternal mortality and morbidity task force of Texas found that the most maternity-related deaths occurred after the 42nd day postdelivery and within the first year. 66
Finally, the health of pregnant women and infants also suffers from the systematic health care bias toward treatment and procedures over prevention. Reimbursement guidelines incentivizing procedures often supersede women’s preferences for more natural birth plans. A hospital can often bill significantly more for a cesarean section compared with a vaginal delivery 67 ; each cesarean section increases the risk of placenta accreta and associated adverse outcomes in a subsequent pregnancy. 68 Furthermore, missed opportunities in family planning—an ultimate form of upstream prevention, with profound health benefits accruing to mothers, families, communities, and even the economy—also undermine the health of women and infants. Women who can plan and space births when they are physically and mentally ready have healthier pregnancies and babies.25,69 Despite the official position of the American College of Obstetrics and Gynecology that “access to comprehensive contraceptive care and contraceptive methods [is] an integral component of women’s healthcare,” many women report subpar access and lack of knowledge to the most effective, long-acting forms of reversible contraception.69-71 As a result, rates of unplanned and teen pregnancy in the United States continue to remain among the highest in the western industrialized world. 72
Promoting Real Health Care Reform: The PURER Approach to Lifestyle Medicine for Women
Faced with the unhealthy root causes driving preventable deaths and morbidity of pregnant women and infants, how can LM practitioners act to reform the care of women? A first step is to recognize that LM is uniquely positioned to support meaningful, salutary advancements in the current public health crisis. Relegating the task of reform entirely to obstetricians or relying prenatal care enhancements alone to rectify the problem is shortsighted and unsupported by recent statistical trends. As Lu et al note, “to expect prenatal care, in less than nine months, to reverse the lifelong, cumulative impact of social inequality on the health of African American mothers, may be expecting too much of prenatal care.”34(p.64) Rather, the greatest potential for promoting healthy pregnancy occurs over the
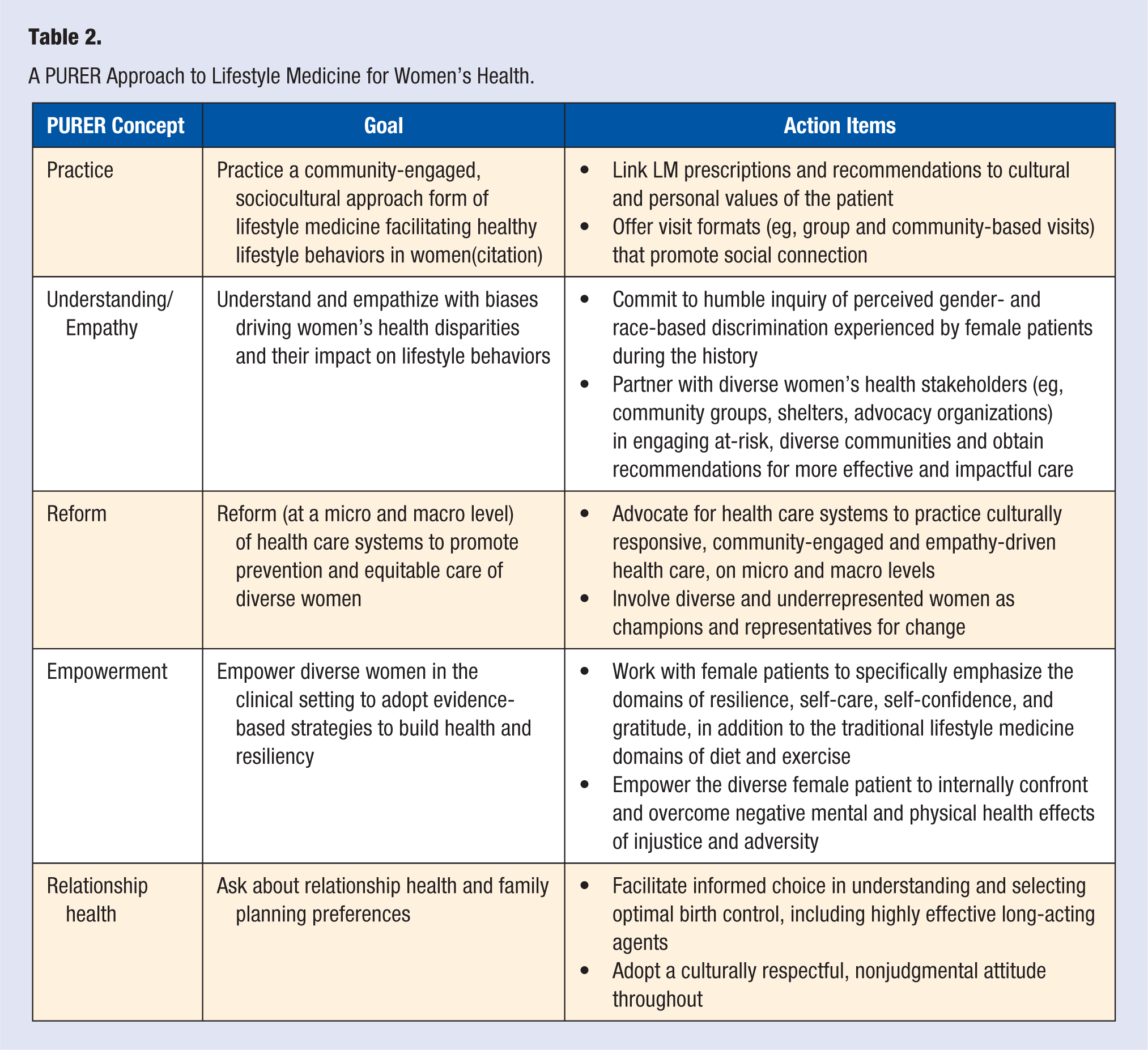
A circumspect LM movement must target not only preventable chronic conditions and specific lifestyle behaviors of diet and exercise, but also build a woman’s resilience to overcome the impact of bias and other social factors on health and behavior; engage diverse women with empathetic, culturally sensitive, and cohesive approaches; inform women on effective choices for family planning and optimizing relationship health; and partner with underrepresented women’s groups to advocate for health care system reform. These concepts can be promoted through a set of prescriptions, summarized by the acronym PURER, for adoption by the LM practitioner. The PURER approach emphasizes addressing the unique needs of diverse women in the areas of (1) practice, (2) understanding/empathy, (3) reform, (4) empowerment, and (5) relationship health. Table 2 describes each PURER prescription and related action items. The rationale for the PURER approach is described in the discussion below.
A PURER Approach to Lifestyle Medicine for Women’s Health.
Addressing systemic discrimination, societal racism, and inequality is a daunting challenge for a single LM practitioner. Nevertheless, the field of LM must prioritize, advocate for, and spearhead the collective impact of empathetic, culturally responsive care internal and external to the health care system—for example, “Real Healthcare Reform.” 73 Such a movement in LM will equip patients and providers with the evidence-based, resilience-building tools needed to overcome modern American stresses. Culturally sensitive, empathy-driven care that responds to the needs of women—and particularly those of specific higher-risk ethnic groups—is paramount to this movement, an antidote to the multiple health care biases affecting the well-being of women nationwide. 74 Community-engaged LM (CELM), an evidence-based framework emphasizing cultural responsiveness to promote health equity, represents one pathway toward such positive outcomes. 75 Details of this framework, including specific principles of cultural responsiveness and community engagement and examples of practice approaches, are presented in other publications, including a sister article within this conference edition.74-76
LM practitioners already are well versed in the principles of effective listening and counseling, motivational interviewing, and patient-centered care.77,78 These skills fill a void in a health care landscape that systematically ignores preferences and needs of women. LM practitioners can also internalize lessons learned from the “Hispanic paradox,” a phenomenon where immigrant Hispanic communities facing adverse social influences of poverty and social stress have lower-than-expected rates of maternal and infant mortality. 79 Research on the Hispanic paradox suggests that a strong connection to community and cultural identity are protective factors, able to at least partially “immunize” against negative social influences and stresses. 80 Fragmentation and social isolation, on the other hand, can prove detrimental to health status and lifestyle. LM practitioners can build trust and connection with their female patients by committing to ask about, understand, and respond empathetically to the impact of perceived injustice or bias on patient behaviors and health. Moreover, LM practitioners can promote social connection and cohesion by engaging women in innovative visit formats such as group visits, which are well received and linked to improved behavioral health outcomes. 81 Finally, LM practitioners can empower pregnant patients in their practice to take an active role in facilitating a healthy birth, through mechanisms such as developing birth plans, engaging in stress-reduction practices, and partnering with health care professionals such as midwives and doulas (associated with better birth outcomes and maternal satisfaction).82,83
LM practitioners can also harness opportunities for prevention by advocating for reform within health care settings. Advocacy by LM practitioners champions the needs of diverse women to improve cultural responsiveness and quality of health care for diverse women at a micro (local) or macro (systemwide) level. LM practitioners can also be present and participate in community boards, meetings, and town halls offered by local women’s groups and stakeholders. 76 In line with the community-engaged approach, advocacy should be bidirectional. 84 Thus, advocacy efforts should specifically engage diverse and vulnerable women in setting the reform agenda and in the development and presentation of data, stories, concerns, and recommendations to administrators.84-86
The forte of the practicing LM physician is the prevention, treatment, and even reversal of chronic common diseases, such as diabetes and cardiovascular disease, via optimization of weight, diet, activity, stress, and sleep levels.77,78,87 Applying the LM core competencies for women across the life span can translate to profoundly protective effects during pregnancy and childbirth. For example, preventing or reversing diabetes in a woman of childbearing age could potentially reduce the risk of preeclampsia and associated adverse birth outcomes by 3- to 4-fold; controlling or reversing high blood pressure prior to pregnancy could potentially reduce the chance of preterm birth and perinatal death by nearly 3- and 4-fold, respectively.9,88,89 Applying the core competencies for women of childbearing age to prevent and reverse obesity, the “most common medical problem in pregnancy” today, also holds potential for tremendous public health impact.90,91 Some evidence suggests that the use of smartphone “apps” to promote is a feasible and effective way to engage women in healthy behavior change. 92 Thus, an effective LM women’s health practitioner will continue to engage women in the evidence-based, prevention-oriented partnership care model that builds confidence and motivation to engage in optimal habits of eating, activity, and self-care.
Finally, the LM practitioner can take an active role in asking about relationship health and facilitating informed choice of evidence-based contraception and family planning services. All primary care LM providers (including family, internal, and pediatric physicians and physician assistants; health coaches; behavioral health specialists; midwives and nurse practitioners; and others) should participate in the provision of family planning or women’s health services.93-95 Such integration will reduce the barriers of access and trust and will engage not only adult women, but also adolescents and male / female partners. Whereas a complete discussion of current contraception methods, practices, and provider attitudes is beyond the scope of this article, substantial evidence suggests that facilitating informed choice for long-acting reversible contraception (LARC) carriers has profound health benefits for women, infants, families, societies, and economies at large. 93 Yet the use of LARC contraceptives remains low in the United States because of several barriers, including misperceptions among both providers and patients, cost barriers, and patient access to LARC devices.94-96 LM practitioners should enquire whether patients wish to become pregnant in the subsequent year. 97 If the answer is no, the LM practitioner should provide comprehensive counseling concerning the different methods available for both male and female family planning and offer information on emergency contraception and how to access it. For patients desiring LARC, same-day insertion is recommended. 95 The PEARLS approach (Partnership, Empathy, Apology, Respect, Legitimization, Support) 98 to effective counseling can be applied to initiating family planning conversations. Table 3 presents this approach, along with specific questions that can be used to initiate family planning conversations.
Two Approaches to Initiating Family Planning Conversations.
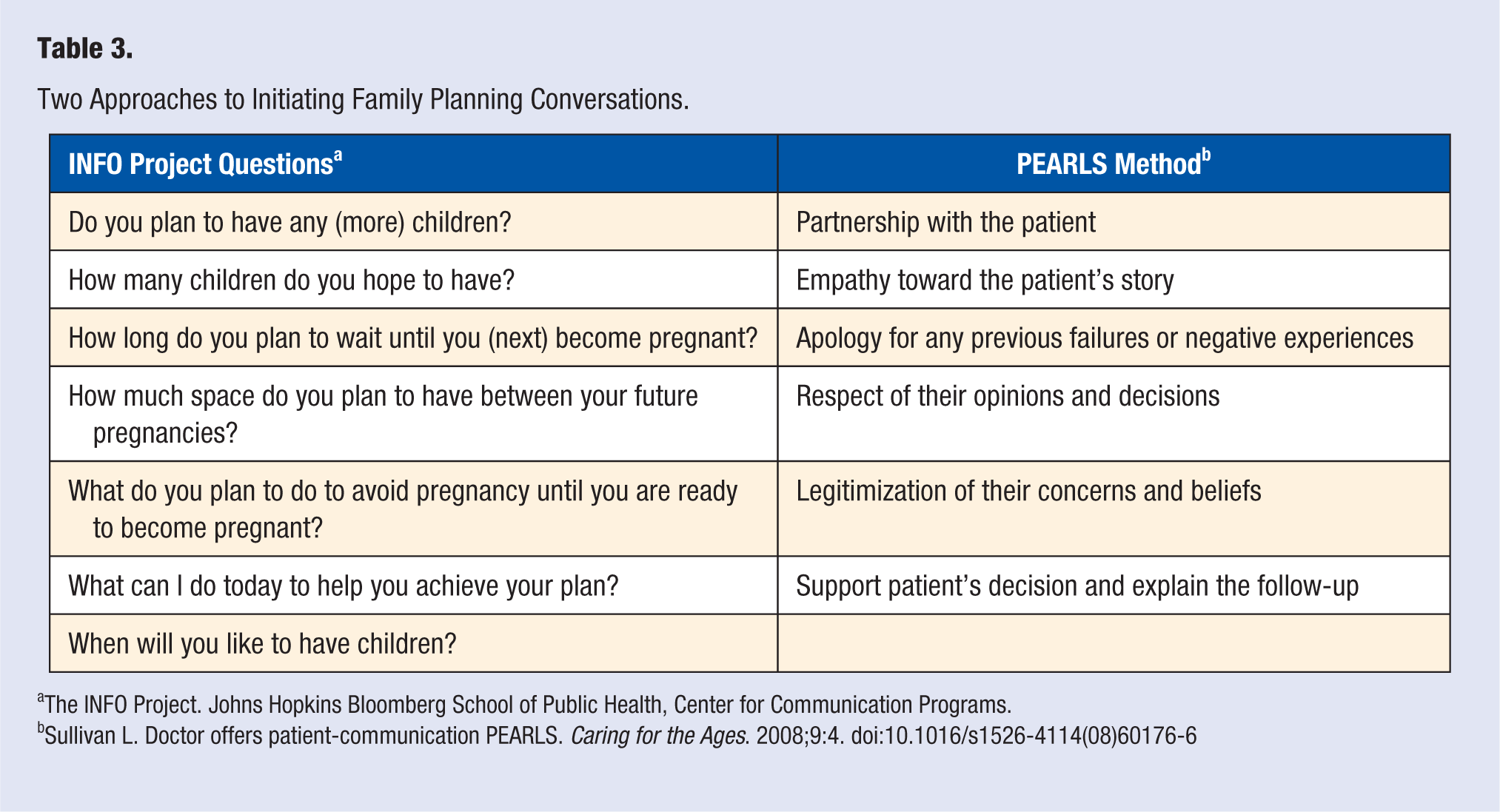
The INFO Project. Johns Hopkins Bloomberg School of Public Health, Center for Communication Programs.
Sullivan L. Doctor offers patient-communication PEARLS. Caring for the Ages. 2008;9:4. doi:10.1016/s1526-4114(08)60176-6
Conclusion
A recent American Public Health Association policy statement described the US crisis on maternal mortality as a “significant human rights issue,” representing the “ultimate failure” of maternal health efforts. 99 Indeed, infant and maternal mortality are significant indicators of the social and public health of a nation, reflecting quality and access to medical care, socioeconomic conditions, public health practices, and the overall health conditions of women and families. The recent IMR plateau, its persistent elevation relative to other developed countries and Healthy People 2010 target goals, and continued increase in MMR have spurred great concern among researchers and policy makers. 100 Such factors support an urgent need for LM-led “Real Health Care Reform” promoting health care equity, which must occur in concert with social efforts to rectify and eliminate systemic discrimination experienced by African American and other disadvantaged minorities and women at large.
Eliminating structural and systemic discrimination against women and ethnic minorities may appear as a long-term, lofty vision. However, the LM community can and must support such outcomes via micro-level practice changes focusing on empathetic support and empowerment of the female patient. This article presents an approach, PURER, that can be implemented by LM practitioners to begin promoting better health in women. Evidence-based tools promoting resilience, perseverance, self-confidence, and intrinsic motivation for healthy behavior can enable women to overcome experiences of injustice and adversity and heal mentally and physically. LM practitioners can further act as advocates for minority women, removing existing barriers to culturally competent care within their health care systems and improving the quality of culturally tailored, motivational interviewing and patient-centered care skills. Furthermore, LM practitioners can improve current and future maternal health outcomes by continuing to partner with patients to achieve healthier lifestyle choices. Finally, fundamental to the future health of women, infants, and society is culturally tailored education on and provision of evidence-based, long-acting contraception for women who desire it.
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of the following persons: Anisha Daxini, MD, second year internal medicine resident at Nazareth Hospital, Philadelphia, Pennsylvania; the following individuals from the University of Texas Rio Grande Valley School of Medicine (Edinburg, TX): Robert Nelson, MD, MS; and Tony Ogburn, MD; the Hidalgo County Healthy Families Team (Brenda Salazar, MPH, CPH; Amanda Sierra, MPH; Diana Lopez, Ercilia Ramirez, CHW; Maria Hernandez, CHW; and Angela Tanguma, NP); the Hidalgo County Public Health Department (Eddie Olivares, Nancy Trevino); and the University of Texas System advisory team (Austin, TX): Divya Patel, PhD, Nagla Elerian, David Lakey, MD, and Melissa Valerio, PhD, MPH.
Author’s Note
This article is based on a workshop given at the Annual Meeting of the American College of Lifestyle Medicine 2018 in Indiana, IN. Janani Krishnaswami is currently affiliated with UWorld LLC, Irving TX.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.