
Abstract
The purpose of this systematic review was to summarize and evaluate the impact of physical activity (PA) interventions that were implemented in specific school settings on children’s PA in those settings. Four research databases were searched to identify PA interventions. Of the 13 706 articles identified, 1352 abstracts were screened and 32 intervention studies were reviewed. Five intervention settings were identified (active travel, after school, classroom, physical education, and recess). Among these settings, a greater proportion of positive findings (ie, significant increase in PA) were found in the classroom (75%) and active travel (67%) settings. Additionally, a higher proportion of interventions implemented in these settings were of high methodological quality (active travel [33%] and classroom [33%]). These findings indicate that interventions in active travel and classrooms settings positively influence youth PA. Importantly, as evidenced in this review, evaluating intervention effects in the targeted setting may provide unique information for future researchers to consider when developing school-based multicomponent PA interventions.
‘Among the many approaches that have been tested, multicomponent school-based interventions have been most consistently successful in increasing students’ PA [physical activity]’
Considerable evidence suggests that engaging in physical activity (PA) provides important health benefits for children and adolescents.1,2 Given this, the 2008 Physical Activity Guidelines for Americans indicate that youth should participate in 60 minutes of moderate-to-vigorous PA per day. 3 However, less than 50% of American youth comply with this recommendation. 4 To address this deficiency, many authorities have called for implementation of interventions to increase PA in youth.5,6 Because most young people spend large amounts of time in school, the school setting is seen as an attractive one for implementing PA interventions.7,8
Over the past 2 decades numerous school-based PA interventions have been evaluated.9,10 Among the many approaches that have been tested, multicomponent school-based interventions have been most consistently successful in increasing students’ PA. 11 Such interventions typically have combined strategies in school settings such as physical education classes, transport to school, recess, classroom activities, and after-school programs. While multicomponent interventions have been successful in modifying youth PA, these changes are modest, at best. 12 These small changes may be a result of the study designs employed, which have possibly been limited to the measurement of PA across the school day or entire day. 13 Consequently, evaluating the intervention effects across an extended period of time potentially results in diluted changes in youth PA.
An optimal multicomponent school-based intervention would combine intervention strategies, each of which is known to substantially increase students’ PA in the targeted setting. However, because previous reviews on school-based PA interventions have likely focused on the impact of such interventions on overall daily PA, 13 the effectiveness of these interventions on youth PA in the setting in which the intervention was implemented has not yet been evaluated. To our knowledge, no previous review has been designed to assess the effectiveness of setting-specific interventions on children’s PA levels when observed in those settings. Accordingly, the purpose of this review was to summarize and evaluate the impact of PA interventions that were implemented in specific school settings on children’s PA in those settings.
Methods
Search Strategy and Selection of Articles
The literature search for this review was conducted with the purpose of identifying interventions aimed at promoting PA among youth in various school settings. Five school settings were identified prior to the literature search: active travel, after school, classrooms, physical education, and recess; however, the search was not restricted to these settings, allowing for others to potentially be discovered.
Four electronic research databases were searched (PubMed, Web of Science, Academic Search Premiere, and PsychInfo) to identify interventions aimed at increasing PA among youth. Various combinations of the following keywords were used to identify full-text peer-reviewed articles: (“physical activity” OR “exercise”) AND (“interventions” OR “trials” OR “programs” OR “school interventions”) AND (“afterschool” OR “classroom” OR “breaks” OR “recess” OR “active travel” OR “active transport” OR “physical education”). Bibliographies of articles and review papers identified by the searches were scanned to ensure a thorough collection of the literature. There were no restrictions placed on date of publication or location of the study; however, in order to be included in this review, studies had to meet the following inclusion criteria:
Included a control condition
Evaluated PA as the primary outcome
Implemented in a school setting
Measured PA at baseline and postintervention in the intervention setting
Included participants between ages 3 and 18 years of age
In addition, studies that exclusively measured total day PA were excluded as the intervention effects on youth PA in the setting (eg, active travel, after school, classroom) in which the intervention was implemented could not be ascertained.
Data Extraction
Data extracted from the selected articles included country, study design, sample size, participant characteristics, intervention details (ie, duration, setting, and components), methods used to measure PA, and primary outcomes. Participant information gathered from the studies included age, grade level, and sex and racial/ethnic composition of the sample. The intervention details included information on the duration (eg, number of weeks), the setting where the intervention took place (eg, recess), and the major components of the intervention and any variations across the experimental conditions. Data collected on the methods used to measure PA included all objective (eg, accelerometer) or subjective (eg, survey) tools used to measure PA in the intervention setting. For the primary outcomes, information regarding the intervention effects on PA was extracted for only the setting in which the intervention was implemented. Additionally, if the intervention was effective at increasing PA for the whole sample, the findings were reported as “positive.” If significant intervention effects were specific to a group (eg, males, normal weight) or were not sustained over multiple time periods, the findings were reported as “mixed.” Last, if the intervention did not result in any significant effects on PA the findings were reported as “null.” Following data extraction, the studies were grouped by the settings the interventions targeted (eg, recess), and the methodological quality and levels of evidence were assessed separately for each of the identified settings.
Methodological Quality
Methodological quality was assessed using an established scale, 14 which has been used previously to determine the strength of evidence for the effectiveness of PA interventions among youth. Criteria for the quality assessment can be found in Table 1. Two researchers (SM, MC) independently evaluated each study and scored each criterion (10 criteria for randomized controlled trials [RCTs] and 9 criteria for quasi-experimental studies) as “positive,” “negative,” or “insufficiently described.” Studies receiving a score of “negative” or “insufficiently described” were eventually collapsed into one category for ease of reporting. If any disagreements arose during the process, the authors reached a consensus by discussion.
Methodological Quality Assessment Criteria a .
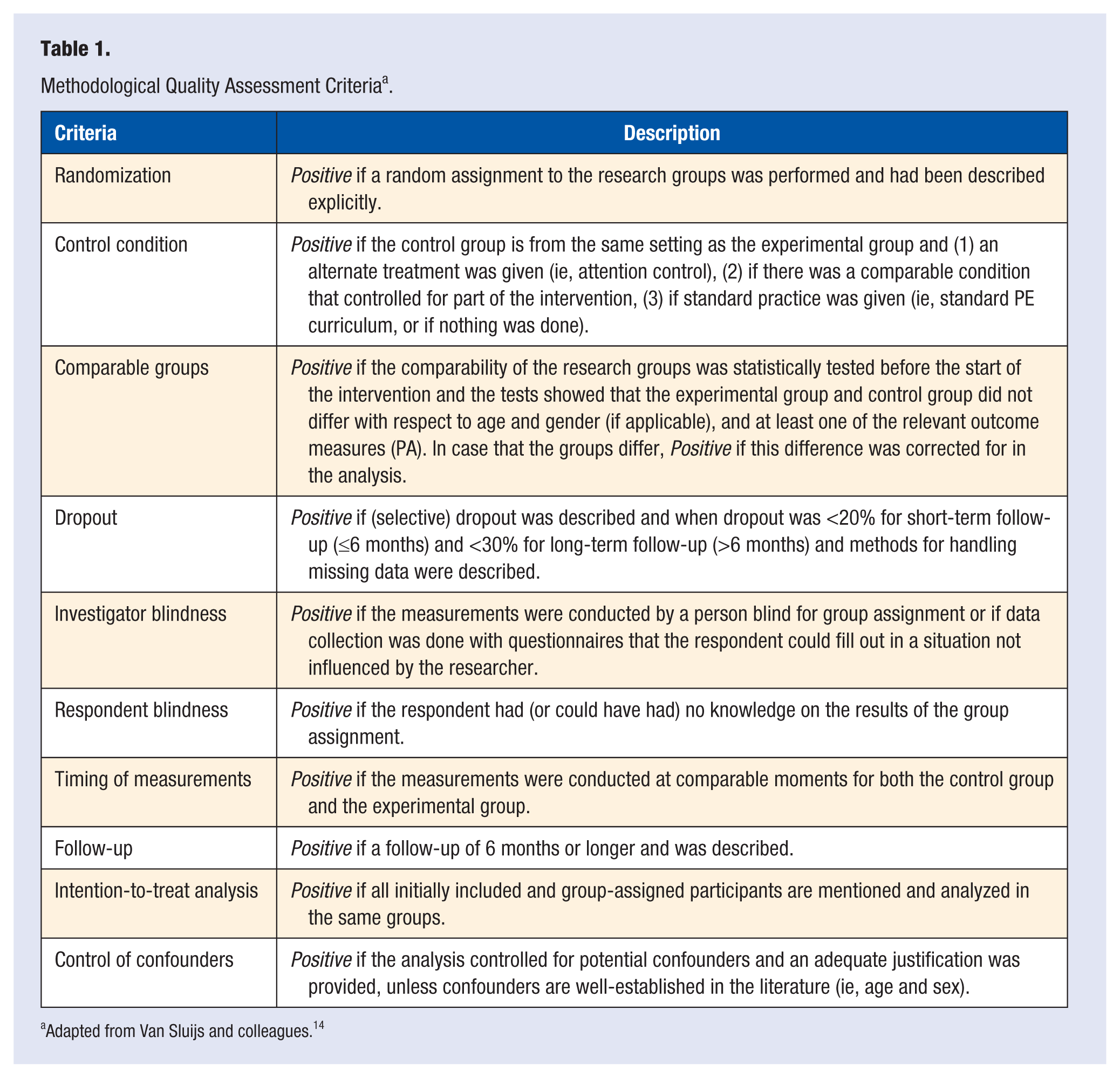
Adapted from Van Sluijs and colleagues. 14
After the methodological quality assessment was completed, 2 of the criteria from the assessment tool, “blinding (investigator)” and “blinding (respondent),” were dropped due to the difficulty of blinding in school settings. As a result, a total of 8 criteria were used to assess methodological quality for RCTs and 7 criteria for quasi-experimental studies. After all the criteria were scored, only the criteria with a “positive” score were tallied for each study. Methodological quality was categorized as either “high” (score ≥5 for RCTs and ≥4 for quasi-experimental designs) or “low” (score <5 for RCTs and <4 for quasi-experimental studies) based on the total number of “positive” scores.
Levels of Evidence
To evaluate the level of evidence for the impact of interventions on youth PA across different settings, a previously established process developed by Van Sluijs et al 14 was used. In addition to assessing the intervention effects, this process also considered the study design, methodological quality, and sample size of the intervention studies. There were 5 possible levels of evidence that could be achieved in this process: strong, moderate, limited, inconclusive, or no. For each of these levels, certain criteria must have been met for the selected intervention studies. First, in order to reach a “strong” level of evidence, 2 or more large (>250 participants) high-quality RCTs with consistent positive findings were needed. Consistent negative findings yielded a “No,” whereas mixed findings resulted in an “inconclusive” level of evidence. If there was only one large high-quality RCT, findings from large low-quality or small (≤250 participants) high-quality RCTs or large high-quality quasi-experimental studies were considered. However, given the less rigorous nature of these studies, consistent positive findings among these studies resulted in only a “moderate” level of evidence. If none of these types of studies were available, then in addition to the one large high-quality RCT, large low-quality and small high-quality quasi-experimental studies were considered. However, only a “limited” level of evidence could be obtained for consistent positive findings. If none of these studies were available for review, then the level of evidence for the effects of PA interventions on youth PA was considered “inconclusive.”
If no large high-quality RCTs were available for review, large high-quality quasi-experimental, low-quality RCT, or small high-quality RCT studies were considered. If there were 2 or more of these studies with consistent positive findings, then the level of evidence was “limited.” If there was only one of these studies available, regardless of the findings (positive, negative, or mixed), the evidence was deemed “inconclusive.” Last, if none of these studies were available for review, then small high-quality and low-quality quasi-experimental studies were considered, and irrespective of the results, the level of evidence was determined to be “inconclusive.” If none of these studies existed in the literature, then it was determined that there was no evidence available to suggest that PA-promoting interventions were effective at influencing PA among youth.
Results
The systematic literature search identified 13 706 unique records, and all titles were screened for relevancy. Of the 13 706 titles screened, 12 354 were excluded because they were irrelevant to the purpose of the review, resulting in 1352 abstracts available for screening. Of the 1352 abstracts screened, 919 were excluded due to irrelevancy, yielding 433 studies available for eligibility screening. Of these, 359 studies were excluded for the following reasons: only assessed total PA (n = 184), no control group (n = 58), nonexperimental design (n = 30), nonspecific setting (n = 11), no PA assessment (n = 48), and other (n = 28). The remaining 74 studies were selected for the initial review. An additional 29 studies were identified through reference tracking, yielding 103 studies. Seventy-one of these studies were excluded as they failed to meet the inclusion criteria on further review: only assessed total day (n = 16), no control group (n = 6), nonspecific setting (n = 39), nonexperimental design (n = 2), and other (n = 8), resulting in 32 studies deemed eligible for final review. For further details on the study selection and ascertainment process, see Figure 1.
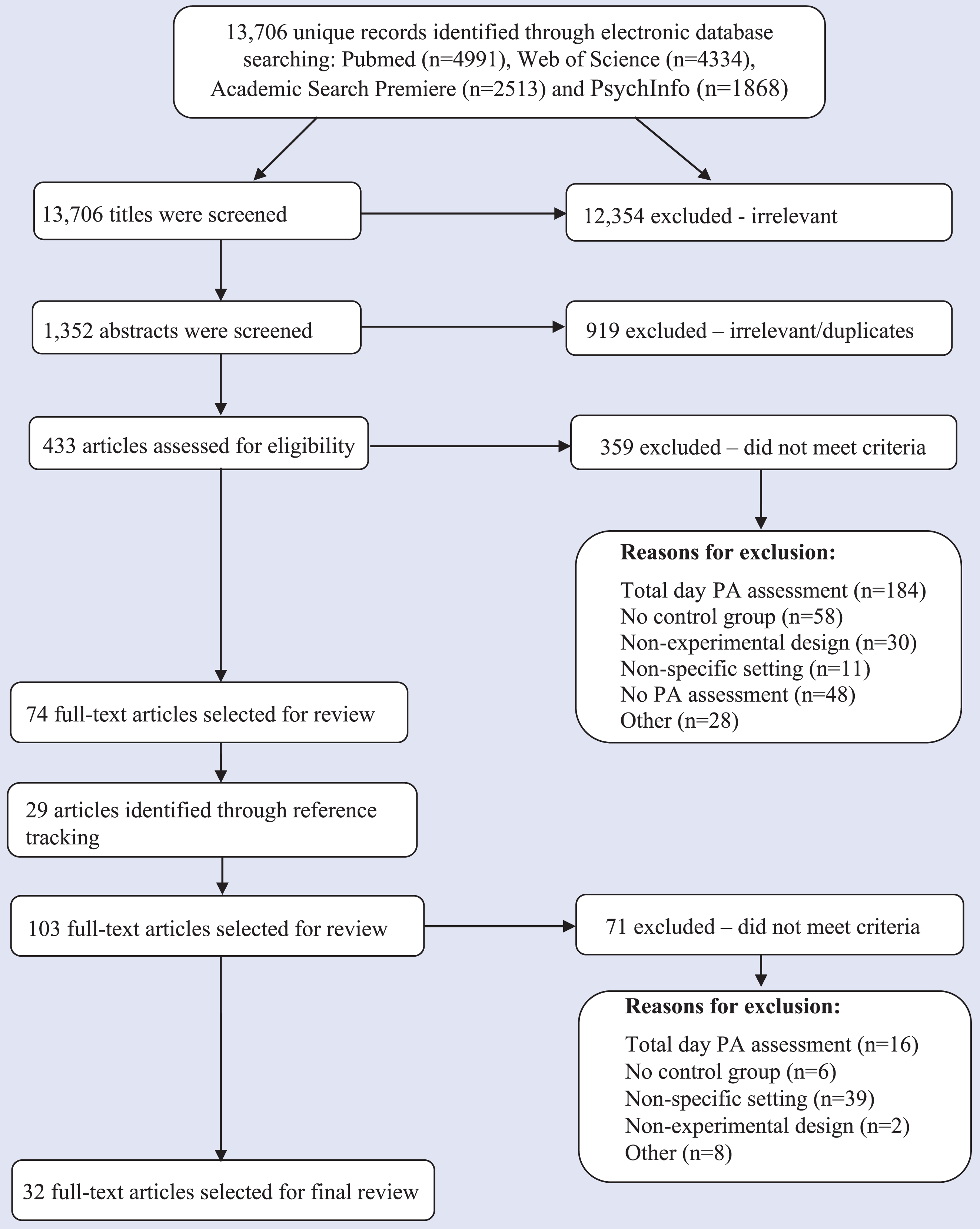
Study Selection and Ascertainment Process.
Overall Study Characteristics
Fifty-percent of the intervention studies employed an RCT study design (see Table 2). 15-17, 19-30, 32 Seventeen studies were conducted in the United States,* 12 in Europe (Amsterdam [n = 1], 24 Belgium [n = 2],16,30 Cypress [n = 1], 23 England [n = 6],26,38-42 and Scotland [n = 2]43,44), and 3 in Australia.15,45,46 A majority of the studies (97%) were implemented in samples consisting of boys and girls aged 5 to 13 years. One study was conducted in females only. 26 Fourteen studies reported the racial/ethnic composition of their sample (predominantly White [n = 7] † and mostly non-White [n = 7]).18,22,27,31-34 The intervention studies were published between 1993 and 2013.
Characteristics of Youth PA Interventions Among School Settings.

Abbreviations: ES, elementary school; MS, middle school; PS, primary school; ASP, after-school program; NH, non-Hispanic; AA, African American; AI, American Indian; NA, Native American; PI, Pacific Islander; INT, intervention condition; CON, control condition; PA, physical activity; MPA, moderate physical activity; MVPA, moderate-to-vigorous physical activity; VPA, vigorous physical activity; HR, heart rate; BMI, body mass index. “Finding” = the intervention effects were categorized as “positive,” “mixed,” or “null.”
Active Travel
Seven intervention studies aimed to increase PA in youth through active travel ‡ to and from school. RCTs were employed in 3 studies,15,17,32 and the remaining 4 used a quasi-experimental design.18,35,43,44 Sample sizes ranged from 60 to 1966. All studies were conducted in elementary school-aged children (5-11 years). The duration of the active travel interventions ranged from 1 month 17 to 2 years. 35 Interventions in 3 studies consisted of providing education materials (eg, packets, lessons) to children and/or parents regarding active travel to and from school.15,43,44 The remaining 4 interventions implemented the Walking School Bus Program, which provided transportation to specific “drop-off” locations where students walked on predetermined routes to and from school with supervised personnel.17,18,32,35 Three intervention studies utilized objective measures of PA (eg, accelerometers [n = 3]),17,32,43 and the remaining 4 used self-report measures.15,18,35,44 Four of the intervention studies reported significant increases in PA outcomes (ie, % active travelling to school, PA, moderate-to-vigorous PA [MVPA], distance walked to school).17,18,35,44 Two studies reported no statistically significant changes in PA,32,43 and 1 study reported mixed findings. 15
Results of the methodological assessment for each criterion can be found in Table 3. Briefly, 2 of the 3 RCTs provided sufficient information on randomization procedures.15,32 Seventy-one percent of all active travel studies used an appropriate control condition.15,17,18,32,44 A majority (57%) did not provide or insufficiently described attrition rates and/or methods for handling missing data.18,35,43,44 Only 14% of studies had a follow-up period (≥3 measurements and ≥6 months). More than half (57%) of the studies either failed to control for important confounding variables (eg, age, sex) or provided inadequate information on potential covariates.17,18,43,44 Two of the 3 RCT studies were considered high quality,15,32 and all 4 quasi-experimental studies were of low quality.18,35,43,44
Methodological Study Quality Assessment of Physical Activity Interventions by School Setting a .
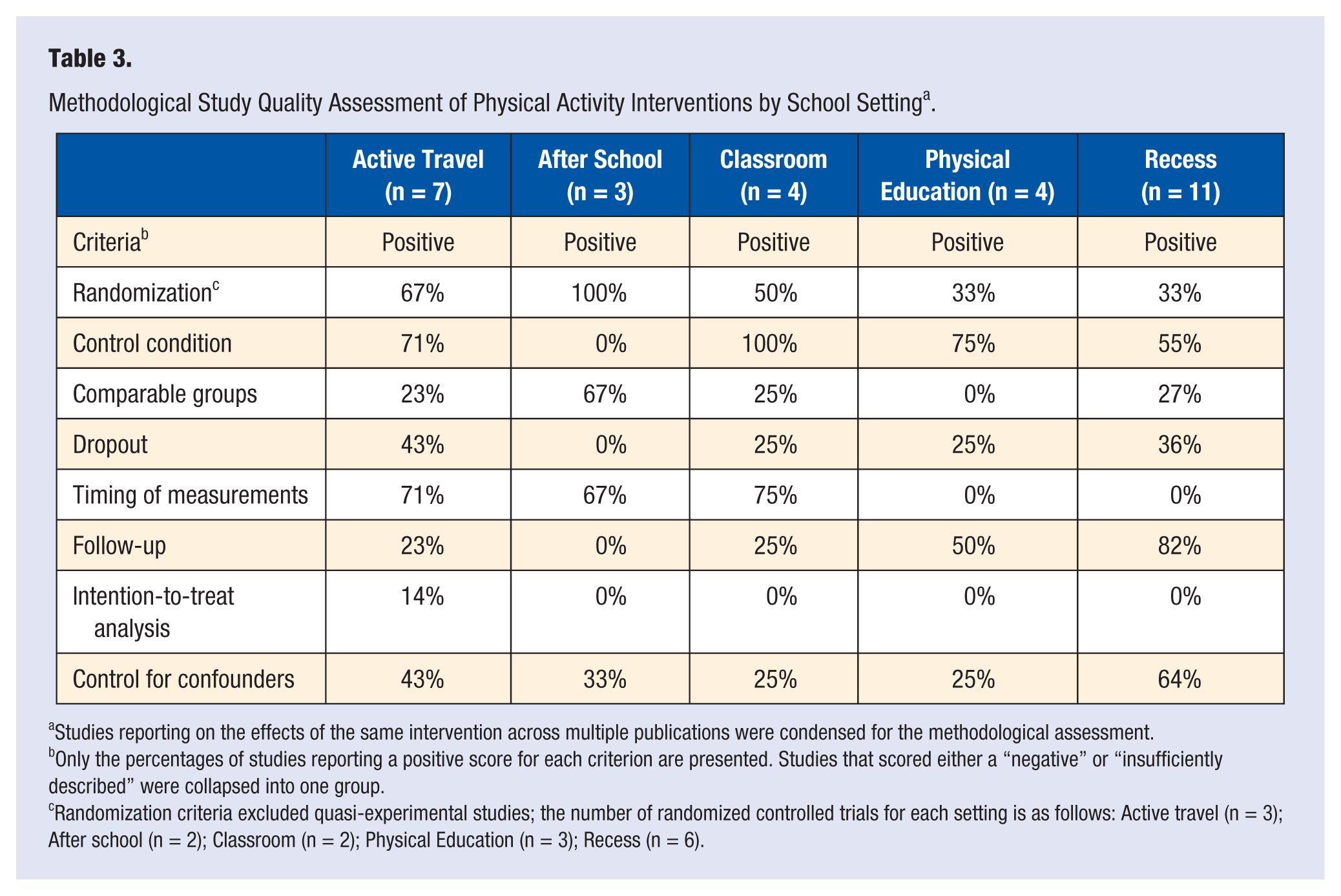
Studies reporting on the effects of the same intervention across multiple publications were condensed for the methodological assessment.
Only the percentages of studies reporting a positive score for each criterion are presented. Studies that scored either a “negative” or “insufficiently described” were collapsed into one group.
Randomization criteria excluded quasi-experimental studies; the number of randomized controlled trials for each setting is as follows: Active travel (n = 3); After school (n = 2); Classroom (n = 2); Physical Education (n = 3); Recess (n = 6).
After School
Three studies were conducted in the after-school setting,22,28,33 of which 2 employed an RCT design.22,28 Sample sizes varied from 156 to 273 participants aged 9 and 10 years. The duration of the interventions ranged from 6 months to 3 years. All 3 studies utilized a multicomponent approach to increase PA in this setting (eg, goal setting, skill training, education). Two of the intervention studies created objectives that included engaging youth in 30 minutes of PA,28,33 while the remaining study used the game of soccer as a means to increase PA. 22 All 3 studies used an objective method to measure PA (accelerometers [n = 2], SOFIT [n = 1]). One study reported statistically significant increases in the percent of time spent in MVPA, 33 and the other 2 studies reported mixed findings.22,28
Both studies employing an RCT design provided adequate information on randomization procedures.22,28 All 3 studies either did not describe or insufficiently described their control condition. Two of the 3 studies tested for baseline differences in participant characteristics between the experimental conditions.22,28 No studies provided information on attrition rates or had a follow-up period (≥3 observations and ≥6 months). Based on the methodological assessment, all studies received a low-quality rating.22,28,33
Classroom Breaks
Four studies implemented interventions designed to increase PA during classroom breaks.29,31,36,37 Two studies used an RCT design.29,31 All studies were conducted in elementary school-aged children. The duration of the classroom break interventions ranged from 4 months 31 to 3 years. 29 Sample sizes varied considerably, from 106 to 4599 children. All 3 intervention studies educated teachers on how to integrate PA breaks into their classrooms. PA goals varied greatly across the studies. One study only required teachers to implement a single 10-minute bout of PA each day 36 ; one study suggested implementing 10-minute bouts of PA throughout the day “as desired,” 31 while the remaining 2 studies trained the classroom teachers to provide at least 30 minutes of PA on at least 3 days of the week.29,37 All 4 studies used objective measures of PA (SOFIT [n = 3]29,31,37 and pedometers [n = 1] 36 ). Three studies reported statistically significant increases in PA,29,36,37 and 1 study reported null findings. 31
One of the 2 studies employing an RCT design sufficiently reported randomization procedures. 29 All 4 studies reported adequate information on their control condition. Only 25% of the studies tested for baseline differences in participant characteristics between the experimental conditions. 29 In addition, only 1 study provided information on attrition rates. 31 Three studies either did not control for important confounding variables or did not adequately describe the methods for handling potential covariates.31,36,37 Only 1 study received a high-quality rating, 29 while the remaining studies received a low-quality score.31,36,37
Physical Education (PE)
Five intervention studies were conducted in physical education classes.19-21,26,46 Four studies employed an RCT design.19-21,26 The interventions were implemented among youth aged 8 to 13 years, and sample sizes ranged from 1 school 26 to 24 schools. 19 The duration of the interventions ranged from 6 weeks 26 to 3 years. 20 One study consisted of a female-only sample. 26 Two studies assessed the short-term 21 and long-term effects 20 of the SPARK intervention, which focused on developing PE curricula designed to increase PA through fitness and sport skill development. One intervention study consisted of modifying current PE curricula to increase MVPA, 19 and one trained teachers to modify lesson objectives to increase PA (eg, equipment use, group organization, active learning). 26 Another study used a multicomponent approach to increase PA (eg, education, equipment, workshops). 46 All 5 studies used an objective measurement tool for PA (SOFIT [n = 5]). One study reported positive significant findings for increases in MVPA, 26 and the remaining 4 studies reported mixed results.19-21,46
Because 2 studies reported on the same intervention20,21 (ie, short-term and long-term effects), only one of these studies was used for the methodological assessment. 20 Only one study reported adequate information regarding its randomization procedures. 20 Twenty-five percent of the studies provided details on study attrition rates. 19 Half of the studies included a follow-up period,19,20 and 75% did not provide sufficient information or did not control for important covariates.19,20,26 None of the studies reported on or tested baseline differences in participant characteristics. All 4 studies received a low-quality rating.
Recess
Thirteen studies implemented interventions in the recess setting. * Six intervention studies employed a, RCT design.16,23-25,27,30 Three of the 13 studies assessed the effects of the same intervention over time (6 weeks, 6 months, and 12 months).40-42 Sample sizes ranged from 60 to 2310 children aged 5 to 11 years. The duration of the interventions ranged from 4 weeks 30 to 12 months. 42 Two interventions consisted of training teachers to maximize PA opportunities during recess (eg, organized games, behavior management) and provided recess equipment (eg, balls, Frisbees, hula hoops).25,34 Seven intervention studies restructured playgrounds with markings (eg, activity zones) and provided equipment. † Two studies only provided play equipment as the intervention.16,39 One study employed an intervention that educated children on the benefits of MVPA and taught children active recess games. 27 All intervention studies used one or more objective measures of PA (accelerometers [n = 10], ‡ heart rate monitors [n = 3],38,39 pedometers [n = 1], 45 SOPLAY [n = 2],24,25 and CAST 3 [n = 1] 45 ). Three studies reported positive significant findings for PA during recess.24,38,41 Five studies reported mixed results,16,23,25,27,34 and the remaining 5 studies found no significant intervention effects.30,39,40,42,45
Three of the 13 studies reported on short-term (ie, 6 weeks and 6 months) and long-term effects (ie, 12 months) on the same intervention; therefore, methodological quality was assessed once for the 3 studies, yielding 11 studies for the methodological quality assessment for recess interventions. Sixty-seven percent of the studies employing an RCT design provided either no or insufficient information regarding their randomization procedures.16,23,25,30 A majority (73%) of the studies either did not test or report baseline differences in participant characteristics. § Only 36% of intervention studies reported study attrition rates.16,30,34,39 Eighteen percent of the recess intervention studies included a follow-up period,24,42 and 64% of the studies reported controlling for important covariates.‖ One of the 6 RCT studies was considered to have high methodological quality. 24 In addition, 1 of the 5 quasi-experimental studies received a high-quality rating. 38 The remaining 9 studies received low-quality ratings.
Effectiveness of Physical Activity Interventions
Only 38% (n = 12) of all the intervention studies reported significant positive changes in PA levels. ¶ Active travel and classroom break interventions reported the greatest number of positive findings, 75% and 67%, respectively. Significant positive changes in PA were found in less than 40% of the interventions implemented in physical education classes (25%), after-school settings (33%), and recess (27%). Similarly, only 17% (n = 5) of all intervention studies were considered to have high methodological quality, and 80% of these employed a randomized controlled trial design. Additionally, intervention studies conducted in the active travel and classroom settings included the greatest number of high-quality studies (33%). Only 22% of studies implemented in the recess setting had high methodological quality, while no intervention studies conducted in the after-school or physical education settings received a high methodological quality rating. The level of evidence for the effectiveness of PA interventions on youth PA was deemed “inconclusive” for each of the intervention settings after accounting for the intervention effects, study design, methodological quality, and sample sizes of the intervention studies.
Discussion
The purpose of this review was to summarize and evaluate the impact of PA interventions that were implemented in specific school settings on children’s PA in those settings. The major findings of this review include the following: (a) interventions implemented in the classroom and active travel settings were consistently found to produce increases in youth PA, (b) less than 20% of studies were of high methodological quality, (c) less than half of PA interventions resulted in significant positive changes in PA, and (d) the level of evidence regarding the effectiveness of PA interventions on youth PA was deemed inconclusive for each specific setting.
One of the unique aspects of this review was determining whether interventions were successful at increasing PA in their targeted settings. Using this approach allowed for the discovery of 2 settings (ie, active travel and classroom) that may provide the best opportunity for PA interventions to succeed. The “successfulness” of the interventions in these settings may be, in part, attributable to the intervention approach used. For example, of the 4 intervention studies conducted in the active travel setting that reported positive effects, 3 used the Walking School Bus program. This program consisted of school buses dropping students off at designated locations and groups of students then walking on predetermined routes to and from school with supervised personnel. Some attributes of this program, which may have contributed to its positive impact on PA, are the use of existing resources (eg, school buses), limited training for volunteers, and ability of the intervention to be integrated into a child’s daily routine (ie, getting to and from school). Similar to the intervention approaches used in the active travel setting, the interventions implemented in the classrooms were of comparable intensity, which may also explain their positive findings. These interventions required teachers to integrate PA into the classroom lessons throughout the school day. While these studies required slightly more training, specifically for the teachers, only a few resources (eg, activity cards, active videos) and little equipment were necessary for implementation. Given the decreased burden (eg, few resources and training) of the interventions in these 2 settings, teachers, volunteers, parents, and children may have been more receptive and compliant, potentially explaining the positive influence on youth PA.
Contrary to recent reviews,47,48 the findings from this review identified physical education and recess settings to be less consistent in producing increases youth PA. And, consistent with the findings from Pate and O’Neill, 49 the effectiveness of PA interventions in the after-school setting were limited. These findings do not suggest that future interventions should not be implemented in these settings, as evidence indicates that schools are an efficient vehicle for intervention implementation,7,50 but rather that the intervention approaches used and methodological study quality should be improved. In contrast to the intervention approaches used in the active travel and classroom settings, the strategies used in after-school and physical education interventions, in general, were more burdensome. These interventions generally required more intensive training of teachers and staff members, curriculum modifications, professional development workshops, and so on. The increased burden of these interventions may have led to decreased teacher and staff compliance and a reduction in the intervention dose delivered, which may have resulted in a modest influence on youth PA. Similar to the active travel and classroom intervention studies, recess intervention approaches were fairly straightforward, as a majority of them consisted of playground renovation (eg, playground markings and play equipment). Despite the simple nature of these approaches, only 27% of recess interventions resulted in positive effects on youth PA. It is possible that only providing equipment and the opportunity for PA may be insufficient to influence PA. Previous studies suggest that other factors, such as adult participation and encouragement of PA, may be necessary. 51
An additional explanation for the increased reporting of positive findings among active travel and classroom intervention studies may be the dichotomous behaviors (active vs sedentary) to which the intervention and control groups are exposed. For example, in the active travel and classroom settings, participants in the intervention groups are exposed to the active behavior of walking to school or engaging in short bouts of activity while participants in the control groups continue to engage in sedentary activities such as riding on a school bus, travelling in a car to school, or sitting at a desk. As a result, because of the distinct differences in these behaviors, changes in PA may be more pronounced and easier to detect. Conversely, in settings where PA opportunities already exist (ie, recess, physical education, and after school), the differences in the behaviors to which each group (intervention vs control) are exposed may be considerably less. For example, in physical education settings, participants in the intervention may engage in a PE lesson aimed at enhancing the quality of PA offered via strategies such as curriculum modification or providing additional equipment, while the control subjects continue participating in their existing physical education curriculum. As a result, because both groups are engaging in an active behavior (ie, PE lesson), detecting substantial changes in PA may be more challenging. 52
Consistent with previous systematic reviews,14,53 a majority of PA interventions among youth had low methodological quality. In this review, only 20% of the intervention studies received a high-quality score. Specifically, interventions implemented in the active travel and classroom settings included the greatest proportion of high-quality studies, mostly RCTs, which may in part explain their increased effectiveness on youth PA. While all the interventions could have improved on at least one criterion on the methodological assessment, in this review, most studies failed to report study attrition rates, which is consistent with previous reviews. 53 Additionally, contrary to other reviews12,14 only one study performed an intention-to-treat analysis. Future studies should report study attrition rates, as they provide valuable information about the intervention, such as which population finds the intervention more attractive or useful (eg, younger, White, healthy) and the degree of burden imposed on participants. Likewise, future researchers should consider performing an intention-to-treat analysis, as this may provide important information about what dose of the intervention may be necessary to create positive effects (eg, number of PA sessions).
Given that nearly 80% of studies achieved a low methodological quality rating and only 38% reporting positive findings, it is not surprising that the level of evidence for the effectiveness of PA interventions on youth PA was deemed “inconclusive.” However, despite the fact that a majority of active travel (67%) and classroom (75%) interventions reported positive effects on PA and had a greater proportion of high-quality studies (33%), the level of evidence for these settings was “inconclusive.” In this case, considering the majority of the studies reported positive findings in these interventions, it seems that the large proportion of low-methodological quality studies may have been responsible for reducing the level of evidence for these settings.
There are strengths to the current systematic review, including the approach used to evaluate the effectiveness of PA interventions. In contrast to previous reviews,12,13,53 this review systematically assessed the influence of PA interventions on youth PA in their targeted settings. Using this approach allowed for a more direct evaluation of the intervention effects on youth PA compared to the effects on PA throughout the day, which may be influenced by factors outside of the intervention. Another strength of this review was the established 14 process for determining the level of evidence used which resulted in a more thorough evaluation of the effectiveness of PA interventions on youth PA.
As with any review, there are some limitations that warrant attention. First and foremost, the findings from this review on the effectiveness of interventions implemented in active travel, after school, classroom, physical education, and recess settings, are reflective of those intervention studies that measured PA in their specific setting. As a result, we cannot extend the conclusions drawn from this review on to intervention studies that solely assessed intervention effects on overall (or total day) PA. Second, it is possible that intervention studies may have been missed or excluded if the authors did not clearly state when PA was measured or in which setting the intervention was implemented. Third, the high level of heterogeneity of the measurements and expressions of PA (eg, minutes of MVPA, percent of time spent in PA, distance walked to school) precluded our ability to state the magnitude of the changes in PA found among the different settings. Fourth, in this review, the effects of an intervention were only considered “positive” if they were reflective of the entire sample, which may conflict with previous reviews. Using these criteria may have unfairly assessed the effectiveness of PA interventions, as it may be unlikely that a single intervention will elicit positive effects across all subgroups (eg, Black/White, male/female) of a particular sample. Nonetheless, it may also be argued while reaching all subgroups of a population is important, the implementation of several interventions to accomplish this may not be feasible.
The findings from this review suggest that interventions implemented in the active travel and classroom settings consistently resulted in positive influences on PA among youth, and future researchers should continue to develop interventions in these settings. Although the after-school, recess, and physical education settings were found to be less consistent in producing increased youth PA, more research in these areas is warranted. Collectively, for the school settings identified in this review, the level of evidence regarding the effectiveness of interventions on youth PA was deemed “inconclusive,” in addition to a large proportion of the intervention studies achieving low methodological quality. Because of this, it is strongly recommended that more large-scale, rigorously designed intervention studies are needed. Importantly, the results of this review highlight the necessity for researchers to evaluate the impact of their intervention in the targeted setting. By doing so, this allows intervention settings that result in positive influences of PA levels among youth to be identified and enable researchers to develop more robust interventions, especially those using a multicomponent approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.