
Abstract
Objective. To examine the impact of the health self-empowerment theory–based, culturally sensitive Health Self-Empowerment (HSE) Workshop Series to Modify and Prevent Obesity on levels of health promoting (health-smart) behaviors, motivators of and barriers to these behaviors, health promoting lifestyle variables, and health status indicators (body mass index [BMI] and blood pressure) among a culturally diverse sample of overweight/obese adults from mostly low-income households. Design. A total of 153 overweight/obese adults participated in an immediate treatment (IT) group (n = 100) or a waitlist control (WC) group (n = 53). Results. Post-intervention, the IT group compared with the WC group reported (a) significantly higher engagement in physical activity and healthy eating; (b) significantly less intake of calories, total fat, trans fat, saturated fat, sugar, and added sugar; (c) significantly higher motivators for engaging in 2 of 4 specific health-smart behaviors; (d) significantly lower barriers to engaging in 3 of 4 specific health-smart behaviors; and (e) significantly lower BMI and systolic blood pressure. Conclusion. The HSE Workshop Series may be an effective intervention for treating and preventing obesity among diverse low-income adults—individuals who often perceive/experience limited power over their health. Health care providers, particularly physicians, have important health empowerment roles in this intervention.
A health promoting lifestyle can prevent or modify overweight/obesity and related diseases.
More than 73% of adults in the United States are overweight or obese. 1 This is alarming, especially given that obesity is associated with many serious health problems, including cardiovascular disease, type 2 diabetes, hypertension, and some types of cancer. 2 While obesity and its associated health problems affect all groups in the United States, they disproportionately affect some racial/ethnic minority groups and individuals from low-income backgrounds. 3
A health promoting lifestyle can prevent or modify overweight/obesity and related diseases.4-6 Central among the actions that constitute a health promoting lifestyle are engagement in health promoting behaviors, such as healthy eating, exercising consistently, limiting sedentary behavior, stress management practices, and health responsibility behaviors. 7 Individuals from minority and low-income groups—as compared with individuals from nonminority and high-income groups—report lower engagement in physical activity, 8 have higher rates of overweight/obesity,9,10 and perceive more daily life stressors. 11 Given these findings, it is important to examine health promotion interventions designed to modify and prevent obesity among minority and low-income groups.
Culturally sensitive and individually tailored health promotion interventions for African American adults have demonstrated increases in fruit and vegetable intake and physical activity. 12 However, our review of the literature revealed no studies that have examined the impact of such interventions on health status indicators (eg, body mass index [BMI] and blood pressure) of culturally diverse adults who are overweight or obese. The present study examines the effect of the Health Self-Empowerment Workshop Series to Modify and Prevent Obesity (hereafter referred to as the HSE Workshop Series) on health status indicators and motivators of/barriers to health promoting behaviors, in addition to physical activity and healthy eating behaviors.
The present study is novel in that it tests the effects of a culturally sensitive, practical, and cost-efficient workshop series when implemented with culturally diverse adults from mostly low-income households. Such adults often perceive themselves as having limited power over their health because of intractable low socioeconomic status–associated barriers to health (eg, not being able to afford fresh vegetables and living in unsafe or low-resource neighborhoods that deter outdoor physical activities).
Theoretical Underpinnings of the HSE Workshop Series
Health self-empowerment (HSE) theory underlies the structure of the HSE Workshop Series. This theory is responsive to the facts that the social injustice, health inequity, and health illiteracy that contribute to the disproportionately high prevalence of obesity and related diseases among minorities are typically intractable, and thus there is a need for control over one’s health under whatever conditions exist. HSE theory asserts that self-empowerment oriented, cognitive–behavioral self-variables can promote this control over one’s health and are key target variables for understanding and modifying the health behaviors of individuals with low perceived and actual power, such as individuals who live in low-income communities.13,14
Specifically, HSE theory asserts that engagement in health promoting behaviors is influenced by the following 5 literature-based, modifiable, self-empowerment oriented, cognitive–behavioral self-variables: (a) health motivation, (b) health self-efficacy, (c) self-praise of health promoting behaviors, (d) active coping styles/skills for managing emotions such as stress and depression, and (e) health responsibility and knowledge.
Health motivation refers to the desire to engage in health promoting behaviors/lifestyles—a desire facilitated by relevant thoughts, goals, and/or values. Health self-efficacy refers to one’s perceived capability of engaging in behaviors/lifestyles that promote physical health and/or mental health, as well as the expectation that these behaviors/lifestyles will produce desired positive health outcomes such as a healthy BMI. Self-praise of health behaviors is the use of cognitive or overt statements to increase and sustain these behaviors. Active coping style/skills refer to behavioral or cognitive responses to reduce any negative impact of the stressor. Health responsibility refers to being accountable for one’s health to the degree possible, as evidenced by behaviors to promote one’s own health. Health knowledge is an inherent aspect of health responsibility given that one cannot be responsible for one’s health without having knowledge about health promoting behaviors. It is theorized that these HSE theory variables interact to directly or indirectly influence health promoting behaviors (eg, eating healthy foods), which in turn directly influence health status indicators (eg, BMI, blood pressure).
Cultural Sensitivity in Implementing the HSE Workshop Series
Cultural sensitivity in the context of the HSE Workshop Series refers to conveying existence of the knowledge, skills, awareness, and experiences needed to provide health promotion and health care services to culturally diverse individuals in ways that enable these individuals to feel comfortable with, trusting of, and respected by the providers of these services. 14 A core aspect of enabling workshop participants to have these feelings is actively engaging them in customized workshop activities, which is a form of empowerment. Cultural sensitivity in implementing the HSE Workshop Series is conveyed in its content and also its implementation.
Some examples of how cultural sensitivity is conveyed in the content of the HSE Workshop Series are as follows: (a) workshop participants were asked to identify their own motivators of and barriers to health promoting behaviors and to identify goals and strategies for overcoming the barriers and using the motivators; (b) participants could submit anonymous questions to workshop leaders; (c) recognition of common cultural traditions were incorporated into presentations by health professionals; (d) workshop staff used visual materials that accommodated various levels of literacy; (e) the focus of the workshop series was on promoting health, not on losing weight; and (g) participants and workshop staff shared ways to engage in health promoting behaviors without abandoning cultural values and traditions (eg, ways to cook collard greens that taste good with less fat and sodium).
Some examples of how cultural sensitivity was conveyed in the implementation and evaluation of the HSE Workshop Series are as follows: (a) workshop staff were trained to use titles of respect (eg, Mr, Mrs/Ms) when talking with workshop participants unless otherwise specified by the participants; (b) the workshop series was held in a community-based setting near where most participants lived; (c) Spanish language discussion sessions were available for individuals who preferred to speak in Spanish; (d) a diversity of foods were served that represented the various cultural backgrounds of the participants; (e) data collected to evaluate workshop effects were coded to assure participant confidentiality; (f) culturally diverse community members similar to the workshop participants were involved in all aspects of the workshop series, including as consultants, presenters, panelists, data collectors, and food servers; and (g) the workshop staff and health care providers who helped implement the workshops series were culturally diverse (eg, diverse in age, gender, and race/ethnicity).
Study Purpose and Hypotheses
The purpose of the present study was to use an intervention–control group design to test the effects of the HSE Workshop Series on the health behaviors/lifestyles and health status indicators of a culturally diverse sample of overweight or obese adults, the majority of whom were from low-income households. The specific study hypotheses are as follows:
Method
Participants
The present study was approved by the institutional review board of the participating university. Participant inclusion criteria for the present study were as follows: (a) being overweight or obese (ie, having a BMI ≥25 kg/m2); (b) being at least 18 years old; and (c) being able to read and write in English or Spanish and to verbally understand English. Participant exclusion criteria was self-reported pregnancy, having diabetes, or having an eating disorder.
A total of 352 adults were initially recruited; however, only 153 participants actually met study inclusion criteria and provided the needed assessment data to be a study participant. These 153 participants included 100 IT group participants and 53 WC group participants who together, ranged in age from 19 to 85 years (M = 43 years, SD = 13.39). There were 111 (72.5%) female participants and 42 (27.5%) male participants. Sixty-one (39.9%) participants self-identified as European American/non-Hispanic White, 57 (37.3%) self-identified as African American/Black, 16 (10.5%) self-identified as Hispanic/Latino(a), 13 (8.5%) self-identified as Asian American, 5 (3.3%) self-identified as “other,” and 1 (0.7%) did not self-identify as any race/ethnicity.
The reported median annual household income range was $25 000 to $29 900. The majority of participants (58.8%) reported an annual household income of $40 000 or less, indicating a low-income skewed sample. Nearly half (48%) of the participants were racial/ethnic minorities and reported a household income at or less than $24 900.
Instruments
The assessment battery (AB) was available in Spanish or English and the instruments in it were counterbalanced to reduce order effects. Below are descriptions of these instruments.
Demographic Data Questionnaire (DDQ)
The DDQ included questions to obtain participants’ self-reported age, race/ethnicity, gender, and annual household income range.
Motivators of and Barriers to Health-Smart Behaviors Inventory (MB-HSBI)
The MB-HSBI 15 assesses the extent to which certain variables are motivators of or barriers to engaging in 4 health promoting behaviors, called health-smart behaviors (HSBs), using a 4-point scale ranging from 1 (strongly disagree) to 4 (strongly agree). These 4 HSBs constitute the four domains of the MB-HSBI and are as follows: (a) eating a healthy breakfast, (b) eating healthy foods and snacks, (c) drinking water and other healthy drinks, and (d) engaging in physical activity. For each of these 4 HSB domains, there is a motivators scale, which assesses level of agreement that the listed variables/items serve as motivators to engage in that HSB, and a barriers scale, which assesses level of agreement that the listed variables/items serve as barriers to engaging in that HSB. Thus, the MB-HSBI has 4 motivators scales and 4 barriers scales.
Scores on the MB-HSBI in the present study produced good internal consistency coefficients for the 4 motivators scales (.93-.96) and the 4 barriers scales (.88-.97). The published article on the development and validation of the MB-HSBI reports that scores derived from the 8 scales demonstrated adequate internal consistencies (ie, Cronbach’s coefficient αs ranged from .78 to .92) and adequate concurrent validity. 15
Health-Promoting Lifestyles Profile–II (HPLP-II)
The HPLP-II7,16 is a 52-item self-report inventory that measures level of engagement in an overall health promoting lifestyle. It has 6 subscales; however, only the health responsibility, physical activity, and nutrition subscales were used in the present study. On each of these 3 subscales, respondents rate the frequency with which each item/behavior occurs, using a 4-point scale ranging from 1 (never) to 4 (routinely).
The subscale scores on the HPLP-II demonstrated good reliability in the present study, with Cronbach’s αs of .866 (Health Responsibility), .853 (Physical Activity), and .855 (Nutrition). The authors of the HPLP-II have reported that the Cronbach’s αs for its subscales range from .793 to .872, the 3-week test–retest reliability for its total scale is .892, and it has acceptable construct validity. 16
Block Fat–Sugar–Fruit–Vegetable Screener (BFSFV Screener)
This instrument is a shortened version of the full-length Block Food Frequency Questionnaire. 17 The BFSFV Screener is a 50-item self-administered diet history questionnaire used to assess an individual’s nutrient intake. It includes a wide range of foods and drinks and asks respondents to indicate how frequently (ie, how many days per week) they eat each type of food and drink. Responses are recorded on a 6-point scale ranging from 1 (none or less than 1 per day) to 6 (every day). For 32 of the items, respondents also indicate how much of the specific food or drink they usually consume in a given day; a 3-point scale is used that describes number of portions/portion size (eg, for sodas, “1 glass/can, 2 glasses/cans, or 3 glasses/cans;” for fish, “2 ounces, 4 ounces, or 6 ounces”).
The BFSFV Screener produces several nutrient scores, including (a) caloric intake, (b) total fat intake, (c) saturated fat intake, (d) trans fat intake, (e) sugar intake, and (f) fruit and vegetable intake. Nutrient estimates are calculated by multiplying frequency, portion size, and nutrient content, and summing over foods. The BFSFV Screener has been reported to have good test–retest correlations (ranging from .59 to .79) and acceptable predictive validities (ranging from .43 to .68). 18
Body Mass Index and Blood Pressure
Each participant’s BMI was determined using the following standard BMI assessment formula: weight (lbs)/ height2 (in) × 703. 1 Each participant’s systolic and diastolic blood pressure was measured by individuals (eg, nurses) trained to do so.
Procedure
Participant Recruitment
Culturally diverse academic researchers and community members recruited participants from 2 small cities in the Southeastern United States that are close in proximity and similar with regard to demographics, including socioeconomic characteristics and the prevalence of obesity. Participants for the IT group were recruited from one city, and participants for the WC group were recruited from the other city, in order to decrease the likelihood of the potential confound of IT group members sharing intervention information with WC group members. Recruitment methods used were in-person recruitment and the dissemination of flyers at various community sites (eg, supermarkets and churches) and activities (eg, festivals) in low-income communities.
Pre-HSE Workshop Series Screening of Potential Participants, Selection of Participants, and Baseline Data Collection
A total of 352 adults across both cities were recruited; however, only 195 of these individuals became potential participants by attending one of the participant screening sessions held in their city to determine if they met the criteria for study participation. Screening sessions occurred at neighborhood schools and/or community centers in each participating city and were co-conducted by the earlier mentioned culturally diverse team of academic researchers and community members. At these sessions, potential participants completed informed consent procedures and a demographic data questionnaire, and had their height, weight, and blood pressure taken to determine if they met criteria for participating in the study.
Of the 195 potential participants, 190 met study criteria and thus became study participants. Of this 190 study participants, 115 were in the IT group and 75 were in the WC group. Study participants in both groups completed the MB-HSBI and were given the remainder of the pre-HSE Workshop Series (baseline) assessment battery (AB) to complete at home. Participants in the IT group returned the completed AB at the first HSE Workshop Series session, and participants in the WC group returned their completed AB during scheduled drop-off dates and times at designated community locations. WC group participants were informed that they would participate in a version of the HSE Workshop Series in approximately 6 months following completion of the baseline AB. Of the 190 enrolled participants, only 153 (100 out of 115 enrolled IT group participants, and 53 out of the 75 enrolled WC group participants) provided the necessary participation and data to be considered actual study participants whose data were analyzed to test the hypotheses set forth in this study. Thus, the participation rate was 80.5% (ie, 86.9% for the IT group; 70.7% for the WC group).
The pre-HSE Workshop Series screening and data collection phase lasted 2 months. However, BMI and blood pressure data were obtained again just prior to the first workshop in order to have reliable baseline measures of these variables. All participants received $25 immediately after providing their (baseline) health indicator data and measures. Potential participants who did not meet the study participation criteria were paid $10 for their participant screening time.
HSE Workshop Series to Modify and Prevent Obesity
Immediately following the 2-month baseline data collection period, the IT group participants began participating in the HSE Workshop Series, which consisted of three 4-hour workshops. These workshops, which occurred 2 weeks apart at a local community facility, were co-led by workshop staff that included community members, academic health researchers, and health care providers (physicians, psychologists, nurses, nutritionists/dietitians, and physical fitness experts). Given the racial/ethnic diversity among workshop participants, researchers ensured that workshop staff members were also diverse with regard to race/ethnicity and cultural background.
The HSE Workshop Series used the tenants of HSE theory (ie, health motivation, health self-efficacy, self-praise of health promoting behaviors, active coping styles/skills for managing emotions, and health responsibility) to inform educational, motivational, empowerment-focused, and cognitive–behavioral strategies to (a) increase the motivators of and decrease the barriers to health promoting behaviors (called health-smart behaviors; HSBs), (b) increase levels of engagement in HSBs, and (c) improve management of stress and depression. The target HSBs included (a) eating a healthy breakfast each day; (b) eating fruits and vegetables each day; (c) eating whole grains each day; (d) drinking water and other beverages low in sugar; (e) eating healthy foods and snacks that are low in fat, sugar, sodium, and calories; (f) moving and walking rather than engaging in sedentary activities; (g) engaging in moderate-to-intense physical activity each day; and (h) restricting screen time (ie, television/video/computer time) for pleasure to no more than 2 hours per day.
To promote each workshop participant’s health motivation, an individualized coaching session was conducted during the first workshop. In this session, a workshop staff member reviewed a participant’s top motivators and barriers (as indicated on the participant’s baseline completion of the Motivators of and Barriers to Health-Smart Behavior Inventory) and then, based on this inventory data, encouraged the participant to identify and commit to 2 attainable HSB goals (eg, using a pedometer to measure and increase one’s total number of steps walked each day by 20 steps). Based on the participant’s motivators data, realistic strategies for achieving these goals (eg, have a family member be a walking partner) were also identified by the participant, with assistance provided by a workshop staff member as desired.
Additionally, in the first workshop, staff members gave informative and motivational presentations on the various HSBs. Following each presentation small group discussion sessions occurred in which 8 to 10 participants shared personal barriers to engaging in the HSBs, and participants as well as workshop staff members shared strategies for overcoming these barriers.
In the second workshop each participant received a Health-Smart Behavior Resource Guide that consisted of documents at low-to-moderate literacy levels. This guide included (a) tips for increasing and sustaining each of the HSBs (eg, how to incorporate whole-grain foods into one’s diet, and how to read food labels when shopping); (b) tools to foster the occurrence of HSBs (e.g., a chart for recording daily screen time, and a picture guide of basic exercises that can be done at home and without equipment); and (c) tips for identifying and managing stress, depression, and anger. Components of this guide were presented, and participants engaged in small group sessions to discuss ways of incorporating the various resources and strategies into their own lives.
In the third workshop, the following activities occurred: (a) sessions for practicing self-praise of HSBs (eg, I am proud of myself for achieving my walking goal today) and HSB-related self-talk (eg, telling one’s self that I am worthy of taking the time to exercise and to take care of my physical and mental health) with the aim of motivating and sustaining HSBs; (b) sessions involving demonstrating and practicing practical strategies for managing the stress and depression that may impede engagement in HSBs (eg, practicing how to say no, and how to constructively express negative and positive feelings); and (c) an interactive session on easy-to-learn exercises that do not require equipment, including exercises for individuals with limited mobility.
At the end of each of each workshop, a question and answer session was held in which a culturally diverse panel of health care professionals responded to anonymous or direct questions from workshop participants. These questions typically addressed chronic diseases and the health promoting behaviors that could prevent or minimize the negative effects of these diseases. Workshop participants each received $25 for workshop series travel expenses.
Post-Workshop Data Collection
At the end of the third and final workshop session, participants in the IT group were given the AB to complete again at home. Participants in the WC Group were mailed this AB to complete again at home. BMI and blood pressure data of participants in both the IT group and the WC group were collected at any one of several sessions scheduled approximately 3 weeks after the final workshop, where participants also returned their completed ABs. Participants in both groups received $30 for providing this follow-up data. After data collection was complete, a HSE Workshop was implemented with participants in the WC group.
Results
Workshop Attendance
Of the 100 participants in the IT group, 56 (56%) participants attended all three 4-hour workshops. Twenty-seven (27%) participants attended only 2 workshops, and 17 (17%) attended only 1 workshop.
Impact of the HSE Workshop Series on Health Promoting Lifestyle
To evaluate the impact of the HSE Workshop Series on specific aspects of a health promoting lifestyle (ie, Physical Activity, Nutrition, and Health Responsibility subscales of the HPLP-II), we conducted a 2 (group: IT vs WC) by 2 (time: pre-intervention and post-intervention) repeated-measures multivariate analysis of variance (MANOVA) with physical exercise, healthy eating, and health responsibility as the 3 dependent variables. Results showed a significant time by group interaction, F(3, 138) = 10.41, P < .001. Post hoc analyses using Bonferroni correction for multiple comparisons indicated that the IT group and the WC group did not differ at pre-intervention on levels of physical exercise, healthy eating, or health responsibility. However, at post-intervention, the IT group showed significantly higher engagement in physical exercise (P < .001) and healthy eating (P < .001) when compared with the WC group. No group difference was found in health responsibility at post-intervention. See Table 1 for group means.
Pre- and Post-HSE Workshop Series Intervention Changes in Study Variables by Group
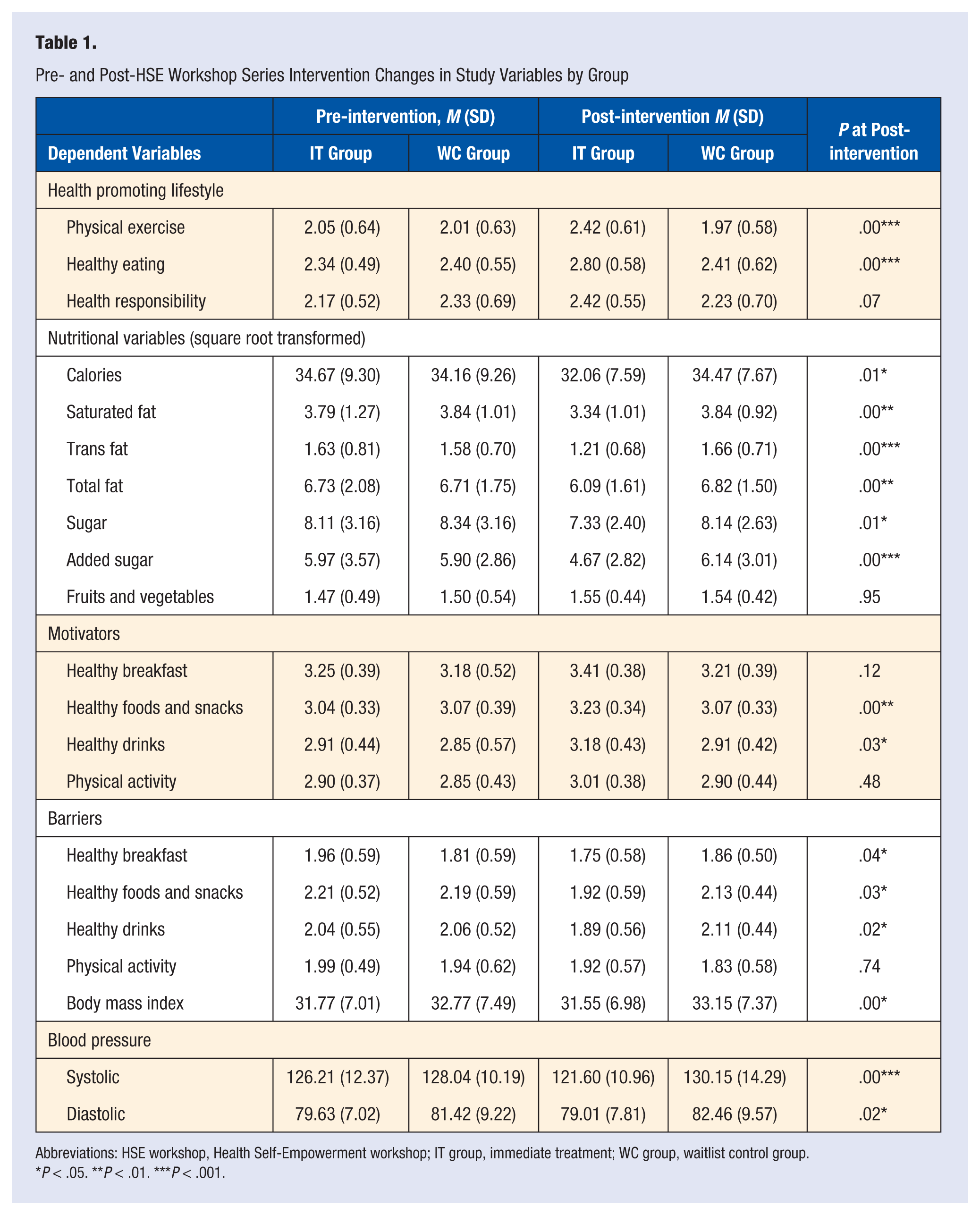
Abbreviations: HSE workshop, Health Self-Empowerment workshop; IT group, immediate treatment; WC group, waitlist control group.
P < .05. **P < .01. ***P < .001.
Impact of the HSE Workshop Series on Caloric, Fat, Sugar, Fruit, and Vegetable Intake
Prior to conducting analyses using the nutrition-related variables (ie, calories, saturated fat, trans fat, total fat, sugar, added sugar, and fruits and vegetables, as measured by the BSFSV Screener), these variables were transformed using a square root transformation due to violating assumptions of normality. Because there were significant group differences at baseline for these nutrition variables, we conducted a multivariate analysis of covariance (MANCOVA) to evaluate the impact of the workshop series intervention on these variables. In the MANCOVA, pre-intervention scores for each of the nutrition related variables were included as covariates, and post-intervention scores were the dependent variables. The group effect was significant, F(7, 116) = 3.91, P < .01. That is, at post-intervention, adults in the IT group consumed significantly less calories, total fat, trans fat, saturated fat, sugar, and added sugar than adults in the WC group. However, no group differences were found for fruit and vegetable intake. Mean scores for the IT group and the WC group on all these nutrition-related dependent variables at pre-intervention and post-intervention are shown in Table 1.
Impact of HSE Workshop Series on Motivators of and Barriers to Engaging in Health-Smart Behaviors
To evaluate the effects of the HSE Workshop Series on levels of motivation to engage in HSBs, we conducted 4 repeated-measures analyses of variance (ANOVAs), using the score on 1 of the 4 HSB domains (ie, eating a healthy breakfast, eating healthy foods and snacks, drinking water and other healthy drinks, and engaging in physical activity) of the Motivators of and Barriers to Health-Smart Behaviors Inventory (MB-HSBI) as the dependent variable in each ANOVA. Results demonstrated significant time by group interactions for (a) motivation to engage in eating healthy foods and snacks, F(1, 74) = 9.56, P < .01, and (b) motivation to engage in drinking water and other healthy drinks, F(1, 72) = 5.12, P < .05. Overall, these results demonstrate that individuals in the IT group showed greater increases in levels of motivation to engage in (a) eating healthy foods and snacks and (b) drinking water and other healthy drinks from pre-intervention to post-intervention, as compared with individuals in the WC group. The group by time interactions for motivation to engage in physical activity and eating a healthy breakfast were not significant (see Table 1 for means and standard deviations).
To evaluate the effects of the intervention on levels of barriers to engaging in HSBs, we conducted 4 more repeated-measures ANOVAs. Results showed a significant time by group interaction for (a) barriers to eating a healthy breakfast, F(1, 66) = 4.41, P < .05; (b) barriers to eating healthy foods and snacks, F(1, 72) = 5.24, P <.05; and (c) barriers to drinking water and other healthy drinks, F(1, 72) = 5.35, P < .05. Overall, individuals in the IT group showed greater decreases in levels of barriers to eating healthy foods and snacks, eating a healthy breakfast, and drinking water and other healthy drinks from pre-intervention to post-intervention compared to the WC group. The group by time interaction for barriers to engaging in physical activity was not significant (see Table 1 for means and standard deviations).
Impact of HSE Workshop Series on Body Mass Index and Blood Pressure
A repeated-measures ANOVA was conducted to examine the impact of the HSE Workshop Series on BMI. Results indicated a significant time by group interaction for BMI, F(1, 134) = 10.90, P < .01. This finding indicates that adults in the IT group showed significant decreases in BMI from pre-intervention to post-intervention compared to the WC group (see Table 1 for means and standard deviations).
To evaluate the impact of the HSE Workshop Series on blood pressure, we conducted a 2 (group: IT vs WC) by 2 (time: pre-intervention and post-intervention) repeated-measures MANOVA with systolic blood pressure and diastolic blood pressure as the 2 dependent variables. Box’s M test was significant, F(10, 42530.45) = 3.22, P < .001, indicating that the assumption of equal covariances was not met. Thus, degrees of freedom were corrected using Wilks’s lambda estimates. Results showed a significant time by group interaction, F(2, 141) = 6.27, P < .01. Post hoc analyses using Bonferroni correction for multiple comparisons indicated that the IT group and the WC group did not differ at pre-HSE Workshop Series intervention on levels of systolic and diastolic blood pressure. However, the IT group showed significantly lower systolic blood pressure at post-intervention compared with the WC group. Additionally, an unexpected pre-intervention to post-intervention group difference was found for diastolic blood pressure, in that there was a significant increase in diastolic blood pressure in the WC group but no significant change in diastolic blood pressure in the IT group (see Table 1 for group means and standard deviations).
Discussion
The results of this study suggest that the tested HSE theory–based, culturally sensitive HSE Workshop Series has much potential for improving health indicators (ie, BMI and systolic blood pressure) and increasing self-reported health promoting lifestyle behaviors among culturally diverse adults who are overweight or obese, particularly for adults with low household incomes. Specifically, it was found that at 3 weeks following the HSE Workshop Series (ie, post-intervention), the adults who participated in the HSE Workshop Series (the IT group) as compared with the adults in the WC group showed significantly higher engagement in physical activity (P < .05) and healthy eating (P < .01) but not in health responsibility. These findings provide partial support for hypothesis 1. It was also found that at post-intervention, adults in the IT group as compared with adults in the WC group consumed significantly less calories, total fat, trans fat, saturated fat, sugar, and added sugar. No significant group differences were found for fruit and vegetable intake. These findings provide partial support for hypothesis 2.
Additionally, it was found that from pre-intervention to post-intervention, adults who were in the IT group as compared with the adults in the WC group showed significantly greater increases in levels of motivation to eat healthy foods and snacks and drink water and other healthy drinks, but no significant changes in levels of motivation to eat a healthy breakfast and engage in physical activity. Furthermore, adults who were in the IT group as compared with the adults in the WC group showed significantly greater decreases in levels of barriers to eating healthy foods and snacks, eating a healthy breakfast, and drinking water and other healthy drinks. No significant changes were found in levels of barriers to engaging in physical activity. These motivator- and barrier-related findings provide partial support for hypothesis 3.
Finally, it was found that at post-intervention, adults in the IT group as compared with adults in the WC group showed significantly greater decreases in BMI and systolic blood pressure. Unexpectedly, at post-intervention, a significant increase in diastolic blood pressure was found among adults in the WC group, but this increase did not occur among adults in the IT group. The cause of this unexpected increase in diastolic blood pressure among participants in the WC group is not known; however, it could be that individuals waiting to begin the program experienced an increase in unhealthy behaviors while waiting (ie, similar to the phenomenon of knowingly overeating during the winter holidays, while simultaneously planning to start a diet at the beginning of the new year). The findings related to BMI and blood pressure provide partial support of hypothesis 4.
Together, findings from this study provide support for future research to test the efficacy of the HSE Workshop Series for health promotion and obesity prevention/intervention, particularly among individuals who are more likely to experience low socioeconomic power. It is important that such future research includes a long-term follow-up period and randomly selected participants. The finding that some of the investigated motivators of and barriers to health-smart behaviors (health promoting behaviors) that can prevent and modify obesity increased and decreased, respectively, from pre-intervention to post-intervention might suggest that clinically significant decreases in BMI and systolic blood pressure may be found over a longer follow-up period (eg, 1 year).
The finding of no significant group differences in perceived health responsibility from pre-intervention to post-intervention was not expected. This finding may be because the participants in this study likely experienced intractable economic and environmental factors that limited changes in perceived personal responsibility for their own health.
The finding of no significant group differences in fruit and vegetable intake from pre-intervention to post-intervention may be explained by the high cost of these foods, which may have deterred participants in the IT group from purchasing these foods even if motivated to eat them. Additionally, fresh fruits and vegetables are not routinely available in many low-income communities.
The finding of no significant changes in levels of motivation to eat a healthy breakfast was surprising. An explanation of this finding may be that the cultural influences on the determinants of what is eaten for breakfast may impede motivation to eat a healthy breakfast. Additionally, many individuals who do not regularly eat breakfast find making this change to be particularly challenging.
The findings of no statistically significant changes from pre-intervention to post-intervention in reported levels of motivation and levels of barriers in relation to engaging in physical activity are also noteworthy. Given that most of the participants in this study were from low-income communities, these findings could be linked to the existence of environmental barriers to physical activity in such communities, such as lack of safe areas for walking and biking. 19
Notably, this study used data from each participant’s completed MB-HSBI to customize the goal setting for that participant. Given the important role of goal setting in promoting motivation to engage in desirable behaviors HSBs, 20 research is needed to evaluate the independent effects of this inventory-based customized goal-setting approach. Results of the present study also suggest that health care providers (physicians, psychologists, nurses, dietitians, nutritionists, and physical fitness experts) can play major roles in low-income community-based/partnered health promotion interventions such as the HSE Workshop Series. Specifically, health care providers can contribute by advocating for such programs and by answering anonymous questions from program participants (eg, patients and future patients) that these individuals are often too anxious to ask or never have the chance to ask. Because physicians (like pastors) hold much status and authority among members of low-income communities and the medically underserved, a small amount of time from these physicians to answer anonymous health-related questions from such community members has much potential for promoting health knowledge and health promoting behaviors among these community members.
It is also noteworthy that participation of physicians and other health care providers in the HSE Workshop Series appeared to facilitate the workshop participants’ comfort level with these providers, particularly among the racial/ethnic minority participants. Specifically, by the second workshop the racial/ethnic minority participants had generally moved from asking questions to providers anonymously to directly asking these questions. Furthermore, most of the participants reported in their workshop evaluations that the panel sessions with providers were the most helpful parts of the HSE Workshop Series. The providers, including physicians, who participated in the panel sessions reported that their experience as panel members made them increasingly aware of the kinds of questions they need to address with their patients in order to effectively promote their health.
Importantly, cultural sensitivity (as indicated by having knowledge, skills, experience, and awareness to promote health among culturally diverse individuals and displaying these competencies in ways that enable these individuals to feel comfortable, trusting, and respected in the health promotion process) was conveyed in the content and implementation of the HSE Workshop Series. Because of the small number of participants in each racial/ethnic minority group and in the non-English preference group in the present study, the data analyses to assess the impact of participating in the HSE Workshop Series were not conducted separately by racial/ethnic group and by language preference as would be ideal to show respect for cultural differences in these analyses. In future similar studies to the present study, efforts should be made to have larger samples of different racial/ethnic groups and non-English preference groups so that such a culturally sensitive data analysis approach can be used.
Though the exact influence of cultural sensitivity in the content and implementation of the HSE Workshop Series on the findings in the present study cannot be empirically assessed, there are several indicators of this influence. For example, the participants in the workshop series actively participated in the discussion sessions as informal teachers and learners, which suggests that they were comfortable in these roles. Additionally, some participants in the discussion groups shared very personal information regarding their efforts to cope with stress and depression and their motivators of and barriers to engaging in health promoting behaviors. Such personal sharing can be linked to the skills of the workshop leaders for promoting trust among the workshop participants. These skills include listening to the preferences and concerns of the workshop participants and being supportively responsive to both, as well as encouraging group confidentiality and modeling personal sharing.
It is also noteworthy that many participants in the workshop series provided unsolicited feedback to the researchers regarding the fact that they learned a lot about healthy eating and exercising without being made to feel stupid. These participants also reported finding the practice exercises and training demonstrations interesting, informative, and fun. Additionally, these participants stated that they felt respected by the way they were addressed (eg, Mr, Ms, Sir) and by the culture-informed food that was served and the music and dances (eg, salsa) used in the physical activity training sessions. Nearly all participants in the workshop series voluntarily commented on the respect they felt during the individual coaching in that they were encouraged to choose their own health promotion goals and strategies for overcoming them based on their identified motivators and barriers to health promoting behaviors.
The aforementioned observations and feedback indicating links between cultural sensitivity of the workshop series and the effectiveness of this intervention have some implications for culturally sensitive health promotion by primary care physicians and other health care providers within health care settings. Specifically, providers can prompt individuals to self-identify motivators of and barriers to health behaviors and strategies to overcome the identified barriers, elicit and acknowledge cultural traditions that affect health promoting behaviors, include visual materials to deliver health information, and emphasize culturally congruent benefits of engaging in health promoting behaviors (eg, to promote health status instead of to lose weight).
Additional strategies for providers to convey cultural sensitivity include ensuring that services and interventions are delivered in the preferred language of their patients, consulting with providers of the same cultural background as their patients, and periodically delivering preventative care or health promotion interventions near where individuals live such as in churches and community centers. Physicians and other health care providers can also invite their patients to submit questions about their health and health problems by e-mail or a secure question box prior to and following their health care visit. Finally, health care providers can host sessions periodically (eg, bimonthly) to answer health-related questions from their patients and community members and to provide an opportunity for participating patients and community members to learn health promotion strategies from each other.
Though informative and important, the present study has some limitations. First, self-report measures were used to assess all of the investigated variables except BMI and blood pressure, which were objectively assessed by individuals trained to do so. Use of more objective measures of HSBs (eg, use of pedometers) should be used in future similar studies.
Second, participants in the IT group and those in the WC group were in different cities to avoid the potential contamination of sharing intervention information across groups. It is important that future studies to test the HSE Workshop Series occur in large cities with multiple low-income communities so that these communities can be assigned to an intervention or control group using a cluster randomization approach.
Third, although this study involved a primarily low-income adult sample by targeting participant recruitments in low-income communities, having a low-income was not an inclusion criterion for study participation; thus, it is not possible to generalize the findings from this study to overweight or obese persons from low-income households. Researchers chose not to use “low-income” as a study inclusion criterion because of input from community member consultants that this criterion would likely be viewed negatively by members from the target communities and may act as a deterrent to study participation.
Fourth, this study lacked a measurement of stress and depression and did not assess some of the HSE theory variables (specifically, health self-efficacy, self-praise, and coping skills for managing stress and depression). Measurement of these variables in future similar research is needed to validate our assumption that the components of HSE theory contributed to the found positive changes in the investigated HSBs, motivators and barriers, nutrition variables, and health status variables.
Given the above-specified limitations, the findings of this study must be considered preliminary and interpreted with caution. Yet these preliminary findings and the many strengths of this study suggest that it is an important study that can and should guide future clinical research on treating and preventing overweight/obesity. These study strengths include that the participant sample was comprised of a large percentage of individuals with low household incomes and individuals who are racial/ethnic minorities—persons often underrepresented in health research.
Additionally, the tested HSE Workshop Series is anchored in an empowerment-oriented theory (ie, HSE theory) and is culturally sensitive. Such an intervention seems appropriate for further investigation with groups most negatively affected by overweight/obesity and related health disparities—groups such as racial/ethnic minorities and the medically underserved. Such groups often experience low perceived and/or actual power over their health and their level of engagement in health promoting behaviors for overcoming and preventing obesity.
Finally, a major strength of this study is its inclusion of health care providers (physicians, nurses, psychologists, nutritionists, dietitians, and physical fitness experts), community members, and academic researchers as partners in the implementation and evaluation of the HSE Workshop Series. Support for this view comes from comments by workshop participants on the evaluations of this HSE Workshop Series that one of the most important aspects of this intervention was participation in it by physicians in particular and health care providers in general. Clearly, health care providers can play important roles in treating and preventing obesity that go beyond medical/clinical settings and their traditional health care roles. These nontraditional roles include promoting health literacy and/or health empowerment in low-income communities to help prevent/treat overweight/obesity among the members of these communities.
It is also noteworthy that workshop participants additionally identified the following components of the HSE Workshop Series as particularly helpful: (a) group discussions in which participants had the opportunity to share their barriers to HSBs and strategies found to be effective in addressing these barriers, (b) individual goal setting that was realistic for their personal life conditions, and (c) learning strategies from psychologists for self-managing their stress and depression. This feedback further suggests that empowering individuals to take charge of their own health and HSBs may be an effective approach in future interventions designed to address overweight/obesity among individuals from low-income communities.
It is also important to note that the present study has an important implication for future studies of health promotion interventions with culturally diverse adults who are overweight or obese. Specifically, the present study suggests that future studies of health promotion interventions to address overweight/obesity should explicitly include and further examine the benefit of culturally sensitive content and implementation strategies in these interventions. Researchers who implement these studies can pay closer attention to the cultural sensitivity of the content and implementation of interventions tested in their studies by including culturally diverse adults who are overweight or obese as research partners in all study phases, including the development of intervention content and implementation phase. It is also helpful for the researchers and their partners to be culturally diverse. Additionally, researchers should ideally learn more about the culture and living environments of the target participants before designing any intervention study or other study to address obesity or other health problem among these participants. Researchers can achieve this learning by participating in activities in the environment where target participants (eg, target culturally diverse adult overweight or obese adults) live and doing so over months rather than a few days.
The present study is particularly significant in that it advances theory, research, and practice in the health promotion field. It advances theory in this field by providing the needed groundwork to establish the utility of HSE theory for developing health promotion interventions to modify and prevent obesity among minority and low-income groups. This study also fosters the development and testing of such health empowerment theories through research that includes large samples of racial/ethnic minorities and individuals with low incomes—individuals who experience real and/or perceived limited control over their health and over many other aspects of their lives. Such individuals likely need health empowerment oriented interventions to overcome obesity and related diseases.
This study advances research in the area of health promotion by demonstrating culturally sensitive participant recruitment, data collection, and intervention research strategies. These strategies include involving community members as co-researchers throughout all aspects of the research process.
This study advances the practice of health promotion by demonstrating how health care providers can be integrated into community-based health promotion interventions aimed at promoting health and reducing obesity/overweight in racial/ethnic minority and low-income communities. Such integration of health care providers into community-based health promotion interventions can help foster deinstitutionalization of health care and health promotion and help make these interventions accessible to racial/ethnic minorities and individuals with low-incomes—groups that typically underutilize health care institutions.
Footnotes
Acknowledgements
We express our gratitude to members of the University of Florida Health Psychology and Behavioral Medicine research teams, and to the various health professionals who contributed to the intervention tested in this research, including but not limited to Dr Mary B. Smith, Mrs Cynthia Filer, Dr Freddy Kaye, Mrs Jennifer Bleiweis, Mrs Mabelissa Acevedo, Ms Shelly Baric, Ms Stephanie Pollard, Mrs Vivian Filer, and the Black Nurses Association of Gainesville, Florida.
This research was funded by a grant from the PepsiCo Foundation.