
Abstract
Morbidity and mortality associated with cardiovascular disease can be significantly modified through lifestyle interventions, yet there is little emphasis on nutrition and lifestyle in medical education. Improving nutrition education for future physicians would likely lead to improved preparedness to counsel patients on lifestyle interventions. An online anonymous survey of medical residents, cardiology fellows, and faculty in Internal Medicine and Cardiology was conducted at New York University Langone Health assessing basic nutritional knowledge, self-reported attitudes and practices. A total of 248 physicians responded (26.7% response rate). Nutrition knowledge was fair, but few (13.5%) felt adequately trained to discuss nutrition with patients. A majority (78.4%) agreed that additional training in nutrition would allow them to provide better clinical care. Based on survey responses, a dedicated continuing medical education (CME) conference was developed to improve knowledge and lifestyle counseling skills of healthcare providers. In postconference evaluations, attendees reported improved knowledge of evidence-based lifestyle interventions. Most noted that they would prescribe a Mediterranean or plant-based diet and would make changes to their practice based on the conference. An annual CME conference on diet and lifestyle can effectively help interested providers overcome barriers to lifestyle change in clinical practice through improved nutrition knowledge.
Strategies that combine nutrition and physical activity appear to be cost-effective in reducing long-term risk of diabetes and CVD [cardiovascular disease].
Cardiovascular disease (CVD) is responsible for 1 in every 3 deaths in the United States and approximately 92 million adults are living with cardiovascular disease. 1 Approximately 45% of cardiometabolic deaths are attributable to poor diet. A healthy lifestyle (including proper nutrition) is increasingly being recognized as a critical and cost-effective modifiable risk factor in cardiovascular disease. 2 Strategies that combine nutrition and physical activity appear to be cost-effective in reducing long-term risk of diabetes and CVD. 3
A healthy lifestyle has been shown to be as effective as medications in some studies 4 and even more effective in others in the prevention and management of chronic diseases.5,6 Guidelines by numerous authoritative bodies recommend nutrition as first line therapy and/or adjunctive therapy for medical management of chronic disease.5,7,8 The US Preventive Services Task Force (USPSTF) recommends intensive behavioral dietary counseling for adult patients with dyslipidemia and other known risk factors for CVD by primary care clinicians or other specialists. 9 The American College of Cardiology (ACC) and the American Heart Association (AHA) recognize a heart healthy diet and physical activity as crucial components for CVD risk reduction, recommending physicians provide specific dietary guidance to those at risk for, or those with established, CVD. 10 The National Lipid Association states in their Recommendations for Patient-Centered Management of Dyslipidemia that patients with dyslipidemia or risk factors such as overweight or obesity be referred to professionals like registered dietitian nutritionists (RDNs) for lifestyle counseling. 11 Despite these recommendations, studies have shown that nutrition counseling only occurs in about one-third of all primary care office visits 12 with low counseling rates for CVD prevention, particularly in the areas of diet and exercise. 13 In a survey of more than 1200 primary care providers, less than half reported recording body mass index (BMI) of patients regularly or always counseling on diet, physical activity or weight management. 14 An interesting finding of this survey was that pharmacologic and surgical interventions were more common referrals (70% and 86%, respectively) than lifestyle interventions (43% for diet, 50% for physical activity), which are considered to be the first-line therapy for weight management. 15 Additionally, referral rates to RDNs and other nutrition professionals remain low. Physicians report several reasons for not providing nutrition counseling, including lack of training and low levels of confidence. 16 A 2-hour educational intervention completed in a group of medical students illustrated that a brief curriculum could increase confidence and self-efficacy in nutrition education in this group. 17 Still, a dedicated nutrition course is offered in less than one-third of US medical schools and just over one-fourth of schools meet the recommended minimum of 25 hours of nutrition training, a guideline set by the National Academy of Sciences. 18 As part of their Nutrition in Medicine project, the University of North Carolina at Chapel Hill releases a survey of national medical schools every 4 years and they not only reflect a dearth of nutrition training in medical education, but they also show the dedicated time spent on nutrition in the curriculum is actually declining. 19 In a 2006 survey of more than 2300 medical students, respondents reported low levels of nutrition training (20%) and importantly, the value placed on lifestyle interventions actually declined over the course of medical training. 20 While 72% of these students reported nutrition counseling to be highly relevant in their first year, only 46% did in their final year. The lack of training, and declining interest in nutrition, is further complicated by the fact that there are no specific nutrition requirements in Internal Medicine Residency or Cardiovascular-Disease Fellowships, 21 leaving students with minimal motivation to seek out nutrition training. This also means that if there is no nutrition provided in undergraduate medical education (UME), there is no guarantee that this would be remedied in the graduate medical education (GME) system.
The results of a survey published in 2017 reported that 95% of cardiologists polled believed it was incumbent upon them to provide basic nutrition information to their patients, with the majority reporting that they spend about 2 to 3 minutes per visit discussing nutrition with patients. 5 Only 8% of those surveyed reported they have “expert” nutrition knowledge. Interestingly, the researchers found that those who reported healthier dietary habits, as measured by reported fruit and vegetable intake, were more likely to report that nutrition counseling was their responsibility; however, only 20% of physicians surveyed reported meeting the 5-a-day minimum goal for fruits and vegetables.
Physicians face several barriers in counseling their patients about nutrition, including lack of time, financial disincentives, competing priorities, and uncertainty of effectiveness of their counseling; however, one important and modifiable barrier is lack of knowledge.22-25
Prior studies have illustrated some of the limitations in nutritional knowledge of physicians, medical students and other health care professionals17,26-29 but prior to our survey few have queried basic, practical knowledge important for counseling patients and few included assessment of cardiologists. In addition, many of the surveys were done prior to the publication of randomized controlled trials for the Mediterranean diet and were conducted during a time when a low-fat, low-cholesterol diet was the most commonly recommended diet. Others have focused predominantly on guideline adherence,27-29 which can be difficult to measure and are subject to change. Thus, we surveyed internists and cardiologists to assess their evidence-based and practical knowledge, as well as their personal views and practice patterns with respect to nutrition clinically relevant to CVD prevention with the goal of developing a potential intervention to address this deficit.
Methods
An online, anonymous survey was distributed to Internal Medicine (IM) and Cardiology faculty, fellows, and residents at New York University Langone Health in February and March of 2014. Requests for survey completion were distributed through preestablished email listservs, and questions were created, distributed, and analyzed using the Qualtrics online survey database. The Institutional Review Board at New York University Langone Health reviewed and approved the survey. Completion was voluntary, and no incentive was given for participation. Participants were allowed to complete the survey at any point during the prespecified participation period, and individuals received 2 reminder notices at weekly intervals.
The survey consisted of 26 multiple choice and true/false questions regarding demographics, attitudes, practices, and nutritional knowledge (see the appendix). In order to query “practical” nutrition knowledge, the survey asked questions about guideline-based nutrition interventions (eg, best sources of monounsaturated fats or which fish are considered to be “oily fish”) to determine if respondents could make recommendations that were more relevant to patient counseling. All questions originated from prior validated surveys or were generated by RDNs and preventive cardiologists. Prior to distribution, the survey was piloted among 20 physicians and RDNs to ensure content validity and modified accordingly. Data were collected prospectively and analyzed at the end of the participation period in May and June of 2015. BMI was calculated from respondents’ self-reported height and weight. Chi-square tests were used to compare proportions and independent 2-sample t tests were used to compare mean differences for continuous variables. The main outcomes of interest were nutritional knowledge as assessed by percent correct response to fact-based questions and self-reported attitudes and practices.
Results
Of the 636 IM physicians and 248 cardiologists, 140 and 96 responded, respectively. Overall response rate was 26.7% (22.0% of IM physicians and 38.7% of cardiologists). The average time to complete the survey was 7 minutes. Average age of participating physicians was 41 ± 12.4 years. Most were attending physicians (65.6%) and more than 30% were 15 or more years out of training. Slightly more than half of respondents were male (52.8%) and the vast majority identified an academic medical center as their primary practice environment (84.4%).
Overall, 50% of physicians rated their personal diet excellent or very good, while 13% rated their diets as fair or poor and this correlated well with their reported BMI (P for trend = .0014) (Figure 1). This is a highly relevant finding, as previous work in the United States and abroad has shown that the preventive health practices of physicians is associated with those of their patients, and this is not limited to dietary behaviors.30,31 Furthermore, when physicians disclosed their own healthy dietary and exercise habits, patients reported them more believable and motivating (in a sample of 131 general medicine patients). 32 Although 58.1% of cardiologists reported their diet quality to be very good or excellent compared with only 41.1% of IM physicians, they were more likely to be overweight or obese (39.6% vs 23.9%) based on reported BMI. Cardiologists in our survey were also more likely to be male (73.9% vs 43.6%), and older (46.7 ± 13.1 vs 37.2 ± 10.4).
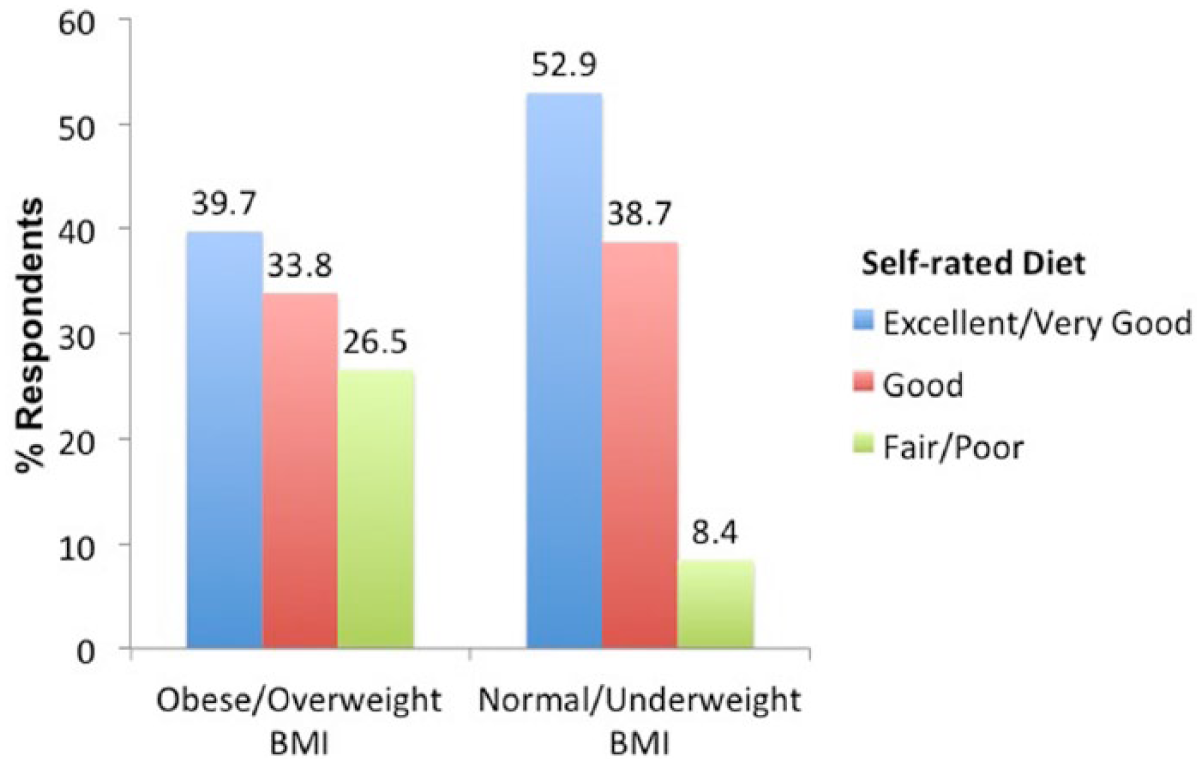
Personal diet as it relates to body mass index (BMI). P=0.0014 for trend.
Attitudes
Of physicians surveyed, only 13.5% agreed or strongly agreed that they were adequately trained to discuss nutrition with their patients (Figure 2a). A significant majority (78.4%) thought additional training in nutrition would help them provide better clinical care in the prevention of CVD (Figure 2b). When physicians were asked to rate the importance of different therapies in CVD risk reduction on a scale of 1 to 10 (with 10 being the most important), respondents rated nutrition (8.1 ± 2.05) and physical activity (8.2 ± 1.56) as important as statins (7.8 ± 2.11).
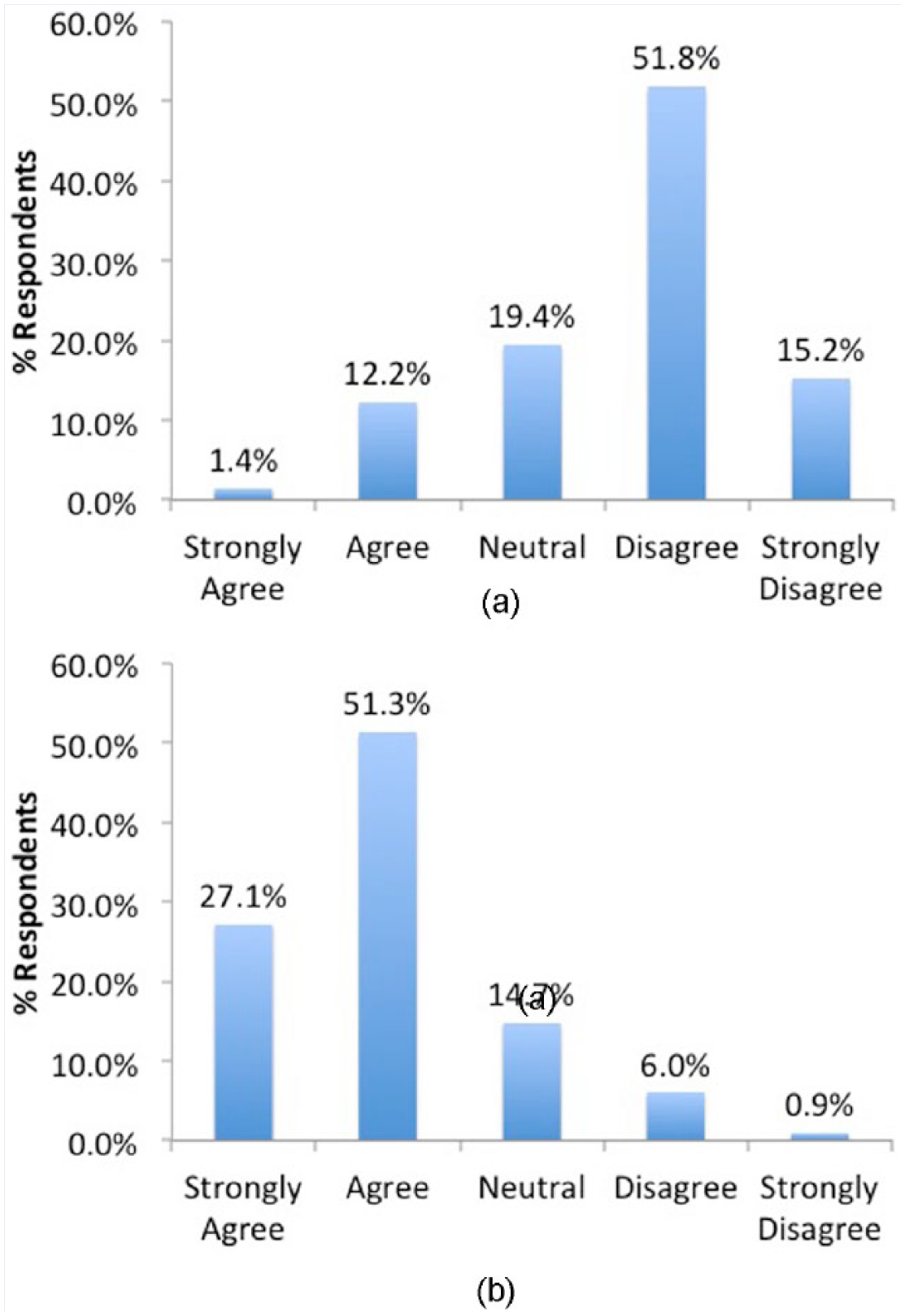
(a) Percent of respondents who agreed that physicians are adequately trained to discuss nutrition with patients. (b) Percent of respondents who reported that additional training in nutrition would result in better clinical care.
Practice
Physicians most commonly reported that they recommend the Mediterranean diet (55.1%) followed closely by low fat (40.4%), DASH (Dietary Approaches to Stop Hypertension) (38.2%), low glycemic index (18.2%), and low carbohydrate (16.4%). Sixteen percent of physicians did not recommend a specific diet to their patients. The majority of physicians (57.7%) spent 3 minutes or less counseling their patients about diet and lifestyle to prevent CVD during a routine appointment. On average, cardiologists spent more time on this type of counseling than IM physicians (P = .0006 for trend). Regardless of specialty, female providers spent more time on average on lifestyle counseling (P = .02 for trend), a relevant finding especially due to recent results from a study of Medicare beneficiaries that showed patients of female providers had lower readmission rates and lower mortality rates. 33 This finding is also consistent with earlier work showing that female providers were more likely to provide systematic counseling about unhealthy lifestyle behaviors than male physicians. 34 A more recent study done in Germany of more than 4000 primary care physicians found that female physicians reported fewer barriers to lifestyle changes and were more likely to ask patients lifestyle-related questions. 35 Referral rates to dietitians in our survey were also notably low. More than half (59.6%) of physicians refer 10% or less of their patients to a nutritionist or RDN, and an additional 5.6% never refer. Cardiologists were less likely to refer their patients to a RDN, with almost 30% responding that they refer <1% or none of their patients (P = .007 for trend). Studies show that providers who report a healthy lifestyle are more likely to counsel on lifestyle and to refer to a RDN, 5 but in the current survey, the association of perceived diet and counseling and referral practices did not reach statistical significance.
Knowledge
On average, 70% of knowledge-based questions on a very basic questionnaire were answered correctly, with no significant difference between IM physicians (68.2%) and cardiologists (72.3%, P = .08) (Table 1). Almost all (89.7%) physicians knew that the Mediterranean diet reduced CVD events in randomized controlled trials, but only 45.5% knew this was not true for low-fat diets. Knowledge regarding blood pressure lowering effects of fruits and vegetables and low-density lipoprotein cholesterol lowering effects of soluble fiber was good (81.7% and 87.6%, respectively). In contrast, only 69.5% correctly identified foods high in soluble fiber and only 30.8% could identify an omega-3 rich fish. Cardiologists did not score higher on any individual knowledge question than IM physicians.
Physician Knowledge (Percent Correct).
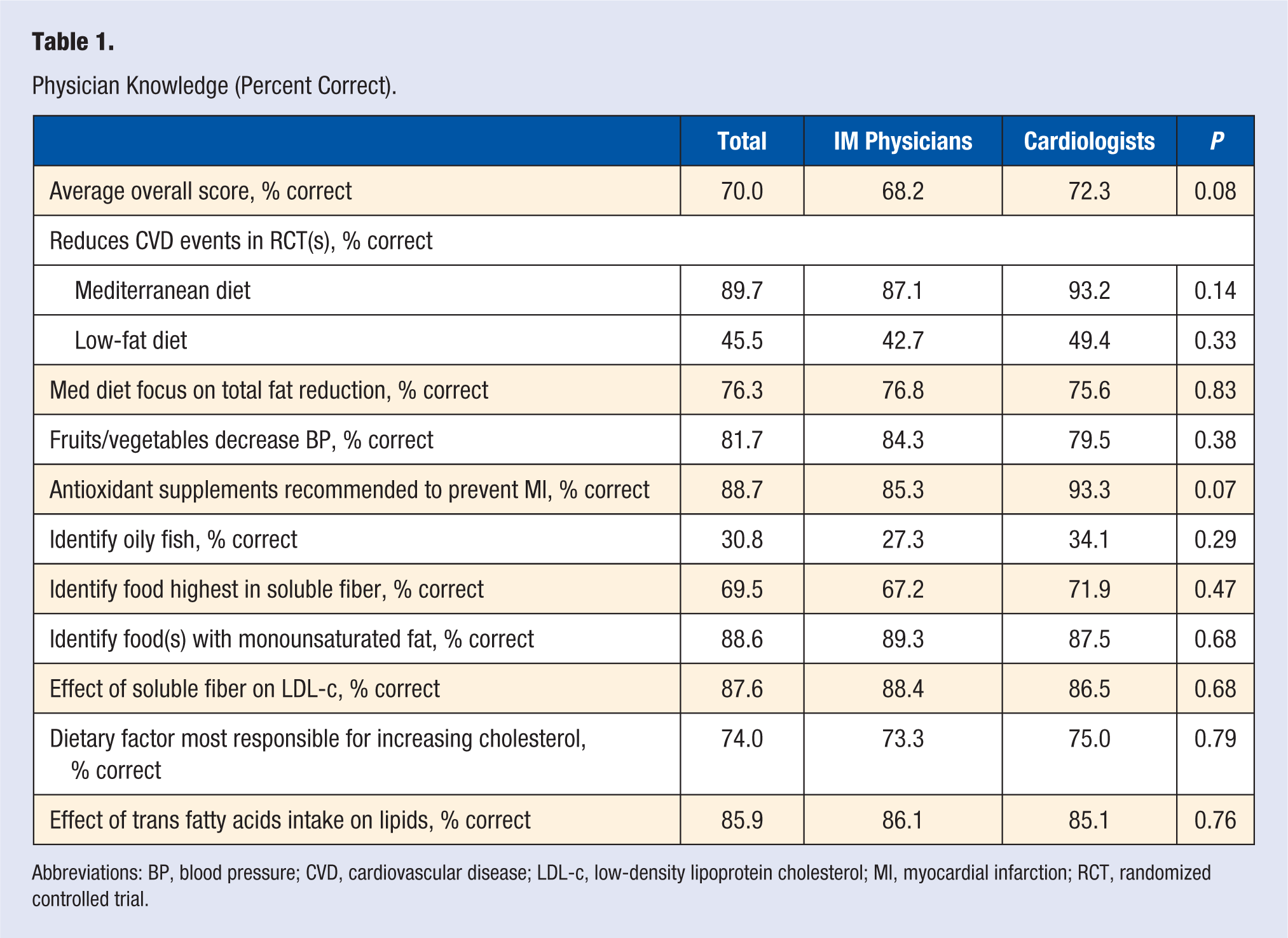
Abbreviations: BP, blood pressure; CVD, cardiovascular disease; LDL-c, low-density lipoprotein cholesterol; MI, myocardial infarction; RCT, randomized controlled trial.
Educational Intervention
The results of the survey illustrated the value physicians ascribe to dietary counseling for their patients, the potential for improvement in dietary knowledge and the willingness of physicians to obtain additional training in the field. Based on this feedback, the New York University Center for the Prevention of Cardiovascular Disease has held 3 annual continuing education symposia titled Dietary and Lifestyle Strategies for Cardiovascular Risk Reduction in conjunction with its preexisting annual Cardiovascular Risk Reduction symposium designed to enhance the education of health care providers, including (but not limited to) physicians, physician assistants, nurse practitioners, dietitians, nurses, pharmacists, and trainees. The survey responses were used in the planning of the agenda to specifically address the deficiencies in dietary knowledge and counseling that were noted. Each year, the conference has been structured to meet certain standard educational objectives, comprehensively reviewing the research to date on various dietary interventions, understanding the most current dietary guidelines and gaining specific skills in dietary assessment and education with a specific focus on motivational interviewing (topics and speakers for previous sessions can be found at https://med.nyu.edu/medicine/cardiology/center-prevention-cv-disease/education/continuing).
Topics included in each year’s conference included the Mediterranean diet, plant-based whole food diets, the DASH diet, Dietary Guidelines for Americans, as well as dietary assessment and counseling. Each was also supplemented with presentations on the most current evidence on diet and lifestyle change as well as innovative research in the areas of lifestyle and dietary reform. More than 200 health care professionals from a variety of disciplines registered for the conference (Supplemental Table 1, available in the online version of the article) each year, with 278 registered in 2018. Registrants hailed from 16 states across the United States and traveled from as far as Canada to attend the conference.
Feedback from the attendees of the conference was positive with specific appreciation for the unique course material covered and the awareness brought to the importance of dietary factors in the treatment of patients with or at risk for CVD. Attendees reported that they found the course material to be practical and concise enough to incorporate into their patient care. Completion of the survey was required for receipt of CME credits, so response rate was nearly 100% for the posttest survey.
As a result of the 2016 conference, 96% of respondents agreed that they would advise their patients to increase fruit and vegetable intake and/or follow the Mediterranean diet or a whole food, plant-based diet. In 2017, the majority (87%) reported that they learned that adequate intake of vitamins and minerals through diet is preferred over supplementation. When asked, “based on your participation in this activity, what changes will you make in the types of diets you recommend to patients for CVD health?,” 85% to 95% of respondents reported that they would recommend a plant-based diet (both overall and specific to diabetes, hypertension, and dyslipidemias). This is in contrast to only 14.3% of those in the original survey reporting that they would prescribe a vegan or vegetarian diet. Based on the 2018 conference, attendees would recommend the Mediterranean or whole food, plant-based diet to their patients. The major obstacles to incorporating nutrition counseling into practice reported by attendees were time constraints (75%) and lack of educational resources for patients (22.5%). Nearly 90% (88.5%) of 2018 attendees agreed or strongly agreed that they could more effectively counsel patients with diabetes, hypertension and specific dyslipidemias after attending the conference.
Discussion
Unlike prior studies, this study specifically measured practical knowledge, in addition to attitudes and practices of physicians and compared these findings in cardiology and general internal medicine. Although dietary knowledge was fair for a simple knowledge questionnaire, there were clear areas identified for improvement. Poor referral rates to dietitians, especially from cardiologists, indicate a specific area to target for improved clinical care of the patient with CVD risk factors as well as improved nutrition training for physicians.
The limitations of this survey include a low response rate and the potential for selection bias. The rates of adequate knowledge and training may in fact be lower in the nonresponders to the survey. In addition, this is a single center study from which it is difficult to extrapolate to other medical centers. Finally, we relied on self-reported information, which is subject to bias.
Survey findings identified a clear deficiency in medical education and provided the needs assessment with which to justify a dedicated conference to specifically address this deficiency. While an effort to improve medical education within UME and GME training is imperative, CME presents other opportunities for addressing these gaps in medical education. The attendance and survey results from the three annual conferences provide evidence that the information and techniques presented are deemed useful to providers and fill a very important knowledge gap.
Courses offering instruction for trainees and physicians are providing separate avenues to increase dietary knowledge and counseling and to impact the referring behaviors of physicians to nutrition professionals. Globally available programs, such as the ACPM/ACLM-competency-based Lifestyle Medicine course from NextGEnU.org (nextgenu.org), as well as the US-based Nutrition in Medicine (University of North Carolina at Chapel Hill, nutritioninmedicine.org) and Introduction to Food and Health (Stanford Center for Continuing Medical Education, med.stanford.edu/cme/courses/online/food-and-health.html), are offered at no cost for the motivated provider, and with free or lost cost CME opportunities. The National Heart, Lung and Blood Institute (NHLBI, nhlbi.nih.gov) of the National Institutes of Health in the United States, The Need for Nutrition Education / Innovation Programme (NNedPRO) in the United Kingdom (nnedpro.org.uk/) and Deakin University in Australia (deakin.edu.au/students/faculties/faculty-of-health/school-of-exercise-and-nutrition-sciences/research/wncit/about-wncit) offer further resources and guidance for planning curricula.
The CME conference offered at New York University Langone Health is another step toward improving nutrition knowledge and counseling skills of physicians and other health care professionals through continuing medical education. Attendees traveled to the conference from all over the country and from out of the country, which may reflect a lack of offerings in other areas of the United States, in addition to a highly valuable course content being offered.
Conclusion
This survey and subsequent training events not only highlight the lack of nutrition training and counseling skills among physicians, but they may also serve as a model for other institutions and major organizations to create similar programs to help fill the current gaps in formalized training programs. The combined use of education for physicians regarding the current nutrition research base and practical approaches to counseling could result in increased physician emphasis to patients on the importance of diet and lifestyle. Strategies that include the healthcare team in a concerted effort to improve dietary and lifestyle factors may also improve rates of referral to nutrition counseling. Efforts to improve medical nutrition education will greatly improve cardiovascular health overall and decrease the downstream healthcare costs of chronic disease.
Supplemental Material
Gianos.AppendixSupplementalTable – Supplemental material for Physicians’ Dietary Knowledge, Attitudes, and Counseling Practices: The Experience of a Single Health Care Center at Changing the Landscape for Dietary Education
Supplemental material, Gianos.AppendixSupplementalTable for Physicians’ Dietary Knowledge, Attitudes, and Counseling Practices: The Experience of a Single Health Care Center at Changing the Landscape for Dietary Education by Nicole Harkin, Emily Johnston, Tony Mathews, Yu Guo, Arthur Schwartzbard, Jeffrey Berger and Eugenia Gianos in American Journal of Lifestyle Medicine
Footnotes
Appendix
Acknowledgements
The authors thank Dr Scott Sherman, Dr Melanie Jay, and Dr Jiyoung Ahn for their assistance in creating and pilot testing the survey questions. Survey questions were also adapted from Mosca, L, et al. and Temple, et al.
Authors’ note
The authors would like to thank their statistician Yu Guo for her tremendous dedication to this project. Yu Guo is affiliated with Department of Population Health, Center for Healthful Behavioral Change, New York University School of Medicine, New York.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board at New York University Langone Health reviewed and approved the survey.
Informed Consent
Not applicable because the survey participation/completion was voluntary.
Trial Registration
Not applicable, because this article does not contain any clinical trials.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.