
Abstract
Purpose. To present results of a scoping review focused on skin cancer risk behaviors and other related health risk behaviors. Skin cancer is highly preventable, yet it is the most common form of cancer in the United States with melanoma rates increasing. Limited research has been conducted examining the relationship between skin cancer prevention behaviors and other health risks, yet multiple behavioral health risk interventions have shown great promise for health promotion and reduced health care costs. Methods. Online databases were searched for research articles on skin cancer risk behaviors and related health risk behaviors. Results. Thirty-seven articles met inclusion criteria examining skin cancer behaviors including risk, sun protection behaviors, sunburn, and indoor tanning. The majority of existing studies focused on the relationship between skin cancer prevention behaviors and physical activity, body mass index, smoking, and alcohol abuse. Adults were the primary population of interest with some studies of adolescents. Conclusions. Poor skin cancer prevention behaviors were associated with alcohol use, marijuana use, and smoking among adolescents and adults. Studies on body mass index and physical activity had mixed relationships with skin cancer prevention behaviors and warrant further investigation. Indoor tanning was associated with other risky behaviors but other skin cancer prevention behaviors were not studied.
‘Melanoma, the deadliest skin cancer, accounted for more than 76 000 cases of skin cancer in 2014.’
Skin cancer is the most common form of cancer in the United States, with more than 3.5 million cases of basal and squamous cell skin cancer diagnosed in the United States every year. 1 Melanoma, the deadliest skin cancer, accounted for more than 76 000 cases of skin cancer in 2014. Furthermore, 1 out of every 5 people in the United States will develop skin cancer during their lifetime. 2 The economic consequence of this cancer has resulted in a direct annual treatment cost of more than 4 billion dollars. 3 The 3 most common types of skin cancer include squamous cell carcinoma, basal cell carcinoma, and melanoma. Nonmelanoma skin cancers (NMSC), including squamous and basal cell carcinomas, are the most common forms of skin cancer and are rarely fatal. 4 However, though not the most common form, melanoma is the most lethal. 5 An estimated 12 190 deaths (9180 from melanoma and 3010 from other nonepithelial skin cancers) occurred in 2012 in the United States. 1
Skin Cancer Causes
Ultraviolet (UV) radiation from the sun or indoor tanning machines has been directly linked with the development of skin cancer and has been declared a carcinogen by the US Department of Health and Human Services.
6
Exposure to UV light is the single most modifiable risk factor for skin cancers and is mostly preventable by avoiding the sun and indoor tanning machines.
3
The American Cancer Society recommends avoiding the sun during peak hours (10
There is evidence to support the relationship between inadequate sun protection and cancer because melanoma is now the most common form of cancer for people aged 25 to 29 years. 7 Unfortunately, melanoma rates are increasing for this population. In fact, over the past 40 years, melanoma rates among those under the age of 40 have increased 800% in women and 400% in men. 8 This is not surprising given young adults aged 18 to 29 comprise the most active age group engaging in risky UV exposure. 9 Childhood, adolescent, and young adult UV exposure is damaging because it accumulates toward later skin cancer risk. 10 Furthermore, young adults, specifically college students, obtain a majority of their lifetime UV radiation exposure before and during this time of life. 7 Although this group is spending significant time in the sun, only about 5% of college students properly use sunscreen. 11 Further evidence of poor sun protection behaviors was illustrated in a national telephone survey of young adults, which revealed that 72% reported having had at least 1 summer sunburn, 30% reported at least 3 sunburns, and 12% reported more than 5 sunburns. 12 Sunburns are the short-term effect of excessive UV exposure. Factors associated with increased odds of sunburn include greater sun sensitivity, lighter skin tones, younger ages, hours spent outdoors, sunbathing, and desirability of a tan. 12
Indoor tanning is another avenue for UV exposure, with an estimated 40% to 60% of college students having used indoor tanning machines. 9 Indoor tanning, also referred to as sunlamps, tanning booths/beds, and artificial tanning, has been positively associated with skin cancer.13,14
Skin Cancer Prevention
According to Healthy People 2020, the US Department of Health and Human Service’s framework for national health, skin cancer has been recognized as a pressing national public health issue. As a result, a set of objectives have been developed for adolescents and adults to reduce high-risk behaviors. The 2020 objectives for adolescents include the following: (a) reduce sunburn and indoor tanning use by 10% among 9th- to 12th-grade students and (b) increase proportion of 9th- to 12th-grade students that use sun protection by 10% (from 9.3% to 11%). The objectives for adults over the age of 18 are similar: (a) reduce sunburn rates by 10% from 37.5% adults reporting one sunburn in the past year to 33.8%, and reduce melanoma deaths by 10% to 2.4 per 100 000 (currently at 2.7 per 100 000) and (b) increase the proportion of people who use at least one sun protection strategy to 73.7% of the US adult population (currently at 67%) and reduce indoor tanning rates by 10% from 5.6% to 3.6%. 3
As evidenced by the Healthy People 2020 objectives, national skin cancer rates are at unacceptably high levels and are continuing to increase, particularly among young adults. Existing skin cancer prevention programs have fallen short, and public health professionals should consider other approaches to reduce risky UV exposure.
Problem Behavior Theory and Multiple Health Behavior Research
Problem behavior theory (PBT), a social psychological framework specific to adolescents and young adults, offers a theoretical foundation that uses the interaction between 3 major systems to explain risk behavior: personality, environment, and behavior. 15 PBT asserts that the 3 major systems are interrelated and provide a social context to describe problem behavior. The theory posits that the social life of young people presents constant opportunities to learn new behaviors and then social expectations reinforce those learned behaviors. 16 Additionally, the risk and problem behaviors cluster because they become part of an individual’s internal validation system, similar to affirmation from parents or acceptance from peers. 16 Jessor further asserted that health risk behavior can develop into “risk behavior syndrome” as a result of the underlying latent variables, and individuals who develop health risk behaviors as young adults will continue to develop more health risk behaviors throughout their lives. 15
Multiple health behavior risk research based in PBT is showing great promise to improve public health in a cost-effective manner by providing a framework to address many clustered health risk behaviors within a single intervention. 17 In fact, the National Institutes of Health and the Robert Wood Johnson Foundation have allocated special funding to study multiple health behavior change for disease prevention and management. One study funded by this initiative found significant improvement when intervening on multiple risky behaviors among ninth graders. The intervention targeted smoking, diet, and sun exposure by employing a home-based technological intervention with parents of high school students. 18 Also, a similar multiple health behavior intervention aimed at lowering cancer risk in the primary care setting focused on smoking, diet, skin cancer, and mammography resulted in significant positive outcomes. 18 Changing multiple health behaviors offers the opportunity to improve quality-of-life outcomes, reduce health care utilization, and save resources by using a bundled health care approach. This is becoming more essential given the likelihood that having multiple health risk factors increases with age. 19 Furthermore, targeting several risk behaviors aligns with the Affordable Care Act’s emphasis on efficient preventative care “bundled” in a clinical setting. 20 Research has shown that prevalence of health risk behaviors increases with age. One study found that only 8.3% of adolescents aged 12 to 13 engage in multiple health risk behaviors, while nearly 33% of 14 to 17 year olds and more than half of college student engage in multiple health risk behaviors, showing a clear increase in clustered risk behavior. 21
The purpose of this article is to present the results of a scoping review of studies that have examined skin cancer prevention and other correlated health risk behaviors.
Materials and Methods
The authors conducted a scoping review of skin cancer risk behaviors and other correlated health risk behaviors. A scoping review methodology was selected to examine the amount of existing research rather than a systematic review that includes a formal quality assessment. 22 Scoping reviews require 5 key steps: (a) a clear research question, (b) identification of relevant studies, (c) selection of studies, (d) creation of a data chart, and (e) organization and reporting of the results. 23
Research Question
This scoping review aimed to answer the following research question: What health risk behaviors are correlated with skin cancer risk behaviors?
Identification of Relevant Studies
The researchers searched online databases in PubMed, PsychINFO, and Science Direct. Search terms included “sunscreen,” “sun protection,” “tanning,” “sun safety,” “skin cancer prevention,” “skin cancer,” “college student,” “young adult,” “health risk behaviors,” “multiple health risk behaviors,” and “correlates.” To yield additional results, specific health risk behaviors salient to college students, including “alcohol,” “sexual behavior,” “smoking,” “texting,” “physical activity,” “exercise,” “drugs,” “substance abuse,” and “mental health,” were searched individually with a combination of the previously noted key words. Titles and abstracts were reviewed for relevance, and then pertinent articles were categorized by sun category (skin cancer risk, sun protection, sun exposure, or indoor tanning) and health risk domain. Reference lists of the relevant articles were cross-referenced, and related sources were examined for inclusion.
Selection of Studies
Final articles for inclusion were selected based on scoping review guidelines; inclusion and exclusion criteria may be based on pertinence rather than study rigor. 22 To be included, studies must have met the following criteria: (a) addressed some form of skin cancer risk, including sunscreen use, sun protection, sun exposure or indoor tanning; and (b) involved correlations with other health risk behaviors. Articles examining attitudinal, cognitive, and other latent constructs were excluded. The researcher scored the article’s relevance to the research question. Fifty-five studies were identified for in-depth consideration. Systematic review articles (n = 4) that included broader tanning correlates or skin cancer interventions but did not specifically address skin cancer prevention and other correlated health risk behaviors were included in the first screen. Their reference lists were reviewed and then crosschecked with the other articles meeting inclusion criteria, and prospective publications were pulled for consideration (n = 3). After further examination, 37 articles were deemed to address some form of skin cancer risk behavior and other behavioral correlates. Only studies written in English and published in peer-reviewed publications between 1994 and 2014 were considered. Figure 1 shows the article screening process.
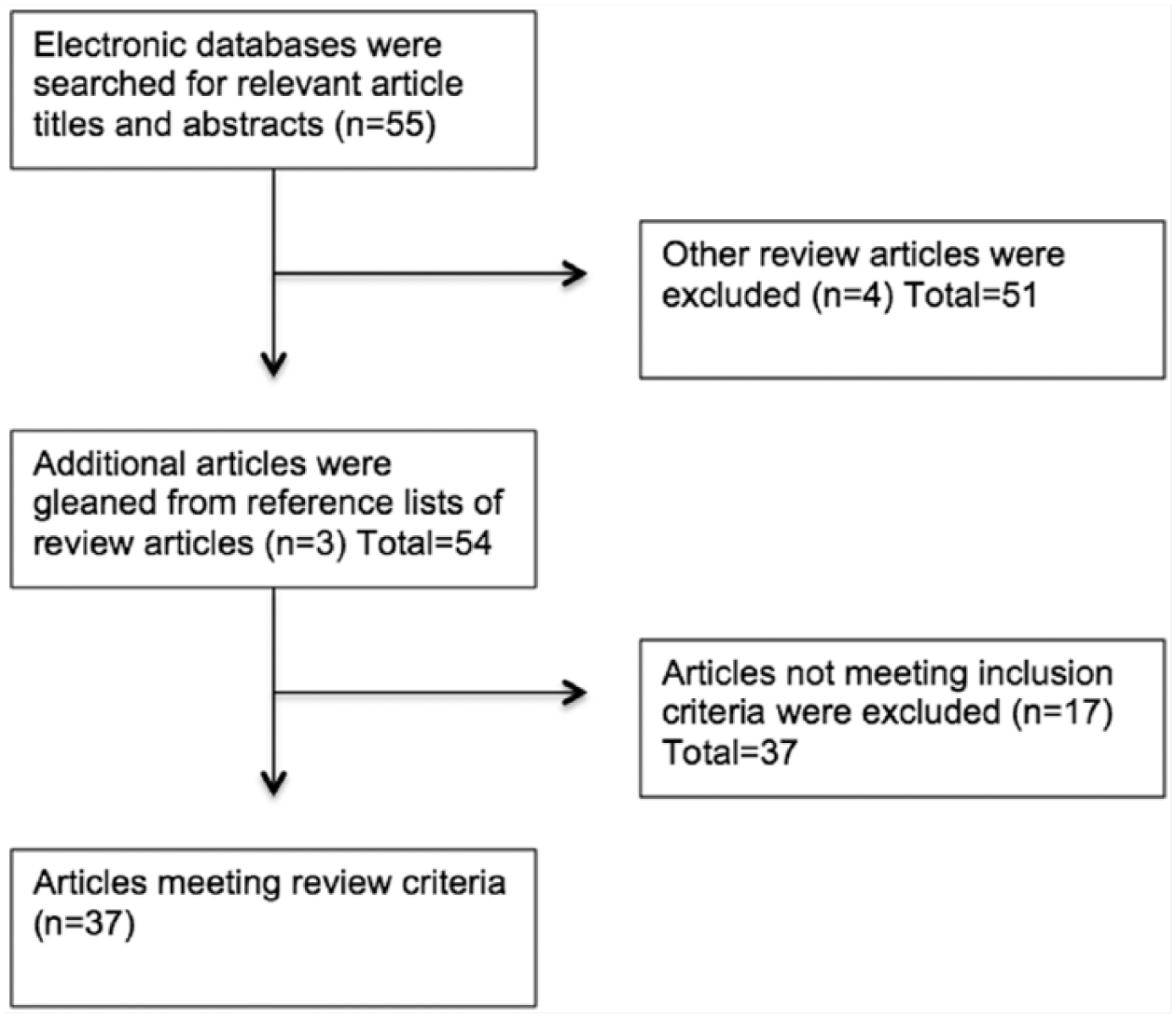
The Screening Process for the Scoping Review of Skin Cancer Prevention Behavioral Correlates Yielded 37 Studies.
Results
The search and screening process yielded 37 peer-reviewed articles examining skin cancer risk and other behavioral correlates. Author information, year of publication, country, study design, participants, sample size, skin cancer risk behavior, and significant findings are documented in Table 1. The studies were primarily quantitative using mostly cross-sectional approaches with some case–control designs. There was a wide range of number of participants in the studies, ranging from 168 individuals to more than 102 000 participants. Ages ranged from 9 to 93 years, with the majority of studies examining adults over the age of 18 (n = 26), adolescents (n = 10), college students (n = 6), and combined adolescents and adults (n = 3).
Skin Cancer Prevention Key Findings.

A majority of the 36 studies that met inclusion criteria were conducted in the United States (n = 26). The remaining studies came from Denmark (n = 3), Australia (n = 2), Canada (n = 2), Sweden (n = 1), the United Kingdom (n = 1), Norway (n = 1), and France (n = 1). The majority of articles included both genders with a greater proportion of female participants, and 2 studies focused exclusively on men. Most of the studies addressed skin cancer risk including NMSC and melanoma (n = 8), indoor tanning (n = 8), both indoor and outdoor tanning (n = 8), and sunburn (n = 6). The other studies covered sunscreen use (n = 5), overall sun protection (n = 4), and tanning dependence (n = 1). Many of the articles addressed multiple correlates of skin cancer prevention behaviors, including physical activity (n = 15), body mass index (BMI; n = 13), smoking (n = 13), alcohol abuse (n = 12), fruit and vegetable consumption (n = 6), drug use (n = 5), sunscreen use—as a correlate of indoor tanning (n = 4), depression (n = 3), unhealthy weight loss (n = 3), seatbelt use (n = 2), suicide (n = 1), steroid use (n = 1), obsessive compulsive disorder (n = 1), drinking and driving (n = 1), riding with someone who has been drinking (n = 1), sexual risk taking (n = 1), and indoor tanning—as a correlate of sunscreen use (n = 1).
Although the findings are mixed and warrant further investigation, current research suggests there is an association between skin cancer prevention behaviors and other health risk behaviors. However, the scoping review revealed that existing studies on skin cancer prevention behaviors and other related health risk behaviors are limited. Specifically, it is notable that the college population has not been studied beyond indoor tanning and tanning dependence.
Physical Activity and Exercise
The relationship between sunburn, NMSC, melanoma, sunscreen use, tanning, and physical activity was broadly studied with mixed findings. Sunburn is a useful metric to gauge skin cancer prevention because sunburn indicates UV overexposure with poor protection and is associated with increased melanoma risk. In fact, those with more than 5 lifetime sunburns double their chance of developing melanoma. 24 Three large-scale cross-sectional studies25-27 revealed that increased levels of physical activity among adults were associated with higher levels of sunburn than those who did not exercise. In Australia, adults that engaged in more than 7 hours per week of exercise were significantly more likely to report sunburn, while adults who exercised were more likely to use sunscreen than their sedentary counterparts. 28 Additionally, adults between the ages of 18 and 29 and between 40 and 49 who engaged in more exercise were more likely to tan indoors. 29 Findings were more complex among adolescents, with lower sunscreen use among sedentary adolescents when compared with their physically active peers. 30 Additionally, physically active girls were less likely to tan indoors than girls that did not exercise, 31 yet high school males that played sports were more likely to tan indoors. 32
Studies examining the relationship between physical activity and skin cancer risk revealed provocative findings. Significantly greater NMSC risk was apparent in physically active men and those who worked outdoors yet not among women.33-35 Interestingly, in adults with a previous history of skin cancer, physical activity rates were higher, yet those with skin cancer had lower sun exposure rates than those with no history of skin cancer. 36 Higher levels of exercise (more than 5 days per week) worked as a protective factor in a case–control examination of melanoma patients with higher levels of exercise. 37 Although these studies did not directly examine coexisting health behaviors, they warrant inclusion because they strengthen the case for additional long-term follow-up studies of the relationship between exercise and skin cancer. However, it will be difficult to establish causality given the lapse of time between UV exposure and the long-term outcome of developing skin cancer.
Body Mass Index
As with physical activity, the relationship between BMI and skin cancer prevention behaviors is complicated but bears compelling findings. Although unhealthy BMI is not a health behavior, rather the result of poor health behaviors, there is strong evidence to suggest a relationship between obesity and a multitude of chronic diseases, including high blood pressure, high cholesterol, diabetes, heart disease, stroke, and some cancers. 38 Specific to skin cancer risk, a higher BMI was not positively associated with melanoma and was inversely associated with NMSC.39,40 Given that NMSC is associated with cumulative sun exposure rather than sunburn, the findings suggest less cumulative exposure among overweight and obese participants. 39 However, another study found an increased risk of melanoma in overweight men, but not the same effects for overweight women when compared with people of normal weight 37 yet Kirkpatrick and colleagues found a great melanoma incidence among overweight women than overweight men. 41 Among farmers in Iowa and North Carolina, a higher BMI was associated with more melanoma risk, 42 and among operating engineers, a higher BMI was associated with more sunburn. 43 In a large-scale national retrospective study, Holman and colleagues found overweight and obese participants were more likely to sunburn than those of normal weight. 25 Furthermore, among high school students, sunscreen use was better among normal weight students than overweight students. 30
The dynamics of BMI and indoor tanning are far more complex because of the underlying appearance motivations and intentionality of indoor tanning. Heckman and colleagues coined the term tanning dependence to describe the addictive nature of indoor and outdoor tanning and found that obese adults were less likely to be tanning dependent than their healthy and overweight peers. 44 One study found adolescents with low BMI were more likely to indoor tan, 31 while another study found that underweight and normal weight girls were more likely to tan outdoors when compared with their overweight and obese peers. 45 However, there were curious age differences in the 2005 US National Health Interview Survey, which found normal weight people between the ages of 30 and 39 tanned indoors more than their overweight and obese peers, yet these findings were not apparent in any other age groups; 18 to 29, 40 to 49, or over age 50. 29
Smoking and Tobacco Use
Among several years of a large-scale national cross-sectional study, adult smokers were far less likely than nonsmokers to use sunscreen27,46 and more likely to sunburn. 47 Similar effects were found internationally: Swedish adult smokers engaged in sunbathing more often than nonsmokers 36 ; women smokers in the United Kingdom were less likely to use sunscreen 48 ; and French adult indoor tanners were more likely to be smokers. 49 Among adolescents, those who smoke were more likely to tan indoors,50-52 sunbathe, 53 not use sunscreen, or engage in any sun protection.30,54 Heckman et al found current smokers to exhibit more signs of tanning dependence than nonsmokers. 44 Indoor tanners between the ages of 18 and 65 29 and college women 55 were more likely to smoke than those who had never tanned indoors.
Alcohol Abuse, Binge Drinking, and Driving Under the Influence
Alcohol use and abuse across the lifespan is positively correlated with high-risk UV exposure. Among adolescents in Connecticut, those who did not use sun protection were more likely to use alcohol, 54 and high school students that reported never using sunscreen were more likely to consume alcohol. 30 In addition, Hall et al found that high school students that did not use sunscreen were also more likely to drink and drive as well as ride with someone who had consumed alcohol. 30 In a US study of more than 28 000 adults, men who consumed more than 15 drinks a week and women who consumed more than 8 drinks a week used less sun protection than those considered low-risk drinkers. 27 Studies on sunburn and alcohol use showed increased sunburn rates among those with higher alcohol consumption25,47 and adults classified as “problem drinkers.” 43 Alcohol consumption was also a variable when comparing individuals with a previous history of skin cancer. Those who reported significantly higher levels of alcohol consumption were more likely to have skin cancer. 36
Indoor tanning behaviors across the lifespan also showed a pattern associated with alcohol consumption and abuse among minors,31,32,50,54 binge drinking among college students,56-58 and problem drinking among adults. 29 Among 12- to 18-year-old females, those who had used an indoor tanning device more than 10 times were more likely to consume alcohol. 50 Demko et al found that white adolescents between the ages of 13 and 19 that used alcohol were also more likely to visit a tanning bed more than 3 times (visiting a tanning bed less than 3 times is considered experimental usage). 31 Patterns were consistent among college-age indoor tanners with those reporting indoor tanning also reporting higher alcohol use 56 and strong associations between college women, indoor tanning, and binge drinking behavior.56,57 Past tanning bed experience was also found to be associated with binge drinking, yet less sun risk behavior. 58 And the behaviors were consistent among US adults between the ages of 18 and 65, with a higher prevalence of indoor tanning among those who engaged in high levels of alcohol use (men who consumed more than 15 drinks a week and women who consumed more than 8 drinks a week). 29
Fruit and Vegetable Consumption and Unhealthy Weight Loss Practices
Fruit and vegetable consumption was low among most respondents in all of the studies given the Dietary Guidelines for Americans set by the Department of Agriculture, which recommended a minimum of 5 servings of fruits and vegetables per day as part of a balanced diet. Few studies included fruit and vegetable consumption, so unhealthy weight loss practices are included in this section given the paucity of research. Among male high school students, indoor tanning was associated with unhealthy weight control practices such as fad dieting yet the same students were more likely to eat 5 or more fruits and vegetables per day than those who did not tan indoors. 32 The association between indoor tanning and unhealthy weight loss methods (laxative use or vomiting) and dieting was also found among adolescent girls.31,50 Girls who did not use sun protection were more likely to be on a diet. 54 Among adults, inadequate daily fruit and vegetable consumption was associated with indoor tanning in the previous year, 29 and better fruit consumption was associated with better sunscreen use. 43
Drug Use
Few studies examined illicit drug use in relation to risky sun behavior. The only study to examine sun protection and drug use found that white adolescents that did not use sun protection were more likely to use marijuana than their peers that used some form of sun protection. 54 Adolescent females that frequently used tanning beds were also more likely to use marijuana.31,50 Finally, college students who met indoor tanning addiction metrics were also more likely to use marijuana. 55
Mental Health
Among adolescents, both boys and girls who never used sun protection were more likely to be depressed than those who used sun protection. 54 Among university students in London, depressive symptoms were associated with poor sunscreen use among women but not among men. 48 In one study of adult engineers, sunburn and symptoms of depression had a positive relationship in bivariate analysis. 43 With regard to indoor tanning, high school boys that used indoor tanning were more likely to attempt suicide. 32 Indoor tanning use among college students was associated with anxiety and obsessive compulsive disorders in men but not among women. 55 College students that were classified as having an addiction to indoor tanning were more likely to report anxiousness, but there were no effects for depression.55,57
Sunscreen
Sunscreen use, sunburn, sunbathing, overall sun protection, and indoor tanning were examined as independent variables in a few studies with counterintuitive findings. In a large study of Danish adults ages 15 to 59, those who sunbathed with the intention of tanning were more likely to use sunscreen than “unintentional” tanners, 59 while adult indoor tanners were more likely to use sunscreen than those who did not tan indoors. 49 These findings were consistent among college students in the United States, with those who had past indoor tanning experience engaged in less risky sun behaviors. 58 When considering tanning dependence, indoor tanning, sunburn, and poor sunscreen use were all associated among university students. 60 However, in a population of beachgoers in Rhode Island, Weinstock and colleagues found those who did not use indoor tanning demonstrated better sun protection behaviors. 61
Discussion
This review uncovered a limited range of existing studies that suggest there is a relationship between skin cancer prevention behaviors and other health risks across the lifespan. The dearth of studies examining skin cancer prevention behaviors other than indoor tanning among college students represents a gap because as adolescents age, they are less likely to use sun protection and clustered risk behaviors increase, making the college age span a critical time for intervention. 17 PBT offers insight to the clustered nature of high-risk behaviors among adolescents by suggesting that latent personality variables enable these behaviors and then environments reinforce them. For instance, sunbathing has been associated with risk-taking, 62 and those who sunbathe and do not use sun protection could have latent issues such as low self-esteem and engage in self-destructive behaviors. 54 Additionally, adolescence is a period of rebellion for some and being healthy might be an unappealing social construct for a defiant teen, particularly if a parent is encouraging healthy behaviors. Substantial research has found clustered problem behavior such as alcohol and drug use, sexual risk taking, and injury risk occur in late adolescence. PBT predicts that these high-risk behaviors are developed to help adolescents “look cool and fit in” with peers. 58 Unfortunately, these habits established in adolescents and young adults might grow into lifestyle behaviors, hence the importance of examining multiple health risk behaviors during the college age span.
Among adults who may have established unhealthy behaviors in their youth such as smoking, drinking, and drug use but have moved past the social norms to fit in, poor health behaviors may have already become an addiction or habit. Specifically, recent studies have examined the addictive nature of tanning and people might become tanning dependent just as those who are nicotine dependent. 60 Tanning addiction shares some characteristics with nicotine addiction in that those with a tanning addiction have a fear of quitting tanning and experience withdrawal symptoms when they are unable to regularly tan. 60 Smoking is often associated with a myriad of other health risk behaviors including alcohol abuse, 63 low rates of exercise, 64 and poor diet. 65
Smoking is widely known as the leading preventable cause of death and disease and is responsible for 90% of lung cancers and more than 80% of chronic obstructive pulmonary disease deaths in the United States. 66 From the public health perspective, smoking shares some parallels with UV exposure because there is clear evidence of the causal relationship between smoking and lung cancer, similar to the link between UV exposure and skin cancer. Despite the widespread public awareness of the relationship, people continue to engage in these high-risk behaviors. This paradox suggests that smokers are not concerned about long-term health outcomes nor are those who deliberately engage in high-risk skin cancer behaviors.
Consistent with PBT’s premise that underlying personality issues drive clustered health risk behaviors, the self-presentation (appearance) concerns related to physical activity, BMI, dieting, and substance abuse help explain the relationship with skin cancer prevention behaviors. Personal appearance motivations and the belief that being tan enhances appearance are among the strongest latent predictors of engaging in risky tanning behaviors. 67 Other research has found correlates between self-presentation concerns and risky healthy behaviors, across a spectrum of behaviors including condom use, drug and alcohol use, and physical activity. 67 When people are most concerned about what others think of them, rather than their own self-view, they are more likely to engage in risky health behaviors. 67 People with high self-presentation concerns tend to be high social monitors, publicly self-aware, and hyperconscious about their physical appearance.
The relationship between indoor tanning, weight, and dieting is supported by the literature, suggesting the link between indoor tanning and appearance concerns. In line with self-impression concerns, many health risk behaviors including smoking, marijuana use, and alcohol also cluster with indoor tanning. The clustered relationship is speculated to be a result of peer and mass media influences that promote a thin, tanned person engaging in “fun” activities such as social drinking, smoking, and glamourized drug use.
The findings between physical activity and skin cancer present a potential conflict that public health practitioners must carefully navigate. Regular exercise is a known protective factor against a host of chronic diseases including high blood pressure, diabetes, heart attack, stroke, cancer, arthritis, and symptoms of depression and anxiety. 68 However, as evidenced by the findings and simple logic, sun protection and outdoor physical activity are at odds with each other because to be outside jogging or playing sports, one is likely exposed to the sun, with only sunscreen as a defense strategy. People who exercise outdoors would be at higher risk for NMSC, which is due to cumulative sun exposure rather than acute. More physically active people might be outdoors and exposed to more UV radiation than sedentary people; therefore, sun safety campaigns should be careful to not discourage outdoor physical activity but rather encourage good sun protection strategies such as avoiding peak sun hours and the use of sun protective clothing, and proper sunscreen application. For instance, a study of college athletes found that nearly 80% of NCAA track athletes did not wear sunscreen in the week prior to the study. 69 However, more precise studies are needed because most of the existing studies do not differentiate between indoor and outdoor exercise and is complicating the exact relationship between physical activity and skin cancer.
Although BMI is not a literal health behavior, it is frequently used as a behavioral correlate in health behavior research to illustrate physical activity and diet constructs given the causal impact on weight. Overweight and obesity rates have been steadily increasing over the past 20 years, 70 and the relationship with skin cancer risk is seemingly inconsistent but there is an underlying logic to the findings. People who are overweight or obese may not be in the sun as consistently as those with a normal BMI, but when they do go in the sun, they are more likely to burn because they have not been in the sun and they have larger surface areas to protect. 25 These findings follow the logic that overweight and obese people might not want to expose their bodies publicly during outdoor activities such as exercise or sunbathing; therefore, they have less sun exposure. Appearance concerns are particularly salient among adolescents with underweight and normal weight teens engaging in more sun exposure than their overweight counterparts. However, indoor tanning bed use was the same between groups, suggesting overweight teens might not want to be seen sun bathing. Body dissatisfaction emerged as an important theme and is often linked to other risky behaviors including disordered eating. 71
There is a significant gap in the scientific literature examining multiple health risk factors related to risky UV exposure during the pivotal college experience. National skin cancer rates are at unacceptably high levels and are continuing to increase particularly among young adults. As discussed, the harmful effects of skin cancer could mostly be avoided with simple sun protection strategies and the avoidance of indoor tanning. Unfortunately, college students are not taking the advice of their parents and public health campaigns to use sunscreen and avoid tanning beds. It should be noted that the indoor tanning industry spends millions of dollars every year to promote the idea that indoor tanning is a safer alternative to natural sun exposure, which undoubtedly furthers confusion. 72 Mass media public health campaigns have made great strides in increasing awareness of the link between UV exposure and skin cancer, yet these efforts have not improved behaviors. There are limited theoretically based skin cancer prevention interventions for the college population. In fact, many of the existing UV education interventions focus on indoor tanning and the constructs are salient to appearance motivations rather than broader sun safety behaviors. Indoor tanning is an important area of inquiry; however, overall sun safety education, specifically sunscreen use, affects a greater proportion of college students and the general population.
Thus, given the prevalence of inadequate sun protection and increasing skin cancer rates, the early identification of college students at risk for engaging in multiple health risk behaviors is important for public health practitioners in several ways. First, existing interventions can be improved by targeting the clustered health behaviors rather than delivering a variety of disjointed health programs. Second, helping college students establish a constellation of healthy behavioral habits at a young age can have lifelong health benefits. Finally, the improved quality of life gains by establishing healthy behaviors at a young age can reduce overall health care system expenditures.
Study Limitations
There are expected limitations given the depth and breadth of studies included. These limitations should be considered when evaluating the findings. Many of the studies relied on cross-sectional data to analyze multiple health risk correlates. Beyond self-selection and self-report bias intrinsic in cross-sectional studies, 73 the approach is limited in the ability to provide insight on the specific reasons for engaging in these behaviors. Specifically, the latent variables that drive health behavior and this area of study would benefit from more qualitative studies to illuminate the underlying characteristics associated with poor skin cancer prevention behavioral correlates. Although risky tanning and appearance motivations have been extensively studied, the inclusion of multiple health behaviors is relatively novel and would benefit from the richness of context that observational, focus groups, and open-ended interview studies provide. Also, large-scale data sets often lag behind emerging health trends. For instance, texting while driving became a serious public health threat several years before questions were added to national instruments. Additionally, some of the retrospective designs did not use standardized skin cancer prevention questions, which limits comparison of findings with other studies. There was also a noticeable absence of longitudinal studies to better understand health behavior trends. Furthermore, many of the studies used different terminology, referring to skin cancer prevention behaviors including sun exposure, sun protection, and indoor tanning, which further complicate the ability to generalize and compare findings. Future studies would benefit from using a validated instrument such as the standard National Cancer Institute’s core skin cancer prevention questionnaire. 74 Even when using gold standard measurements, it should be noted that precise measurement of proper use of sun protective behaviors is difficult to assess because there are nuances to sunscreen application including amount of sunscreen used per application and frequency of reapplication.
Footnotes
Acknowledgements
The authors wish to thank Amanda Jeter for her excellent editorial assistance.
Authors’ Note
The study received institutional review board approval at the University of North Florida (#10-125).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.