
Abstract
“In these settings, optimizing function as well as physical, emotional, and spiritual well-being become the driving factors in clinical decision making.”
Introduction
Clinicians, patients, and caregivers are continuously seeking ways to improve quality of life (QOL) and symptom management in patients receiving palliative or hospice care.1,2 Lifestyle interventions 3 have the potential to play a critical role in meeting these needs because they can confer health benefits as well as serve to empower a patient during what could be a particularly distressing time in that person’s life. However, attempting to implement lifestyle interventions in this vulnerable and usually frail population also has the potential to lead to feelings of guilt, inadequacy, and failure, which can worsen QOL. 4 Additionally, in settings in which prolongation of life may no longer be the primary goal, it is important that lifestyle recommendations be carefully tailored to the individual patient’s stage of illness, needs, and specific goals. In these settings, optimizing function as well as physical, emotional, and spiritual well-being become the driving factors in clinical decision making. 2
Whereas it is clear that lifestyle medicine can play an important role in the care of patients receiving palliative care, research on interventions in this particular patient population is somewhat limited, likely because of the physical and emotional vulnerability of these patients. The goal of this review is to determine the current state of research and expert recommendations regarding lifestyle medicine interventions in palliative care and hospice patients. Although palliative care interventions can be applied throughout the full spectrum of a patient’s illness, from early to late disease, 1 for the purposes of this review, we will focus on the subset of patients with advanced or end-stage disease, with associated limited life expectancy, who are receiving palliative or hospice care.
Methods
Initial Review and Establishing Scope
Two authors (GA, HAM) scanned the literature to assess the scope of research specific to lifestyle interventions in patients with advanced or end-stage disease receiving palliative or hospice care. Four main topic categories emerged: physical activity, nutrition, stress reduction, and substance use reduction. Given the relative paucity of studies specific to patients with limited life expectancy, our review question remained broad, and we decided to use a wide search strategy, including quantitative and qualitative studies, descriptive reports, reviews, and practice guidelines, to capture as much of the clinically relevant literature as possible.
Literature Search
Four authors (HAM, GR, JG, TH) then embarked on a comprehensive literature search, each taking 1 of the 4 main categories identified in the initial scan. One author (GA) did a brief independent search to make sure no significant articles were omitted.
Search Parameters
Patient population
Palliative care patients were defined as patients with advanced stage disease (including, but not limited, to hospice patients). Initial search terms included “palliative care,” “serious illness,” “advanced illness,” “advanced disease,” and “hospice” alone or in conjunction with a variety of specific diseases: for example, “cancer,” “COPD,” “end-stage lung (or pulmonary) disease,” “end-stage cardiac (or heart) disease,” “end-stage renal disease,” “Alzheimers disease”).
Lifestyle intervention
Each of the above terms was searched in conjunction with a specific lifestyle intervention category. For exercise, initial search terms included “exercise,” “physical activity,” “rehabilitation,” “cardiac rehabilitation,” and “pulmonary rehabilitation.” For nutrition, terms included: “diet,” “diet modification,” “nutrition,” and “nutrition support.” For stress management, terms included “stress management,” “stress reduction,” “mindfulness,” “yoga,” “meditation,” “music therapy,” “spiritual practice,” “prayer,” and “support.” For substance use, initial search terms included “tobacco use,” “smoking cessation,” “alcohol,” “alcohol rehabilitation,” “opioid dependence,” and “opioid misuse.”
Search locations
Our search began with the search engines PubMed and Google Scholar. Given our goal of achieving a comprehensive search, we then used a snowballing search strategy utilizing initial articles to find additional pertinent articles (eg, in reference lists and gray literature).
Inclusion and Exclusion Criteria
Each section author reviewed abstracts of articles found through this search method and focused on articles that discussed advanced palliative care patient populations and at least 1 form of lifestyle medicine intervention.
Narrative Review
Four authors (HAM, GR, JG, TH) each organized and wrote a cogent narrative of literature review findings for each main topic section, including relevant information from studies, reviews, and expert recommendations. One author (GA) briefly reviewed all articles and wrote and/or edited all sections of the manuscript focusing on clinical relevance. Two authors (GA and GR) critically reviewed the entire manuscript for accuracy and clinical relevance. All authors reviewed, edited, and approved the final manuscript for submission.
Results
General Findings
Several themes emerged from this literature review that highlighted the unique needs and challenges encountered by patients with advanced disease and/or limited prognoses, who are considering lifestyle interventions.
Relative Paucity of Well-Conducted Studies
Although numerous articles exist regarding the vast array of lifestyle interventions that have been proposed for this population, many are opinion pieces, and existing studies are fraught with multiple challenges, including small sample sizes, inconsistent definitions, and lack of control groups. Additionally, studies regarding patients receiving palliative care are at more risk of patients withdrawing from the study because of disease progression.4,5 Patients with advanced cancer are the most studied group, but even studies in this group vary by type and stage of the cancer. Expert opinion consensus reports of lifestyle interventions are rare in this population.
Point in Illness Journey May Affect Participation
A common theme throughout this literature is the clear variability in acceptability, feasibility, and effectiveness of lifestyle interventions related to the individual’s illness trajectory and life journey. Patients with advanced disease receiving palliative or hospice care face intense physical, emotional, and spiritual challenges that change as they progress in their disease. Therefore, effectiveness of a lifestyle intervention for a particular patient may vary with time. For example, a study of music interventions found that music preference of individual patients changed at different points in the study. 6
Age, Smoking, and Diagnosis May Affect Participation
Given the small sample size of many studies, it is hard to determine the effects of age, gender, and other variables on participation in lifestyle interventions. One study of 100 patients, newly diagnosed with cancer undergoing a comprehensive lifestyle intervention, demonstrated that cancer type, smoking, and age increased the probability of participant withdrawal from the study. Additionally, patients >70 years old were less likely to participate at baseline and at 4 months. 5 Similarly a qualitative study of palliative cancer patients regarding their experiences participating in lifestyle interventions noted that none were smoking at the time of study inclusion. 4
Importance of Goals-of-Care Conversations
A prominent theme in many articles discussing lifestyle interventions in patients receiving palliative care is the importance of honest goals-of-care conversations with patients and families. Choosing and implementing the most appropriate lifestyle interventions for a particular patient depends heavily on the patient’s and family’s understanding of prognosis, overall goals, and the likelihood that the intervention will positively contribute to QOL and well-being. This is particularly true for nutrition and substance use interventions.7,8
Physical Activity
Physical activity–based interventions aimed at improving QOL in the palliative care setting have been shown to have some success while also having promising effects on secondary related domains, such as improving aerobic capacity, strength, overall physical function, and fatigue. 9
Acceptability and Barriers
There are numerous barriers facing those patients receiving palliative or hospice care who could benefit from physical activity, most commonly related to their attitudes and perceptions regarding these interventions. For example, patients report experiencing feelings of abandonment and disruption to their daily lives brought on by their diagnosis, both of which can dissuade them from seeking physical activity interventions. 10 Despite this, almost two-thirds of patients in a study of 53 patients in an outpatient palliative chemotherapy setting would be receptive to physical activity as a means to improve QOL. 11 Smith et al 12 found that cancer survivors believe that physical activity is good for them, and many desire to be more active. However, they feel discouraged because of limited guidance available regarding appropriate physical activity. Additionally, many patients cite their own health, specifically fatigue and effects of cancer treatments rendering them less physically fit, as reasons why physical activity would not be possible for them, even though it could potentially improve their QOL. 12
Feasibility
Although in some cases it is not possible to deliver exercise-based interventions for patients with advanced illness, in most cases, some form of physical exercise intervention appears feasible. In a study of 572 terminally ill cancer patients, an estimated 92% of patients were able to receive some form of physical exercise or physical therapy intervention. 13 In addition to physical activity, interventions such as breathing therapy, relaxation therapy, and positioning exercises are also achievable in the palliative care population. 13 Although these interventions appear feasible, among patients with cancer, several factors such as age, smoking status, and the type of diagnosis have an impact on the probability that patients will discontinue these interventions. 5
Patients With Advanced Cancer
Quality of life
The primary palliative care population in which physical exercise interventions have been studied is patients with advanced cancer. Palliative treatment incorporating physical activity appears to produce desirable QOL improvements in patients with a variety of advanced stage cancers and limited life expectancy. For patients with hepatocellular cancers, twice-weekly exercise sessions involving maintaining a 60% target heart rate, resulted in higher self-reported QOL scores by patients. 14 In a study measuring the effect of palliative physical activity on the QOL of women with metastatic breast cancer, intervention participants were statistically more likely to be able to complete a Bruce Ramp Treadmill test compared with the control group. 15 One study on patients with colorectal cancer failed to find a link between physical activity and QOL; however, this study measured self-reported physical activity rather than objective effects of a purposeful intervention. 16 Whereas these studies targeted patients with specific cancer diagnoses, others examined interventions on palliative cancer patients with a variety of cancer types.17,18
Fatigue
Therapeutic physical activity has the potential to help reduce symptoms in palliative cancer patients. Of these symptoms, chronic fatigue appears to be the most targeted by exercise intervention studies. A Dutch study utilized a combination of interval aerobic exercise and muscular resistance training to see if fatigue would improve in 26 palliative care patients with advanced cancer. After 6 weeks of this combination intervention, patients reported reduced fatigue, improved QOL, and improvements in physical measures such as muscular strength, maximum walking distance, and reduced body fat percentage. 19 Physical exercise interventions appear effective even when only administered for a short duration. In a Polish study, 30 palliative care patients participated in six 30-minute physical activity sessions over 2 weeks. Patients reported lower fatigue scores after the intervention compared to a control group. 20
Physical and mental functioning
Other studies targeting physical fatigue in cancer patients receiving palliative care do not show a reduction in fatigue but do demonstrate other benefits in physical and mental functioning.17,21 Schuler et al 21 investigated the effect of structured, individual sports programs on fatigue in patients with cancer receiving palliative care. Although there was no significant change in physical fatigue compared with the control group, there was a significant improvement in mental fatigue. Oldervol et al 17 studied an intervention in which 231 palliative cancer patients engaged in supervised exercise for 60 minutes biweekly for 8 weeks, with the intention of improving fatigue. Although they did not see significant improvements in fatigue, the intervention group did have significant improvements in a shuttle-walk test (a standardized endurance test) and in hand grip strength compared with the control group. 17 An earlier, smaller pilot study by Oldervol et al 22 did show significant improvements in both mental and physical fatigue compared with a control group.
A Swiss study on the effects of combined diet and physical activity on QOL for 58 palliative cancer patients diagnosed with metastatic lung and gastrointestinal (GI) cancers in an outpatient setting did not find any significant benefits to overall QOL. However, the intervention did result in significant reductions in patients’ nausea and vomiting, contributing to general well-being. 18
Patients With Alzheimer Disease
Another palliative care population in which physical activity interventions have been studied is patients with Alzheimer disease. Physical activity interventions appear to improve QOL, physical, and psychological well-being in patients with Alzheimer’s.23,24 El-Kader and Al-Jiffri 23 investigated the effects of aerobic treadmill training on 40 elderly Alzheimer patients, with the aim of reducing systemic inflammation, and found that there was a significant improvement in levels of tumor necrosis factor-α and interleukin-6, and in Beck Depression Inventory and SF-36 health QOL scores. 23
Home-based interventions may be effective as well. A study at the University of Arkansas examined the differences between traditional walking-based physical activity interventions and computerized home-based interventions based on the Wii-Fit gaming platform, for Alzheimer patients. This study aimed to determine whether the type of intervention made a difference in QOL and confidence regarding falls. Results showed that the home Wii-fit intervention improved both QOL and fear regarding falls compared with the control group, which engaged in a walking-based exercise intervention. 24
Group Exercise Interventions
Some studies have examined group exercise programs in palliative settings. Patients report positive experiences with group exercise, with palliative care patient interviews showing themes such as mutually supportive relationships with other patients, improved mood, improved coping, and the development of feelings of independence and a return to a better state of physical functioning. 25 Patient interviews also reveal that group exercise can help alleviate the sense of hopelessness that they experience as they enter hospice care, fostering a sense of belonging, which improves their QOL.25,26
Studies in Progress
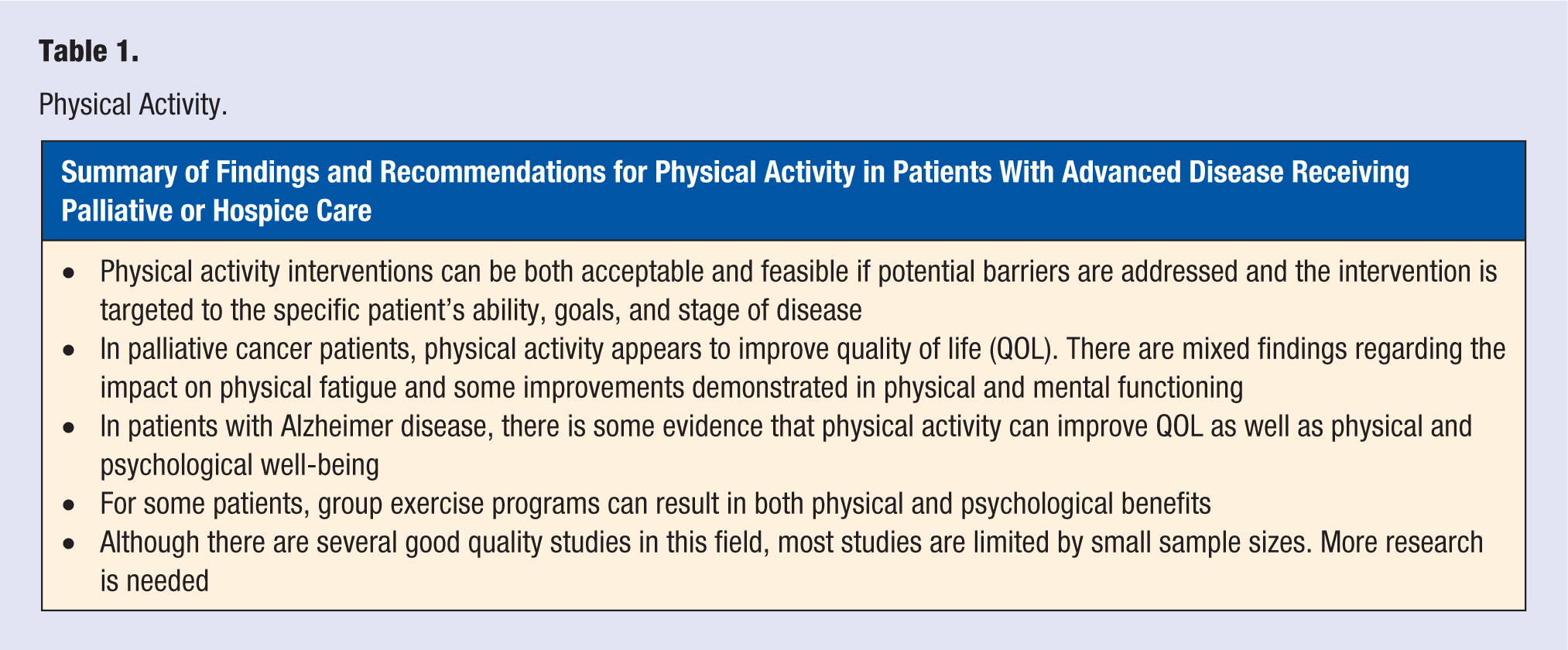
Several studies in progress are building on previous studies to examine the effects of physical activity on the QOL of palliative care patients. The POSITIVE study is using a combination of aerobic endurance training and resistance training in nonoperable lung cancer patients with the aim of improving QOL and physical performance. 27 The TIRED study is comparing the effects of graded exercise therapy with cognitive behavior therapy in palliative care patients with incurable cancer, with the primary aim of reducing fatigue and secondary aims of improving physical functioning and QOL. 28 A summary of findings and recommendations for physical activity are presented in Table 1.
Physical Activity.
Nutrition
Dietary recommendations for palliative care patients with advanced illness and/or approaching end of life can be a highly emotionally charged subject for patients, family, and health care providers. The act of eating or feeding a loved one carries with it significant QOL benefits, such as enjoying the taste of food, feeling nurtured or nurturing others, and feeling socially connected. Conversely, nutritional support interventions can also carry risks that could significantly worsen QOL or even shorten the duration of life in patients approaching the end of life. Therefore, decisions regarding nutritional interventions, including artificial nutrition, for patients in palliative care and hospice settings are often very complicated, involving consideration of the patient’s wishes, social situation, medical concerns, cultural and religious beliefs, and ethical issues. 7
Anorexia and Cachexia in Advanced Disease
Anorexia and cachexia, common findings in advanced palliative patients, often trigger concerns that prompt consideration of a variety of nutritional interventions in the care plan. Studies show that patients with advanced cancer and their families frequently express concerns about anorexia, weight loss, malnutrition, and starvation29,30 and that changes in physical appearance resulting from severe muscle wasting and weight loss (cachexia) can be distressing to both patients and families. 31
This weight loss in advanced cancer is frequently a result of insufficient caloric intake as well as cancer-mediated hypermetabolic and catabolic mechanisms, which accelerate muscle wasting.32-34 However, patients with very limited prognoses usually do not report suffering from hunger or thirst as their illness progresses toward death, 35 nor is the patient considered to be starving. 36 Nutritional deficiency at the end of life produces a metabolic state of ketosis that reinforces the lack of desire for food intake and is widely considered a natural part of the dying process. 35 To complicate matters further, there has been some debate regarding the ethics of withholding artificial nutrition in the advanced palliative care patient, with some arguing that it may be seen as basic nursing care, 37 whereas a consensus panel would disagree, stating that “artificial nutrition and hydration are a medical intervention” requiring the consent of a competent patient. 7
Assessment Approach
Given these complex physiological changes and emotional issues, several authors recommend that advanced palliative patients with progressive weight loss should have careful clinical and nutritional assessments for potentially reversible causes, such as inadequate calorie/protein intake or depression.31,34,38 Additionally, nutritional concerns should trigger establishment of clear goals of care, which is critical for determining the most appropriate nutritional approach for the individual palliative or hospice care patient.
Many experts recommend that the patient’s goals of care and end-of-life wishes should be assessed through individual and family discussions and then clearly documented.7,38-40 Care should be taken to ensure that patients with decision-making capacity are never treated against their wishes. As with all medical decisions, the patient should benefit from proposed nutrition interventions.7,41 These interventions should be focused on the patient’s needs regarding improving QOL through nutrition. 42 The goal should be to promote comfort from food while reducing uncomfortable symptoms, such as nausea, bloating, or diarrhea.33,38
Risks and Benefits of Various Nutritional Approaches
Oral nutrition and supplementation
General oral nutrition recommendations for advanced palliative care and hospice patients include eating favorite, well-tolerated foods frequently and in small quantities at a time. The pleasure of tasting food should be emphasized over calories, though high caloric foods such as eggs, puddings, mashed potatoes, and protein-enriched shakes should be encouraged.38,43 The social benefits of sharing food together with friends and family should also be recognized. 41 Although some patients may benefit from nutritional supplementation, patients and families should be counseled that simply increasing caloric intake does not reverse the underlying process causing anorexia and cachexia toward the end of life.31,36 In fact, studies show that aggressive feeding may cause uncomfortable symptoms such as nausea, vomiting, early satiety, bloating, aspiration, peripheral and pulmonary edema, and ascites. 38 Additionally, aspiration of food into the lungs caused by a weakened swallowing reflex or dysphagia can result in significant physical and emotional suffering. 30
No studies have consistently shown benefit from various vitamin and mineral supplementation. Prevost and Grach summarize several studies that have shown short-term benefit and improvement in QOL with oral nutrition supplementation enriched with omega-3 polyunsaturated fatty acids. One study showed the importance of targeting systemic inflammation in the prevention and treatment of cancer cachexia with nutrition support. 44
There is no consensus regarding specific recommended diets for advanced palliative patients, but the Mediterranean and other anti-inflammatory diets may be beneficial because of their high omega-3 fatty-acid content. These diets promote olive oils, nuts, and greens, focusing on plant-based, whole foods. Energy and protein supplement shakes may be required to maintain the minimum daily requirements to help prevent the rapid loss of muscle mass.34,45,46
Artificial Nutrition/Hydration (ANH)
General considerations
Forms of artificial nutrition are enteral (eg, tube feeds) and parenteral nutrition (PN), often used as nutrition delivery to patients with terminal illnesses, including advanced cancer, severe debilitating stroke, dementia, and neurological diseases. It has been suggested that artificial nutrition should be considered for patients with a serious or terminal illness receiving palliative care, if it either (1) prolongs life expectancy or (2) enhances QOL until death occurs. If QOL is not improved, artificial nutrition may be seen to actually prolong the dying process. 31
Parental nutrition involves the intravenous delivery of a mixture of lipids, carbohydrates, amino acids, vitamins, and minerals. 32 PN is usually considered outside the standard of care for most patients with advanced incurable cancer and has become quite controversial.7,34,40 Easson et al 31 argue that there is no physiological basis to assume that PN would affect the inflammatory and catabolic aspects of cachexia. According to Capital Health guidelines, cancer patients may be appropriate for home PN if they meet several criteria, including if death from starvation/malnutrition is likely earlier than anticipated from disease progression alone, and life prolongation is consistent with the patient’s goals of care. 47
Enteral feeding entails delivering liquid nutritional supplement directly into the stomach or small intestine through a surgically placed portal (eg, G-tube, J-tube). Although on first inspection this appears to be a good solution for meeting the nutritional needs of palliative care and hospice patients, studies have demonstrated significant risks associated with this intervention.40,48,49
General risks
All forms of artificial nutrition have the potential for complications and involve expense and energy in order to be delivered safely. 32 PN brings potential risks and burdens such as laboratory testing, indwelling intravenous lines, infections, metabolic derangements, and liver and pancreatic dysfunction. 47 Other risks include aspiration pneumonia, agitation, diarrhea, gastric discomfort, and fluid overload, including ascites and edema.50,51 Tube feeds carry risks associated with any surgical procedure, and aspiration has been documented as the most significant complication. 40
Evidence of benefit versus harm
Patients near end of life: No strong evidence exists supporting the use of PN for terminally ill patients; however, very few well-designed studies researching the subject have been completed. 52 In fact, there are currently no published randomized controlled trials regarding artificial nutrition for adult palliative patients. 53 Literature reviews have found little evidence that artificial nutrition improved nutritional status or survival in terminally ill cancer patients.29,34,36
Advanced dementia: Studies have shown that artificial nutrition in patients with advanced dementia does not prolong survival or improve QOL.48,49,54,55 The risks and harms associated with feeding tubes placed in patients with advanced dementia include pain, infection, bleeding, aspiration, risk of pressure injuries likely resulting from excessive diarrhea causing skin breakdown, GI symptoms, fluid overload, and an increased perception of hunger.39,54 A prospective cohort study of 36,492 nursing home residents with advanced dementia and new problems eating showed that neither insertion of a percutaneous endoscopic gastrostomy (PEG) feeding tube, nor timing of insertion affected survival. 48 Additionally, a propensity-matched cohort study of nursing home patients with PEG tubes inserted (n = 1124) versus those without (n = 461) found that hospitalized patients with PEG tubes were more likely to develop new ulcers and that those with pressure ulcers already were less likely to have the ulcer heal when they had a PEG tube placed. 49 The American Geriatrics Society has recommended careful hand feeding where possible while discouraging the use of feeding tubes in patients with advanced dementia. 56
Patients with acute stroke: In a study of acute stroke patients, those who received PEG tube placements were found to have a high mortality rate, and survivors were unlikely to be functional or have improved eating abilities after hospitalization. Authors recommend that discussions involving patients’ goals of care should occur when PEG tube placement is being considered. 57
Other patient groups: Artificial nutrition may benefit patients with ALS, mechanical GI tract obstruction, or head/neck/esophageal cancers.29,36,40 In ALS patients, expert recommendations are that consideration for and placement of a gastrostomy tube should occur early, with tube placement done before forced vital capacity drops below 50% predicted values. 58
Consensus Recommendations for Cancer Patients
The only consensus recommendations we could find regarding nutrition in palliative care patients were for cancer. The European Society for Clinical Nutrition and Metabolism (ESPEN) recently published comprehensive guidelines for all stages of cancer based on available evidence and expert opinion. 34 For patients with advanced cancer receiving no anticancer treatment, authors note that there is no randomized controlled trial evidence showing improved clinical outcomes, morbidity, or mortality for patients receiving nutrition screening. Despite weak evidence, the authors strongly recommend screening advanced cancer patients to assess for individual nutritional needs, including reversible issues, based on disease progression, prognosis, and patient’s goals of care. Appropriate nutritional interventions should then be offered and implemented, after weighing risks and benefits. In the very advanced cancer patient with days to weeks to live, authors again note weak evidence but strongly recommend that nutritional offerings should be based on comfort and according to social, cultural, and emotional significance. Artificial hydration and nutrition are not likely to provide any benefit for most patients at this stage of the illness. 34
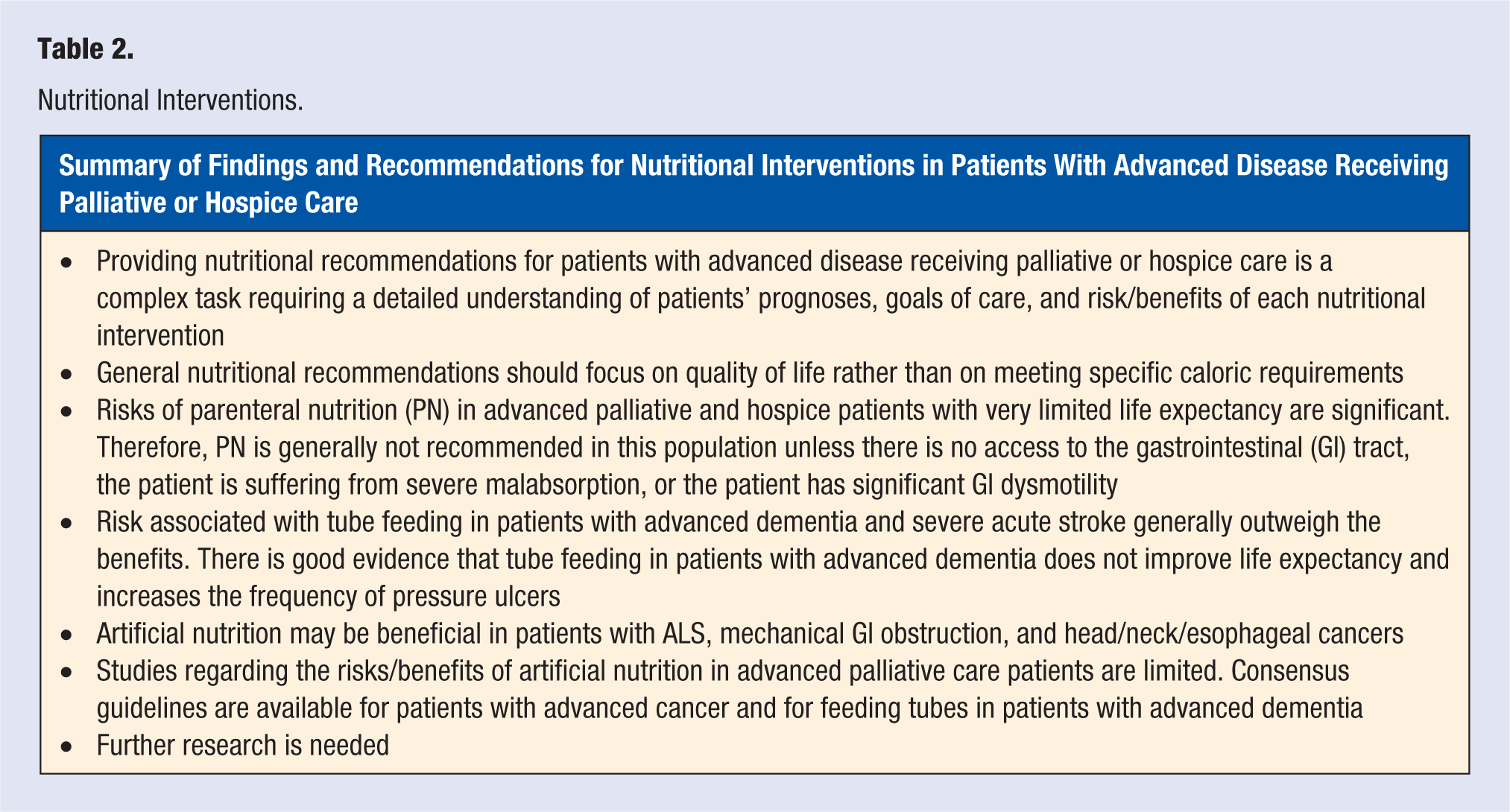
ESPEN has also developed consensus guidelines on ethical issues surrounding ANH. 7 Authors state that ANH are medical interventions requiring informed consent of a capable decision-making patient. This requires open and honest communication with patients and families. They recommend that, like all therapies, ANH should adhere to the ethical framework of patient autonomy, treatment beneficence and nonmaleficence, and justice. 7 A summary of findings and recommendations for nutritional interventions are presented in Table 2.
Nutritional Interventions.
Stress Management
Numerous articles in the medical literature examine stress management interventions for a variety of clinical conditions. However, although the interdisciplinary team approach, including spiritual care and social support, is a central feature of hospice and palliative medicine, studies focusing on stress management techniques in this population are few. Of the studies available, many are limited by factors such as small sample sizes, lack of a control group, and lack of uniformity in definitions of some modalities (eg, spirituality or mindfulness). Music therapy and mindfulness meditation are the most commonly studied in palliative care patients.
Music Therapy
Most studies regarding music interventions for palliative care patients target the relief of specific symptoms. Some attempt to understand the nuances of the effects of this lifestyle intervention in relationship to the patient’s illness journey.
Pain
Krout 59 found that after a single session of music therapy, the 80 hospice patients studied had more control over pain and felt more relaxed and comfortable, based on both self-report and behavioral observation. Similarly, Gutgsell et al 60 report that compared with “standard care” only, care including a single session of music therapy significantly reduced pain in a study involving 200 inpatients with terminal disease.
Dyspnea and anxiety
Interestingly, a 2015 retrospective analysis of the electronic medical records of 10 534 patients with cancer, revealed that music therapy did not reduce pain or anxiety, although those who received music therapy reported marginally less trouble breathing and having received “the right amount” of spiritual support. 61 A 2016 study by Mofredj et al 62 also focused on breathing and the potential benefit of music therapy for intensive care unit patients. Authors hypothesized that music decreased anxiety during mechanical ventilation and abated the stress response. Furthermore, they measured cardiac workload and oxygen consumption and found both to be lower after music therapy. Thus, music therapy appears to induce nonpharmacological overall relaxation. The authors also speculated that music may improve the quality of sleep, reduce pain and sedative use, and allow quicker weaning from the ventilator. 62
Multiple symptoms
Two recent publications, the “realist literature review” by McConnell and Porter 63 and a retrospective study by Gallagher et al 64 both claim that music therapy produces multiple therapeutic benefits. McConnell and Porter, after a review of 51 articles, report that music not only relieves physical, psychological, emotional, and spiritual suffering, but that it does so cost-effectively. The retrospective study by Gallagher et al reviewed self-collected data from more than 1500 patients, ultimately finding only 293 who met all criteria for inclusion in the study (similar to criteria for the present article). Of these 293, 96% commented positively on their music therapy experience. Overall improvements in pain, anxiety, depression, shortness of breath, mood, facial expression, and vocalization were also reported by participants. The researchers also note that symptoms were most effectively improved by vocal music that was “emotional.” 64
Physiological changes
Warth et al 65 studied 84 patients in a palliative care unit. They measured vagally mediated heart rate variability (VM-HRV) and blood volume pulse amplitude (BVP-A) during 1 of 2 conditions: live music or a prerecorded mindfulness exercise. Music therapy reduced VM-HRV and, in women, increased BVP-A levels as compared with the control group assigned to the recorded mindfulness exercise. 65
Impact of type of music and timing
In a trial of at least 2 music therapy sessions for 41 patients with terminal cancer, Preissler et al 66 aimed to identify types of music most suitable for different demographic groups. They reported inconclusive results and that the most practical course of action appeared to be to identify the music each individual likes and that answers her or his needs at a particular time (music that offers “diversion,” for instance, as opposed to that which strengthens “sense of self”). 66 O’Callaghan et al 6 faced similar challenges in their study of 52 Australian cancer patients. They found that concerts and broadcasts were not personalized enough to relieve stress in all the participants. Additionally, the music that a patient initially expressed a preference for was less comforting at a different point in the course of their disease and a shift to exploration of unfamiliar music was noted.
Mindfulness/Meditation
Mindfulness and meditation, although popular topics in the literature, are even more difficult to measure and categorize than music therapy. Furthermore, there is the additional complication that mindfulness and meditation are perceived as—and often are—closely related to spirituality and religion. Some research regarding patients receiving palliative care, however, has been published.
A review of mindfulness-based interventions for cancer patients that includes published, unpublished, and ongoing work, both qualitative and quantitative, was published in 2011. 67 Despite the inclusiveness of the criteria, however, the authors included only 13 articles. These studies reported significant improvements in anxiety, depression, stress, sexual difficulties, physiological arousal, and immune function. More recently, Ball and Vernon 68 reviewed the literature on meditation in terminally ill patients with similarly broad parameters. These researchers found that little work had been published on indicators of physical health—blood pressure, intensity of pain, and sleeping patterns. Studies tended to focus on patients with end-stage cancers, excluding other life-limiting conditions. Interestingly, the effect of mindfulness was rarely studied in conjunction with mental health—anxiety, compliance, depression, and stress. The work reviewed reported that most of those who meditated rated the experience as positive. The authors concluded that further research was needed to reinforce these findings.
Beng et al 69 investigated the effects of 5 minutes of mindful breathing compared with an equal amount of time devoted to communicating with an attentive listener on palliative care patients and family caregivers with high distress scores by the Distress Thermometer. Although distress was reduced much more in the meditators than in the communicators, the study was limited to 20 participants and included patients and caregivers.
Ando et al 70 presented a well-crafted statistical analysis of 28 Japanese patients who were receiving chemotherapy for some form of cancer. The researchers documented a decrease in both anxiety and depression after meditation. It must be noted, however, that the stages of the cancer were not specified and that patients were excluded from the study if they reported severe pain.
Particularly interesting is a study by Johnson 71 in 2011. None of the 32 terminally ill study participants had had instruction in or experience of meditation; 16 had a 1-day intensive session with a Zen master who used “dialogue” to induce a deep meditative state in the participants but did not instruct them in formal Zen sitting practice. On all measures of stress, these briefly trained meditators reduced their anxiety significantly compared with the untrained. 71
Given the generally low reported level of adverse effects of mindfulness or meditation interventions, it is possible that successful interventions in healthy individuals or other populations could be generalizable to patients with life-limiting conditions receiving palliative care. Unfortunately, although several very recent systematic reviews and meta-analysis studies report promising findings in areas such as blood pressure control, chronic pain, posttraumatic stress disorder, insomnia, and immune markers, all authors conclude that further research is still needed in this field.72-78 A 2007 extensive report (263-page) reviewed mantra meditation, mindfulness meditation, yoga, tai chi, and qigong. The authors concluded that studies generally lacked methodological quality and that “firm conclusions on the effects of meditation practices in healthcare cannot be drawn based on the available evidence.”79 (p. 6)
Yoga
Similar to other stress management modalities, the literature on yoga tends to comprise small studies or expert opinion. For example, a 2017 study showed promising positive effects of yoga on dyspnea in 15 patients with chronic obstructive pulmonary disease (COPD) and heart failure. 80 The severity of participants’ disease was not specified. Participants in this 8-week, twice-weekly TeleYoga course demonstrated significantly improved dyspnea and distress following a 6-minute walk test compared with a control group. Similarly, McDonald et al 81 judged a 12-week pilot program in Dru (gentle) yoga “highly successful” with a small group of patients in a single-day care palliative setting, based on self-report.
A 2017 meta-analysis of yoga for breast cancer patients 82 found moderate-quality evidence suggesting that yoga outperformed no therapy in reducing fatigue and sleep disturbances. Compared with psychosocial/educational interventions, yoga was, based on moderate-quality evidence, better at reducing anxiety and depression. The authors found only very low-quality evidence, however, that yoga is “as effective as” other exercise programs in reducing stress. In a previous review, authors acknowledged the positive experiences of yoga participants, its cost-effectiveness, and its lack of adverse effects but claimed that it was “impossible to see a significant effect.” 83
Other Stress Management Methods
Complementary and alternative medicine (CAM) use is widespread in palliative care and hospice settings. However, studies focusing on this patient population are rare. Smith et al 84 reviewed the effectiveness of complementary therapies in several patient populations and noted flaws in most studies. They reported small samples and “mixed results” for mindfulness research but included it on their list of “likely to be effective” therapies, along with exercise, massage, cognitive behavioral therapy, music therapy, and progressive muscle relaxation. Art therapy, hypnosis, expressive writing, acupuncture, and a variety of pharmacological agents fared less well than the “mixed results” of the interventions recommended.
Similarly, although studies regarding the prevalence of CAM use by palliative care patients85,86 show that prayer is one of the most commonly used modalities, studies specifically exploring prayer in this population are rare, with mixed results.87,88
Additionally, considerable research has been conducted regarding the relaxation response, a physiological response that counters the “fight or flight” stress response, which can be elicited through a variety of techniques, including meditation, yoga, prayer, and progressive muscle relaxation. 89 The relaxation response has been found to be beneficial in a variety of patient populations, including patients with moderately severe congestive heart failure 89 and severe medication-resistant depression and anxiety, 90 and appears to be linked to both physiological changes and increased experience of spirituality. 89 However, we were unable to find studies specific to advanced palliative or hospice patients.
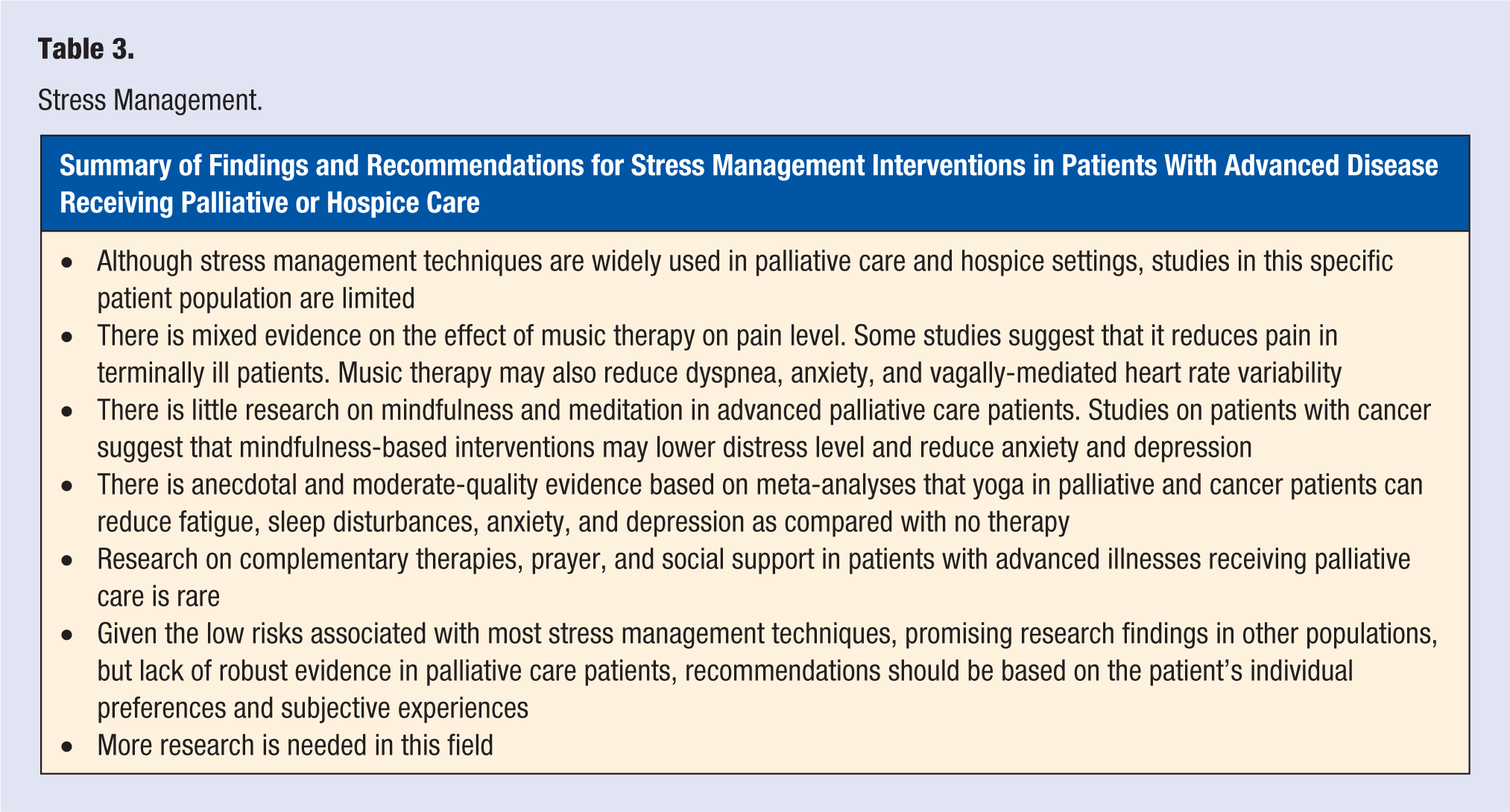
Finally, although social support is a hallmark of hospice and palliative care and is documented to be of benefit in other populations, high-quality studies focusing on this particular population are rare. A summary of findings and recommendations for stress management interventions are presented in Table 3.
Stress Management.
Substance Use
The appropriate management of symptoms in patients with advanced life-limiting illnesses who also have substance use disorders (SUDs) is extremely complicated, especially because opioids and benzodiazepines remain the cornerstone for treatment in hospice settings. Guidelines for caring for these complex patients are only recently being developed.91,92
Given the prevalence of SUDs in the general population and the opioid crisis in the United States, 93 it is not surprising that physicians encounter patients eligible for palliative or hospice care who enter this phase of treatment with complex histories related to tobacco, alcohol, recreational drugs, and/or opioids. Studies suggest that 18% to 43% of patients in palliative care or hospice settings are at risk for substance misuse or chemical coping,94-97 defined as “ the use of opioids to cope with emotional distress, characterized by inappropriate and/or excessive opioid use.”98 (p. 704) Additionally, a national survey of palliative care fellowship programs revealed that 50% “agreed” that substance abuse and diversion was a problem for their program (with only 25% disagreeing). 99
Patients receiving hospice or palliative care often experience severe pain as a result of progression of their advanced-stage illness. In this setting, it is critical to attend to patients’ pain management needs, avoiding both the historical undertreatment of pain in dying patients and the stigmatization of patients with addictions. However, many authors argue that it is also very important to manage suffering caused by untreated SUDs, avoid misuse of medications, and prevent diversion or overdose.91,92,100 They argue that patients with SUDs are at high risk for worse symptom expression and chemical coping–related stress and anxiety that can oppose the efforts of care providers. Even for those patients with a very limited life expectancy (ie, receiving hospice services), the effects of untreated SUDs can undermine measures to improve QOL.91,92,100
As with other lifestyle interventions in palliative care and hospice patients, studies related to substance use and cessation are somewhat sparse. Decisions regarding the best interventions for patients depend on a variety of complex factors and require an in-depth knowledge of a patient’s prognosis, goals of care, and effects of the use of various substances on symptoms, symptom management, and overall care management.
Substance Use and Symptom Experience
Over the past decade, studies have furthered the understanding of the role of substance abuse in end-of-life care. Alcohol and tobacco use present unique challenges for palliative care providers. A 2011 chart review study of 598 cancer patients screened for alcohol, tobacco, opioids, and recreational drug use identified both a higher reported pain experience in tobacco users and higher chance of recreational drug use in patients with signs of alcohol abuse. 101 This finding was further clarified in a 2016 study of 300 advanced cancer patients, which showed a higher occurrence of alcohol abuse and illicit drug use in smokers compared with nonsmokers. 102 Increased pain and symptom reporting in these patients are trends that require further consideration as potential contributors to chemical coping in advanced cancer patients.103,104 Any risks of chemical coping and substance abuse in hospice and palliative patients need immediate attention because of the risk of care deviation and even narcotic diversion. Screening on entry to palliative and hospice care is crucial to ensure that patients will receive appropriate interventions to maximize QOL.91,92
Screening and Identifying at-Risk Patients
Several methods have shown efficacy in screening patients at risk of substance abuse. Screener and Opioid Assessment for Patients with Pain (SOAPP) was studied as a tool for identifying patients who are at risk of opioid abuse during long-term treatment. 105 Study participants were being treated for noncancer pain, but results demonstrated the ability of SOAPP to identify characteristics of at-risk patients. CAGE (Cut Down, Annoyed, Guilty and Eye Opener) is a similar questionnaire developed to identify alcohol abuse disorder and has been demonstrated to help identify patients at risk for substance abuse during pain management.8,101,106 These 2 well-known screening tools have been demonstrated to be effective in identifying at risk patients in chronic pain management and cancer pain treatment.101,107 Although several authors advocate for using screening methods on entry to palliative care treatment in order to balance opioid abuse risk with the benefits of pain reduction,91,92,97,100 recent studies suggest that there is no uniformity in screening practices across hospice agencies or palliative care fellowship programs.99,108,109
Strategies for Encouraging Lifestyle Changes
Encouraging patients to make lifestyle changes related to substance use is particularly challenging in patients with advanced or end-stage disease. Studies of effective strategies are few. Hui et al 110 suggest that a first step involves allowing the patient to be more involved in their care. For example, encouraging patients to choose what pain level they would like to achieve during care allows the establishment of tangible goals that the patient can work toward. 110 A patient set goal can become a stepping stone to more substantial changes in behavior.
Tobacco Dependence
Smoking cessation is often recommended as a means of reducing one’s risk of cancer and pulmonary disease. However, patients with end-stage COPD and cancer can no longer benefit from the preventive effects of smoking cessation 111 ; therefore, their motivation level for lifestyle change may be even lower than at earlier periods in their lives. In fact, studies have shown that smoking status is negatively correlated with participation in any lifestyle intervention in palliative patients.4,5 Some authors suggest that smoking cessation can be proposed as a means of achieving the patient’s pain goal by introducing it as an opportunity to reduce pain. 112 Similarly, the goal of decreasing breathlessness may act as a motivator. Pulmonary rehabilitation uses a multifaceted approach that can be tailored to assist cessation of smoking in both patients with COPD and with lung cancer, resulting in less exacerbations of breathlessness.113-115 Although challenging to implement, the benefits of changing smoking behavior go beyond improving symptoms in patients with respiratory difficulty and into reducing risks of further substance abuse.
Alcohol Dependence
In a recent review of alcohol dependence in palliative care, MacCormac 8 found no definitive recommendations for addressing alcohol dependence in the context of palliative care. Patients present unique social, physical, and psychological needs as they approach the end of life, requiring physicians to consider a course of treatment that will allow the greatest amount of comfort. This can be achieved by supporting abstinence through inpatient treatment or by planning treatment around continued alcohol use. The few studies in this area suggest that screening and acknowledging dependence are barriers to care, with 67% to 87% of patients being identified as alcohol dependent for the first time on entry into palliative care settings. 8
Narcotic Dependence
The task of managing pain in patients with advanced and/or terminal diseases, such as metastatic cancer, is extraordinarily challenging in patients with a history of narcotic abuse. In this situation, narcotic tolerance may necessitate higher doses of medication than usually necessary for patients with similar disease. 116 Additionally, concerns regarding the possibility of narcotic diversion either by the patient or family members might cause providers to inadequately treat a patient’s debilitating pain. 117
Some studies have examined systems issues to address this issue. For example, one outpatient palliative care center implemented more regular visits and urinary drug tests to manage at-risk patients. 118 This allowed health care providers to intervene early with treatments for the cause of chemical coping.
Other systems-level interventions address the training of physicians. In a 2012 study, 102 hospice and palliative care fellows were surveyed regarding their preparedness to handle opioid abuse in their patients. Less than half reported having received any training in addiction management. 119 Similarly, less than half of the hospice organizations in Virginia reported that they had any required training in substance abuse. 109 Although the sample sizes were small and studies focused on this topic are limited, these studies do call to attention the need to train hospice and palliative care providers in methods to manage addiction in a specialty where opioid use is almost universal.
Finally, adequate documentation has been identified as a potential weakness in providing consistent and appropriate treatment of high-risk patients. One study in particular found that 18% of patients with advanced cancer were chemically coping, but only 4% of the charts documented this history. 96 Despite the potentially short life expectancy of patients on entrance into hospice and palliative care, there is a high probability of multiple specialists encountering the patient in that time, making it crucial that all aspects of a patient’s substance use history are clear to all providers.
Expert Opinion Recommendations
Two recent articles91,92 provide expert opinion guidelines for the management of pain in palliative care or hospice settings, taking into account the opioid crisis in the United States. Recommendations include the following: (1) increase SUDs education for hospice providers; (2) screen all patients for SUDs, pain, opioid use, and depression/anxiety; (3) open communication with patient and family; (4) adapt practices from SUD treatment programs to hospice/palliative settings; (5) utilize an interdisciplinary, compassionate, and nonjudgmental approach; (6) treat comorbid psychiatric conditions; (7) consider nonopioid and adjuvant analgesics; (8) consider opioid type and formulations (eg, use methadone or buprenorphine); and (9) consider selective use of naloxone. A summary of findings and recommendations for substance use modification is presented in Table 4.
Substance Use Modification.
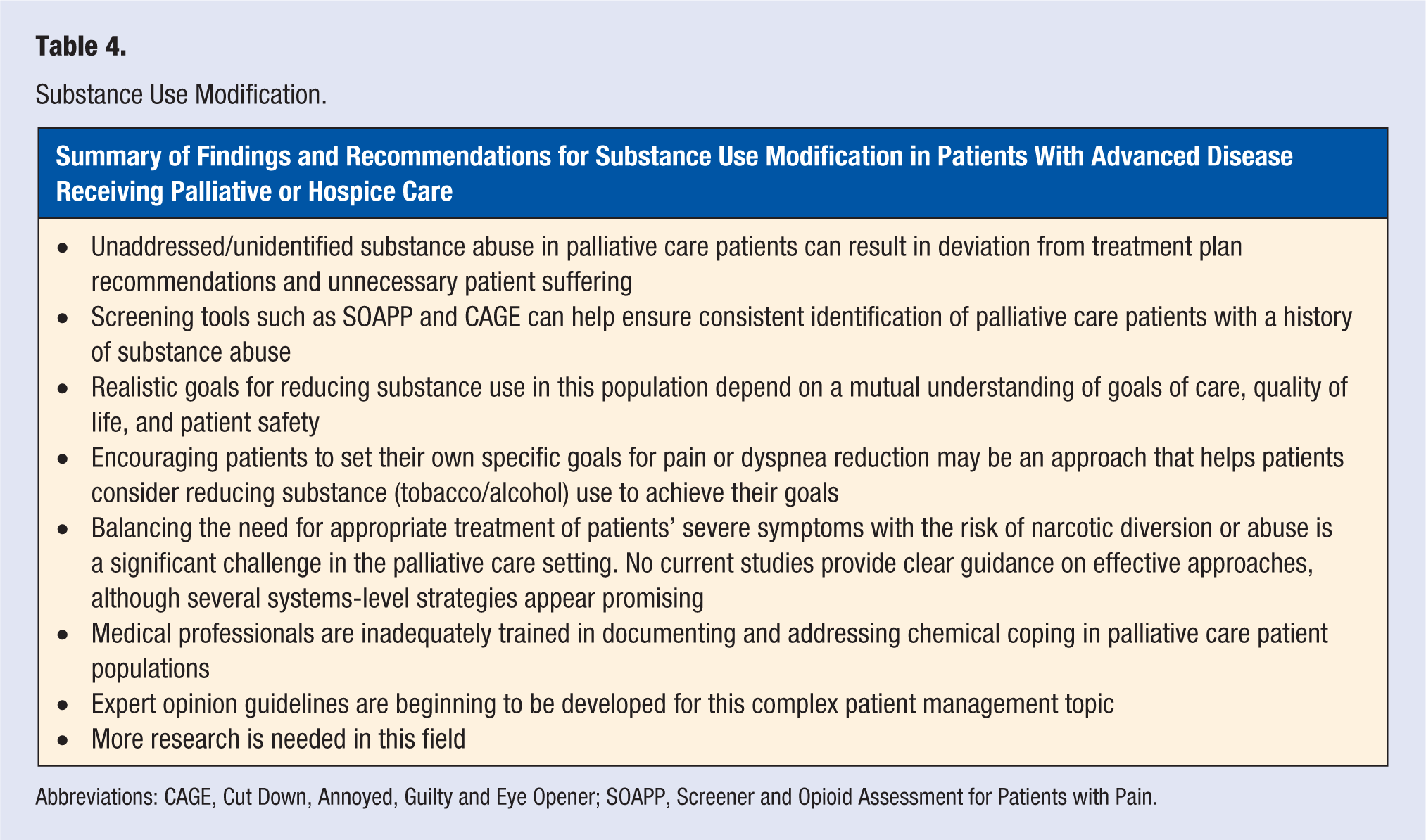
Abbreviations: CAGE, Cut Down, Annoyed, Guilty and Eye Opener; SOAPP, Screener and Opioid Assessment for Patients with Pain.
Conclusion
Lifestyle medicine approaches are widely used in palliative care patients with advanced or terminal disease and have the potential to improve symptom management and QOL. Although studies do exist regarding physical exercise, nutrition, stress management, and substance use modification in this patient population, the literature is limited. Methodological flaws or a focus on specific symptoms, rather than broader QOL measures, limit many existing studies. Additionally, the limited life expectancy and frailty of this vulnerable population may limit participation in studies. Further complicating this field is the fact that the effectiveness of various interventions appears to depend heavily on the individual patient’s stage of disease and emotional/spiritual journey. Given the current limited state of the literature, decisions regarding the use of lifestyle interventions should be tailored to the specific patient’s prognosis, goals of care, and emotional state, with a focus on QOL and safety. Further research is needed in this emerging field of study.
Footnotes
Authors’ note
Gregory Rachu, MD is currently affiliated with Hope Hospice and Palliative Care Rhode Island (and is no longer affiliated with Rhode Island Hospital).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.