
Abstract
Lifestyle medicine (LM) is a relatively new branch of clinical practice (like travel medicine, sports medicine, etc), but to date with little accepted structure or methodology. The current review extends a previous attempt to define the determinants of chronic disease by expanding this to include (1) the knowledge base (the science) or epidemiology of chronic disease, (2) the skills (the art) or practice of LM, (3) the tools (the materials) that can add to LM diagnoses and prescription, and (4) the procedures (the actions) that help update conventional medicine to include practices required for a new era of lifestyle and environmentally related chronic disease.
‘The germ theory of the early 20th century provided a monocausal focus for managing infections. No such thing has happened with chronic diseases, which are still dealt with in silos . . .’
Introduction: The Field of Lifestyle Medicine
The discipline of lifestyle medicine (LM) had its genesis toward the end of the last millennium. Its aims were to provide evidence-based treatment and prevention tools to better manage the shift in advanced societies from infectious to chronic diseases and conditions. Since then, professional associations in LM have arisen around the world. Postgraduate training is currently offered in a number of tertiary institutions, and a growing number of texts are now available.1-5 The current article is an edited version of a chapter from one of these, 3 detailing a proposed structure and methodology for LM under 4 headings: (1) knowledge, (2) skills, (3) tools, and (4) procedures.
Knowledge (The Science)
Causality with infectious diseases can usually be ascribed to biological factors (germs). With chronic diseases and conditions, this is more problematic. 6 The closest we can get is often describing determinants of disease at various levels. 7
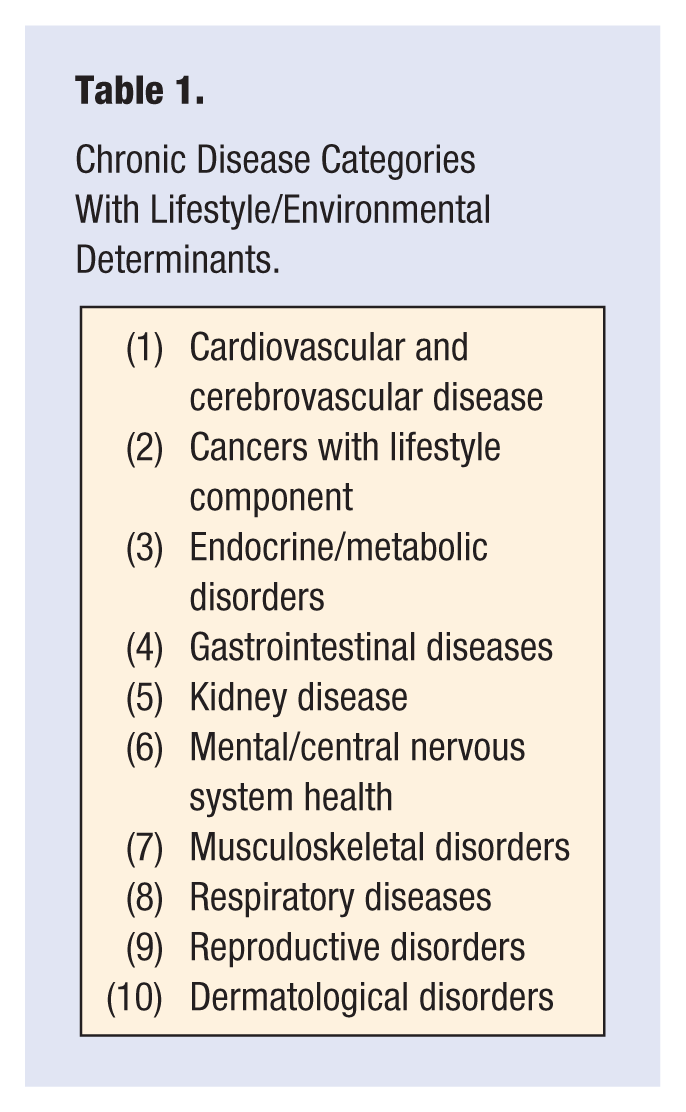
The germ theory of the early 20th century provided a monocausal focus for managing infections. No such thing has happened with chronic diseases, which are still dealt with in silos (heart disease, cancers, respiratory problems, etc) with no clear monocausal link. The discovery of a form of low-grade, systemic inflammation (called metaflammation) in the 1990s, 8 however, has changed this, because of its underlying presence in most, if not all, chronic conditions. Identifying the determinants of metaflammation (while not exactly the causes) as man-made environments, their by-products, and/or lifestyles encouraged by these environments, or anthropogens, 9 provides a single focus for the chronic disease categories shown in Table 1, like the germ theory afforded infectious diseases in the 19th and early 20th centuries.
Chronic Disease Categories With Lifestyle/Environmental Determinants.
Identifying Anthropogens
In most discussions of chronic disease etiology, smoking, poor nutrition, inactivity, excess weight, and alcohol use stand out as the dominant preventable determinants. 10 Recent research has expanded this considerably to take into consideration social, cultural, occupational, environmental, and other factors, which interact with each other in a systems-type model. 11 In a previous article in this journal, 12 we discussed anthropogens for chronic disease using the acronym NASTIE ODOURS. Other authors have covered these independently in detail,13-15 and hence, they are only repeated in summary form here (Table 2), but with the addition of 3 psychological determinants (Meaninglessness, Alienation, and Loss of Culture), expanding the acronym to NASTIE MAL ODOURS.
Anthropogens in Chronic Disease in Advanced Societies. a
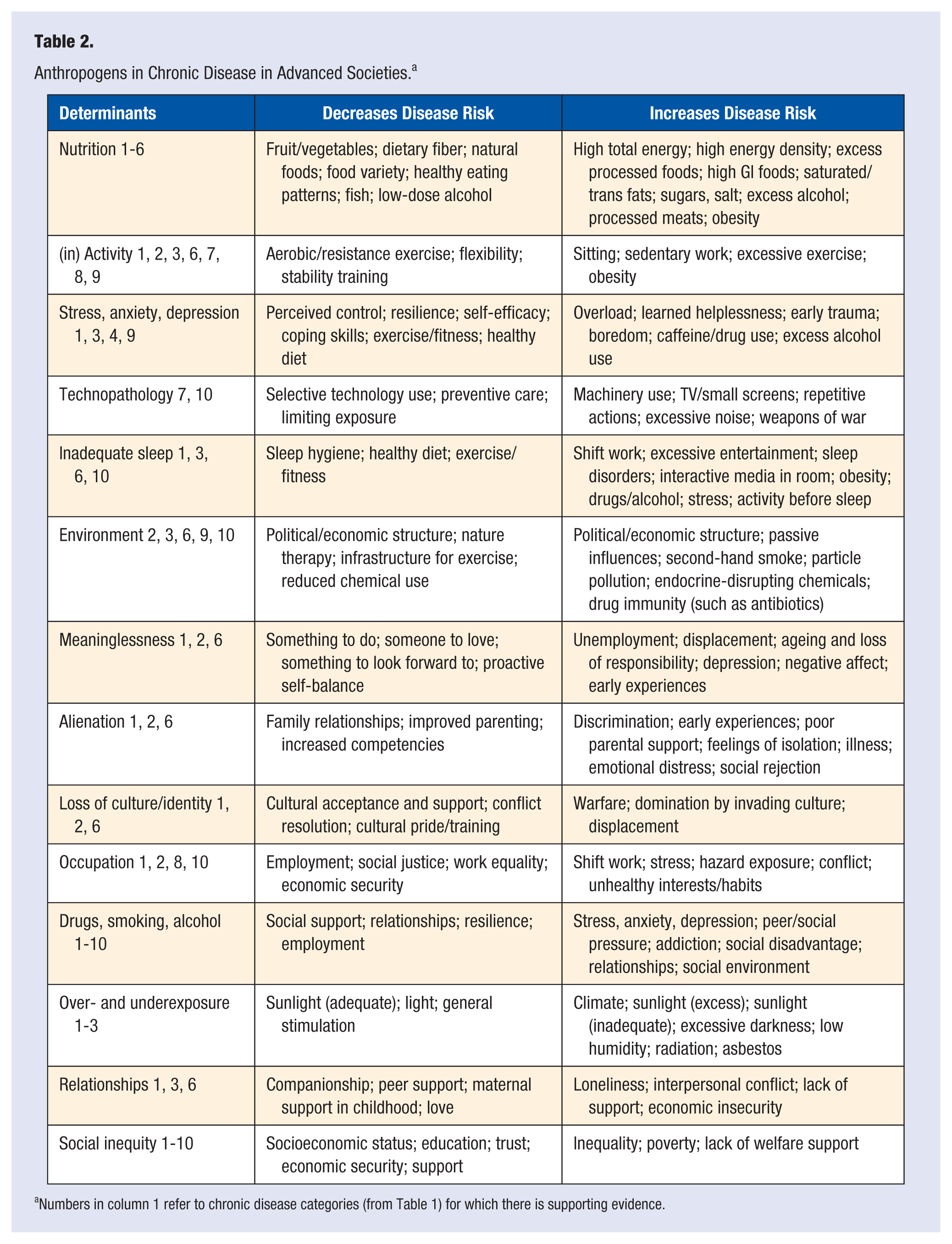
Numbers in column 1 refer to chronic disease categories (from Table 1) for which there is supporting evidence.
Chronic disease determinants (labeled anthropogens) have varying levels of potency depending on a range of factors such as genes, environment, and exposure. Although each may have an impact independently, recent findings suggest that it is more realistic to think of interactions as a systems model both within and between determinants. 11 Isolating nutrients from foods, for example, ignores the interactive relationship of nutrients found in whole meals, just as considering inactivity, sleep, or social factors alone in the absence of nutrition, stress, occupation, and so on provides only part of the etiological answer to disease manifestation. The systems model interactions between determinants may be hidden below the surface, like an iceberg (as in Figure 1), but this is a most important aspect of a modern LM approach to chronic diseases and conditions. From a practical perspective, this requires the clinician to consider not just each determinant in a linear, or physics-type fashion, but as a biological system with interactions and feedback between some or all determinants.
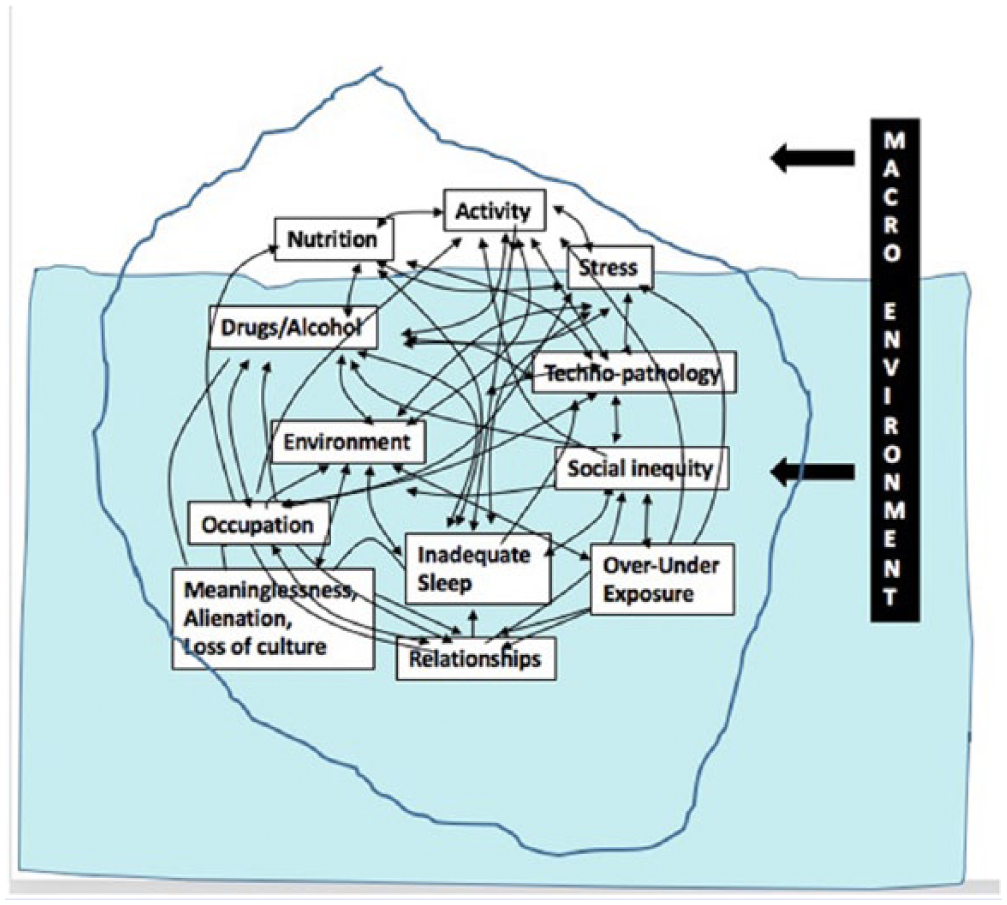
An iceberg analogy of a systems model for lifestyle medicine shown as insert.
Skills (the Art)
Elaborating the determinants discussed above is relatively straightforward. Developing the skills required to change unhealthy lifestyles and (at least the micro) environments driving these is more complicated. Clinical skills are similar to those required in conventional health care: diagnosis, prescription, and counseling in particular. The processes, however, are different and draw more on the science of behavior change and the principles from this as espoused in the psychological literature, including, but not limited to, components of influence, motivational interviewing, the art of coaching, coaxing and nudging patients from extrinsic to intrinsic motivation, and other processes to facilitate long-term change to healthy lifestyle behaviors.
Diagnosis in LM should focus on the underlying mechanisms and determinants of disease discussed above rather than the disease itself. Most chronic diseases share common dysfunctions/mechanisms (such as metaflammation) and signs in clinical practice (such as elevated inflammatory markers, gut dysbiosis, etc). Addressing these can improve risks for several diseases. For example, obesity is a function of energy imbalance. But energy intake (food and drink) and energy expenditure (metabolism, physical activity) can be influenced by a range of other, less obvious factors, which should be considered in any systems model approach. Stress, for example, can influence (positively or negatively) energy intake and metabolism as well as activity levels. Inadequate sleep can lead to low activity levels during the day, which can then affect diet and relationships, which can ultimately affect body weight outcomes.
Prescription in the case of LM involves both pharmaceutical and nonpharmaceutical interventions, although medication use is often an adjunct to a therapeutic lifestyle intervention, more than as the primary treatment. This comes about with the recognition that medication is primarily aimed at disease or risk modification, whereas a more upstream lifestyle change is targeted for long-term management.
Deprescription is a response to the overuse of medications (polypharmacy) that has become commonplace in modern affluent societies, particularly in the elderly. Achieving the complex balance between managing disease and avoiding medicine-related problems may require discontinuing prescribed medicines. Deprescribing techniques have, thus, arisen to assist patients in stopping medications that not only may cause harm, but are also unlikely to result in benefit. Although only in their infancy, such skills are likely to become a standard procedure in managing chronic diseases in the future. 16
Whereas all the usual counseling skills, such as motivational interviewing, health coaching, interpersonal relationship training, cognitive behavior therapy, and self-management training, are necessary in LM, they may not be sufficient for dealing with behaviors and the environments driving chronic diseases. Management may, thus, require a lateral shift, leading to different procedures, such as group education and shared medical appointments (SMAs), as discussed below, and acknowledging that this is still a work in progress.
Tools (the Materials)
Although technology has introduced new problems into the health arena (such as through technology-induced pathology discussed above), it has also provided tools that can be used in clinical practice. New and developing devices help track and monitor signs and determinants related to lifestyle such as blood pressure, blood glucose, and physical activity levels. Digital tools can monitor and prompt action related to lifestyle, such as reducing sitting time, by alerting the user. Improvements in technology have given rise to new devices and developments called mHealth or health care and public health practices supported by mobile devices and other advances in telemetry (see Table 3).
Lifestyle Medicine Tools.
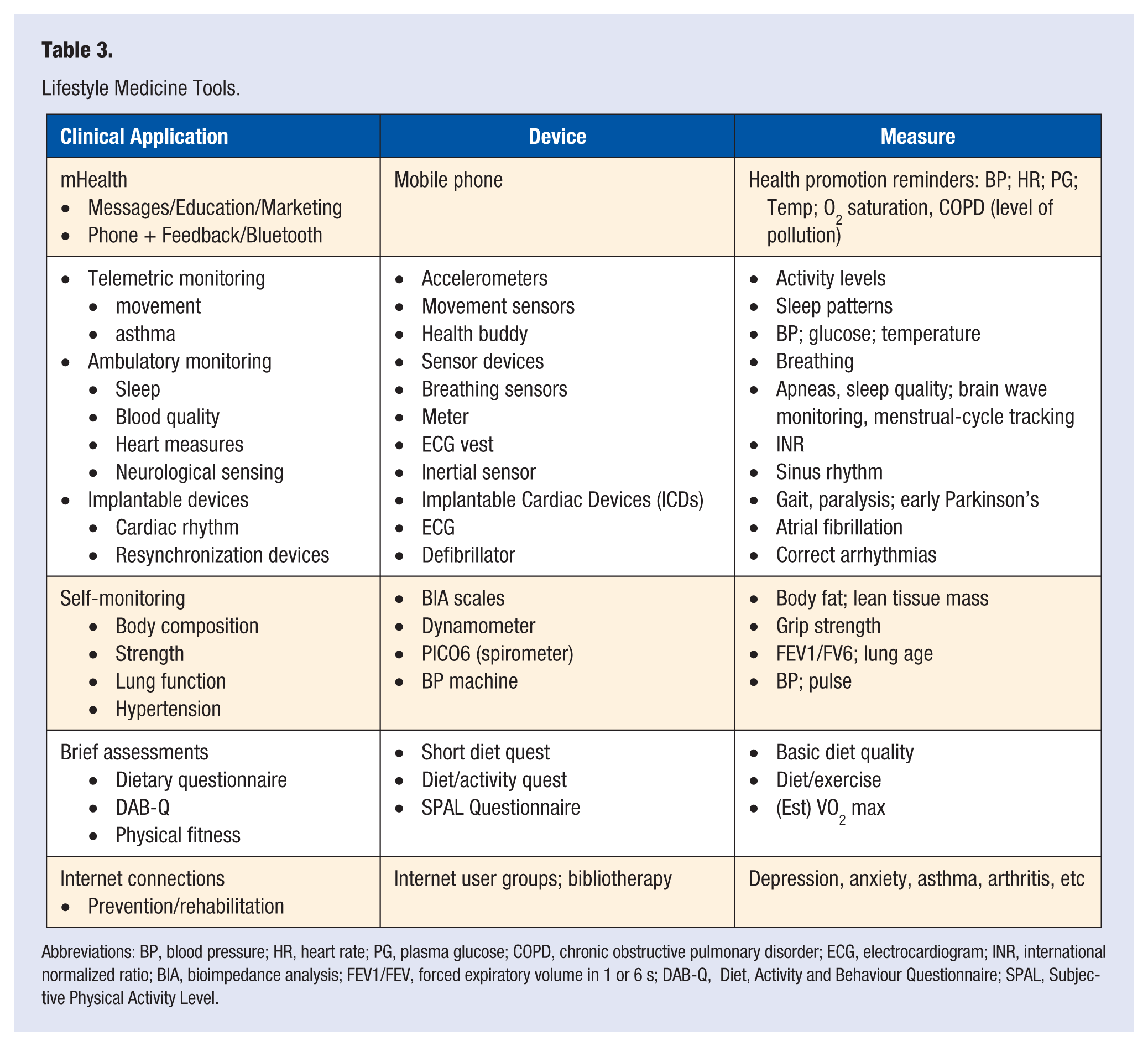
Abbreviations: BP, blood pressure; HR, heart rate; PG, plasma glucose; COPD, chronic obstructive pulmonary disorder; ECG, electrocardiogram; INR, international normalized ratio; BIA, bioimpedance analysis; FEV1/FEV, forced expiratory volume in 1 or 6 s; DAB-Q, Diet, Activity and Behaviour Questionnaire; SPAL, Subjective Physical Activity Level.
Limited evaluations of mHealth devices have appeared in the literature since 2003. At least 2 systematic reviews of such devices to date have highlighted the potential of these as a new set of tools for chronic disease management.17,18 A further review notes that “increasing adherence may have a greater effect on health than improvements in specific medical therapy.”19 (p 31) Well-controlled studies comparing adherence with mHealth devices compared with prescriptive advice controls typically show a 50% improvement in adherence from the former, more than justifying these for chronic disease management. For example, adherence to smartphone food tracking for weight loss is higher than that for traditional food diaries.20,21
Mobile connective technology holds promise as a scalable mechanism for augmenting the effect of physician-directed weight loss treatment. 22 SMS messages are the most popular current mHealth devices, used for medication reminders, education, or information about disease management. Simple SMS reminders or information about new programs or treatments are not only effective, but also cost-effective. Fine targeting combined with a personalized invitation from the patient’s GP could hold the key to better long-term chronic disease management in a number of disease areas. 23
Other mHealth devices include mobile phones plus software or applications, specific medical telemetry devices, or phone plus wireless or Bluetooth-compatible devices. Between them, these not only deliver education and reminders but also monitor functions such as blood pressure, heart rate/rhythm, and blood sugars for patients and providers.
Multiple outcome measures were used in the most recent review, 18 including usability, feasibility, and acceptability of the mHealth tools studied as well as adherence and disease-specific outcomes. Examples of improved management included reduced glycated hemoglobin, reduction in hyperglycemic events, improved lung function, reduced blood pressure, better use of nebulizers, improved fitness levels, and so on. mHealth tools have also been found to increase self-care awareness and knowledge, improve patient confidence to monitor symptoms and signs of chronic diseases, and decrease anxiety about disease. Improvements were noted across all age and socioeconomic categories. However, as might be expected, take up and use by adolescents was shown to be particularly effective.
Significantly, an mHealth system between the patient and provider was less burdensome and judgmental compared with face-to-face contact, making such tools likely to be even more effective in a SMA context (see below) or with individuals who are apprehensive of the doctor-patient environment in a closed setting, such as indigenous individuals or people of low health literacy.
The future for the management of chronic long-term conditions and the potential for lifestyle-related disease management through mHealth is encouraging but somewhat unclear. Questions that need to be considered are the following: Which mHealth devices have most utility? Who is responsible for the incoming data? and What frequency of contact is required. There are now telemetry tools such as movement sensors, portable sleep monitors, bioimpedance analysis scales, grip-strength dynamometers, pulse measures, and other tools for self-monitoring, many of which are in the form of wearable devices. 24 There are also skills for motivation, brief assessments, self-care measures (primary prevention), and self-management measures (secondary/tertiary prevention) that expand the prescriptive environment developed for acute disease. Instantly accessible Internet assistance, self-help groups, and virtual games provide further assistance.
Procedures (the Actions)
A procedure in clinical practice is a sequence of steps to be followed in establishing a course of action. Examples of evidence-based procedures specific to an LM approach are weight loss programs, quit smoking programs, drug or patch therapy, meditation classes, and art therapy. Other examples include sleep hygiene, light therapy, chronic pain management programs, occupational health and safety, and self-help programs such as Alcoholics Anonymous and Narcotics Anonymous. Possible future processes include fecal microbial transplants or diet therapy for recolonization of the gut microbiome. Other new or innovative procedures currently on the fringe of LM practice are discussed in what follows.
Self-management Training
Self-management is an important part of chronic disease management. Training is at different levels, from individual assistance by a health professional 25 to group learning processes. 26
Shared Medical Appointments
At a conventional level, it has been assumed that the clinical process of one-on-one (1:1) consulting in medical practice (despite the lack of data supporting this over other forms of clinical engagement) would continue to play the part in chronic disease management that hitherto it has done for acute diseases and injury.
Yet chronic diseases and conditions have distinct requirements over acute care. Consequently, short consultations, as covered by health systems determined in an acute disease era, are unlikely to be wholly appropriate for an era of chronic diseases. Health education in groups, with an experienced leader (such as a diabetes educator, dietitian, exercise physiologist, or other health care professional) arose to help overcome these problems. But group education lacks medical input. Personal consulting, on the other hand, has medical input but lacks the educational component, time available with the doctor, and peer support associated with group education.
SMAs are “consecutive individual medical visits in a supportive group setting where all can listen, interact, and learn.”27 (p 27) These have been used as an adjunct clinical approach now in several countries.28,29 They provide more time with the doctor, faster access to care, increased peer support, and greater opportunity for self-management. SMAs sit between clinical 1:1 care and group education, as shown in Figure 2. In the future, they are likely to become a standard procedure in clinical LM.

Where shared medical appointments fit.
Telephone Triaging
Telephone triaging is a system used in an increasing number of centers in the United Kingdom to speed up the process of consulting with a doctor or appropriate allied health professional and utilize the doctor’s time to better manage the 21st century tsunami of chronic diseases in primary care. Because this requires more than just a cursory 10-minute consultation and prescription, which generally has been appropriate for most acute infectious disease episodes, screening by phone enables others in the medical center (initially a receptionist, then a nurse or allied health professional) to triage cases into different levels of need, with different health professionals assigned to counsel for low-acuity chronic disease management cases, leaving the physician to deal with higher-acuity cases. This, then, allows for assessment of medical issues before utilizing valuable resources. It also means that patients suffering long-term conditions, which require more attention and self-management opportunities, can get the required level of help while managing limited resources.
Community Referrals
There is a range of community activities, interests, and services in a community, either broadly or narrowly related to chronic diseases. Clients are referred to these in programs such as Act-Belong-Commit (ABC), which is a community mental health initiative developed in Western Australia. 30 A list of community services is combined with a screening process to enable referral from LM practitioners, either through SMAs or in standard consultations. Referrals can be to professional internet sites, such as http://www.beyondblue.org.au or http://www.blackdoginstitute.org.au for depression, or in the form of a “Green Prescription” for physical activity developed in New Zealand. 31 An example of a green prescription script based on Australian National Physical Activity guidelines to be filled in by the patient and physician is shown in Figure 3.
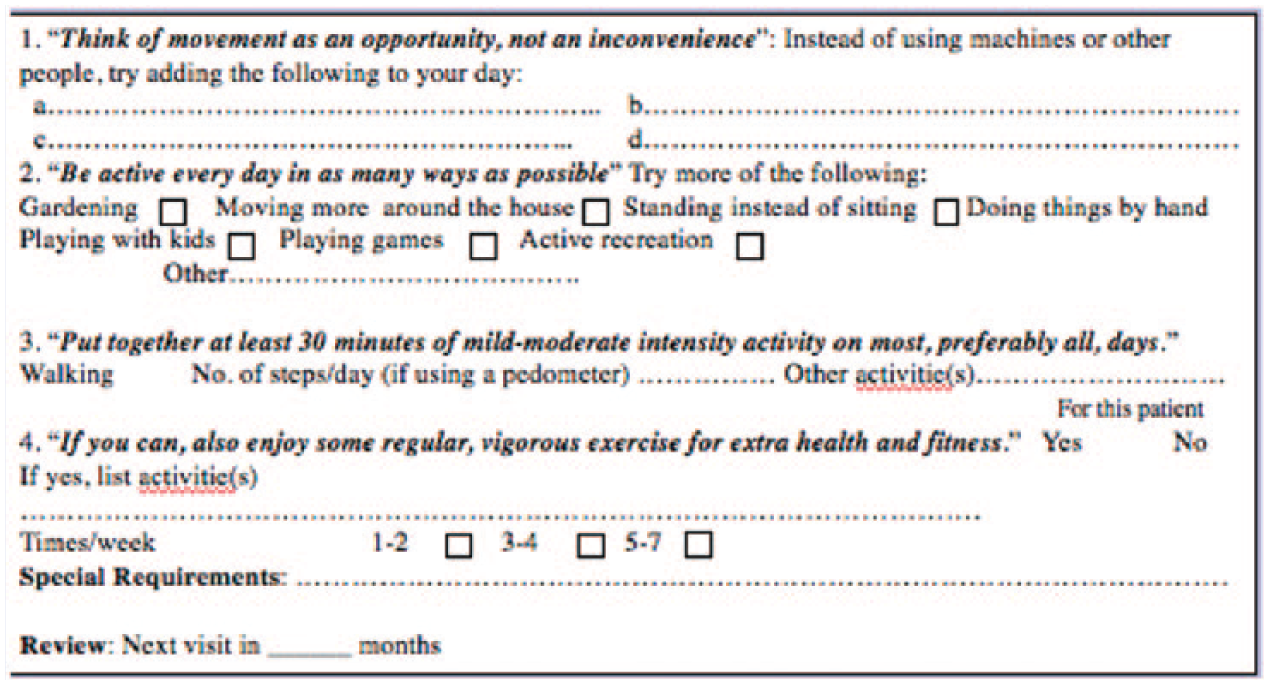
An example activity script.
Eduventures
Eduventures are a new concept in experiential learning developed in Australia to help bring health professionals and patients together over an extended period (2-7 days) of interaction combined with continuing professional development training during an extended physical activity. These include trail and beach walking, kayaking, skiing, sight-seeing, and cycling, generally from point A to point B, as a form of pilgrimage. Adventures and interactions between providers and patients are carried out during the day, lectures and group discussions are held at night and mornings, sometimes around a campfire, in cabins, or meeting places along the way. Eduventures offer the unique opportunity of walking the talk in relation to lifestyle behaviors and health (Figure 4).

Lifestyle medicine Eduventures for patients and providers.
Summary
Rather than being a departure from conventional practice, LM knowledge, skills, tools, and procedures provide an adjunct approach to managing lifestyle and environmental determinants of much modern chronic disease. Although still a work in progress, LM fits a role between clinical medicine and public health, enticing clinicians to consider both the underlying biological mechanisms and more distal environmental determinants of chronic disease than treating risk factors. Self-management, SMAs, total telephone triaging, and educational adventures (Eduventures) provide adjunct procedures for conducting LM consultations. New tools, such as mHealth, are useful to capitalize on modern technological developments and increase treatment options. Undoubtedly, the field will expand as further research assessing these ideas bears fruit.