
Abstract
Background. Increasing evidence suggests that vigorous physical activity (VPA) in youth may yield greater health benefits than moderate (MPA) or moderate-to-vigorous physical activity (MVPA). The purpose of this review was to assess the relationship between PA intensity and body composition, cardiorespiratory fitness (CRF), and cardiometabolic (CM) biomarkers in youth. Methods. We conducted a systematic review of observational studies examining PA intensity and selected health outcomes in youth aged 6 to 18 years. Forty-five articles were selected for final review. Results. VPA was more strongly associated with reduced body fat and central adiposity compared with MPA and/or MVPA. Additionally, VPA was more strongly associated with increased CRF when compared with lower intensities. Findings were inconclusive between all PA intensity levels and CM biomarkers, and several significant relationships observed for VPA were attenuated when controlling for CRF. Conclusions. A potential VPA dose is identified as yielding favorable health benefits in adiposity and fitness. While CM biomarkers were not consistently associated with PA intensity level, the literature suggests VPA may yield health benefits above those received from MPA for reduced adiposity and improved CRF. This review highlights the need for longitudinal observational and experimental studies to determine optimal VPA dose for CM health in youth.
‘Accumulating evidence suggests that VPA [vigorous physical activity] may be more beneficial than moderate PA (MPA) for several health outcomes among youth.’
Among youth, substantial evidence has documented that physical activity (PA) is associated with several favorable health outcomes, including body composition, fitness, and an optimal cardiometabolic (CM) profile.1,2 On the weight of this evidence, the US Department of Health and Human Services (USDHHS) developed PA guidelines, which recommend that youth engage in 60 minutes of moderate-to-vigorous PA (MVPA) daily. 3 Evidence from several observational studies supports that 60 minutes of MVPA per day is a sufficient dose to elicit reductions in obesity, increases in fitness, and improvements in CM biomarkers indicative of chronic disease.4-7 However, only one-fourth of youth report achieving this 60-minute MVPA recommendation, 8 with objective assessments indicating considerably fewer. 9
Accumulating evidence suggests that VPA may be more beneficial than moderate PA (MPA) for several health outcomes among youth.10-12 This has been observed in adult populations, where a PA intensity dose-response relationship has been demonstrated for favorable health outcomes.13-15 As a result, PA recommendations for adults include a specific dose for VPA. 9 However, among youth no specific dose for VPA exists in the current PA guidelines. 3
While previous reviews have assessed the influence of PA intensity on health outcomes among youth, many included self-reported measures of PA.11,12 Considering the ubiquitous use and superiority of objectively measured PA tools and more recently published studies, an updated review of studies evaluating the association between PA intensity and health outcomes among youth is warranted. Thus, the purpose of this review is to summarize and evaluate the scientific literature on studies assessing the impact of PA intensity on adiposity, cardiorespiratory fitness (CRF) and CM biomarkers in the youth population. Our hypothesis is that the studies in this review will demonstrate that VPA is a stronger predictor of adiposity, CRF, and CM biomarkers compared with lesser PA intensities. As such, the aim of this study is to provide an evidence base from which VPA-specific recommendations may be developed for youth.
Methods
Four electronic research databases were searched (Web of Science, PubMed-Medline, CINAHL Complete, and Physical Education Index) to identify peer-reviewed articles assessing the effect of PA intensity on health outcomes in youth. Search terms were categorized into 4 main domains: activity, age group, mode of measurement, and health outcome. The following keywords were used in varying combinations: activity (eg, “physical activity” OR “exercise” OR “sport” OR “dance”) AND youth (eg, “child” OR “adolescent” OR “teen”) AND objective monitoring (eg, “accelerometer” OR “heart rate monitor”) AND health outcomes (eg, “BMI” OR “adiposity” OR “fitness” OR “performance” OR “blood pressure” OR “cholesterol” OR “triglycerides” OR “glucose” OR “insulin”). Age group was limited to youth aged 6 to 18 years. There were no restrictions for publication date. In order to be eligible for analysis the studies must have satisfied the following inclusion criteria:
Observational study design (eg, cohort or cross-sectional)
Utilized objective measures of PA (eg, accelerometers or heart rate monitors)
Published in peer-reviewed journals in the English language
Intervention studies were not included, as the focus of this review is on the benefits of PA incorporated into daily activity as opposed to the effects of acute changes in PA over a limited duration. In addition, all studies must have independently evaluated and reported the relationship between VPA and health outcomes of interest. For example, studies that assessed MVPA but did not evaluate VPA separately were excluded. Moreover, accelerometer validation studies as well as those assessing PA as an outcome variable were excluded. Studies drawing from the same cohort were included if they reported different outcomes.
Data Extraction
Data were extracted by the primary author (MG) from all selected articles, including sample size, participant demographics (age, sex, race/ethnicity, country), and the identified cohort when applicable. Information on PA assessment methods was also gathered, which included details regarding the assessment tool (accelerometer model) and PA intensity cut-points (eg, accelerometer counts). Statistical results describing the association between VPA and selected health outcomes were extracted to examine the magnitude and directionality of the relationship. For studies that also assessed the relationship between MPA and/or MVPA for the selected health outcomes, similar statistical information was extracted for comparison purposes.
Two additional reviewers (SM and CB) interpreted the statistical data to determine the independent associations of PA intensities (MPA, MVPA, VPA) with health outcomes. In the case where partial correlations and regression data were both reported, results from regression models were chosen to represent the relationship between PA intensity and the health outcome of interest. Studies only reporting unadjusted bivariate associations were removed from the review, as established covariates were not adjusted for, to reduce bias in the findings.
Results
A flowchart describing the study selection process is depicted in Figure 1. Initial searches for all databases yielded a total of 1691 records. Titles and abstracts were examined, and of these, 1566 were excluded yielding 125 articles eligible for the initial review. After a full-text review, 46 articles were eliminated for failing to meet inclusion criteria such as it did not assess VPA (54%; n = 25) or did not assess health outcomes of interest (22%, n = 10), resulting in 79 articles for further review. Of these, an additional 34 articles were removed for reasons including assessment of PA intensity as an outcome variable (59%; n = 20) or failing to adjust for covariates (20.6%; n = 7), resulting in 45 articles eligible for the final review.
Flowchart of study selection and ascertainment processes.
Demographics
Participant demographics are presented in Table 1. Geographical locations varied across the studies with 7 conducted in the United States,16-22 4 in Canada,23-26 and 33 in Europe.27-57 One study was conducted internationally 7 and the final study did not specify location. 58 Sample sizes varied considerably ranging from 36 to 6539 participants.7,38 A majority of articles (~96%) used a sample that included children and adolescents of both sexes and the remaining studies consisted of female-only 16 or male-only 57 samples. Several individual studies were derived from numerous large-scale studies, including the European Youth Heart Study (EYHS; n = 6)31,32,41,42,44,46 and Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA; n = 6).33,35,36,39,40,54
Sample Demographics From Articles Reporting the Relationship Between Moderate Physical Activity, Moderate-to-Vigorous Physical Activity, and Vigorous Physical Activity and Measures of Body Composition, Cardiorespiratory Fitness, and Cardiometabolic Biomarkers in Youth.
Abbreviations: y, year; N, population size; n, sample size; NR, not reported; OW, overweight; OB, obese; RCT, randomized control trial; NW, normal weight; BMI, body mass index; PA, physical activity; CM, cardiometabolic; %BF, percent body fat; SGA, small for gestational age; NHW, non-Hispanic white; NHB, non-Hispanic black; CRF, cardiorespiratory fitness; UH, unhealthy; H, healthy; A/PA, Asian/Pacific Islander; AA, African American; NA, Native American; ES, elementary school; MS, middle school; HS, high school.
Cohorts: QUALITY, Quebec Adiposity and Lifestyle Investigation in Youth; EYHS, European Youth Heart Study; HELENA, Healthy Lifestyle in Europe by Nutrition in Adolescence; IDEFICS, Identification and prevention of Dietary- and lifestyle-induced health EFfects In Children and infantS; AFINOS, La Actividad Fı’sica como Agente Preventivo del Desarrollo de Sobrepeso, Obesidad, Alergias, Infecciones y Factores de Riesgo Cardiovascular en Adolescentes: Physical Activity as a Preventive Agent of the Development of Overweight, Obesity, Infections, Allergies and Factors of Cardiovascular Risk in Adolescents; PACE+, Patient-Centered Assessment and Counseling for Exercise Plus Nutrition Project; SPEEDY, Sport, Physical Activity and Eating Behaviour, Environmental Determinants in Young People;
Outcome Variables
Because of varied methods of statistical reporting, results were categorized according to the directionality and statistical significance of the relationships for comparison within each intensity level. Magnitudes of the associations are listed in Table 2, which includes all reported relationships regardless of statistical significance. Outcomes are presented separately by sex, age, PA measurement modality, and/or analytical method employed within a study. A representation of proportional directionality of associations between PA and all health outcomes are summarized in Tables 3-5.
Reported Relationships Between Moderate Physical Activity, Moderate-to-Vigorous Physical Activity, and Vigorous Physical Activity and Measures of Body Composition, Cardiorespiratory Fitness, and Cardiometabolic Biomarkers in Youth.

Abbreviations: PA, physical activity; BMI, body mass index; CRF, cardiorespiratory fitness; CM, cardiometabolic; y, year; MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; VPA, vigorous physical activity; n, sample size; OR, odds ratio; AA, African-American; N/R, not reported; r, Pearson partial correlation; SBP, systolic blood pressure; ns, nonsignificant; TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglycerides; %BF, body fat percentage; β, standardized regression coefficient; min, minute; sec, second; WC, waist circumference; GEE, generalized estimating equation; VO2peak, peak volume of oxygen consumption; MetS, metabolic syndrome; min/d, minutes per day; HbA1c, glycated hemoglobin; IR, insulin resistance; TBF, total body fat; AFM, abdominal fat mass; abs, absolute; kg, kilogram; LBM, lean body mass; DBP, diastolic blood pressure; ow, overweight; ob, obese; VO2max, maximum volume of oxygen consumption; FFM, fat-free mass; BIA, bioelectrical impedance analysis; CVD, cardiovascular disease; Q, quartile; TBF, total body fat; INS, insulin sensitivity; FMI, fat mass index; LMI, lean mass index; DXA, dual energy x-ray absorptiometry; SF, subcutaneous fat; MAP, mean arterial pressure; ROC, receiver operating characteristic.
Cohorts: GEMS, Stanford Girls Health Enrichment Multisite Studies; QUALITY, Quebec Adiposity and Lifestyle Investigation in Youth; HAPPY, Health and Physical Activity Promotion in Youth; EYHS, European Youth Heart Study; HELENA; Healthy Lifestyle in Europe by Nutrition in Adolescence; NHANES, National Health and Nutrition Examination Survey; AFINOS, La Actividad Fı’sica como Agente Preventivo del Desarrollo de Sobrepeso, Obesidad, Alergias, Infecciones y Factores de Riesgo Cardiovascular en Adolescentes: Physical Activity as a Preventive Agent of the Development of Overweight, Obesity, Infections, Allergies and Factors of Cardiovascular Risk in Adolescents; ACLS, Aerobic Center Longitudinal Study; PACE+, Patient-Centered Assessment and Counseling for Exercise Plus Nutrition Project; SPEEDY, Sport, Physical Activity and Eating Behaviour, Environmental Determinants in Young People
Standardization not reported.
Log-transformed.
Unstandardized.
p < 0.05.
p < 0.01.
p < 0.001.
Summary of Articles Reporting Beneficial, Not Beneficial, or No Association Between Physical Activity Intensity and Body Mass Index/Body Composition Outcomes in Youth.
Abbreviations: MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; VPA, vigorous physical activity.
Summary of Articles Reporting Beneficial, Not Beneficial, or No Association Between Physical Activity Intensity and Cardiorespiratory Fitness Outcomes in Youth.
Abbreviations: VO2peak, peak volume of oxygen; VO2max, maximal volume of oxygen; Wmax, maximal power output; MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; VPA, vigorous physical activity.
Summary of Articles Reporting Beneficial, Not Beneficial, or No Association Between Physical Activity Intensity and Cardiometabolic Biomarker Outcomes in Youth.
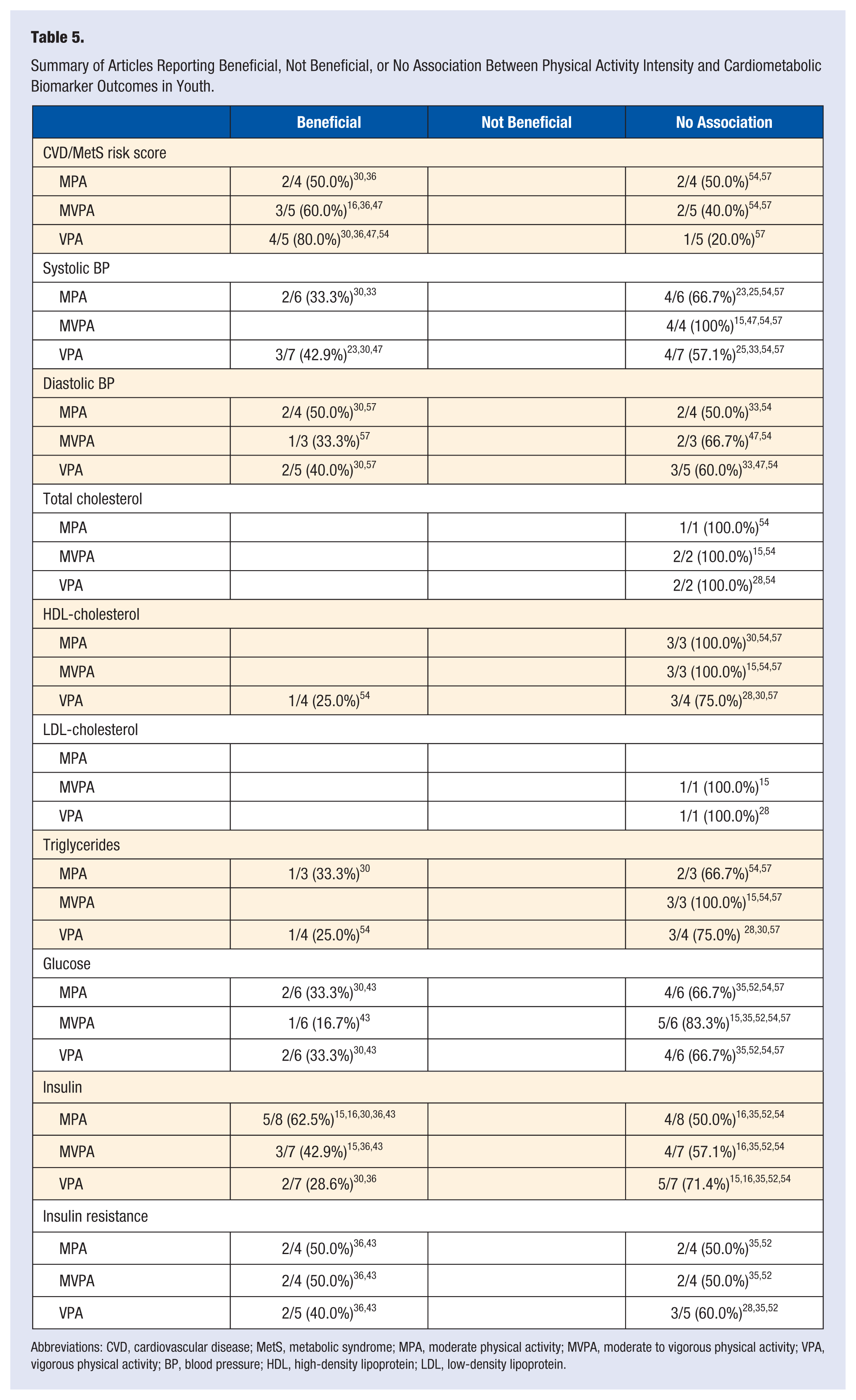
Abbreviations: CVD, cardiovascular disease; MetS, metabolic syndrome; MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; VPA, vigorous physical activity; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Body Composition
Body Mass Index
Nineteen studies examined the link between PA intensity and body mass index (BMI). * Eleven of the 19 associations tested indicated that VPA was significantly, negatively correlated with weight status, and the magnitude was greater than the relationship between MPA or MVPA and BMI for both sexes. † Two studies45,57 demonstrated that VPA was more strongly associated with BMI only among boys,45,57 with MVPA being a stronger predictor among only girls. 45
The remaining 8 associations from 7 studies did not demonstrate a significant relationship between PA and weight status, regardless of intensity.22,27,32,36,38,53,55 Despite these nonsignificant findings, there were several noticeable trends between PA intensity and weight status. Three of these 8 associations found VPA to be a stronger negative predictor of weight status,27,32,53 whereas 4 reported MPA to be either more strongly related to weight status than VPA or of equal magnitude with VPA.36,38,55 Mixed results were found for the remaining study as there were no consistent trends observed. 22
Body Fat
Seventeen studies addressed PA intensity and its connection with percent body fat (%BF). ‡ Of these studies, 13 (~76%) demonstrated that VPA was negatively associated with %BF and at a greater magnitude than the relationship between MPA or MVPA and %BF. § One of the 17 studies 17 found that MPA was more strongly associated with %BF than VPA while another study 31 found MPA and VPA similarly associated in magnitude. For 1 report 25 that employed various analytical techniques (eg, partial correlation, logistic and mean regression), each technique observed a different PA intensity more strongly and negatively predicting percent body fat. The remaining study found a nonsignificant relationship between PA intensity and percent body fat. 22
Two studies38,47 assessed the relationship between fat mass index (FMI) and PA intensity. One study found significant, negative connections between the 2 variables for both VPA and MVPA, with a strong association reported with VPA. 47 Although the other study reported nonsignificant findings, VPA was more strongly associated with FMI than MPA or MVPA. 38
Central Adiposity
Seventeen studies assessed the relationship between PA intensity and a measure of central adiposity ‖ with 2 studies addressing 2 separate central adiposity measures,33,50 resulting in a total of 17 associations. Eleven of the 17 associations were statistically significant, ¶ of which 10 demonstrated that VPA was a stronger negative predictor for central adiposity compared with MPA or MVPA. # Of these, one study 36 found this relationship only among females. The remaining association reported MVPA as a stronger negative predictor compared to VPA. 19
Six of the 17 associations were nonsignificant for all PA intensities with central adiposity.17,24,31,53,55,58 Albeit nonsignificant, 4 of these 6 relationships reported a stronger link between VPA and central adiposity compared with MPA or MVPA.24,31,53,55 The remaining studies found MVPA to be a stronger negative predictor of central adiposity compared with MPA or VPA.17,58
Ortega et al 41 showed that when the association between PA intensity and central adiposity was stratified by CRF level, findings were contradictory. Among youth with a high CRF level, MPA and MVPA yielded significant positive associations with central adiposity, but this relationship was reversed and nonsignificant for those with low CRF levels. 41
Age and Sex
Eight articles presented information on sex differences in the relationship between PA intensity and markers of body composition, which yielded mixed findings.21,22,28,35,36,39,45,56 For youth younger than 12 years, Blaes et al 28 indicated that a significant, inverse correlation was observed between VPA and %BF for males, but not females. In contrast, Rowlands et al 45 reported females exhibiting a stronger relationship between VPA and %BF than males, although nonsignificant. Still, Fairclough et al 56 showed equal odds of normal weight status from VPA engagement for both sexes.
Similar evidence was presented for youth older than 12 years. Two articles reported stronger correlations observed between VPA and body composition markers for males than females.35,39 Significant inverse relationships between VPA and body composition markers was observed for females but not males in another study, 36 and the last article reported similar findings irrespective of sex. 21 Interestingly, Treuth et al 22 found that while all non-significant, elementary and middle school-aged females exhibited stronger relationships between VPA and markers of body composition than males. 22 However, this observation was switched in high school–age youth.
Cardiorespiratory Fitness
Sixteen studies assessed the link between PA intensity and CRF. ** Fifteen of the 16 studies reported a significant, direct relationship between PA intensity and CRF with the remaining study demonstrating mixed findings. 30 Ten articles demonstrated that VPA was more strongly associated with CRF compared with MPA or MVPA. †† Three of the 15 studies found MPA or MVPA to be more strongly and positively associated with CRF compared with VPA.17,48,49 Interestingly, 2 studies found VPA to be a significant negative predictor of CRF.20,30
Age and Sex
In youth aged 6 to 7 years, Dencker et al 49 found that MPA was significantly related to CRF for both males and females, but only males retained this significance as intensity increased. Similarly, age at 12 (±2) years showed a significant direct correlation between MPA and CRF in females only, while a significant inverse relationship existed between VPA and CRF in males only. 30 For youth older than 12 years, strength of relationship between VPA and CRF was similar for both sexes. However, males displayed stronger relationships at lower PA intensities.36,54
Cardiometabolic Biomarkers and Disease Risk Scores
Cardiovascular Biomarkers
Seven articles evaluated the association between varying levels of PA intensity and cardiovascular biomarkers (systolic blood pressure [SBP; n = 7],24,26,31,34,48,55,58 diastolic blood pressure [DBP; n = 5],31,34,48,55,58 and mean arterial pressure [MAP; n = 1]). 48 Overall, findings from the 7 studies did not suggest that any PA intensity was more strongly related to cardiovascular markers. Among studies assessing SBP as an outcome, 2 studies24,48 reported that VPA was a significant, negative predictor of SBP of a greater magnitude than MPA and/or MVPA, while 2 other studies31,34 reported that MPA was significantly and more strongly, negatively associated with SBP than VPA and/or MVPA. The remaining studies reported a nonsignificant correlation between PA at all intensities and SBP.26,55,58
Of the 5 studies evaluating DBP as an outcome, 2 reported a significant result, one of which 31 indicated MPA as a stronger negative predictor of DBP than VPA and/or MVPA, and the other 58 having significant negative associations for all PA intensities. The 3 remaining articles yielded nonsignificant observations between DBP and PA intensity, with 1 study 48 finding MVPA to be more strongly and inversely related with DBP than VPA, while another 55 finding the association to be equivalent across MPA, MVPA, and VPA. In the final study, it could not be determined which PA intensity potentially resulted in a stronger influence on DBP as only the significance (P value) of the association was reported. 34 The 2 studies examining the link between PA intensity and MAP found both to be nonsignificant with relatively equal magnitudes of association.48,58
Metabolic Biomarkers
Nine studies assessed the relationship between PA intensity and metabolic biomarkers (total cholesterol [TC; n = 3],16,29,55 high-density lipoprotein cholesterol [HDL-C; n = 5],16,29,31,55,58 low-density lipoprotein cholesterol [LDL-C; n = 2],16,29 triglycerides [TGs; n = 5],16,29,31,55,58 glucose [n = 6],16,31,44,53,55,58 insulin [n = 7],16,17,31,36,44,53,55 insulin resistance [IR; n = 4],29,36,44,53 and insulin sensitivity [INS; n = 1]). 36 Of the 5 studies evaluating lipids (TC, HDL-C, LDL-C, TG) as an outcome,16,29,31,55,58 2 studies assessed the influence of a single PA intensity and found nonsignificant associations for both MVPA 16 and VPA. 29 Among the 3 remaining studies, 1 study found that VPA was significantly directly associated with HDL-C and significantly inversely related to TGs, and more strongly linked with these biomarkers than MPA and/or MVPA. 55 The second study found a significant inverse correlation between MPA and TGs, greater in magnitude when compared to MPA and/or VPA. 31 The last study reported nonsignificant associations among all PA intensities. 58
Of the 6 articles that assessed the relationship between PA intensity and glucose,16,31,36,44,55,58 one study assessed the influence of a single PA intensity and found a non-significant association for MVPA. 16 Two of the 5 remaining studies demonstrated that PA intensity was significantly and negatively associated with fasting glucose levels,31,44 with 1 study 44 finding a stronger inverse correlation for VPA, and the other 31 observing a stronger connection between MPA and glucose levels. The remaining 3 studies reported nonsignificant relationships between PA intensity and glucose.53,55,58 Of these nonsignificant findings, 1 study 55 observed VPA to have a stronger negative association with glucose levels compared with MPA and MVPA, and the others had conflicting findings.53,58
Seven studies measured insulin16,17,31,36,44,53,55 as an outcome with only 3 observing a significant and negative association between PA intensity and insulin.16,31,44 Of these significant findings, 1 article 44 reported that VPA was inversely and more strongly related to insulin than MPA or MVPA, while the others showed a stronger relationship for insulin and MPA 16 or displayed similar findings between MPA and VPA. 31 Two of the 7 studies observed a nonsignificant association between PA intensity and insulin, with 1 study 55 demonstrating VPA as a stronger negative predictor of insulin whereas the other 17 found MPA to have a stronger relationship. 17 The remaining 2 studies reported mixed findings between PA intensity and insulin: one found nonsignificant direct correlations for MPA and MVPA whereas VPA demonstrated a nonsignificant inverse correlation, 53 and the other exhibited conflicting results between sexes when stratified by CRF. 36 Among females with low CRF, MVPA exerted a significant and stronger negative influence on insulin levels compared with MPA and VPA. This relationship in females became nonsignificant with increased CRF for all PA intensity levels. Conversely, for males, regardless of the level of CRF, PA intensity was not significantly associated with insulin levels. 36
Four studies assessed the link between PA intensity and IR29,36,44,53 with 1 study assessing the influence of a single PA intensity and found a nonsignificant relationship with VPA. 29 Of the remaining 3 articles, only 1 significant association was reported, which indicated that VPA was a stronger negative predictor of IR compared with MPA and MVPA. 44 Another found conflicting results between the sexes when stratified by CRF. 36 Among females with low CRF, MVPA displayed a significant and stronger inverse association with IR compared with MPA and VPA; however, higher levels of CRF yielded nonsignificant findings for all PA intensities. Among males, nonsignificant relationships were found for all PA intensities and IR. 36 In the remaining report, 53 the influence of PA intensity on IR was conflicting as VPA demonstrated an inverse relationship with IR, whereas a positive relationship was found for MPA and MVPA.
Only 1 study examined the link between PA intensity and INS and found that the results differed by sex when stratified by CRF level. 36 The findings of this study suggested that MVPA significantly and positively influenced INS compared with MPA and VPA only among females with low CRF. This relationship was nonsignificant among females with moderate to high CRF. No association existed among males between any PA intensity and INS regardless of CRF level.
Cardiovascular Disease and Metabolic Syndrome Risk Scores
Five articles evaluated the association between PA intensity and cardiovascular disease (CVD)37,48 and/or metabolic syndrome (MetS)31,55,58 risk score, of which all but one demonstrated significant relationships. 58 Two studies found VPA was more strongly inversely associated with disease risk score than MPA and/or MVPA.48,55 However, the correlations with MPA and MVPA with MetS risk score were nonsignificant for one of these studies. 55 In this report, the magnitude of association between VPA and MetS risk score was substantially attenuated and became nonsignificant after further adjustment for CRF. 55 Another article found that across all quintiles of PA (highest PA level as referent), MVPA demonstrated a significant negative and stronger influence on CVD risk score compared with MPA and VPA, however, only occurring among females. 37 In males, MPA was a significant negative predictor of CVD risk score compared with MVPA and VPA, although only among those with the lowest level of PA. 37 The remaining study showed both MPA and VPA to be significantly and negatively associated with MetS risk score, with impact appearing to be similar in magnitude. 31
Age and Sex
Three articles reported outcomes for PA intensity and CM biomarkers by sex.36,37,48 Tanha et al 48 showed that males and females, aged 7.9 to 11.1 years, had relatively similar, significant correlations between VPA and CVD risk score, as well as MVPA and CVD risk score. The 2 other articles, both by Jiménez-Pavón et al,36,37 found mixed results. In youth aged 6 to 9 years, females had higher CVD risk scores than males across all PA intensities. 37 While CVD risk for both sexes generally declined with increasing PA quintiles, it increased with increasing MPA in females. Additionally, the odds ratio retained significance for females as PA quintiles increased, whereas males lost significance. 37
In the second report concerning youth older than 12 years, Jiménez-Pavón et al 36 noted that partial correlations yielded stronger significant findings for females regarding the connection between VPA and insulin and INS. However, males had a stronger, significant correlation between VPA and IR, and a stronger nonsignificant correlation between VPA and glucose. 36 When intensity decreased, these relationships for males became nonsignificant, but females retained significance, although strength was reduced but still stronger than respective results for males. When reporting regression coefficients, stronger nonsignificant associations for females were demonstrated concerning MPA and MVPA versus insulin, INS, and IR, with males showing a stronger nonsignificant relationship between VPA and these biomarkers. 36
Discussion
The purpose of this review was to systematically examine the current literature on the associations between PA intensity and body composition, CRF, and CM biomarkers in youth. Major findings of this study were (1) VPA was more strongly negatively associated with body composition, and more strongly positively associated with CRF compared with MPA or MVPA, (2) no specific PA intensity appeared to consistently and more strongly associate with CM biomarkers, and (3) among the majority of studies demonstrating that VPA had a stronger relationship with adiposity and CRF outcomes, participants often engaged in at least 10 minutes of VPA, potentially suggesting that 10 minutes of VPA may be a sufficient dose for youth.
In a previous review of PA intensity and health outcomes related to adiposity and fitness, which examined 17 observational studies published between 1999 and 2009, authors noted that a shorter duration of VPA yielded a stronger association with body fat than a longer duration of MPA. 11 A more recent review remarked that every minute of VPA yields the same improvements in body composition as 2 or 3 minutes of MPA. 12 In our expanded and updated review, among the studies that found VPA significantly related to BMI, body composition, and central adiposity compared with other PA intensities, a majority reported participants engaging in an average of at least 10 minutes of VPA. ‡‡ Considering that the “dose” of VPA was relatively modest in many of these studies, as well as the sporadic nature of PA in youth with brief intermittent bouts of VPA, 61 it is conceivable that VPA may be more attainable simply because a health-improving dose is less time-consuming to attain. Therefore, it could be suggested that VPA should be promoted independent of MPA as a behavior. Additionally, Martinez-Gomez et al 62 and Katzmarzyk et al 7 conducted receiver operating characteristic analyses on activity dose and identified that 17 and 20 minutes of VPA in boys and 9 and 11 minutes of VPA in girls, respectively, mitigated the risk of being overfat and/or obese, highlighting possible sex differences in VPA recommendations.7,62
In line with previous studies, we found that VPA was consistently more strongly associated with CRF compared to MPA and/or MVPA. This finding has also been demonstrated among exercise training studies with intensities greater than 70% of age-predicted maximum heart rate (vigorous intensity) eliciting significant changes in CRF. 3 A prior review by Ortega et al 63 on fitness and health outcomes in youth discussed the importance of VPA to increase CRF for favorable changes in adiposity and CM profile. Additionally, among adults substantial evidence indicates that there is a dose-response relationship between PA intensity and CRF, with the greatest improvement in CRF found among very high intensities (90% to 100% VO2max). 64 Importantly, CRF has been demonstrated to be a strong predictor of morbidity65,66 and mortality67-69 among adults, and some evidence indicates that CRF tracks modestly from childhood to adolescence to adulthood.70-72 As a result, it is reasonable to suggest that increasing CRF among youth should be a public health priority; as such, including a dose of PA that may elicit improvements in CRF (ie, VPA) in the PA guidelines is warranted. Among the studies in this review that found VPA to be more strongly associated with CRF, a majority described youth engaging in at least 10 minutes of VPA (range 12-46 minutes), suggesting this dose of VPA may be a good starting point for youth.36,43,46,53-55,60
In contrast to the previous findings of this review, associations between PA intensity and CM biomarkers were equivocal. We did not find a PA intensity (MPA, MVPA, or VPA) that was strongly associated with any of the CM biomarkers consistently when compared with other intensities. VPA did not display a strong relationship with MetS/CVD risk score in youth, and in fact became nonsignificant after controlling for CRF. 55 This finding was echoed for insulin and IR, with higher levels of CRF negating any significant influence of VPA on these CM biomarkers. 36 It is possible that the conflicting findings in our review may be due to the inherent healthiness of children and adolescents. The review by Owens et al 12 suggested that VPA was associated with a more favorable blood lipid profile and glucose-insulin profile. Conversely, inconclusiveness of findings between PA intensity and CM biomarkers was demonstrated in a previous review 6 that examined BP, plasma lipid and lipoproteins, and MetS. However, authors noted that favorable changes in blood lipids and lipoproteins post-exercise intervention were more likely to occur in high-risk participants, indicating that the initial health status of the study population may greatly affect the observed association. 6
In addition, Gutin and Owens 10 in their review of both observational and intervention studies identified fitness and fatness as mediating factors of the relationship between PA and CM biomarkers among youth, noting that PA interventions conducted among overweight and obese youth had a beneficial effect on several CM biomarkers. Conversely, the evidence was limited for PA interventions targeting nonobese youth. 10 However, there is evidence demonstrating the emergence of obesity-related complications in early childhood that includes the premature manifestation of CM risk factors.73-76 Ferreira et al 77 noted in their longitudinal study following 450 participants from adolescence to young adulthood that increases in body fat, declines in CRF, and a greater shift from time spent in VPA to light-to-moderate intensity PA were characteristic of MetS at the age of 36 years. As such, the findings of our review provide additional support for weight control and improving CRF in youth as a preventive measure for future CM disease.
There are several strengths to this review that warrant attention. Few reviews in the past have solely focused on objective PA measurement, which has now become more standardized in PA assessment. We also included CM biomarkers in addition to body composition and CRF, which are often not collectively examined despite their connections. Additionally, this is the first review to identify a possible VPA dose for youth. As with any study, there are also limitations that are worth mentioning. We chose not to examine intervention studies as done in prior reviews,10-12 narrowing our focus to observational studies. Even though not limited to objective measurement tools, we felt these previous reviews provided sufficient support for the changes that high-intensity structured exercise could make over the course of an intervention, and chose instead to focus on larger observational studies that gathered data on VPA when incorporated in normal daily activity. Nonetheless, this review highlights the importance of further conducting PA interventions focused on intensity in youth for future review.
An additional limitation in the observational studies we reviewed also involves variation in method of PA measurement. All articles used accelerometry to measure PA intensity, but accelerometer model, length of wear, and VPA cutpoints varied widely. The Actigraph GT1M model was primarily used (33.3%; n = 15) §§ or one of its predecessors (ActiGraph 7164, MTI 7164, or CSA 7164; 43.9%; n = 18), ‖‖ but even when using the same model, VPA cutpoints applied were inconsistent (eg, 3000 to 4012 counts/min; Actigraph GT1M).20,34 Considering that youth primarily engage in very short periods of VPA at a time, a 60-second or even a 10-second epoch may not adequately differentiate VPA as it is combined with periods of rest or light PA.61,78
In conclusion, while there are certainly benefits to MPA, as evidenced in this review, VPA was a stronger predictor of improved body composition, particularly for reduced body fat and central adiposity, and increased fitness compared with MPA and/or MVPA. These patterns were observed even when findings were nonsignificant. From our results, it appears that a dose of 10 minutes of VPA/day may be sufficient to elicit favorable changes in these health outcomes, with possible differences for male and female youth. However, these suggestions need to be confirmed with rigorously randomized controlled exercise training studies.