
Abstract
The science and practice of step counting in children (typically aged 6-11 years) and adolescents (typically aged 12-19 years) has evolved rapidly over a relatively brief period with the commercial availability of research-grade pedometers and accelerometers. Recent reviews have summarized considerations for assessing physical activity using pedometers in young people (both children and adolescents), but 3 areas have received little attention: pedometer monitoring protocols, minimal (as opposed to optimal) step counts necessary for maintaining basal levels of health, and appropriate pedometer-based interventions for young people. Therefore, the objective of this review was to evaluate the current evidence and identify future research directions in these areas. The challenges of objective monitoring of physical activity in children and adolescents reinforce the importance of using protocols that minimize participant burden and the potential for tampering/reactivity. Evidence for a sedentary lifestyle cut point is limited; researchers are therefore encouraged to investigate several cut points (ie, <5000, <6000, <7000 steps/d) in children and adolescents to identify the health consequences of very low levels of ambulatory activity. Personalized messages may be necessary for health behavior change in pedometer-based interventions, but there is a need for more high-quality studies to develop the existing evidence base.
‘As technology evolves and proliferates, so does the potential for using pedometers in behavior change interventions. . . .’
The science and practice of step counting in children (typically aged 6-11 years) and adolescents (typically aged 12-19 years) has evolved rapidly over a relatively brief period with the ever increasing commercial availability of research-grade pedometers and accelerometers. Unlike accelerometers, which are more expensive and generally require specialized software to interpret data, pedometers provide a cost-effective and feasible approach for measuring ambulatory physical activity in young people (both children and adolescents). 1 In 1997, Rowlands et al 2 wrote a seminal article presenting the potential for using pedometry to study children’s free-living physical activity and subsequently followed up with the first publication of expected values for steps/d in 8- to 10-year-old children. 3
Today, a simple PubMed search (December 3, 2013) using the keywords children and pedomet* yields more than 300 articles. Among these include 2 methods-based studies,1,4 a systematic review of pedometer-based interventions in young people and a review article 6 compiling expected values for children’s and adolescents’ steps/d on weekdays vs weekend days, as well as steps accumulated during school, recess, physical education (PE) classes, and after school. An international effort has produced a researchers’ consensus statement addressing the question of “how many steps/d are enough?” in terms of children’s and adolescents’ health. 7 Steps/d are also now routinely collected as an outcome of interest in large accelerometer-based studies, 8 and recently the protocol of accelerometer-determined peak cadence (steps/min) indicators (a measure of the best daily effort) has been applied to children and adolescent data. 9
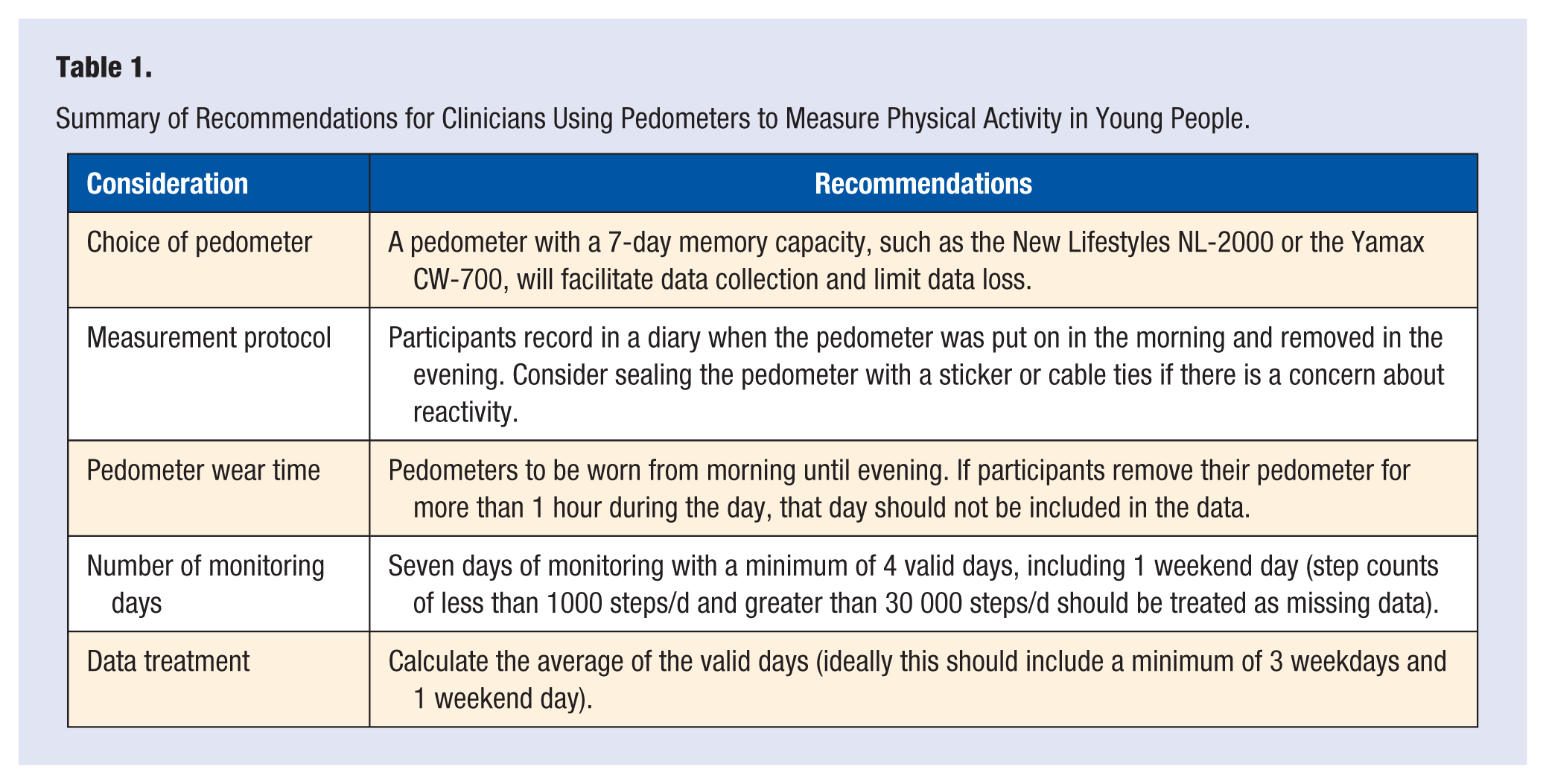
Recent reviews have summarized considerations for assessing physical activity using pedometers in children and adolescents.1-3 These reviews have provided recommendations regarding pedometer monitoring periods, wear time, data treatment, reporting, and choice of pedometer. It has been suggested that 7 days 4 or between 4 and 9 days 5 are needed to capture habitual activity in children and adolescents. However, compliance decreases with increases in the monitoring period; therefore, it is more feasible to opt for 4 full days with at least 1 weekend day. 1 An issue related to monitoring frame is pedometer wear time. In monitoring studies, participants are typically asked to record in a diary the time of morning when the pedometer was put on, along with any time during the day that it was removed. It has been recommended that monitoring studies exclude data from a particular day if a participant reports the removal of his or her pedometer for more than 1 hour on that day, 1 as has been done in previous studies.6,7 Finally, Yamax (Yamax, Tokyo, Japan) pedometers are the most widely used pedometers in large-scale surveillance studies, 1 but the New Lifestyles NL-2000 pedometer (New Lifestyles, Inc, Lees Summit, MO, USA) is also a popular choice8,9 because it has a 7-day memory capacity, making it practical for storing step counts in 1-day epochs. 1 Based on the existing literature, a summary of the recommendations for clinicians interested in measuring physical activity in young people using pedometers is provided in Table 1. A number of issues relating to pedometer use in young people have received little attention. First, systematic research comparing the quality of data obtained from different protocols is sparse.10,11 Specifically, few studies have explored the factors contributing to reactivity and tampering, especially in adolescent populations. Second, although Tudor-Locke and colleagues 12 have provided evidence for a sedentary lifestyle index for adults (ie, <5000 steps/d), researchers have failed to identify an equivalent value for children and adolescents. Physical inactivity has serious health consequences for young people,13,14 but is there a minimum number of steps necessary to prevent ill health in young people (both children and adolescents)? Finally, pedometers and step-counting devices have been used extensively in interventions to promote physical activity in adults,15,16 but less is known regarding the utility of pedometers for increasing physical activity in young people. As technology evolves and proliferates, so does the potential for using pedometers in behavior change interventions, raising the question, “How can pedometer-based interventions be implemented to optimally increase young people’s physical activity?”
Summary of Recommendations for Clinicians Using Pedometers to Measure Physical Activity in Young People.
Therefore, the aims of this narrative review are 3-fold: (1) to discuss pedometer monitoring protocols for young people and explore issues of reactivity and tampering; (2) to evaluate the evidence for establishing a step-defined sedentary lifestyle index, perhaps separately for children and adolescents; and (3) to present pedometer-based interventions undertaken to date for young people and identify research directions focused on optimizing their positive effects on physical activity in children and adolescents.
Pedometer Monitoring Protocols
Although there has been a proliferation of studies using pedometers to measure physical activity in children and adolescents,1,4,10,17 little research has focused on comparing different monitoring protocols (in terms of maximizing best quality data) and young people’s reactions to the assessment process. Reactivity (ie, a change in normal activity pattern as a result of being monitored) is considered an inherent threat to the accuracy of pedometer data collection. 18 Although some studies have revealed little evidence of reactivity in children and adolescents,17,19-21 others have shown reactivity is present in young people.18,22 Sealing pedometers (eg, using cable ties or adhesive stickers/tape) limits access to feedback and the potential for peer competitiveness.22,23 Monitoring for extended periods of time may also diminish reactive behavior attributed to device novelty,18,19,24 but the increased burden on participants may lead to lower levels of compliance. Daily unsealing/sealing of pedometers by study staff recording data in schools can be an administrative burden for teachers in large-scale studies. 17 Pedometers that have on-board memory functions and thus the ability to record for multiple days are useful for addressing this logistical inconvenience, reducing the effect of visual feedback to the wearer, and eliminating any need for participants to record their own data. Such pedometers may also address the challenges of collecting step counts on weekend days when children are not as easily trackable as when they are gathered together on school days.11,25
Pedometer tampering (“shaking” or “rattling” the pedometer to increase step count) may result in further inaccuracies in pedometer data collection,17,22,26,27 but there is little systematic research to illuminate the magnitude of this potential threat to validity. Almost half of 123 adolescents reported tampering with their pedometer in a recent study. 18 Similarly, 69% of 43 children admitted to shaking the device in another study. 22 Frequency of reported tampering alone does not quantify the potential magnitude of the threat. A few shaken steps produced as a result of a curious child’s interest in a pedometer’s mechanism may be a trivial issue relative to a day’s worth of actual ambulatory steps. Characteristics of individuals given to tampering/reactivity are unknown. At odds with concerns for reactivity of measurement (which would theoretically produce inflated estimates) is the more pressing concern that children and adolescents actually accumulate fewer steps/d than expected, considering their age. Nevertheless, further study of pedometer tampering in child and adolescent populations is needed, as well as strategies to understand, quantify, and ultimately reduce/eliminate or tolerate/accommodate such behaviors to improve interpretation of pedometer monitoring studies.
Pedometers provide a feasible (eg, practical, cost-effective) way to collect objective physical activity data from large groups, but strategies to overcome potential reactivity and tampering, or at least interpret data cognizant of this possibility, require consideration. Further testing of pedometer monitoring protocols and innovative experiments, such as covert monitoring (when participants are unaware that their activity levels are being monitored), 4 may be necessary to identify the optimal measurement protocols for assessing physical activity in young people.
A Step-Defined Sedentary Lifestyle Index for Children and Adolescents
Lower levels of self-reported and accelerometer-determined physical activity have been associated with increased risk of detrimental health outcomes in children and adolescents, including higher cholesterol and blood lipid profiles, 28 higher blood pressure, 29 increased incidence of metabolic syndrome,28,30 and increased incidence of obesity.31,32 Of the direct associations between low step/d and health outcomes in children and adolescents, less desirable body composition33-35 and lower fitness levels3,36,37 have been reported. In addition, Barreira and colleagues 9 recently demonstrated that children and adolescents with higher peak cadence (ie, steps/min) had fewer cardiovascular disease risk factors. Despite this emerging evidence, the question of “How many steps/d are too few for young people?” has not been answered.
Recently, Tudor-Locke et al 12 proposed a step-defined sedentary index of <5000 steps/d in adults, which includes consideration of population distribution, sociodemographic characteristics, contextual factors, health risks associated with taking <5000 steps/d, and the health effects associated with increasing steps/d above 5000. Low step counts may indicate that an individual has spent more time engaged in sedentary behavior (ie, described as activities that involve minimal energy expenditure [1-1.5 metabolic equivalent multiples of rest], typically performed while sitting or lying down). 38 Tudor-Locke and colleagues 12 have argued that estimating time spent in sedentary behavior from lack of steps is consistent with the approach of using low accelerometer counts (eg, <100 counts/min). 39 Using data from cross-sectional 39 and experimental studies, 40 Tudor-Locke et al 12 provide evidence to support the use of low step counts to indicate a sedentary lifestyle (ie, one characterized by more sedentary behavior and less ambulatory behavior) in adults.
As yet, there is limited evidence to support the creation of a sedentary lifestyle index for children and adolescents. Population distribution data among Canadian young people 41 indicate the lowest 15th percentile performing <8448 and <7761 step/d in boys and girls, respectively (aged 5-13 years). Using the 15th percentile cut point in US data 8 highlights the population-specific nature of distribution data, with <6040 and <4855 steps/d in boys and girls, respectively. While this normative information is valuable, it does not provide evidence of the health-related consequences of low step counts for children and adolescents.
To date, body mass index (BMI)–referenced cut points for normal-weight and overweight/obese children have been used as a health-related index for steps/d. Using children’s step count data from the United States, Australia, and Sweden, Tudor-Locke et al 35 identified step counts of 12 000 for girls and 15 000 for boys as criterion-referenced cut points. These analyses get at “how many steps/d are enough?” and, interpreted dichotomously (yes/no), suggest that those not achieving these cut points are not achieving “enough.” A proposed graduated index 42 based loosely on these BMI-determined cut points (the posited values serve as anchors) includes multiple levels, including a sedentary lifestyle index for boys and girls of <7000 steps/d. Using a recent suggestion of a non–sex-specific step-defined sedentary index for young people of <7000 steps/d, 12 approximately one-fourth of Canadian boys and one-third of girls accumulated <7000 steps/d (aged 5-19 years). 43
Importantly, the question of “How many steps/d are enough?” is not the same as “How many steps/d are too few?” The former focuses on an optimal level and the latter on a minimal level to be interpreted as a “red flag” for intervention purposes. To clarify further, a sedentary lifestyle index for young people may enable the identification of individuals at the greatest risk of serious health consequences due to low ambulatory lifestyle behaviors. While the existing evidence base is limited, researchers are encouraged to investigate several cut points (ie, <5000, <6000, and <7000 steps/d) to identify the health consequences of falling below these thresholds in longitudinal studies for children and adolescents.
Using Pedometers to Increase Physical Activity in Young People
Behavioral interventions incorporating pedometers have been used to increase physical activity in child, adolescent, and adult populations.5,15,44 The principle underlying the use of pedometers to increase physical activity is that the “real-time” step count feedback increases an individual’s awareness of how personal behavioral choices influence his or her physical activity. 5 Pedometer-based programs provide individuals with up-to-the-minute information and encourage them to self-monitor and set step goals using tailored (ie, based on specified baseline values), standardized (eg, percentage-based increments), or predetermined (eg, an increase of 2000 steps/d each month) step targets.5,45-48 A range of new and innovative ways to use pedometers and deliver pedometer-based interventions is emerging in the literature.
A previous systematic review of pedometer-based interventions targeting children and adolescents identified 3 major pedometer-based strategies for increasing physical activity 5 : (1) self-monitoring and goal-setting interventions based on personalized or standardized step targets,45-49 (2) open-loop feedback interventions that involve making access to desirable sedentary activities such as television watching contingent on achieving step targets,50,51 and (3) physical activity integration interventions that involve using pedometers as educational tools to increase physical activity throughout the school day. 52 All 3 strategies were found to contribute to increased physical activity, but due to the small number of studies, the high risk of bias and lack of long-term follow-up in published studies at that time, the authors of the review were unable to provide optimal guidelines for pedometer-based interventions for young people. 5
One of the limitations identified in the review was the lack of theory in guiding the development of pedometer-based interventions for young people. In adults, theory-based interventions appear to be more effective in changing behavior than atheoretical approaches53,54 and are hypothesized to affect relevant cognitions, which in turn influence behavior. 55 Despite evidence for the importance of theory, few pedometer-based interventions for young people have aligned their behavior change strategies with a health behavior theory. Notable exceptions were the Learning to Enjoy Activity with Friends46,56 and Program X45,57 interventions, which were guided by social cognitive theory (SCT) and designed to target hypothesized mediators of behavior change (eg, self-efficacy, outcome expectations, and social support). 56 While Zizzi and colleagues 58 did not explicitly cite their theoretical framework, their intervention appeared to be guided by SCT, and they measured potential mediators from SCT. However, none of the 3 interventions45,46,58 found evidence for the mediating effect of any measured SCT variables on changes in steps/d. The failure to identify the mechanisms of behavior change is likely due to the poor measurement of theoretical mediators. Recent reviews examining the effects of physical activity interventions on mediating variables have noted the lack of significant findings and the challenges of accurately measuring constructs in young people.59-61
Pedometer-based interventions designed to increase obese adolescents’ steps/d have involved cognitive-behavioral therapy 62 and coping skills training, 63 also based on SCT. Similar to other pedometer-based interventions targeting healthy-weight adolescents, participants in these studies62,63 were provided with pedometers and log books and encouraged to self-monitor their step counts. Participants were also encouraged to identify barriers to physical activity and formulate strategies to increase their steps and maintain positive health behavior change. These studies, however, did not provide detailed descriptions of the self-monitoring procedures, and therefore it is difficult to evaluate the strategies and recommendations. Goldfield and colleagues 65 employed an alternate approach to promote physical activity in obese children and demonstrated that making access to desirable sedentary activities (eg, TV watching) contingent on physical activity can increase step counts.50,65 While this approach appears to have some utility, there is concern that treating sedentary activities as rewards may undermine children’s autonomous motivation 64 for physical activity and project an unhealthy message about the perceived value of sedentary behaviors.
One possible explanation for the failure of existing health behavior models to adequately explain physical activity behavior change in pedometer-based interventions for young people is that such models were originally designed for “at-risk” adult populations. Motivation for physical activity changes over the life span, 66 and while adults may engage in physical activity to reduce their risk of lifestyle diseases, such outcomes are unlikely to be important to young people. Furthermore, theoretical models that fail to address the social, cognitive, and biological changes that occur during the transition from childhood to adolescence 67 are unlikely to provide a better foundation for behavior change. 68 The importance of integrating health behavior theories68,69 and adopting socioecological models 70 has been noted in the literature, yet such frameworks have not been adopted in pedometer-based interventions for children and adolescents. Health behavior models such as the youth physical activity promotion model 71 and competence motivation theory 72 may have utility for guiding pedometer-based interventions for young people, but they are yet to be tested in experimental studies.
Technological advancements, particularly the proliferation of social media, exergaming, and smartphone technologies, have provided researchers and health professionals with exciting opportunities to combine pedometers with eHealth technology (eg, Internet and smartphone applications) to promote physical activity in young people. Such approaches are appealing as public health initiatives due to their potential for cost-effectiveness and their considerable reach. 73 Young people’s access to technology is increasing at a rapid rate, and in developing nations, there appears to be little evidence of a “digital divide.” For example, smartphone ownership among young people has accelerated rapidly in recent years 74 and does not appear to be moderated by socioeconomic status, 75 creating an ideal opportunity for equitable health promotion. Although smartphones have in-built accelerometers with step-counting features and global positioning systems, their size and design may prevent them from being worn during certain types of physical activity (eg, games and sports). Furthermore, the validity and reliability of such features are only starting to emerge in the literature, 76 and due to the broad range of technologies and brands available, it will be difficult to standardize results across studies.
One of the first studies to incorporate eHealth technology into a pedometer-based intervention for adolescents was Program X.45,57 Participants in the Program X intervention attended interactive seminars on goal setting and self-monitoring and were provided with pedometers and sent personalized email messages encouraging them to achieve their step count goals derived from baseline step counts. 45 The intervention resulted in a significant increase in step counts for boys (~1000 steps/d) and girls (~2000 steps/d), but the strategy for generating personalized feedback was labor intensive for the research team and not feasible for large population groups. In contrast, the Nutrition and Enjoyable Activity for Teen Girls (NEAT Girls) intervention77-79 used bulk short-message service (SMS) text messaging to reinforce health behavior change. Participants in the NEAT Girls intervention were provided with pedometers and sent weekly generic SMS messages during the intervention period. However, there was no intervention effect on accelerometer-determined physical activity at the 12-month posttest. 78 Bulk SMS messaging was considered to have good reach, as messages were sent to 91% of girls, but the SMS messages were not rated highly by all participants, some of whom described the messaging as “intrusive.”
It appears that pedometer-based interventions incorporating eHealth technologies may require a tailored component to engage adolescents. The multicomponent Active Teen Leaders Avoiding Screen-time (ATLAS) program included a purposely built smartphone application (app) to promote physical activity and reduce sedentary behavior in adolescent boys. 80 A unique aspect of the ATLAS app was that it included tailored physical activity messages, based on information reported by participants, and once the app was downloaded, participants received biweekly messages sent via “push notifications” through the app. Although research findings are yet to be published, feasibility data suggest that the app was rated highly by participants and may have utility for physical activity promotion in young people. Similarly, Thompson and colleagues 81 recently evaluated a 12-week pedometer-based intervention guided by self-determination theory (SDT) for adolescents. Participants were not given a daily step goal; rather, consistent with SDT, they were told daily step goals that experts recommend for teenagers, 35 along with their personal average step counts (extracted from 7 days of accelerometry at baseline). Preliminary evidence suggests that modest increases in moderate-to-vigorous physical activity (MVPA) occurred in the expected directions.
Although the number and quality of pedometer-based interventions designed to increase physical activity in young people are increasing at a rapid rate, there are barriers to their successful implementation, evaluation, and interpretation. First, little evidence suggests that behavioral changes resulting from pedometer-based interventions are sustainable. It is possible that participants become fatigued with wearing their pedometers and regress to their preintervention physical activity levels. Most studies have been evaluated over short periods (ie, <6 months), and longer term studies are clearly needed. Second, pedometer-based interventions incorporating eHealth technologies must manage the congestion and competition from other commercial and social medial efforts competing for space using the same media. This may contribute to information overload, thus reducing the efficacy of such approaches for behavior change in young people. Finally, as new measurement devices emerge (eg, Fitbit and Jawbone monitors) that can synchronize with a user’s smartphone and provide instant feedback regarding step counts, estimated energy expenditure, and time spent in physical activity of various intensities, the basic pedometer may become obsolete. However, it is unlikely that pedometers will disappear any time soon. Pedometer-based interventions remain a feasible and effective strategy for increasing physical activity in people of all ages, in part due to their accessibility (ie, pedometers can be cost-effectively distributed to a large group) and easy-to-interpret feedback. There is clearly a need for research comparing the effects and cost-effectiveness of more simplistic pedometer-based interventions with those using new measurement devices (eg, Fitbit and Jawbone monitors), both supported by similar eHealth methods.
Using Pedometers in Schools to Promote Physical Activity in Young People
Schools provide an ideal setting for physical activity promotion among children and adolescents since they have access to most of the population and have the necessary facilities, equipment, and personnel to achieve this outcome. 82 Physical education (PE), school sport, physical activity integration into key learning areas (e.g., mathematics and science), active transportation, after school, and break times represent opportunities for physical activity promotion in and around the school setting. Using pedometers to promote and monitor activity levels in primary and secondary schools is appealing because these devices offer an affordable and accessible technology that provides output in a simplistic format that is easy to understand (ie, steps/d). 16
Physical education is commonly recognized as the major vehicle for the physical activity promotion in young people, and lessons that involve high levels of MVPA can make an important contribution to young people’s overall physical activity levels and their health.83,84 Existing US guidelines suggest that students should be engaged in MVPA for 50% of PE lesson time. 85 Scruggs 86 has demonstrated that pedometer steps/min intervals of 82 to 88 for the Yamax SW651 and SW701 (Yamax, Tokyo, Japan) pedometers and 76 to 80 for the Walk4Life W4L LS2505 and DUO (Walk4Life, Plainfield, Illinois, USA) pedometers 87 are equivalent to the 50% MVPA recommendation for PE in middle schools. These step rates can be used by teachers to evaluate their PE lessons by asking students to wear pedometers during class and then dividing students’ total step counts for the lesson by the duration of the lesson.88,89 Commercial pedometers also are available that can track time above selected steps/min cut points, automating this practice if desired.
Integrating movement into key learning areas, such as mathematics, geography, and science, represents another opportunity for physical activity promotion in the school setting. In one of the earliest studies of its kind, Oliver and colleagues 52 evaluated the feasibility of implementing an intervention that used pedometry to integrate physical activity (subjects included English, social studies, mathematics, statistics, and PE) throughout an elementary school curriculum. Although the overall intervention effect was not statistically significant, increases of approximately 2000 steps/d were observed among children with initially low activity levels. More recently, Riley and colleagues 90 evaluated the Encouraging Activity to Stimulate Young Minds (EASY Minds) physical activity integration program for elementary school students. Similar to the Take 10! program and other physical activity integration interventions that require teachers to provide bouts of MVPA related to curriculum outcomes,91,92 EASY Minds aimed to improve student activity levels, engagement, and attainment in numeracy through the use of cross-curricula teaching strategies. For example, pedometers were used as learning tools to reinforce key concepts regarding measurement, distance, and speed. Preliminary findings suggest that the EASY Minds intervention significantly improved students’ MVPA and reduced their sedentary time measured using accelerometers during the school day. The findings from these studies highlight the potential of pedometers for promoting physical activity within the school day by using their user-friendly and quickly accessible output for a range of learning outcomes across key learning areas.
Recess and lunch breaks, as well a time before and after school while children aggregate on campus, represent important school-based opportunities for young people to be physically active.93,94 However, the potential contribution of these key time segments is dependent on the availability of school facilities and existing policies that support or inhibit student activity levels.88,95-97 For example, schools might have high-quality indoor gymnasiums and well-manicured fields but only allow students access to facilities during scheduled PE lessons. Interestingly, a review of studies designed to evaluate the impact of school-based policies and built environment changes on energy expenditure found that mandatory PE, classroom activity breaks, and active commuting to and from school produced the largest effects. 95 Pedometers provide a feasible means for assessing such physical activity policy initiatives in schools, 98 and their immediately available and interpretable feedback makes them appealing to researchers and teachers.
Conclusions and Future Research
Pedometers are now used regularly in population surveillance studies to determine youth activity levels and in health behavior interventions to promote physical activity. This review focused on 3 areas related to pedometer monitoring in young people, which have received limited attention in the research literature: pedometer monitoring protocols, minimal step counts necessary for maintaining basal levels of health, and appropriate pedometer-based interventions for young people. The challenges of objective monitoring of physical activity in children and adolescents reinforce the importance of using pedometer protocols that minimize participant burden and the potential for tampering and reactivity. There is little evidence for a sedentary lifestyle cut point in young people, and the health consequences of very low ambulatory activity have not been established. Personalized messages and feedback may be necessary for health behavior change in pedometer-based interventions for children and adolescents, but few long-term studies have been conducted. As a final note, we offer the following suggestions for future research:
There is a need to further explore the utility of different pedometer measurement protocols and identify optimal strategies for improving compliance in population monitoring studies, particularly in adolescent populations. While pedometers remain a valid and reliable method for establishing physical activity levels in youth, researchers should avoid using the same instrument to both measure and motivate physical activity in the same study sample.
Further study of the physiological and psychological health-related outcomes of excessively low ambulatory behaviors is required to develop a step-defined sedentary lifestyle index for young people. Researchers are encouraged to investigate several cut-points (ie, <5000, <6000, and <7000 steps/d) in child and adolescent populations to identify the health consequences of falling below this threshold.
Further research is warranted to identify the ideal theory or combination of theories to guide pedometer-based physical activity interventions for children and adolescents. Additional questions remain unanswered that were not explicitly covered here in detail: what combination of procedures and components is most effective in the promotion of physical activity in pedometer-based studies with young people? What are the long-term effects of pedometer-based interventions? Can pedometer-based interventions be regularly repeated in the same population? What is the ideal program length for a pedometer-based intervention, and is it necessary to include “booster” sessions or other forms of contact once the intervention period has ended to maintain step counts? Are tailored interventions (ie, those including personalized feedback on performance) more effective at increasing physical activity in young people and, if yes, what are the ideal characteristics on which to tailor pedometer-based interventions? How can pedometers be integrated into the school environment to induce sustainable behavior change?
Footnotes
Acknowledgements
Ronald Plotnikoff is supported by a National Health and Medical Research Council (NHMRC) Senior Research Fellowship.