
Abstract
Lifestyle medicine interventions are typically intensive by design. This study explored the optimal “dosage” of a well-known lifestyle medicine intervention—the Complete Health Improvement Program (CHIP). A total of 2383 individuals (mean age = 61.0 ± 9.2 years; 34% males) participated in either an 8-session (N = 448) or 16-session (N = 1935) version of the CHIP intervention conducted over 4 weeks in community settings throughout North America. Both the 8- and 16-session groups experienced significant improvements in all the chronic disease risk factors measured. There was no difference between the changes experienced by the 8- and 16-session groups in lipid profile, fasting plasma glucose, or systolic blood pressure. The 8-session group experienced a significantly greater reduction in body mass (0.3 percentage points or 0.8 lbs, P < .01), but the 16-session group recorded a significantly greater reduction in diastolic blood pressure (2.8 percentage points or 2.2 mm Hg, P < .01). There was no clear difference between the outcomes achieved in 4 weeks by the 8- and 16-session versions of the CHIP lifestyle medicine intervention. This study suggests that the short-term outcomes achieved by a 16-session CHIP intervention can be achieved in half the number of sessions, which has implications from a resourcing and cost-effectiveness perspective.
‘Lifestyle medicine interventions are typically intense with regard to the number of sessions individuals participate in, especially in the first 3 to 4 weeks of the program.’
Chronic diseases are responsible for 7 out of 10 deaths in the United States and account for approximately 75% of national health care expenditure. 1 Indeed, there is a desperate need for effective countermeasures to address this pandemic of chronic disease. 2
It is well established that chronic diseases are lifestyle related,3,4 with over 80% of myocardial infarctions, over 90% of type 2 diabetes mellitus, and approximately one third of cancers preventable through healthy lifestyle choices. 4 More encouragingly, an accumulating body of evidence demonstrates that chronic diseases are responsive to therapeutic lifestyle intervention,5 -8 also referred to as “lifestyle medicine” interventions.
Lifestyle medicine interventions are typically intense with regard to the number of sessions individuals participate in, especially in the first 3 to 4 weeks of the program. For example, the Ornish Program, 9 which has demonstrated atherosclerotic plaque regression in a randomized-controlled trial, 6 involves three 4-hour sessions in the first week and two 4-hour sessions for the next 8 weeks. The pioneering residential lifestyle medicine intervention at the Pritikin Longevity Center, 10 the outcomes of which have been published in over 100 scholarly publications, 11 involves a 3-week live-in experience with daily sessions. The community-based Complete Health Improvement Program (CHIP), 12 now used in numerous countries, has historically involved 16 group sessions within the first 4 weeks.
These lifestyle medicine interventions are strategically designed to be intense in the initial stages to facilitate rapid results and subsequently increase participant’s self-efficacy and motivation for behavior change. 12 However, the intense nature of the programs can require high levels of resourcing and associated costs. For lifestyle medicine interventions to be optimally designed to balance efficacy and cost-effectiveness, a greater understanding of the “dose response” is required. To date, little attention has been given to defining the optimal dosage of lifestyle interventions with most programs arbitrarily selecting the number, duration, and density of sessions in the program. A more structured and systematic study of the responsiveness to programs of various intensities is therefore needed.
The present study examined the short-term effects on participant outcomes of halving the number of sessions of the CHIP lifestyle medicine intervention. The CHIP intervention was selected for this study as it has been identified by the American College of Lifestyle Medicine as achieving some of the most clinically significant short-term reductions in chronic disease risk factors in the literature. 12 Historically, the intervention has involved 16 group sessions over a 4-week period. The present study compared the short-term (4-week) outcomes of the traditional 16-session program to a modified 8-session version.
Methods
The study compared the changes in selected chronic disease risk factors of participants in 2 variants of the CHIP lifestyle intervention conducted over 4 weeks: a standard 16-session version and a modified 8-session version. The study was approved by the Avondale College Human Research Ethics Committee (No. 20:10:07).
Subjects
A total of 2383 self-selected subjects participated in the study (mean age = 61.0 ± 9.2 years; 809 males/1574 females). The 16-session group involved data collected from 1935 individuals who participated in 1 of 101 CHIP interventions conducted throughout North America (mean group size = 19.4 ± 17.5). The 8-session group consisted of 448 individuals who participated in 1 of 21 interventions (mean group size = 21.8 ± 8.4), called “Healthy Beginnings,” conducted in 6 communities in Indiana.
Description of the Interventions
The CHIP lifestyle intervention has been described in detail previously in this journal. 12 CHIP is a primarily nutrition-centered program that encourages participants to move toward a whole-food, plant-based eating pattern. In the first 5 days of the program, participants are encouraged to consume only fruits, vegetables, whole grains, legumes, and water as a Jump Start experience. Participants are also encouraged to be physically active, with the goal being to achieve 10 000 steps per day, and attention is given to stress management and increasing emotional well-being. Each session is approximately 1.5 hours in duration, with approximately half this time consisting of group discussion and activities and the other half viewing a prerecorded expert lecture.
The program is informed by the theory of planned behaviour 13 and aims to change participants attitudes toward healthful living through education, achieved by viewing the expert lectures in each session; foster supportive social norms through group activities; and build perceived control by providing participants with a measureable experience of improving their health status through biometric assessments conducted at the beginning and end of the program.
The core themes, messages, and calls to action in the 8-session “Healthy Beginnings” intervention were identical to the CHIP intervention described above. However, while the sessions in the 8- and 16-session interventions were of similar duration, the 8-session version utilized shorter video presentations and more group activities. There were other variant features of the 2 interventions, but these variations also existed within the 2 cohorts. Variant features included the geographical location of the programs and the experience of the facilitators who delivered them. All facilitators were volunteers certified by the Lifestyle Medicine Institute (who administers the interventions); however, the professional background of the facilitators varied widely. In addition, some programs served the participants food samples or full meals during the sessions.
Measurements
At program entry and after 4 weeks, the participants’ body mass and blood pressure (BP) were measured. In addition, blood samples were collected by trained phlebotomists and analyzed at local pathology laboratories for total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides (TG), and fasting plasma glucose (FPG).
Statistical Analysis
The data were analyzed using IBM SPSS Statistics (version 22) and are expressed as means ± standard deviations. The data were initially cleaned and outliers removed. Chi-square was used to assess differences in the gender balance of the groups. Independent samples t tests were used to assess differences between the groups in age and baseline biometrics (Table 1).
Baseline Measures for the 8-Session and 16-Session Groups.
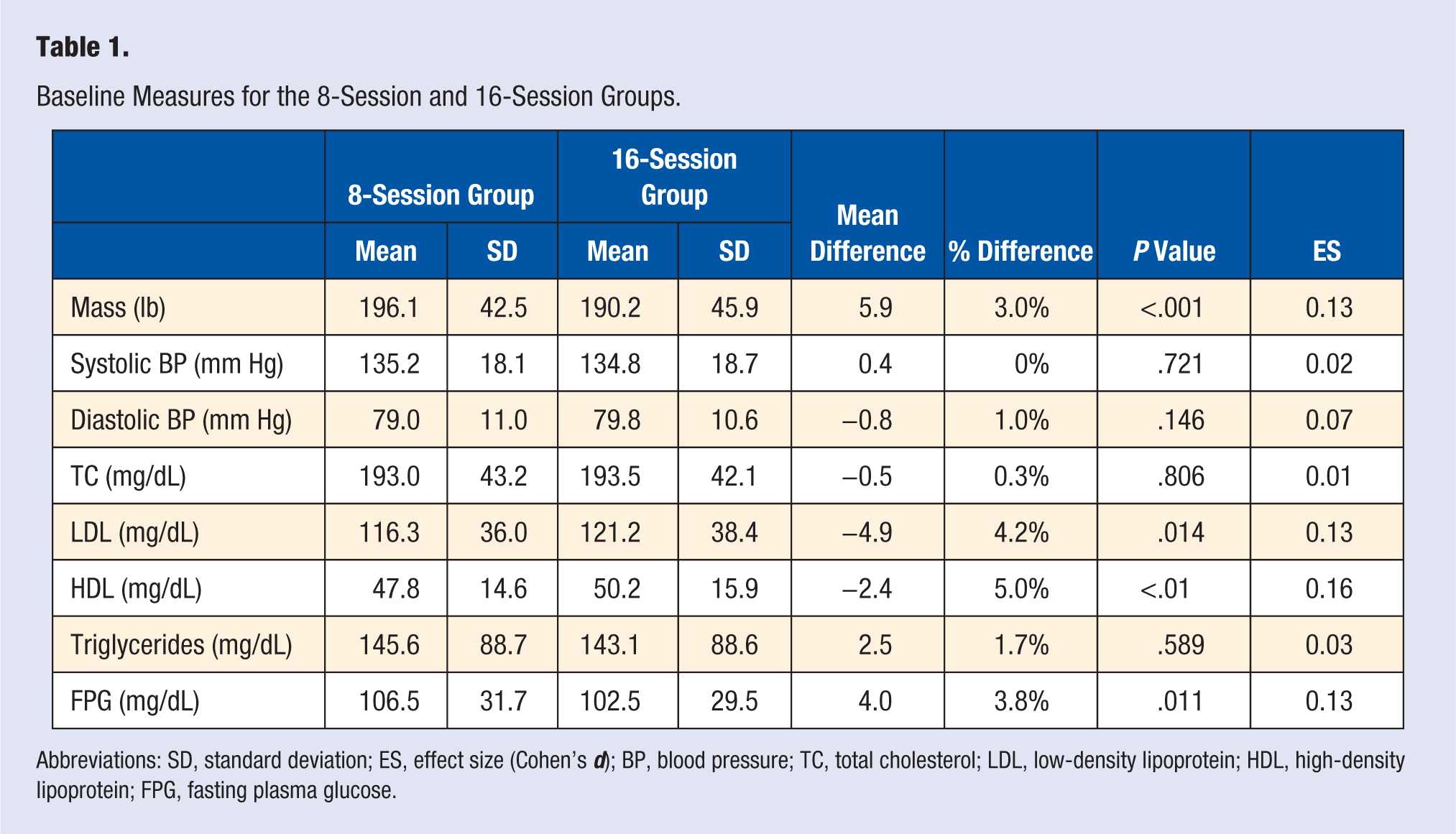
Abbreviations: SD, standard deviation; ES, effect size (Cohen’s d); BP, blood pressure; TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; FPG, fasting plasma glucose.
The primary interest of the study was the effect of group (8 vs 16 sessions) on the pre to post changes in the biometrics. Initially, independent samples t tests were used to assess differences between the groups in the biometric changes with Cohen’s d calculated to express effect size (Table 2). As age, gender, and baseline biometric level can influence changes in the respective biometrics,14 -16 a series of regression analyses were then conducted with change in the respective biometric being the dependent variable in each analysis and age, gender, the baseline value of the biometric and group entered into the models (Table 3). The standardized coefficients and R2 for the models are also reported.
Comparison of the Mean Changes in Selected Risk Factors From Baseline to Postintervention for the 8-Session and 16-Session Groups.
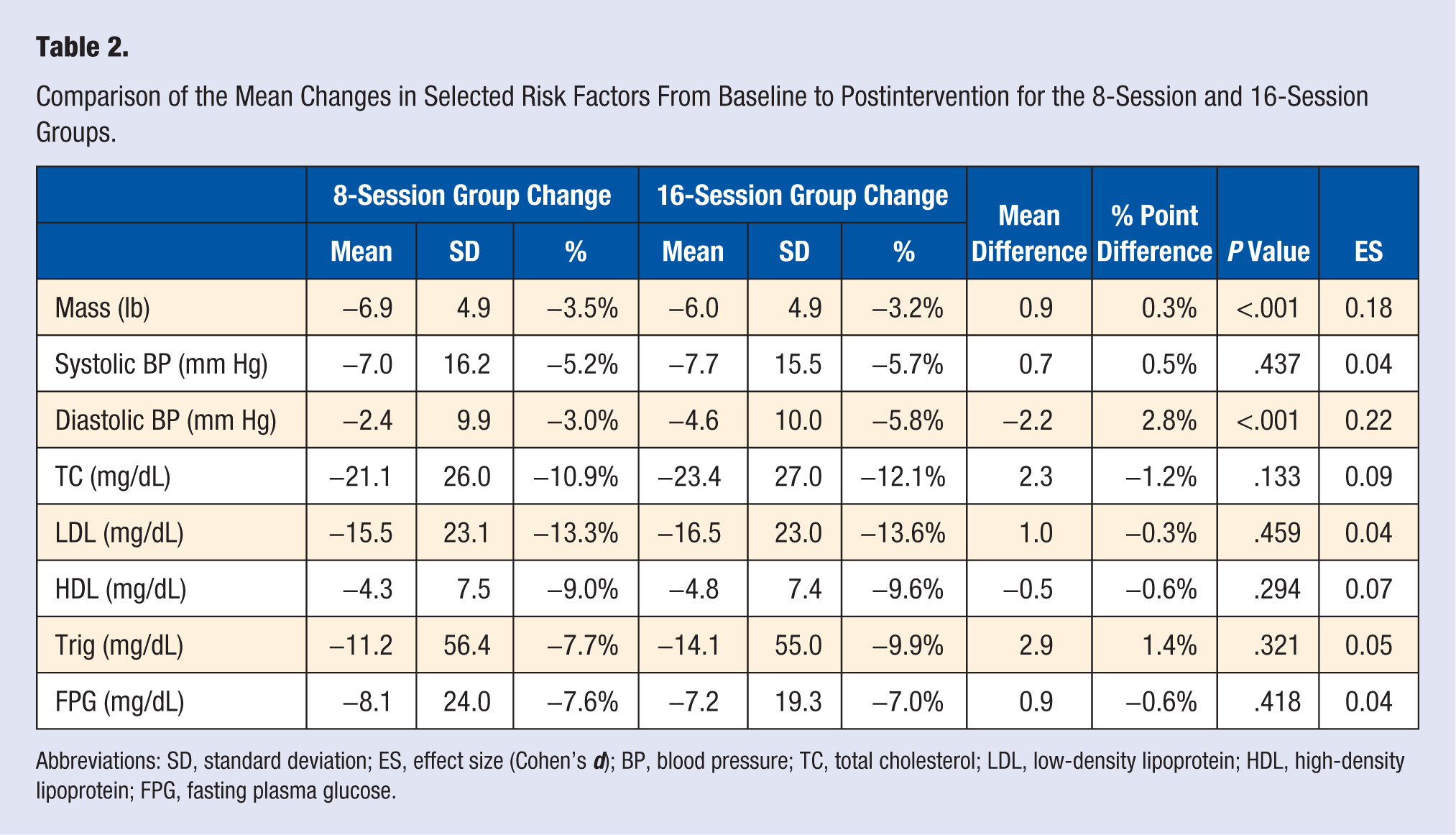
Abbreviations: SD, standard deviation; ES, effect size (Cohen’s d); BP, blood pressure; TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; FPG, fasting plasma glucose.
Regression Analyses Showing the Influence of Age, Gender, Baseline Level of the Respective Biometric, and Group (8-Session or 16-Session) on Pre to Post Biometric Changes.
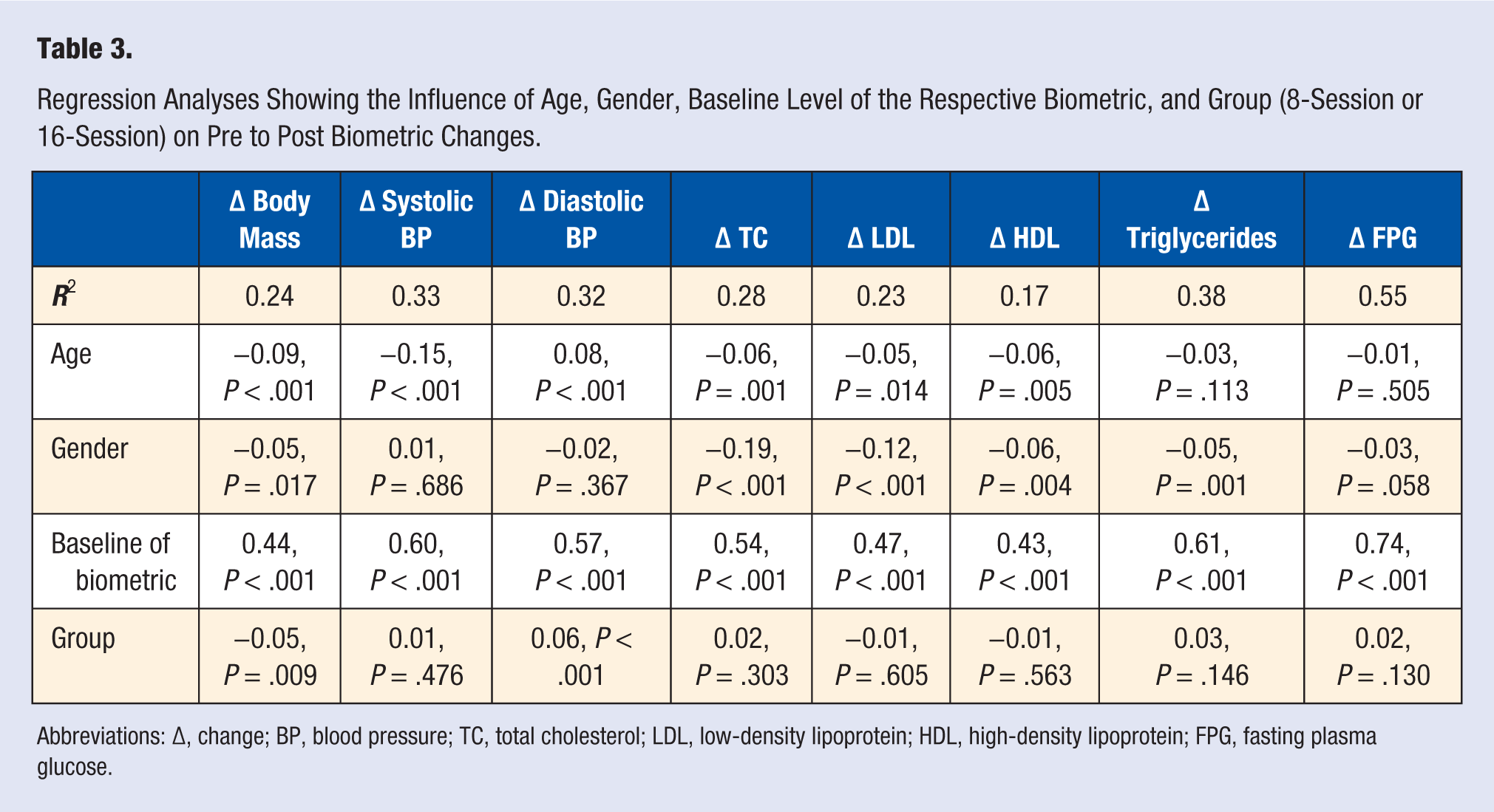
Abbreviations: Δ, change; BP, blood pressure; TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; FPG, fasting plasma glucose.
Results
The participants in the 8- and 16-session groups were similar in age (61.1 ± 9.0 vs 61.0 ± 9.2 years, respectively, P = .81); however, the 16-session group had a higher percentage of males (35% vs 29%, respectively, P = .01).
Table 1 shows the baseline biometrics of the participants in the 8- and 16-session groups. The 8-session group had a higher mean body mass and FPG, but lower LDL and HDL levels.
Comparisons between the 8- and 16-session groups in the pre- to postintervention biometric changes are presented in Table 2. The only significant differences between the groups were the changes in body mass and diastolic BP, although in both instances the effect size was small. The 8-session group experienced a significantly greater reduction in body mass, amounting to 0.3 percentage points or 0.8 lbs greater reduction than the 16-session group. Conversely, the 16-session group recorded a 2.2 mm Hg greater decrease in diastolic BP, equating to 2.8 percentage points. Controlling for age, gender, and the baseline level of the respective biometric, the 8-session group still achieved greater weight loss and the 16-session group greater reductions in diastolic BP (Table 3). Noteworthy, the regression models explained between 19% and 55% of the variance in the biometric changes with the baseline level of the biometric being the most important contributor in all models. As reported previously,14 -16 both age and gender predicted changes in several of the biometrics with the younger males in the cohort generally achieving better outcomes.
Discussion
The results of the present study indicated no clear difference between the outcomes achieved in 4 weeks by the 8- and 16-session versions of the CHIP lifestyle medicine intervention.
An obvious question that arises from this study is how low could the number of sessions be reduced to without compromising the efficacy of the intervention? From a cost-effectiveness perspective, the optimal number of sessions is the minimum number required to still achieve maximum benefits. Further study is therefore warranted to consider the comparative effectiveness of a 4- or 6-session CHIP intervention conducted over 4 weeks. However, it should be noted that further reducing the number of sessions would considerably compromise the comprehensive nature of the content presented in the program, resulting in it being difficult to achieve the learning and experiences currently offered in the program. In addition, as explained in the Methods section, one of the behavior change strategies of the CHIP intervention is to foster group support, which is a common theme in lifestyle medicine interventions,6,8,12 and this would be more difficult to achieve in fewer sessions.
This study contributes to a needed understanding of how the number of sessions in the early phase of a lifestyle medicine intervention (ie, the density of sessions) influences its initial outcomes. However, the intensiveness, or “dosage,” of a lifestyle medicine intervention may also be affected by several other factors, including the duration of the sessions, extent of lifestyle modifications prescribed by the intervention, and the group size.
In this study, the duration of the sessions in both 8- and 16-session programs were similar (1.5-2 hours), but other well-documented lifestyle medicine interventions such as the Ornish 9 and Esselstyn 8 programs involve sessions of longer duration. The Ornish program involves 4-hour sessions, and Esselstyn requires participants to participate in a 5-hour initial consult. Further research is warranted to better understand the influence of session duration on participant outcomes.
With regard to the magnitude of lifestyle change prescribed, lifestyle medicine interventions tend to be nutrition-centered and prescribe a whole-food, plant-based eating pattern.6,8,12 This eating pattern is more rigorous than that recommended by the Dietary Guidelines for Americans, 17 which is commonly used as a guiding principle for more conservative lifestyle interventions that do not target disease regression. However, there are varying levels of dietary “dosage” among the well-documented lifestyle medicine interventions. Esselstyn 18 mandates a very low-fat vegetarian diet (approximately 7% fat), achieved by avoiding even plant foods with higher fat content such as nuts and avocados. The Ornish program, while still low fat compared to National Guidelines (ie, 20% to 35% of total calories), 19 allows the inclusion of low-fat dairy. Ornish has shown that there is a dose-response to lifestyle medicine intervention, with greater changes resulting in greater improvements. 6 However, research is required to better understand the dose-response to lifestyle medicine interventions in order to optimize not only the efficacy but also the acceptability, palatability, and ultimately uptake of these interventions by individuals who could benefit from them.
Finally, studies are required to elucidate the optimal number of participants in lifestyle medicine interventions. While one-on-one coaching has been utilized in programs like the Diabetes Prevention Program, the economic viability and hence scalability of this approach has been questioned and instead group-based programs have been advocated. 20 Interestingly, weight loss studies have indicated that even individuals who prefer one-on-one coaching still achieve better weight loss when assigned to a group intervention. 21 Hence, group-based interventions might be preferable from both cost and clinical perspectives. Notwithstanding, the educational literature shows that excessively large groups/class sizes may not be ideal. 22 The optimal group size for lifestyle medicine interventions, which may vary in different contexts, needs to be investigated.
It is acknowledged that the findings of the study are limited to short-term responsiveness and cannot be extrapolated to longer term outcomes. As this study did not follow-up the participants beyond the 4-week intervention, it is not possible to determine whether the 16-session version more effectively cemented behavior change resulting in greater long-term compliance to the lifestyle practices promoted in the program and less recidivism. A long-term study of the CHIP intervention (ie, 3-5 year follow-up) indicated that participants who attended monthly “alumni” group support meetings conducted after the 4-week intervention were more likely to comply to the lifestyle recommendations of the program and experience greater long-term improvements in chronic disease risk factors. 23 This is consistent with findings of studies of the Diabetes Prevention Program that found that each additional session an individual participated in over a 6- to 12-month period equated to a 0.26 percentage point decrease in body weight. 20 These findings, combined with those of the present study, suggest that 8 sessions are probably enough in the first 4 weeks of a lifestyle medicine intervention to achieve significant reductions in chronic disease risk factors, comparable to that achieved by 16 sessions, but it is beneficial for follow-up sessions to be offered after this initial period to optimize longer term outcomes.
Conclusion
The findings of the study indicate that an 8-session version of the CHIP lifestyle medicine intervention achieves comparable reductions in chronic disease risk factors over 4 weeks to that achieved by the 16-session version of the program. This finding provides perspective on the necessary intensiveness of lifestyle medicine interventions, which is important in order to design programs for optimal clinical and cost effectiveness.
Footnotes
Acknowledgements
The authors would like to thank all the subjects and volunteer facilitators of the interventions involved in the study, in particular Susan Landless, who conducted or coordinated the 8-session “Healthy Beginnings” programs.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.