
Abstract
Interpersonal violence has a profoundly negative impact on individuals and our society. Health care providers are in a unique position to identify interpersonal violence, support survivors, and to contribute to violence prevention. The purpose of this article is to describe the nature, scope, and impact of interpersonal violence, its subsequent trauma on individuals, families, and society, and to delineate how providers can apply trauma-sensitive practice. The authors provide definitions, examples and prevalence rates and review theories of violence and violence prevention. They describe how to create a trauma-sensitive practice by being aware of the trauma that accompanies violence, the barriers to violence prevention, and how to intervene with patients about violence. Providers are urged to adopt universal screening practices, educate themselves on the nature of interpersonal violence and engage in screening, education, collaboration, and social justice activities to reduce interpersonal violence. Resources are provided to assist health care organizations, providers, and patients in addressing interpersonal violence.
‘“. . . creating a trauma-sensitive practice, . . . is the single most important action that health care professionals can take to reduce interpersonal violence and intervene skillfully . . .”’
Interpersonal violence has a profound effect on individuals and societies worldwide, affecting humans throughout their life span. In the United States alone, an average of 4 children every day die from abuse or neglect and 3 million reports of suspected child abuse and neglect representing more than 6 million children were made in 2012. 1 More than 1 in 3 women (35.6%) and more than 1 in 4 men (28.5%) in the United States have experienced rape, physical violence, and/or stalking by an intimate partner in their lifetime. 2 Approximately 22 million women and 1.6 million men has experienced rape, 2 and at least 5% to 10% of Americans older than 60 years will experience elder abuse. 3
Despite its high rate of occurrence, interpersonal violence is often shrouded in secrecy 4 and is not easily disclosed to health care providers and other members of the community. Several factors contribute to survivors’ reluctance to discuss their mistreatment. For instance, most perpetrators of interpersonal violence are parents, relatives, and other members of one’s household.3,5 Given this, child and adult survivors are in an untenable situation—often facing few real choices and anticipated dread associated with the anticipated consequences of disclosure.6,7 Moreover, survivors often experience shame and confusion, disempowerment, and a host of fears related to household disruption, retribution from the perpetrator(s), and an intimidating criminal justice system. 8 These factors and others inhibit disclosure of violence to health care providers. However, based on qualitative and quantitative research, convincing evidence shows that survivors of interpersonal violence are much more likely to discuss their abuse experiences with providers who (a) routinely and skillfully ask about violence, (b) demonstrate an understanding of the complexities of violence, and (c) demonstrate personal comfort with disclosures of violence and abuse. 9 For example, in a survey of 1313 women, 98% believed it is a “good idea” to screen for violence and 97% “felt OK” during the screen process. 10
While preventing interpersonal violence requires a multifaceted and community-based effort, health service providers, among all professional groups, may have the most likely and frequent contact with individuals experiencing, or at-risk of, interpersonal violence. For this reason and others, the American Medical Association (AMA) argued that “physicians have a duty to protect the welfare of all members of society by working to reduce the prevalence of violence and abuse amongst the general population.”11(p2)
We believe that creating a trauma-sensitive practice, including conscientious screening for interpersonal violence and trauma and familiarity with community resources, is the single most important action that health care professionals can take to reduce interpersonal violence and intervene skillfully when it has occurred. Many researchers and policy advocates have recently encouraged creating a “culture of trauma-informed care in health care settings”12(p461) as one key step toward a public health response to interpersonal violence. 13 Additionally, many health care groups, such as the American Academy of Pediatrics Committee on Child Abuse and Neglect, the American Academy of Family Physicians, and the Academy of Nurse Practitioners, have urged clinicians to screen their patients for violence. Despite these strong recommendations, it is believed that a small percentage of providers routinely screen for violence with the majority of their patients.14-17 For example, Lapidus et al., 17 in a survey (n = 903) of pediatricians and pediatric care-providing family physicians, concluded that 12% of respondents routinely screen for intimate partner violence (IPV) at well-child visits and Elliot et al 15 reported an overall screening rate of 10% among 1103 surveyed physicians. Stayton and Duncan, 16 in a review of 32 descriptive studies, indicated that 3% to 41% of physicians routinely conduct IPV screens. The primary focus of this paper is to point to key features of a trauma-sensitive practice and to provide practical suggestions for universal screening and patient support.
Defining Interpersonal Violence
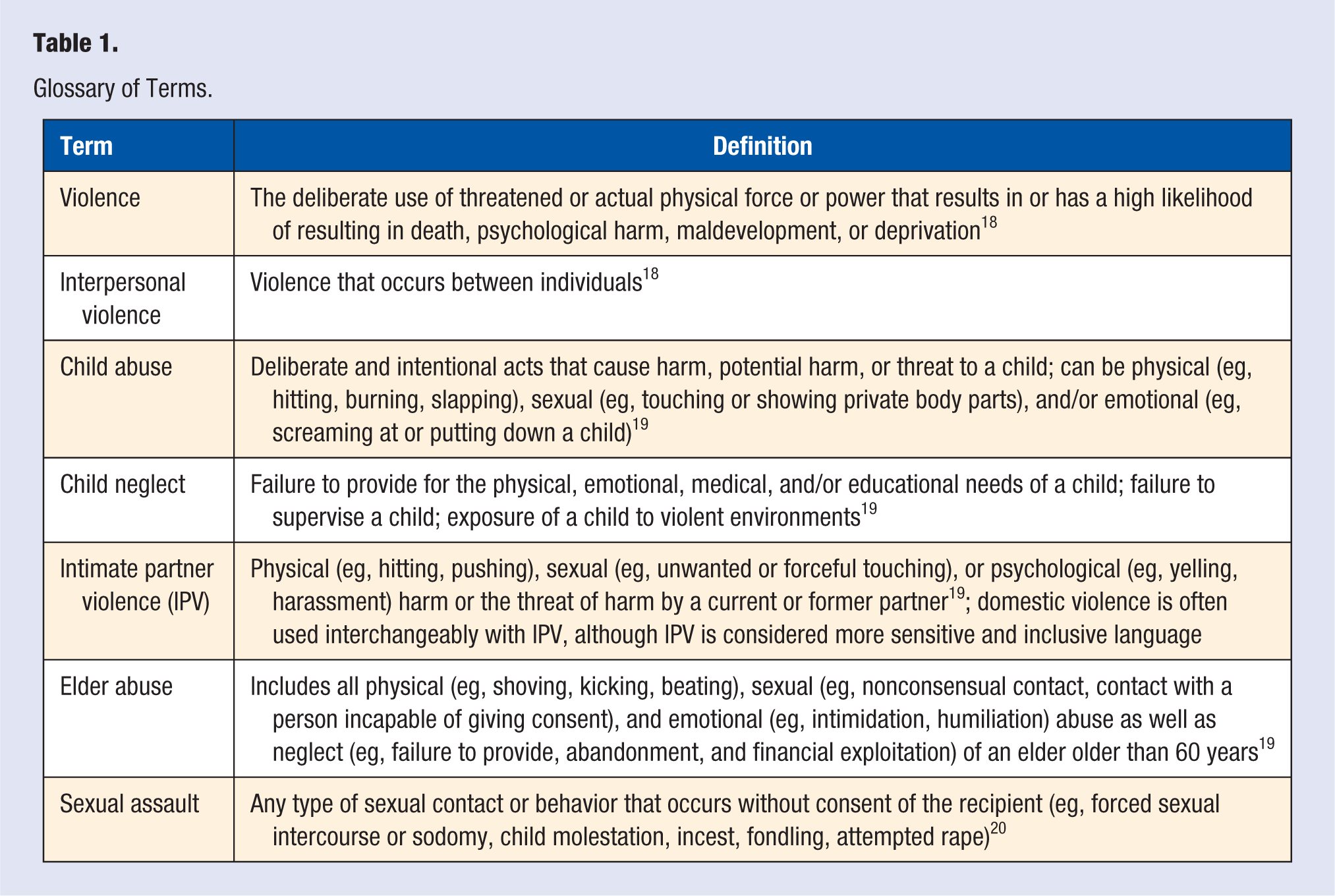
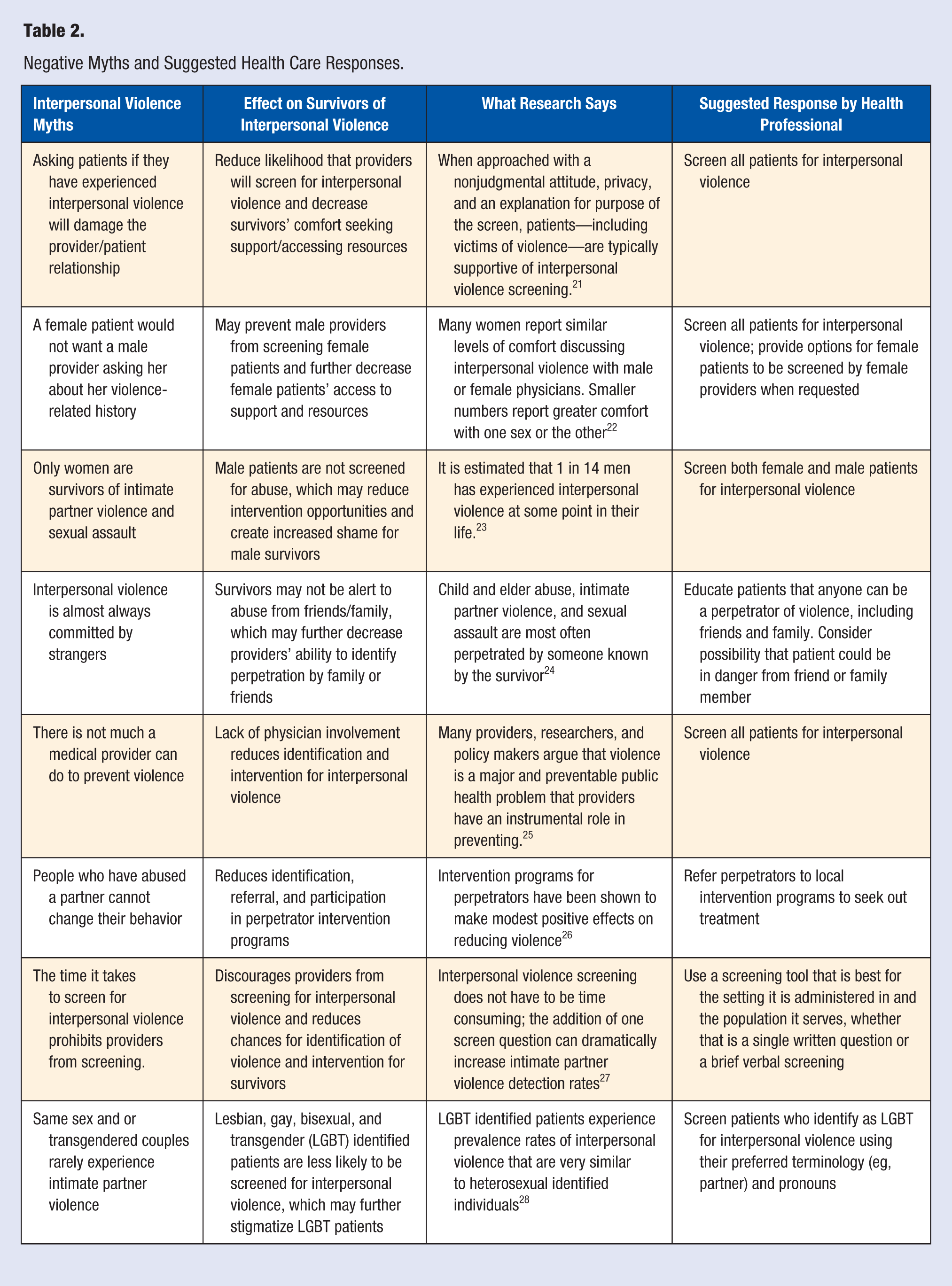
Although many forms of interpersonal violence exist, including, for instance, bullying and hate crimes, we more narrowly focus this review on violence that occurs more frequently among household members such as child abuse, elder abuse, and IPV (see Table 1). These types of violence are experienced by many health care–seeking patients. Table 2 presents some of the myths surrounding interpersonal violence and the suggested responses.
Glossary of Terms.
Negative Myths and Suggested Health Care Responses.
Child Abuse
Child abuse includes physical, sexual, and emotional maltreatment and exposure to (seeing or hearing) IPV.29,30 Physical abuse includes physically harming a child or doing something that could harm a child such as slapping, hitting with objects, burning, or pushing hard. And, often overlooked, neglect is the most common form of child abuse. Child neglect is failure to provide adequate food, clothing, shelter, health care, access to education, supervision, and/or love and emotional support. Emotional neglect includes inadequate nurturing or affection, permitted drug or alcohol abuse, including exposing or addicting a newborn to alcohol or other drugs, and inadequate attention to a child’s educational needs.29,30
Parental behavior that may indicate neglect include being apathetic or presenting with markedly depressed mood, seeming indifferent to the child, and denying the existence of child problems or blaming others for the child’s problems. Additionally, a parent remarking that his or her child is bad or worthless, or an overreliance on the child for adult emotional satisfaction are further parental behavioral warning signs. Common behavioral indicators of neglect for children, include wearing soiled or poorly sized clothing, inadequate clothing for weather, listless behavior or being tired with low energy, poor hygiene, smelling like urine or feces, and having dirty or decaying teeth.29,30
Child sexual abuse includes any sexual contact from an adult, such as touching private body parts or showing private body parts. Perpetrators, most often well known to the child, groom children by developing a relationship with them and then introduce them to sexual activity. Physical signs of sexual abuse often include redness, pain, bleeding or unusual discharge from the vagina or anal area, bruises in the genital area, unexplained urinary infections or sore throats, sexually transmitted diseases, pregnancy, head or stomach aches, and insomnia.29,30 Emotional/behavioral signs include age-atypical sexualized behavior, acting out in an atypical way with toys or objects, nightmares, sleeping problems, regressing to younger behaviors, unexplained mood or personality changes, self-mutilation, and sexual promiscuity in adolescence.29,30
Intimate Partner Violence
Intimate partner violence includes physical, sexual, or psychological harm or the threat of harm by a current or former partner. IPV occurs in all countries, 31 among all socioeconomic sectors, and in heterosexual and same-sex relationships. Several researchers have concluded that women perpetrate violence at rates similar to men in heterosexual relationships 32 though overwhelming evidence indicates that male violence toward women is qualitatively different—it is more severe, lethal, and more frequently occurs in tandem with repetitive coercive control. In 2010 in the United States, 1095 women were killed by their male partner, and 241 men were killed by their female partner. 2 These distinctions are important. As discussed later in this article, gender similarities and differences found in IPV have meaningful implications for screening, risk assessment, and health care intervention.
Intimate partner violence survivor and prevention advocates propose that the purpose of IPV is to use power to maintain control over the survivor. Lenore Walker 33 identified a cycle of abuse in which an abusive or violent event is followed by a honeymoon period where the abuser apologizes, makes promises that it will not happen again, and may directly or indirectly blame the survivor for the abuse. The honeymoon period is followed by building of tension where the survivor may feel like she is “walking on egg shells.” This tension usually ends in another violent outburst. Although this is the most commonly known form of IPV, many other variants exist—from situational couple violence, where violence occurs, though not in the context of a fear-based relationship, to sexual acquiescence, a much less recognized though very painful form of sexual violence. 34
Caregivers and bystanders may wonder why someone who is in an abusive relationship would stay in an abusive relationship. There are many reasons, including emotional and economic dependence on the abuser, fear of retaliation, disempowerment, and fear for the safety and well-being of one’s children. Being in an abusive relationship dampens one’s self-esteem, self-confidence, and self-efficacy. Among relationships where violence has occurred, ending that relationship or other changes in intimacy (eg, during pregnancy, birth of child, return to school, new employment) carries its own risk, including an increased risk of acts of violence, controlling behaviors, and homicide. 35 Moreover, many survivors of IPV for many good reasons do not want the relationship to end—they simply want the violence to stop. For a detailed description of the signs and symptoms associated with IPV, please see Futures Without Violence and the National Coalition Against Domestic Violence (Table 6).
Sexual Violence
Sexual violence is any type of nonconsensual sexual contact or behavior, including for instance forced sexual intercourse or sodomy, child molestation, incest, fondling, and attempted rape. 2 Sexual violence occurs at high rates in US society. For example, in a representative sample of 9086 US women 18 to 59 years of age, 40.3% reported having experienced sexual violence contact in their lifetime. 36 Although stranger rape also occurs at unacceptable rates, it is far more likely that health care providers will encounter sexual violence survivors who were assaulted—or are being assaulted—by someone known to them. 36 Women are sexually assaulted at rates much higher than men; men are most often sexually assaulted by other men. 36 For a detailed description of the features, signs, and symptoms of sexual abuse, please see the National Sexual Violence Resource Center (Table 6).
Elder Abuse
One in 20 elders in the United States will experience some form of elder abuse. 37 There are 6 common types of elder abuse, including emotional, physical, sexual, financial, neglect/abandonment, and self-abuse. 38 For World Health Organization (2008) definitions of elder abuse, please see Table 1.18-20 According to the Administration on Aging’s Elder Mistreatment Study, 37 more than 80% of elder abuse is committed by someone known to the elder. For example, family members accounted for 52% of sexual abuse, of which 40% were spouses/partners. Another 40% of sexual abuse of elders was committed by acquaintances and 85% of these incidences are not reported to police. 3 As with other forms of interpersonal violence, many survivors of elder abuse experience shame and guilt about the abuse. 3 An added source of shame for elders and a complicating factor for health care providers is that the abuser is often an adult child. 3 And, given that the elder typically raised the child, he or she may assume responsibility for their adult child’s abusive behavior. 3 Additionally, fear of consequences such as retribution, loss of freedom, and loss of a loved one increase elder’s reluctance to disclose abuse. 3
Common Features Across All Forms of Interpersonal Violence
Despite some significant differences among the types of violence outlined in this article, there are common factors or themes across all forms of interpersonal violence:
Vulnerability of victims/survivors due to age, gender, physical, intellectual, or emotional state; socioeconomic standing; or lack of social support.36,37,39
Perpetration tends to be committed by a family member, loved one, friend, or trusted acquaintance who is in a more powerful position due to their age, gender, size, strength, experience, knowledge, or social standing.36,37,39
Many survivors of interpersonal violence display similar reactions to the abuse: feelings of fearfulness, betrayal, powerlessness, shame, guilt, self-blame, and reluctance to report abuse. 40
Significant underreporting of child, intimate partner, and elder abuse.41,42
US society tends to deny that interpersonal violence occurs and, in some circumstances, blames the survivor for the abuse, particularly with regard to sexual assault and other forms of IPV. 43
Demographic factors, including gender, age, ethnicity, cultural background, socioeconomic status, and spiritual beliefs play an important part in all forms of abuse, affect the meaning that abuse has to the survivor, their openness to disclosing abuse, and the options that a survivor will consider to remain safe. 44 Providers’ attitudes, beliefs, and stereotypes relative to these factors may also influence providers’ ability to successfully communicate, diagnose, and intervene in abuse situations. 45
Consequences of Interpersonal Violence
Interpersonal violence has serious consequences on the survivor’s physical and emotional health, the well-being of communities and society, and results in enormous financial cost.46,47 Effects of physical trauma can include bruising, burns, lacerations, broken bones, long-term brain damage, other permanent disabilities, and even death. 48 Neglect can lead to malnutrition and lack of medical and dental care and in extreme cases, death. Sexual abuse and sexual assault can lead to sexually transmitted infections including syphilis and human immunodeficiency virus (HIV). Women who have been sexually abused are more likely to experience physical problems such as chronic pelvis pain, gastrointestinal problems, headaches, and obesity. 49 Adults who experienced abuse or neglect as children are more likely to experience heart, lung, and liver disease. 50 These negative health outcomes are linked to stress and behavioral factors, including rates of smoking, alcohol and drug use, and overeating among survivors. 50
Emotional Consequences
Emotionally, interpersonal violence can traumatize its recipients. 45 Many survivors experience anxiety, hyperarousal, intrusive memories, emotional numbness, and memory problems. 45 Children exposed to violence can experience difficulties with attachment and regressive behavior and in comparison with nonexposed children are at greater risk for anxiety, depression, aggression such as bullying and fighting and other conduct problems. 51 Additionally, abuse committed by a caregiver is qualitatively different for survivors. Coined “betrayal trauma,” abuse committed by a close family member or partner is more likely to lead to disassociation, numbness, and constricted relationships. 45 While the majority of violence survivors do not behave violently in the future, the vast majority of people who do use violence are themselves survivors of interpersonal violence.52,53
Economic Consequences
Finally, abuse and neglect is expensive to society at large and has an enormous impact on the health care system. For example, survivors of child abuse and neglect, IPV, and sexual assault have higher health care costs and more visits to hospital emergency rooms than nonabused individuals.2,54 Given that survivors of interpersonal violence frequently present in medical facilities with a host of injuries and other physical, emotional, and behavioral symptoms, health care providers are in a crucial position to acknowledge trauma and provide support.
Theories of Violence
Why do some humans act violently particularly toward more vulnerable individuals? Why do they hurt family members, friends, or acquaintances with whom they have a close bond? Interpersonal violence is a complex array of behaviors that cannot be adequately explained by one theory. Biological, emotional, contextual, community, and societal factors play a part. Many scholars have used a social-ecological approach to understand and explain the causes of interpersonal violence. 55 This approach perceives violence as resulting from a complex interplay of individual, relational, community, and social factors.
Social learning theories of IPV perpetration suggest that we learn from observing and imitating the behavior of others. From this perspective, abusive behavior is learned, both as a result of household experiences and social messages about violence, gender, and conflict resolution. Applied specifically to IPV, social learning theory explains the intergenerational transmission of violence—children learn abusive behavior from their parents and adults modeling those behaviors.56,57 However, this theory certainly does not fully explain violent behavior. Although a correlation between witnessing and experiencing violence in childhood and subsequent perpetration of violence as an adult exists, the majority of adult survivors of childhood abuse do not behave violently later in life. 53
Feminist and political-economic theories argue that violent behavior is largely a consequence of social norms. Feminist theories link gender roles and gender-based power, arguing that IPV can be largely understood as a consequence of patriarchal sexist social norms and their pervasive influence across social systems. 58 From this vantage point, violence is conceptualized as coercive control, as represented by the Domestic Abuse Intervention Project’s “Power and Control Wheel.” 59 This model asserts that power and control is expressed through a variety of tactics including threats, minimization and denial, assertion of male privilege, intimidation, isolation, emotional abuse, economic abuse, and use of children as a pawn toward individual gain. Considering violence as an outcome related to power decreases the psychological tendency to assume that violence is an individual symptom related to disorder, thus reducing emphasis on the need for social change. 58 More recently, feminist theory has aimed to become more inclusive, considering the impact various social locations have on an individual’s experience of violence. 60
Political economic theory offers a slightly different slant on the underlying explanation of violence. This theory uses economic, social, and political factors to explain the ways violence occurs in both local and global contexts, describing these three areas as primary causes behind violent outcomes. 61 In short, political economic theory focuses on the structural, as opposed to individual, explanations for violence. In this way, violence is rooted in material relationships (ie, those relationships that allocate authority, privilege, and/or resources). When determining the underpinnings of violence in any setting, political economic theorists argue that material factors (eg, socioeconomic, employment, and leadership) must be considered; these factors are largely influenced by normative and unequal gender norms globally and place women at disproportionate risk for experiencing violence. Thus, political economic theories posit that more global inequalities—specifically those that are structural and material in nature—perpetuate violence against women. 61 Researchers of sexual assault frame this as a “rape and sexual assault culture,” which promotes the belief of the acceptability of sexual aggression and contributes to difficulties in the criminal justice system that reduces the power of victims and their advocates. 62
Assumptions About Gender and Violence
Being aware of the role that personal assumptions about gender play in IPV universal screening and medical care is an important part of developing a trauma-sensitive practice. Early research identified males as the most frequent perpetrators of violence and women as survivors. 63 Male power and control over the victim was identified as the primary motivating factor of the abuse. 33 While most men are not violent, most relationships characterized by coercive control (intimate terrorism) and most acts of severe violence are orchestrated and committed by men. 2 Male violence toward women is one of the leading causes of injury for women in the United States and is a significant health concern worldwide. 64 This information has been widely used in the development of intervention programs and community responses to violence. More recent data, however, paint a more complex gender-related picture.
While conventional beliefs about IPV have emphasized moderate to severe physical violence, including a set of physically violent and threatening behaviors, pervasive control tactics, and a fear-based relationship, Johnson 32 argued that this form of violence is one type of violence among an array of violence typologies. Conventional definitions of IPV (ie, physical, control, fear-based), named intimate terrorism by Johnson, 32 is almost exclusively perpetrated by men toward women. Johnson and Ferraro 65 estimate that among the general population, only 11% of “violent relationships” meet intimate terrorism criteria.
Johnson 32 proposed 4 distinctly different types of IPV: intimate terrorism, violent resistance, situational couple’s violence, and mutual violent control. Intimate terrorism is described as an ongoing pattern of behavior motivated by a desire to control their partner. This type of abuse, as mentioned, is primarily committed by men. Violence resistance occurs in response to intimate terrorism. Its purpose is to defend oneself and/or retaliate for previous acts of violence. This violence is primarily committed by women in response to intimate terrorism. Situational couple’s violence occurs in the context of couples’ relationships. This violence is sporadic and arises out of conflict in the couple’s relationship. Committed by both male and females, it is the most common form of IPV. Situational violence is not part of an ongoing pattern of control but is understood as a misguided expression of frustration or anger. This type of violence is thought to be symmetrical, with roughly equal numbers of males and females initiating the IPV. 32 Mutual violent control occurs when both members of the couple engage in violence for the purpose of controlling their partner. This type is believed to rarely occur. 66
Based on these data and a growing body of literature, it is now much more widely accepted that IPV and its association with gender is more complex than was originally formulated. While Johnson’s 32 model continues to be investigated and tested, 67 the notion that there are multiple types of IPV and that women as well as men can be perpetrators suggests that providers should reasonably assume that men and women can both be survivors and perpetrators of violence, and that violence quite often takes many forms—from severe acts of physical aggression to much more subtle and confusing forms of violence such as sexual persuasion and acquiescence. 68
A Public Health and Violence Prevention Framework
Winslow 69 envisioned the “public health campaign” as a system designed to prevent disease, injury and disability and to promote physical and mental health. More recently, the Institute of Medicine argued that the mission of public health is “the fulfillment of society’s interest in assuring the conditions in which people can be healthy.”70(p40) When applied to obesity, for instance, these assumptions are self-evident. Health care providers across virtually all disciplines, for example, are expected to understand the basic principles and evidence associated with healthy diet and exercise. By extension, public and private health care professional bodies devise and advocate policies that encourage active lifestyles and the social norms and infrastructure that support those behaviors. In this way, a role for individual providers and professional organizations toward obesity prevention is widely accepted and intervention strategies are plentiful. In contrast, health care providers’ role in preventing violence is much less widely understood, accepted, and practiced.
What can health care providers practically do to reduce violence among their patient population and in the community at large? An expanding array of providers, researchers, and policymakers argue that violence is, indeed, a major and preventable public health problem and that providers have an instrumental role in its prevention. 25 The AMA, in a report by the Council on Ethical and Judicial Affairs (CEJA Report 6-1-07),11(p2) stated that “physicians have a duty to protect the welfare of all members of society by working to reduce the prevalence of violence and abuse amongst the general population.” Similarly, the American Nurses Association urges nurse education programs to ensure their members have the skills necessary for the prevention of violence. A survey conducted by the American Academy of Pediatricians in 2006 concluded that a vast majority of pediatricians believe they can support child abuse prevention by providing “anticipatory guidance.” 71 For these organizations—and many of their counterparts—violence prevention is within health care providers’ scope of practice.
Because of its prevalence and its physical, emotional, social, and financial costs, interpersonal violence is indeed an economic, social justice, criminal justice, and public health problem. Given this, public health strategies are very well suited for violence prevention. Unlike the criminal justice system, which responds to violence after it occurs and targets prosecution, punishment and rehabilitation of individuals, the public health model emphasizes population-level change and includes each of the following components: (a) community-level assessment, (b) primary prevention and social norms change, and (c) active community participation toward problem resolution. 25 Additionally, public health violence prevention strategies target known risk and protective factors in an effort to reduce risks and to enhance known buffers of violent behavior. Taken together, these efforts are designed to change the social conditions that cause violence and those factors that have allowed it to persist across generations.
The Unique Opportunity of Violence Prevention
One of the most salient and challenging factors associated with violence prevention is the fact that violence most often occurs within households and is very often shrouded in secrecy, shame, and self-blame. 4 This occurs at the individual level and is mimicked at the social level in the form of collective denial and minimization of abuse. For example, a randomized community sample of survivors of abuse (n = 351) asked participants 8 : “During the time when you first experienced any of the violence just mentioned, how often did anyone try to help or protect you?” To this question, 47.6% of all respondents reported “never,” 19.4% responded “rarely,” 12.8% responded “sometimes,” and 11.7% responded “often.” Among all participants, the average number of trauma types (eg, physical, sexual, and emotional abuse) was 5.99 and 47.9% were first abused when they were younger than 6 years; 20.5% were first abused between the ages of 7 and 12 years. Moreover, a full 80.6% disagreed or strongly disagreed that the general public “knows how to help people heal from trauma.” These data support the notion that survivors—most of whom are first abused in childhood—are very often left to live in silence with their traumatic experience. Later in life, many survivors have low confidence that the general public understands their experience and knows how to be helpful toward trauma healing.
Given this backdrop, health care providers are in a powerful and unique position to counter the silence that so often is associated with violence and abuse. Health care providers who actively practice violence prevention strategies act as a corrective, healing experience for survivors of violence. In this way, violence prevention practitioners are themselves protective factors and can act as a bridge to the larger community by countering the collective silence that so often accompanies violence.
Specific Actions and Strategies
Health care providers can take specific and practical steps to reduce violence in their communities and in their patient population. This can include the following actions: (a) developing a trauma-sensitive practice, (b) universal screening, (c) policy development, and (d) advocacy and active participation.
Developing a Trauma-Sensitive Practice
The power of a trauma-sensitive practice is that it counters the isolation, shame, and self-blame that otherwise sustains interpersonal violence in our communities. Trauma-sensitive practitioners and workplaces communicate, in word and deed, several key messages to patients and staff: (a) we know that many of our patients and staff are experiencing or have experienced interpersonal violence; (b) you can talk about those experiences here—addressing trauma is a part of your health care needs; (c) we are competent to support you in a safe, skilled, and nonjudgmental manner; and (d) your trauma-related symptoms are a natural response to interpersonal violence; there is nothing wrong with you, our focus is on supporting you to address, to the extent you wish, what happened to you.
Many useful guidelines and recommendations for trauma-sensitive or trauma-informed practice and protocols now exist, and have been adapted for a variety of health care settings and specialties.72-74 In short, trauma-sensitive advocates urge health care organizations to adopt trauma-aware policies and practices in order to create a “trauma-informed culture” that is enacted reliably by individual practitioners and staff. In this way, institutional support is vital for implementation fidelity. 73 Fallot and Harris 75 encourage health care organizations and practitioners to begin with a self-assessment to determine the degree to which their setting and practitioners communicate trauma-sensitivity. Self-assessment items include, for instance, the following:
To what extent do our patients and staff feel physically and emotionally safe here?
Everyone here acts in a respectful, caring, and professional manner.
There are direct and indirect messages in this environment that tell me it is okay to discuss interpersonal violence.
If I discuss interpersonal violence, I have a good idea of how it will be handled. I trust that it will be handled skillfully.
The providers and staff are as sensitive as possible when they ask me about difficult or frightening experiences I may have had.
I feel like I am a partner with the staff and providers; they listen to what I think and what I want, and use that information in decision making.
I get the sense that this practice is healthy; people seem to enjoy working here and working with each other.
For more information about the features of trauma-sensitive practice, please see Table 3 and Self-Assessment and Planning Protocols. 75
Developing a Trauma-Sensitive Practice: Suggestions for Providers. a
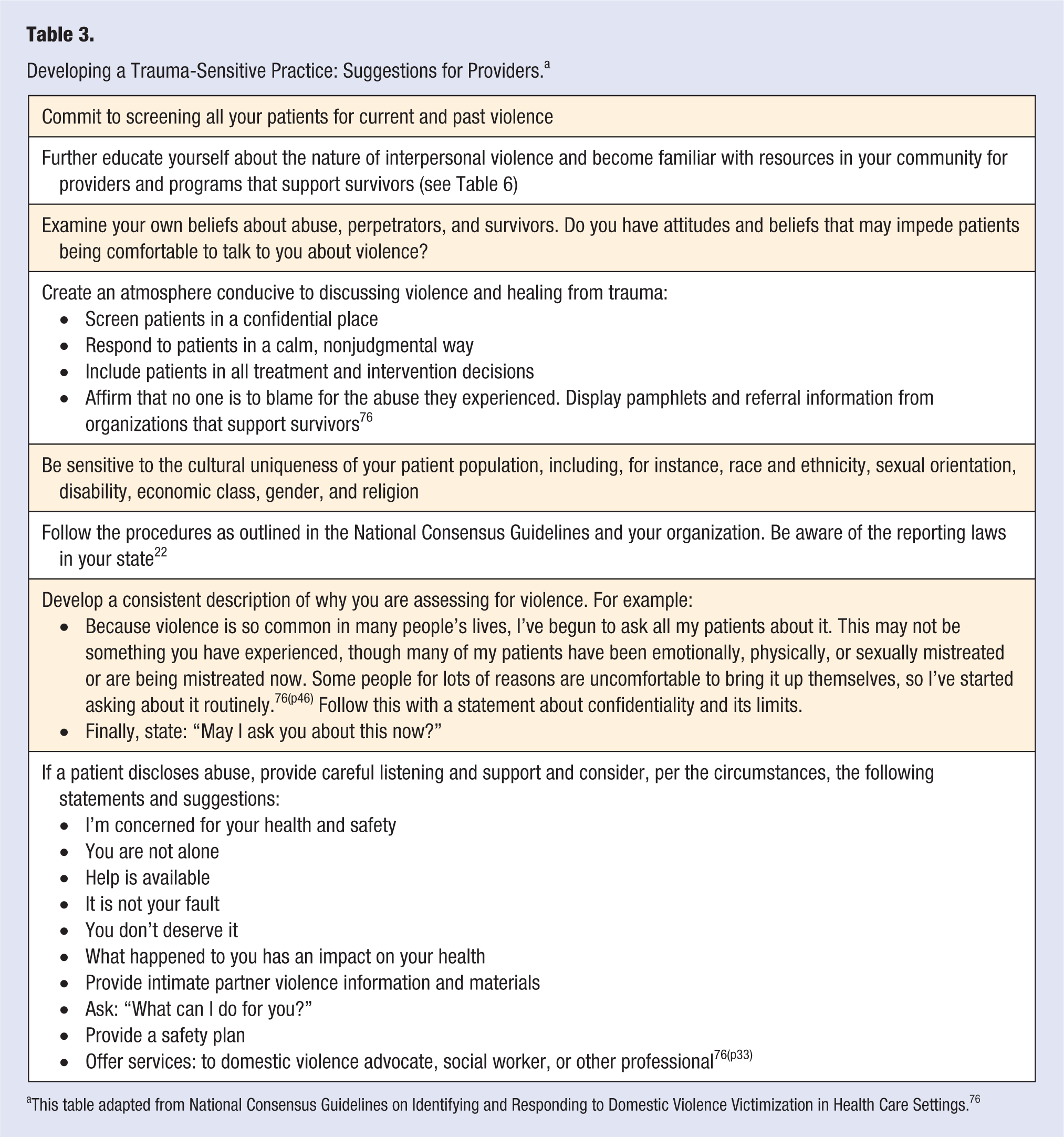
This table adapted from National Consensus Guidelines on Identifying and Responding to Domestic Violence Victimization in Health Care Settings. 76
Universal Screening
Universal screening is the practice of inquiring about violence with all patients regardless of risk factors.
77
Proponents of universal screening argue that routine screening is warranted because (a) violence is prevalent in society and, as such, many patients have experienced or are experiencing it; (b) violence is negatively correlated with well-being; (c) if it is occurring or has occurred, it is a pertinent factor in health care planning; and (d) spontaneous disclosure of violence is unlikely.27,78,79 Many professional associations recommend universal screening, including, for instance: the AMA, the American Academy of Family Physicians (AAFP), the American Academy of Nurse Practitioners (AANP), the American College of Emergency Physicians (ACEP), and the American College of Nurse Midwives (ACNM). A systematic review of universal screening for intimate partner violence concluded, Under certain circumstances (e.g., when conducted with a nonjudgmental attitude, in privacy, and when a clear rationale for the purpose of the screen is provided), patients—including victims of violence—are generally supportive of IPV universal screening. Emerging evidence also suggests that (IPV) universal screening can be conducted safely, increases rates of disclosure, and can lead to more appropriate handling of presenting and underlying concerns.9(p10)
Although patients overwhelmingly report a favorable opinion of screening when performed competently, most health care providers do not screen routinely and many describe a great deal of personal ambivalence and anxiety about screening.9,80,81 A review of 32 descriptive studies concluded that only 3% to 41% of physicians routinely conducted IPV screens. 16 Health care providers, however, are much more likely to screen for violence when they (a) have been trained to screen, feel competent in screening, and receive institutional support; (b) believe violence is prevalent among their patient population; and (c) believe screening is within their role and a part of their responsibility as a health care provider. 9
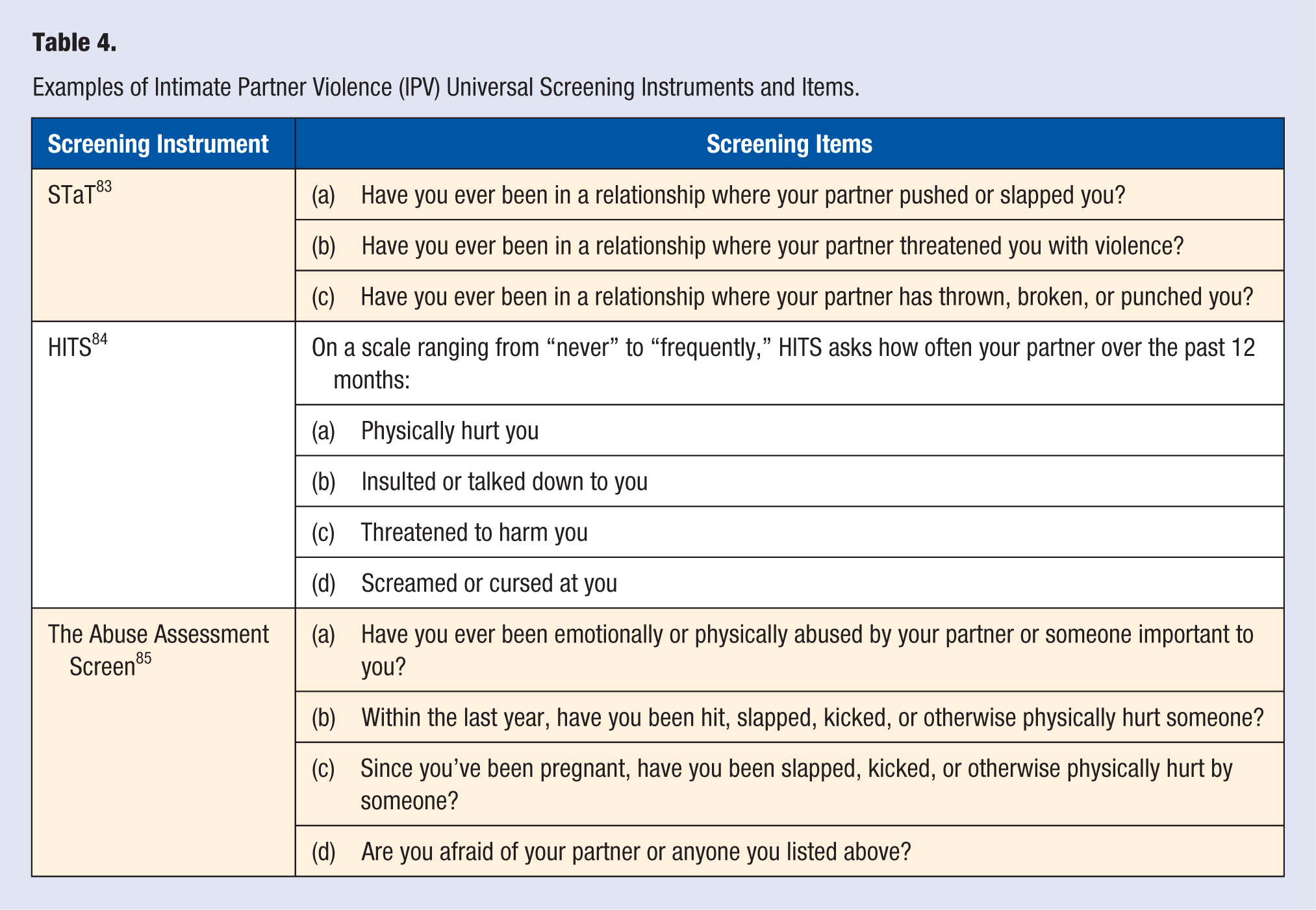
Several models for violence screening exist and most have been designed, specifically, to assess for intimate partner violence. 77 Generally, screening models include the following (a) a set of questions asked of all patients in writing and followed-up orally at intake, time of first visit, or early in the treatment relationship; (b) questions are asked independent of other family members, if applicable; and (c) the questions are often tiered, moving from general screening questions to a more thorough violence assessment and risk assessment, if warranted.9,27,82 For an example of screening questions, see Table 4. For a thorough description of a tiered universal screening model, see Todahl and Walters. 9
Examples of Intimate Partner Violence (IPV) Universal Screening Instruments and Items.
It is important to note that universal screening practice has not been shown to improve health care outcomes.86-89 Klevens and colleagues, 86 in a 3-group blinded randomized controlled trial of women seeking health care services (n = 2364), found that screened patients did not have improved health outcomes relative to nonscreened participants. This calls to question, for some, the utility of universal screening; however, from a prevention perspective, the main objective of universal screening is not a disclosure of violence—or even direct improvement in health outcomes. Instead, universal screening counters the isolation that so commonly accompanies violence and, over time, may function as an individual and collective protective factor for subsequent violence. Todahl and Walters27(p252) argued that universal screening “creates an atmosphere that legitimizes a conversation about violence if and when the patient chooses to discuss it and engenders confidence in the provider’s ability to competently respond to a violence disclosure.” Moreover, the act of skillfully raising questions about violence communicates that health care providers (a) recognize that interpersonal violence is a prominent public health problem, (b) invite conversation about violence should it be relevant in the patient’s life, and (c) are willing to discuss violence at any point during the course of treatment. 67 This is an act of prevention in that it counters the social norm of silence, denial, and minimization that so often surrounds violence.
Advocacy and Active Participation
Health care providers enjoy high social status and are influential members of society. Because of this influence, the health care community is an instrumental partner toward community change. This is fostered when health care professionals (a) advocate for violence prevention policy (such as the AMA’s position on universal screening), (b) actively participate in collective efforts to reduce violence, 90 and (c) advocate for promising and evidence-based violence prevention programs (Table 5).
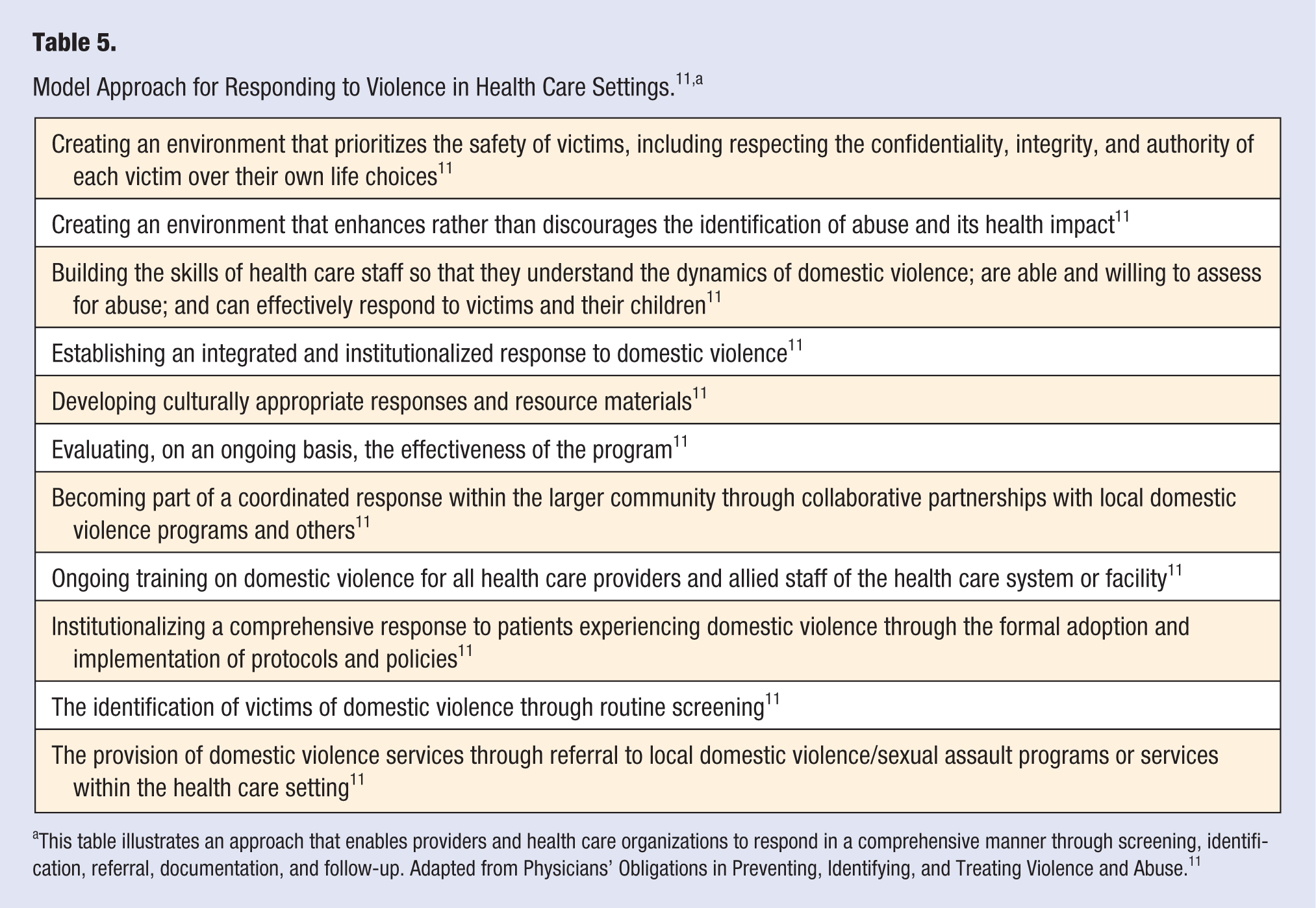
This table illustrates an approach that enables providers and health care organizations to respond in a comprehensive manner through screening, identification, referral, documentation, and follow-up. Adapted from Physicians’ Obligations in Preventing, Identifying, and Treating Violence and Abuse. 11
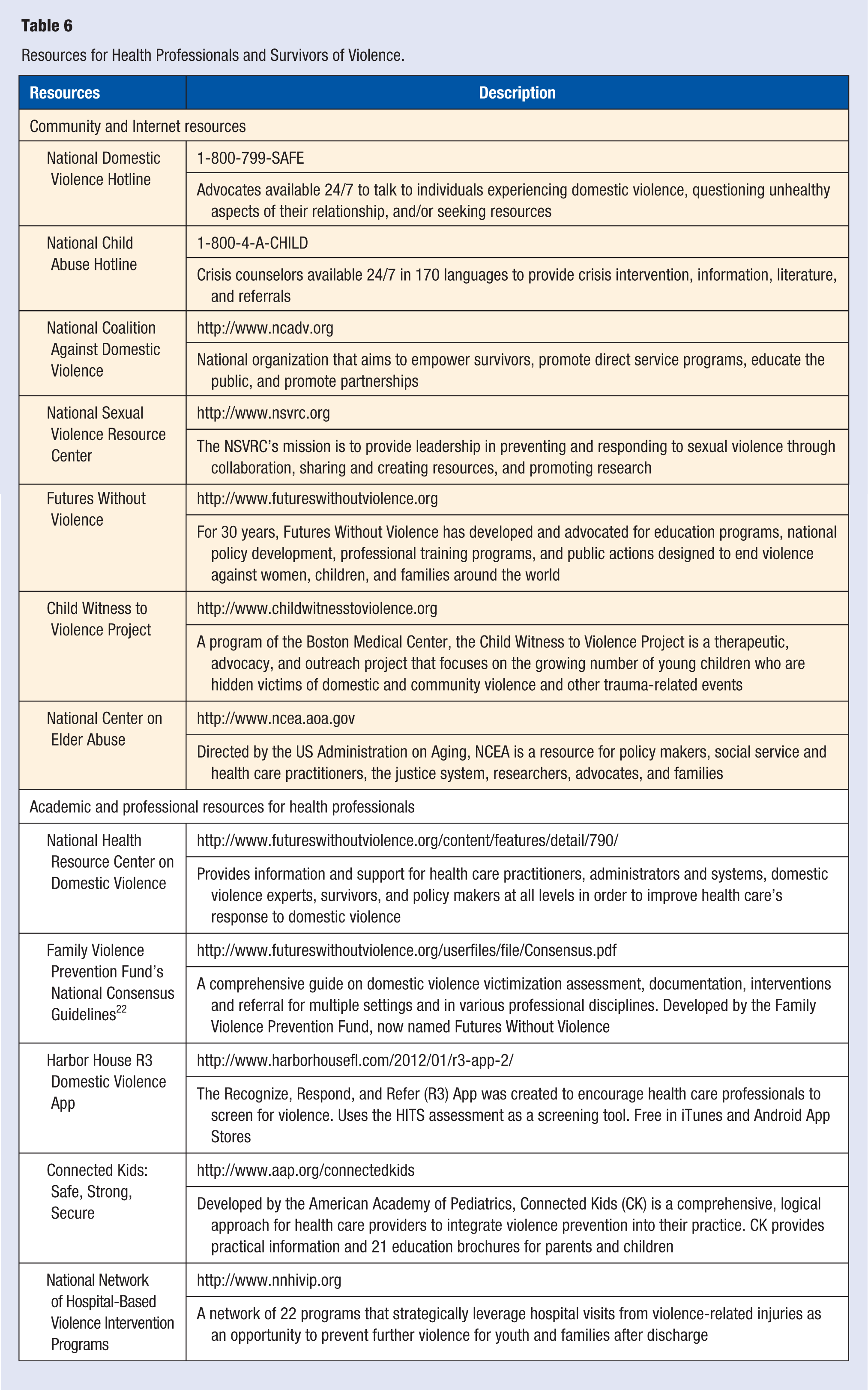
There are many examples of the health care community’s advocacy and active participation in effective and promising violence prevention and intervention programs. For instance, research investigating the impact of Nurse-Family Partnerships (NFP)—which provides home visitation during pregnancy and infancy—found that child participants were less likely to have emotional and behavioral problems and had better receptive language and sustained attention relative to controls. 91 Also, a 15-year follow-up clinical trial of NFP concluded that participants had significantly lower overall reports of child maltreatment relative to controls. 92 Additional examples of health care organizations that provide leadership, intervention and interpersonal violence prevention services include: The National Network of Hospital-Based Violence Intervention Programs; Sexual Assault Nurse Examiner’s Program; the American Academy of Pediatrics Medical Home for Children and Adolescents Exposed to Violence; Connected Kids: Safe, Strong, Secure; the US Department of Health and Human Services Domestic Violence Response in Health Care Settings Model; and Trauma-Informed Care. For a list and brief summary of these programs and others, please see Table 6.
Resources for Health Professionals and Survivors of Violence.
Conclusions
Interpersonal violence causes significant harm to individuals and our society. While reducing this violence will require a team effort involving many different organizations and individuals, health care practitioners are uniquely positioned to respond to this crisis by creating trauma-sensitive practices. Establishing these practices will require health care organizations to develop policies and procedures that encourage universal screening, education for providers and patients, and intervention with survivors of interpersonal violence. It also requires individual practitioners to routinely screen their patients and commit to further develop the attitudes, knowledge, and skills to effectively respond to their patients’ disclosures. Finally, health care providers can use their unique power and privilege to advocate for policies and programs aimed at reducing interpersonal violence. While a thorough detailed description of the assessment and intervention process is beyond the scope of this article, the authors have provided resources to assist you in this process. The authors recognize that implementing universal screening will require providers to take additional time out of their busy schedules, take risks and ask their patients difficult questions. However, we believe that by adopting trauma-sensitive practices, providers can reduce the secrecy and shame that accompanies interpersonal violence and promote the safety, healing and well-being of their individual patients and our society.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.