
Abstract
Sports injuries are a significant clinical and public health concern. There is a growing call to improve the translation of available evidence-based and expert-informed sports injury prevention interventions into sustained use in practice by physicians and others (eg, athletic trainers, coaches, and parents) who care for injured athletes. This article provides a brief overview of the current sport injury prevention implementation literature before focusing specifically on the translation of guidelines (including consensus and position statements) developed to assist physicians and others diagnose and manage athletes with sport-related concussion and the associated return-to-play decisions. The outcomes of more than 20 published studies indicate that physician, athletic trainer, coach, parent, and athlete knowledge, use of, and compliance with sport-related concussion guidelines are limited. More concerted, coordinated, and theory-informed efforts are required to facilitate the widespread dissemination, translation, and implementation of such guidelines. An example is provided of how implementation drivers could be used to inform the development of a comprehensive, multilevel implementation strategy targeting the individual, organizational, and system-level changes necessary to support the translation of available sport-related concussion guidelines in both the clinical and sports settings.
‘. . . effective implementation strategies are needed to complement existing evidence-based interventions in order to significantly reduce the incidence and severity of sports-related injuries.’
While regular participation in sport and physical activity confers health benefits, 1 injuries sustained during this activity can pose significant public health and clinical problems.2,3 Sports injuries are a common4,5 and costly6,7 barrier to ongoing participation in physical activity8,9 and a concern for parents of young participants. 10 As such, the prevention of sport-related injuries should be a priority for physicians, scientists, and sports administrators alike.11,12
The Need for Better Implementation
The evidence-base concerning what works to prevent many common sports-related injuries is large and growing.13-17 However, the translation of this evidence into widespread use is lagging. 18 Two recent reviews of sports injury prevention interventions have articulated the importance of focusing attention on disseminating and implementing efficacious interventions in order to make a significant impact on the public health burden of sports injuries.13,15 Effectively undertaking such knowledge dissemination and translation activities requires an understanding of the implementation setting (context, culture, and capacity), the translation of what is already known into formats (guidelines, programs, resources, policies, etc) that can be accessed and used by target audiences, and the development and operationalization of effective implementation plans.19-21
Despite the importance of implementation activities to maximizing the public health outcomes of sports injury prevention research, historically, little emphasis has been placed on exploring ways to facilitate the implementation of interventions in real-world contexts.22-24 This began to change in the mid to late 2000s, particularly in terms of research exploring how best to maximize intervention uptake among target audiences.20,22,25 The outputs of this research can be grouped into 3 broad categories:
Editorials, commentaries, and study protocols either calling for more and better implementation research or outlining how such research is being, or could be, conducted.18,21,26 -36 This body of work has been underpinned by frameworks and theories from health promotion,37-39 behavioral science,40,41 and more recently, implementation science.26,42,43
Frameworks to guide efforts to translate knowledge and implement sports injury prevention interventions.19,20,26,44-47
Descriptions and evaluations of implementation efforts48-52 and plans.53,54 This work includes identifying factors that influence implementation activities and outcomes55-59 as well as assessing whether physicians, athletes, and coaches know about, or adhere to sports injury prevention interventions, recommendations and guidelines across a range of sports and settings.57,60 -86
Several common themes have emerged from this body of literature. First, there is now general acknowledgment that effective implementation strategies are needed to complement existing evidence-based interventions in order to significantly reduce the incidence and severity of sports-related injuries. Second, encouraging medical personnel (family, emergency and sports physicians, and athletic trainers)66,67,78-80,87 and sports participants (athletes and coaches) † to comply with or use evidence-base injury prevention interventions, guidelines, and regulations can be challenging. Finally, the implementation of sports injury prevention interventions could benefit significantly from what is already known and applied in the fields of health promotion, behavioral science, and implementation science. ‡ This point is particularly pertinent with respect to the need to do more than just educate or disseminate information about evidence-based interventions among physicians, coaches, and athletes. 94
Although there is a clear need to improve the translation of evidence-based injury prevention interventions into sustained practice across all injury issues and sporting contexts, the remainder of this paper will focus specifically on the translation of diagnosis, management, and return-to-play guidelines for sport-related concussion into practice among physicians and those involved in sport. Guidelines can be a useful tool for improving the consistency and efficiency of care and for closing the gap between clinical practice and what the scientific evidence supports.95-97 As such, consistent use of guidelines has the potential to improve the quality of patient care, reduce the risk of medical negligence, and be cost effective for the healthcare system.95,96 However, it should be kept in mind that a lack of knowledge or use of available guidelines is not necessarily an indication of poor or inappropriate clinical care.
Enhancing the Use of, and Compliance With, Sport-Related Concussion Diagnosis, Management, and Return-to-Play Guidelines
Sport-related concussion is a major public health and clinical concern, 98 with an estimated 1.6 million to 3.8 million sports-related traumatic brain injuries (including those who do, and do not, seek medical attention) each year in the United States. 99 However, these figures may underestimate the true incidence by 6 to 10 times because sport-related concussion is often unrecognized by athletes and is often not reported to doctors. 100
Family physicians are important carers of concussed athletes67,80,101 and disseminators of concussion knowledge,68,102 and multiple clinical guidelines, consensus and position statements (hereafter collectively referred to as guidelines) are available to help them make concussion-related diagnostic, management, and return-to-play decisions. For example, it has been estimated that more than 25 sport-related concussion severity grading scales were available in 2001 103 and that approximately 20 concussion management guidelines were published in the 2 decades prior to 2009. 104 New or updated guidelines continue to emerge to reflect developments in the scientific literature, with the American Medical Society for Sports Medicine, 105 the American Academy of Neurology, 106 and the Concussion in Sport Group (CISG) 107 each publishing new or updated concussion guidelines or position statements in 2013.
Over the past decade, 4 CISG meetings have been held to reach consensus about the understanding and management of concussion in sport.107-110 At the 2001 meeting in Vienna, concussion was defined and it was recommended that concussion management strategies be based on an individualized, objective assessment of clinical and cognitive recovery postinjury. 108 From 2001 onward, the CISG stressed that all concussions should be assessed by a medical doctor both at the time of injury and when considering returning-to-play. One of the outcomes of the 2004 Prague CISG meeting was the development of a standardized concussion assessment tool (the SCAT) to help medical personnel diagnose, assess, and manage concussions. A concussion “rehabilitation” protocol was also introduced for a graded return-to-play program. 109 From 2004, it was also recommended that no concussed athlete should return to their sport on the day of injury, although considerations pertaining to the particular circumstances of professional sport were elaborated. At the 2008 meeting, the SCAT2 was further developed to reflect research highlighting the importance of assessing balance and conducting more detailed screening of brain function. In addition, a sideline version of the SCAT2 was developed to help lay people identify concussions on the field of play. These tools were further modified based on published research and testing at the 2013 meeting, and the SCAT3, Child SCAT3, and Concussion Recognition Tool were subsequently produced. 107
This proliferation of published guidelines has been matched by, and often used to inform, the development of fact sheets, position statements, policies, and guidelines developed by government agencies (eg, US Centers for Disease Control and Prevention http://www.cdc.gov/concussion/sports/index.html), professional associations (eg, College of Family Physicians of Canada http://www.cfpc.ca/uploadedFiles/Health_Policy/_PDFs/Position_Statement_Concussions_Approved%20Feb2012_ENG.pdf), and national and international sports governing bodies. In addition, 49 US states now have legislation governing the management of concussion in sport. These laws generally focus on (a) educating coaches, parents, and athletes about concussion and (b) medically assessing the concussed athlete.111,112
To complement the profusion of concussion guidelines, research has explored whether physicians and others who treat patients with sports-related concussion are aware of these guidelines, have used them in their practice, or whether their practice is in line with guideline recommendations. Early investigations found mixed results across a variety of settings and target groups. For example, only 30% of patients from the Children’s Hospital of Alabama received discharge instructions consistent with those recommended in Cantu’s 1986 guidelines 113 following a diagnosis of a sports-related closed head injury. 114 More positive findings were reported by Ferrara et al, 115 with around 82% of attendees at a concussion-specific mini-course at the 1999 National Athletic Trainers’ Association Annual Meeting and Clinical Symposia reporting using a concussion grading scale. However, only 19% reported using some form of return-to-play guidelines. 115
Equivalent lines of research have been conducted among athletes. Only half of the players from teams participating in the 2000 New Zealand national schools rugby union competition were aware of the International Rugby Board (IRB) concussion guidelines that applied to them, and only 60% correctly identified the IRB-mandated 3-week stand down period following a concussion. 116 This is despite the fact that this stand down period has been a law of the game since 1968. Furthermore, of the 62% who suspected that they had been concussed, just more than half reported their suspicions to a doctor or sports (first aid) medic, more than half made their own return-to-play decision, and only 22% received medical clearance before returning to play. 116 A similar lack of compliance with return-to-play regulations following concussion was identified more recently among Australian schoolboy and community rugby union players. 62
A search of the PubMed, Scopus (Elsevier), SPORTDiscus (EBSCO), and Google Scholar databases (using the terms sport AND concussion AND guideline) (1980-2013 inclusive) identified that, since this early research, more than 20 studies examining knowledge of, or compliance with, concussion guidelines have been published in the peer-review scientific literature. This search identified studies that were predominately cross-sectional in nature, investigated guideline knowledge and compliance among a range of stakeholders, including physicians, athletic trainers, coaches, athletes, and parents across a variety of sports. A summary of these studies appears in Table 1.
Summary of Studies of the Knowledge of, and Compliance With, Concussion Diagnosis, Management and Return-to-Play (RTP) Guidelines Among Physicians, Others Who Provide Medical Services in Sports Settings, and Sports Coaches, Athletes, and Parents.

Abbreviations: CMSG = Colorado Medical Society Guidelines; AAN = American Academy of Neurology; NATA = National Athletic Trainers Association; CISG = Concussion in Sport Group; CDC = Centers for Disease Control and Prevention; IRB = International Rugby Board; DNS = date not specified; RTP = return-to-play; CME = continuing medical education.
These data have not been published previously and so are included in full here.
Although most of the published research investigating physician knowledge and use of concussion guidelines has been conducted in North America, it appears that the lack of knowledge, and use, of readily available sport-related concussion guidelines is not restricted to this region. For example, a 2013 study of club medical officers for English League football (soccer) teams identified that more than 25% had not heard of the 2008 CISG consensus statement and more than 50% did not routinely follow the guidelines in spite of the dissemination of information about these guidelines by the Fédération Internationale de Football Association (FIFA), the international governing body in this sport. 78
In 2013, the authors of this review conducted an online survey of a small sample (n = 37) of Australian general practitioners (family physicians) and the main findings are also summarized in Table 1. Although 84% of the responding physicians had diagnosed and/or managed patients with a sport-related concussion (51% in the previous 12 months), 46% were not aware of any specific guidelines for the diagnosis and/or management of sport-related concussion. Of those who were aware of such guidelines, 40% reported that they were aware of the Sports Medicine Australia (Australia’s peak national umbrella body for sports medicine and sports science) Smartplay guidelines, 25% were aware of one or more of the CISG consensus statements, and 5% each were aware of the American Medical Society for Sports Medicine position statement on concussion in sport and the Australian Football League concussion guidelines.
Athletes, parents, and coaches have also been shown to have deficiencies in their concussion knowledge and return-to-play behaviors. § What is particularly concerning from a physician’s perspective is that these findings highlight that providing coaches and parents with information about sport-related concussion is not enough to change athletes’ return-to-play behavior. This is demonstrated by the discrepancy between coaches’ and parents’ knowledge about what they should do if confronted with a return-to-play decision for a concussed athlete or child,68,102,123 and what athletes and injury surveillance reports indicate actually happens.62,69,116
Despite repeated calls for greater investment in translating the available guidelines into improvements in the diagnosis and management of sports-related concussion, ‖ considerable work remains to be done. This situation is not unique to sport-related concussion guidelines. A 2011 systematic review of physicians’ use of a broad range of clinical guidelines identified that, although awareness of guidelines was high (90%), the median proportion of respondents who reported adhering to guideline recommendations was 36% (interquartile range 35% to 56%), with similar proportions of “leakage” (around 15%) between each of the 4 stages from guideline awareness to agreement, adoption, and adherence. 96 In addition, a 2010 systematic review of the effectiveness and efficiency of a wide range of clinical guideline dissemination and implementation strategies indicated that most guideline implementation research is not informed by cognitive, behavioral, or organizational theory 127 and the majority of interventions were associated with modest to moderate improvements in care at best. 128
Although some evaluations of sport-related concussion education initiatives with sports coaches have been published recently,52,129,130 to date there have been no coordinated, well-planned or theory-informed efforts to disseminate or implement sport-related concussion guidelines with physicians. 33 There have, however, been recent discussions about the potential application of knowledge transfer34,35 and social marketing principles 33 and the use of social media platforms such as Facebook and Twitter33,131 to enhance the translation of concussion guidelines into changes in practice among physicians and others involved in sport. Interestingly, nearly all the discussion around increasing the uptake and use of concussion guidelines has focused exclusively on improving or increasing education of physicians, sports coaches, and athletes34,105,107 or embracing new and popular electronic communication channels to better disseminate available guidelines.33,101 Although efforts in these areas are undoubtedly needed, the widespread dissemination of guidelines has been shown to have limited effect on changing physician behaviour.95,132,133 There is also considerable evidence in the broader field of implementation science that having access to information, guidelines, policies, education, and training alone are generally ineffective implementation methods, and that longer term multilevel implementation strategies targeting individual, organizational, and system-level changes are usually more effective. 94
Using Implementation Science to Drive Sport-Related Concussion Guideline Use and Compliance
Implementation science is “the study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice.” 134 It is a growing field that draws on evidence from a wide range of disciplines94,135 and has implications for everyone interested in bridging the gap between research and practice, 136 including in the field of sports injury prevention. 26 Several models and frameworks outlining productive implementation strategies have emerged,137-139 but concern has been expressed that such models are often too complex, academic, or time-consuming for physicians and practitioners to use. 140
One conceptual framework that has emerged from the implementation science literature, and which may be potentially useful for informing future implementation efforts in the context of sport injury prevention, is the notion of implementation drivers developed at the National Implementation Research Network.26,43 These drivers are based on the common elements of successful implementation programs (including in the field of clinical guidelines) 94 and can be used to leverage improved practitioner competence, and to create more supportive organizational systems and environments for the implementation of new programs, practices, policies, and guidelines. Implementation drivers are independent of the quality of the intervention being implemented 141 and can be broadly classified into 3 categories. Competency drivers reflect the capacity of staff or practitioners (eg, physicians, coaches, athletic trainers) to effectively implement the intervention, while organizational drivers focus on the organizational processes necessary to facilitate intervention implementation. Finally, leadership drivers promote implementation at the start of the process and provide ongoing technical expertise to manage and embed the continued implementation of new initiatives. These drivers work together and can compensate for each other to encourage and support the widespread, high-fidelity implementation of new interventions across settings. These implementation drivers provide a useful starting point for guiding efforts to enhance physician and sports-sector knowledge of, and compliance with, readily available sport-related concussion guidelines.
Table 2 provides a detailed description of how these implementation drivers could be applied to enhance the use of sport-related concussion guidelines in clinical and sports settings. Developing and operationalizing strategies that target each of these implementation drivers should, in principle, help to maximize the likelihood that those in clinical and sports settings responsible for diagnosing, managing, and making return-to-play decisions about concussed athletes are knowledgeable about, and skilled in the use of, recommended sport-related concussion guidelines. These strategies are also likely to create environments (eg, supportive systems, policies, procedures, and leaders) that encourage and assist physicians and sports personnel in their guideline implementation efforts.
Example of how the Implementation Drivers Could Be Applied to Enhance the Use of Sport-Related Concussion Guidelines in Clinical and Sports Settings.
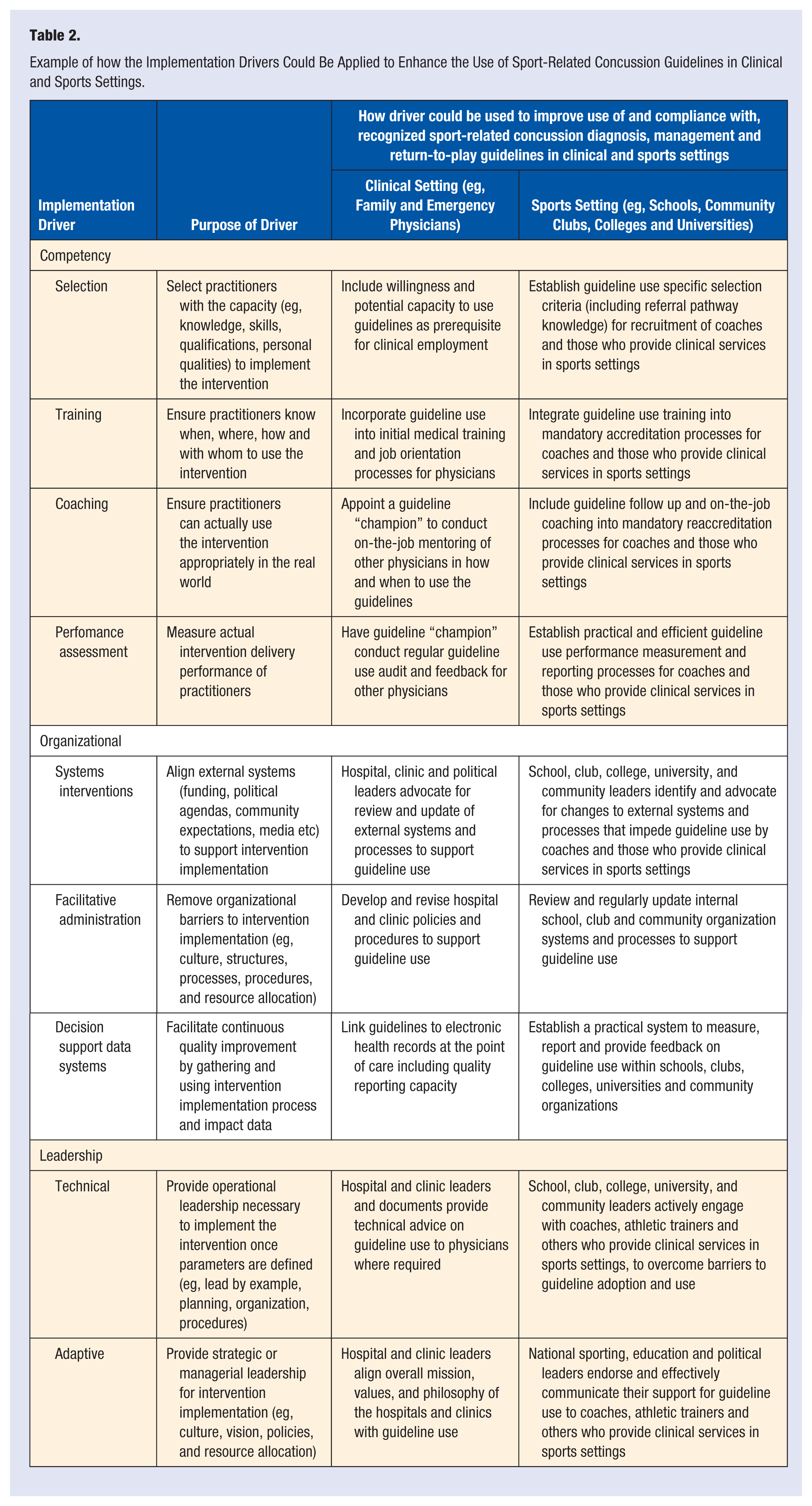
In addition to informing the development of strategies to facilitate the use of available concussion guidelines among physicians and those involved in the sports sector, physicians themselves could also use these implementation drivers to guide their efforts to encourage and support individual patients to comply with concussion-related advice. For example, physicians could step outside their clinics and begin to work in partnership with their local communities (sporting clubs, schools, or community groups) to address the issue of the appropriate diagnosis, management and return-to-play of concussed athletes. This could include providing information, education, training, and mentoring to local sports coaches and athletic trainers about the available concussion guidelines, including when and how to use them. Physicians could also work with local club and school/college sports administrators to develop effective policies, systems, and procedures that encourage and support athletic trainers, coaches, athletes, and parents to follow the diagnosis, management, and return-to-play advice contained in the concussion guidelines. Finally, physicians could provide leadership, perhaps at a regional administrative rather than individual club or school level, to drive the cultural change that may be required to initiate and sustain the use of, and compliance with, available guidelines within their communities.
Conclusion
Sports injuries are a significant public health and clinical concern. A range of evidence-based interventions and guidelines are available to assist physicians and others who care for injured athletes, and research attention has begun to focus more on the translation of these interventions into routine practice. For example, guidelines to aid in the diagnosis and management of sport-related concussion and related return-to-sport decisions have been publicly available in various forms since at least 1986. 113 Yet, as the research summarized in Table 1 of this review strongly indicates, physicians (including family and emergency physicians) and others who care for athletes with sport-related concussion (athletic trainers, coaches and parents) do not routinely know about, use, or comply with such guidelines. Although there has been some recent discussion about the use of knowledge translation theory and social media platforms, there have been no well-planned or coordinated efforts to enhance the knowledge or use of sport-related concussion guidelines among physicians.
Implementation science is a growing field of research that offers the potential to inform the development of targeted and effective strategies to enhance the use of, and compliance with, readily available guidelines among those responsible for diagnosing and managing sport-related concussion. In particular, a multilevel focus on improving competency in the use of such guidelines among all those who care for concussed athletes, developing organizational systems and procedures that encourage and support guideline use, and providing technical and cultural leadership offer significant opportunities to enhance the translation of evidence into practice in this important area of sports medicine.
Footnotes
Acknowledgements
The research with Australian general practitioners presented in this article was part of the work undertaken for a Victorian Sports Injury Prevention Research Grant from the Department of Planning and Community Development, Victoria, Australia. That project’s larger chief investigator team included all co-authors of this paper as well as Angela Clapperton, Willem Meeuwisse, Michael Ewing, John Sullivan, Hugh Seward, and Carolyn Emery. PW’s salary was paid from this grant. CFF was supported by a National Health & Medical Research Council (NHMRC) Principal Research Fellowship (ID: 565900). PM is supported by a NHMRC Practitioner Fellowship. AD’s salary was supported by an NHMRCH Partnership Project Grant (ID: 565907). The Florey Institute of Neuroscience and Mental Health acknowledges support from the Victorian Government, in particular the funding from the Operational Infrastructure Support Grant. The funding agencies were not involved in the collection, analysis, or interpretation of data, nor was it involved in any decisions regarding the publication of data. The Australian Centre for Research into Injury in Sport and its Prevention (ACRISP) is one of four international research centers that are supported through the International Olympic Committee’s Medical Research Network. The authors would like to thank David Sleet for his insightful feedback on early drafts of this article.