
Abstract
An understanding of the environmental factors that contribute to injury risk will allow for the optimization of athletic performance and minimize morbidity. The purpose of this review is to discuss the physical and social environments of sport that affect injury risk, and to review the strategies that sports medicine professionals (eg, clinicians, certified athletic trainers) can implement to prevent injury. Searches using the PubMed, Cochrane, and Google Scholar databases were used to identify injury risk factors pertaining to the physical and social environment of athletics. Physical environmental risk factors identified include weather, air quality, playing surface, and the presence of sports medicine professionals. Social environmental factors include parents, teammates, coaches, media, policy/legislation, and sports medicine professionals. Sports medicine professionals seeking effective prevention and care strategies will benefit from (1) education about the physical and social environmental risk factors that place athletes at risk for injury and (2) a holistic approach that recognizes that physical and social factors are as important as individual risk factors in determining injury risk.
Introduction
Participation in organized sports is at its highest recorded levels. Estimates from the 2010 Sporting Goods Manufacturers suggest that 50% of all US residents older than 6 years are “frequent” sports participants, and 27% are active on a “regular” or “casual” basis. 1 Currently, more than 40 million children and youth participate in sports, 2 including those outside of the school setting, such as club sports, gymnastics, and swimming. In the 2010-2011 school year, there were approximately 7.7 million high school varsity and junior varsity student-athletes in the United States. 3
Insight into environmental risk factors, as well as interventions that may mitigate injury, will improve quality of life for athletes, optimize athletic performance, and minimize morbidity and disability from sports injuries.
Although increased sports participation indicates a positive trend in physical activity levels, it harbors a negative consequence in terms of increases in the absolute numbers of sports-related injury. At the same time, the climate of sports has changed, because of the escalation in the demands placed on youth athletes; increased duration and intensity of training; the presence of year-round training; early sports specialization; high numbers of repetition of specific sport skills; elevated difficulty of skills practiced; heightened interest in recreational activities in the wilderness; and increased participation in “extreme sports” such as skateboarding, BMX, mountain biking, and rock climbing.4-7 Also, the mind-set among some athletes may be to constantly push their bodies in an effort to optimize performance, sometimes ignoring warning signs of pain and overuse from their bodies. More severe injuries can disrupt athletes’ quality of life in the short and long term, by negatively affecting their health and causing them to miss a large part, if not all, of their playing season. 8 Severe injuries are also more likely to require surgery and other advanced medical treatments, and increase the burden on the health care system. 8 Identification of risk factors for sports injury, when used to inform the design and implementation of preventive measures, has the potential to mitigate these negative trends.
The epidemiologic triangle of 3 primary factors—host, agent, and environment—has been extensively used to describe the epidemiology of various outcomes affecting human morbidity and mortality. When applied to sports injury (Figure 1, adapted from Weaver et al 9 ), the epidemiologic triangle consists of the athlete as the host, the energy that causes injury as the agent, and the physical environments in which the athlete exists (eg, weight room, athletic field, playing surface). The concentric circles in Figure 1 signify that multiple social environments (eg, sports team, classroom, family, peer group, fans) exist within the physical environment and contribute to the energy vectors. Runyan 10 provides further details of the adaption of the epidemiologic triangle to injury and the representation of the multiple social environments that surround the athlete.
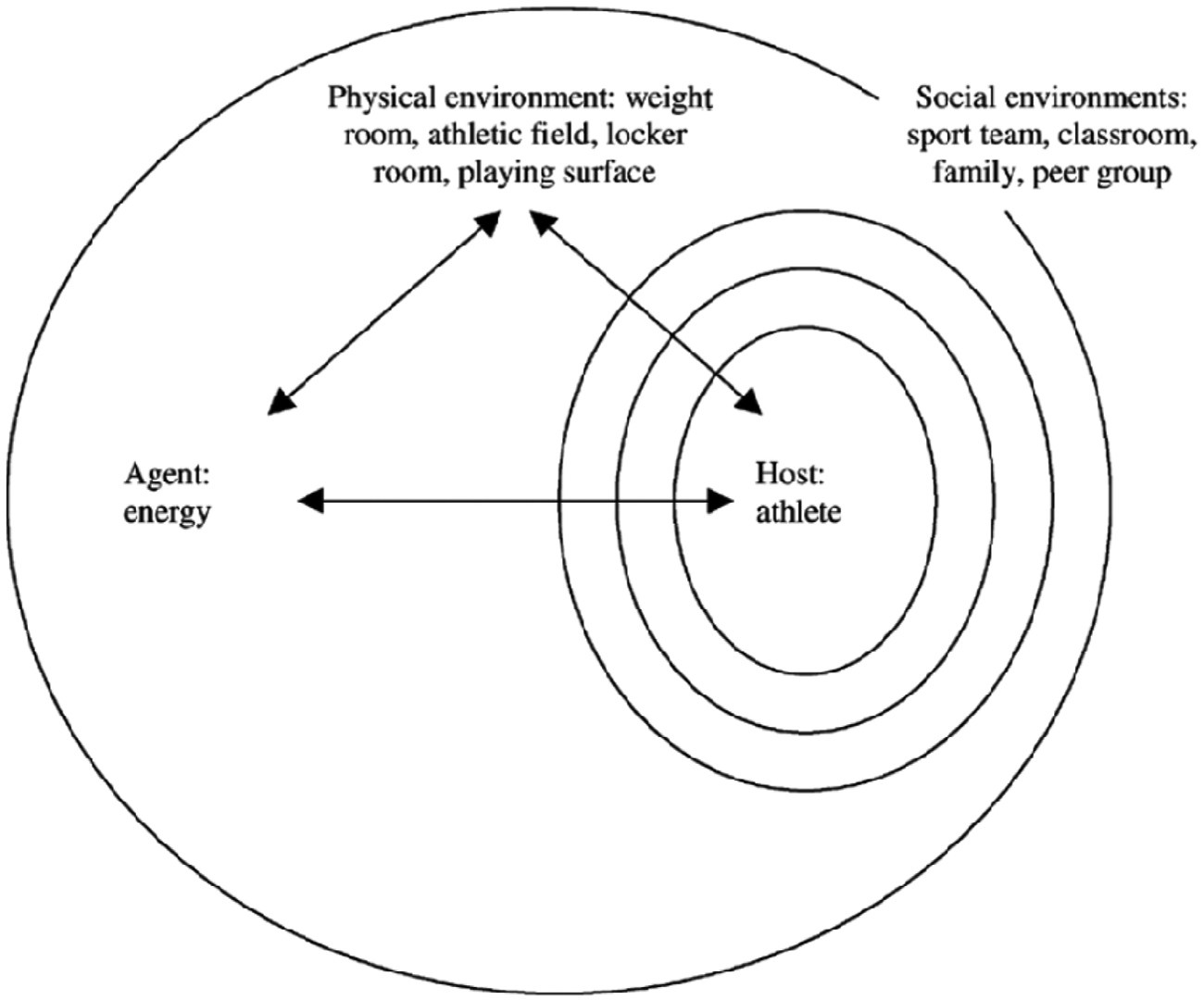
The public health framework applied to sports injury (adapted from Weaver et al, 2002) 9 .
The complexities of environmental factors and interventions have recently begun to receive attention from sports injury practitioners and researchers in the past decade.11-13 It is important to summarize and disseminate our existing body of knowledge in this area so that sports medicine professionals such as primary care physicians and certified athletic trainers can apply research findings to their practice. The purpose of this review is to discuss how the physical and social environments affect sports injury risk and to discuss strategies that sports medicine professionals can implement to reduce injury risk. Insight into environmental risk factors, as well as interventions that may mitigate injury, will improve quality of life for athletes, optimize athletic performance, and minimize morbidity and disability from sports injuries.
Methods
We identified environmental factors through extensive searches on PubMed, Cochrane, and Google Scholar through December 15, 2011. The first author (ZYK) conducted the literature search by first searching the databases with the keywords: “sports,” “injury,” “risk,” “physical environment,” and “social environment.” The first search produced a number of themes related to the physical environment, which we defined a priori as pertaining to the natural environment (eg, weather, temperature, playing conditions), and the social environment, which we defined a priori as pertaining to the influences those involved in sports such as peers, parents, and coaches.
The first author, with assistance from the second author (KGR), then conducted additional searches with new keywords based on specific themes that were found during the literature review. For example, for heat injury, we used search terms such as “heat injury,” “heat trauma,” “heat illness,” “heat exhaustion” “high humidity,” and “hot weather.” The literature was then reviewed by the third and fourth authors (JDS, SWM), who helped to fill in literature gaps where applicable. The various findings, prevention strategies, and current controversies pertaining to sports injury and the environment are discussed in detail.
The Physical Environment
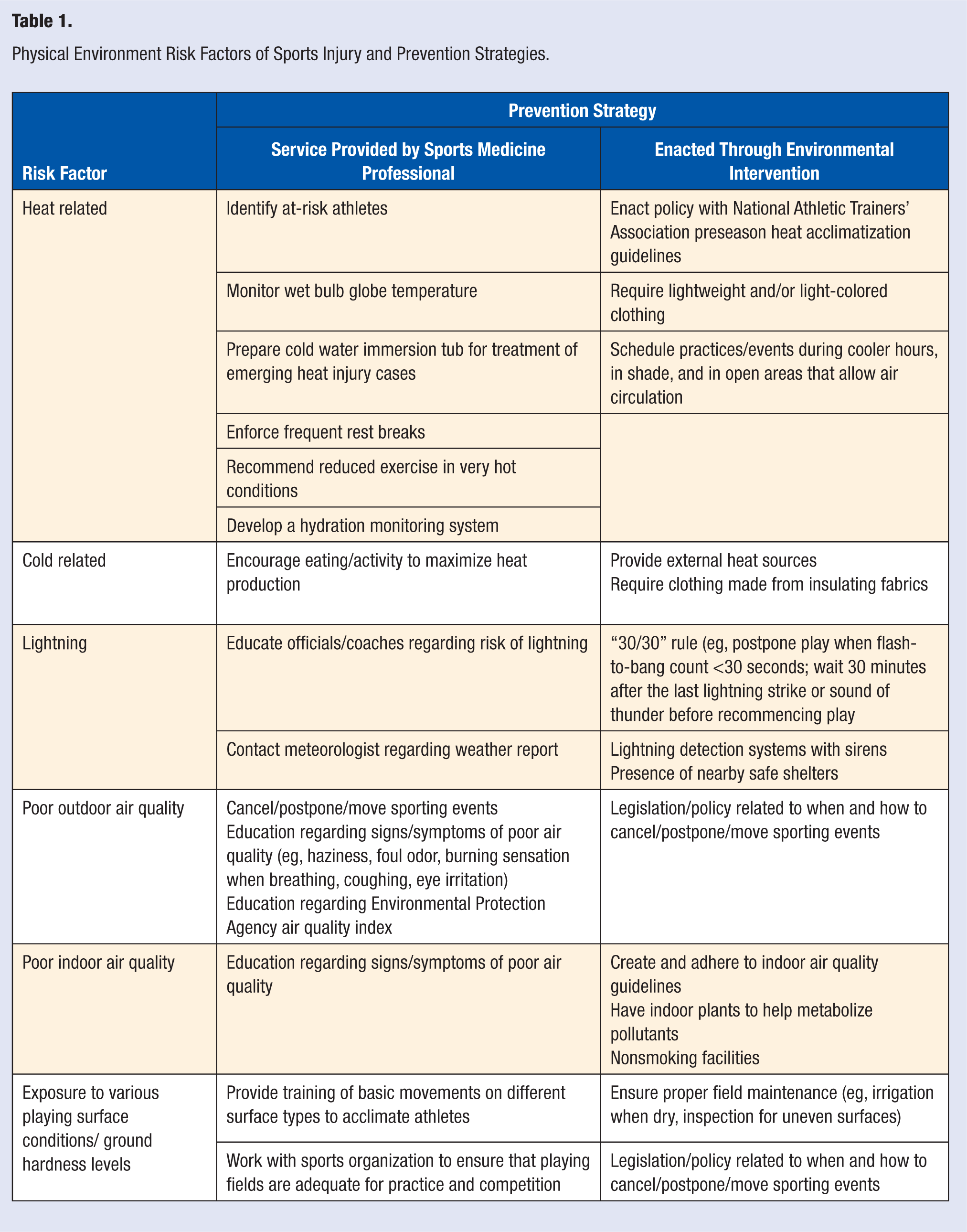
Athletes are exposed to a vast range of playing conditions stemming from the physical environment. Weather, temperature, and playing conditions affect injury burden, severity, recovery, and return to play. Table 1 outlines the various physical environment risk factors and prevention strategies that can be implemented by sports medicine professionals, or through environmental intervention.
Physical Environment Risk Factors of Sports Injury and Prevention Strategies.
Heat-Related Injury
A heat injury occurs when internal body temperature rises faster than the body’s ability to dissipate heat. Although often termed heat “illness,” the condition is in fact a type of injury since it involves uncontrollable energy transfer. Once an individual’s core temperature exceeds 104°F (40°C), cell failure and breakdown occurs, resulting in organ dysfunction and eventually system failure. Heat injury encompasses a wide range of conditions, including mild rash and cramping, through to catastrophic heat stroke that may result in death if not recognized and treated appropriately.
The majority of heat-related deaths in US children and adolescents occur in football, wrestling, cross-country, and other running sports.14,15 From 1995 to 2010, 46 football players died from heat stroke (35 high school, 8 college, 2 professional, and 1 sandlot). 16 In the summer of 2011, there were 6 heat-related deaths in high school football in the United States. 17 This is particularly troubling given the emerging evidence regarding effective treatment of heat-related injuries. More than 9000 high school athletes each year are treated for heat-related injury, with most occurring in football, and during August, when athletes are not yet acclimated to physical exertion in the heat. 18 The incidence rate of nonfatal heat injury for high school football was estimated at 5 per 100 000 athlete-exposures over the 2005-2006 and 2006-2007 academic years. 19 Unfortunately, many athletes are unaware of the onset of the condition and lack a knowledge regarding the potentially catastrophic outcomes of heat injury. Increased awareness and preventive measures are needed,20,21 especially given the advent of tangible climate change. 22
Heat is primarily dissipated through evaporation of sweat from the skin surface. Anything that impedes the body’s ability to release heat through evaporation puts an athlete at risk for developing heat injury. Common risk factors include the following: excessive exercise at high temperature in humid conditions, too much clothing, dark-colored clothing or equipment, insufficient rest breaks, lack of shade, poor acclimatization to exercise in hot climatic conditions, poor physical fitness, and obesity.20,21,23-26 Children are considered to be at an increased risk for heat injury relative to adults. Children have a higher surface area to mass ratio and a greater rise in metabolic heat per mass unit during physical activities, which results in greater heat gain on hot days. 23 Children also have a lower rate of perspiration, which reduces their ability to cool through sweating. 23 Additionally, children and adolescents may be at increased risk simply because they are more likely to be exposed to vigorous physical exercise during warm summer months.
Prevention
The presence of sports medicine professionals at athletic events in hot and humid conditions is critical, as they are specifically trained to recognize and treat such conditions. Sports medicine professionals should also advocate for more administrative policies related to preseason acclimatization, as many state high school associations have not implemented the guidelines recommended by the National Athletic Trainers’ Association (NATA). 27 Coaches should plan to acclimatize athletes gradually to activity in hot humid preseason conditions by providing graduated activity sessions for the initial 10 to 14 days. 21 Athletes should wear lightweight and light-colored clothing.20,21,23-25 In hot and humid conditions, reduction in exercise and frequent rest breaks with adequate hydration are important countermeasures.20,21,23-25
Athletes should also be free to hydrate at any time. Water should never be withheld by coaches as a punishment or incentive. Although hydration is emphasized, sports medicine professionals must also be aware of the dangers of overhydration and ensure appropriate maximum drinking limits (1.5 quarts per hour and 12 quarts per day 28 ).
Coaches and athletic trainers should be prepared to modify, postpone, or cancel practices and competitions in accordance with these published guidelines. Since both heat and humidity play a role in the onset of heat injury, there should also be extensive use of the Wet Bulb Globe temperature, which combines ambient temperature and ambient humidity data into one overall index. Published guidelines for exertion at various levels of Wet Bulb Globe temperature are available. Published guidelines for exertion at various levels of wet bulb globe temperature are available.20,21,24
In addition, any organized athletic event with potential for heat injuries, such as a long-distance run or a preseason high school football practice in hot and humid conditions, should be supervised by sports medicine professionals who are trained to recognize and treat heat-related conditions, and have a written emergency plan that includes instructions for initiating EMS (Emergency Medical Services) response. Preparations for such events should also include ensuring access to EMS transport if necessary, and filling a large trough with ice water prior to the start of competition, so that sports medicine professionals are able to rapidly cool heat-stressed athletes. Table 2 provides Web site links to additional information regarding heat injury prevention, including appropriate work/rest water consumption and tracking hydration with tools such as the Riley card and Ogden cord.
Recommended websites for sports medicine professionals.
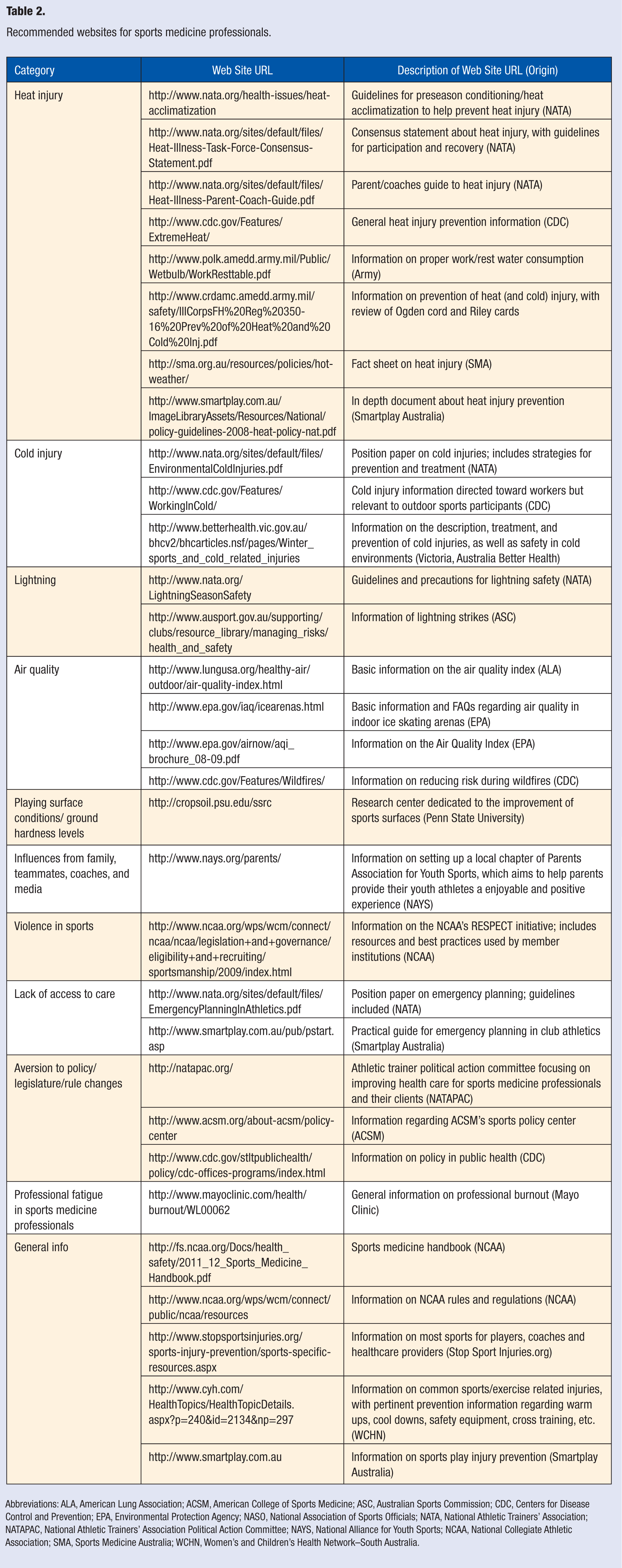
Abbreviations: ALA, American Lung Association; ACSM, American College of Sports Medicine; ASC, Australian Sports Commission; CDC, Centers for Disease Control and Prevention; EPA, Environmental Protection Agency; NASO, National Association of Sports Officials; NATA, National Athletic Trainers’ Association; NATAPAC, National Athletic Trainers’ Association Political Action Committee; NAYS, National Alliance for Youth Sports; NCAA, National Collegiate Athletic Association; SMA, Sports Medicine Australia; WCHN, Women’s and Children’s Health Network–South Australia.
Management
The key elements to treating heat injury are to (1) quickly identify affected athletes and (2) rapidly cool their whole body.29,30 Diagnosing heat injury is often difficult because of the use of external body temperature measurements, which may not be valid. A review by Casa et al 31 concluded that “no device using a site on the outside of the body has ever been proven valid under the conditions of intense exercise in the heat and a significant degree of hyperthermia.”
As an alternative, Casa et al 31 recommend internal heat sensors, which are small electronic devices that an athlete can ingest prior to exercise. They provide rapid and timely telemetry data on internal body temperature to an external handheld or belt-worn external sensor for 24 hours before breaking down within the body. However, these devices may be clinically unfeasible. First, they are expensive and may not fit in the budget constraints of a clinician or certified athletic trainer. Second, someone must monitor the data, which may be unrealistic, particularly in settings with limited medical coverage. Last, the pill must be ingested prior to exercise, and may pass through the body prior to the onset of heat exhaustion, meaning that it would have to be expected a priori that heat injury may be of concern. Given the expense, staffing needs, and a priori assumption of risk needed for internal heat sensors, Casa et al 31 also suggest taking a rectal temperature, noting that its equipment needs are minimal and measurements are not affected by the external environment.
Rapid initiation of whole-body cooling is critical. There is debate about the most effective method to rapidly lower core body temperature32,33; but immediate immersion in ice water is the fastest and most convenient way to initiate whole body cooling. 34 If recognized and treated early, the damage from heat injury is largely reversible. The key factors influencing reversibility are (1) the extent to which the core body temperature was elevated above 104°F (40°C) and (2) the length of time the core temperature was elevated above 104°F (40°C). 20 If the athlete spends too much time at too high a temperature (eg, more than an hour at 107°F [41.5°C], organ damage, coma, and eventually death will result. Table 2 provides Web site links to NATA for additional information on heat injury.
Cold-Related Injury
Cold-related injuries, like heat injury, involve an uncontrolled energy transfer: an uncontrolled loss of thermal energy (rather than an uncontrolled increase as in heat injury). Risk is exacerbated by low temperatures, high humidity, wind chills, high altitude, and prolonged exposure. Consequently, outdoor sport participants (eg, skiing, water sports, cold-weather distance running, cycling) are most at risk.
Hypothermia occurs when the internal body temperature goes below 95°F (35°C),35,36 because of the body being unable to maintain heat when exposed to low temperatures. Wet conditions added to cold conditions can increase the rapidity of the onset of hypothermia. 37 The physically active elderly population may be at higher risk for hypothermia because of an impaired ability to sense a drop in temperature, 38 and less heat production because of lower metabolic rates. 39 Unlike heat injury, hypothermia incidence has not been well documented, possibly because mild cases are easily treated with rewarming techniques. 35
Frostbite occurs when “a local anatomic area loses so much heat that ice crystals form in the extracellular spaces and water is extracted from cells.” 39 In most documented cases, frostbite occurs in body parts that tend to have the poorest circulation, the greatest exposure, and the largest surface areas (eg, feet, big toe, hands, ears, and other exposed areas of the face). 40 Immersion, or trench foot, is similar to frostbite. However, immersion is seen as less severe as ice crystals do not form in the extracellular spaces. 39
Prevention
Prevention of cold-related injury involves maximizing heat production and minimizing heat loss. 39 The body will naturally shiver to maximize heat production, but eating and body movement will also cause the core body temperature to rise. External heat sources are also beneficial but may lead to overheating and dehydration from excessive sweating. Clothing made of good insulating fabrics (eg, polypropylene, wool, Gore-tex) is essential for outdoor activities in cold weather and should cover areas most at risk (eg, gloves, goggles, hooded sweaters/ski caps). Socks and gloves should also be double-layered, with the first layer being polypropylene, and the second layer being wool. Sports medicine professionals should educate patients on proper sportswear and should recommend cancelling events when cold weather poses a serious risk to athletes. 39
Management
Frostbite treatment, outlined by MacCauley et al, 41 involves a rewarming process and requires a careful series of steps to ensure proper recovery. 39 For immersion, exposure to air (commonly referred to as “open treatment”) typically resolves symptoms. 39 In addition, sports medicine professionals can use a variety of passive and active rewarming techniques to aid recovery. 39 Hypothermic athletes can be moved to warmer environments, covered in dry blankets, and given heating blankets, hot packs, and warm water immersion. To prevent “rewarming shock,” or hypotension, caused by the rapid rewarming of the body, qualified clinicians can use “active core rewarming techniques,” which include administering intravenous fluid warmed to 104°F (40°C) through an endotracheal tube or supplying heated and humidified air/oxygen through a mask. 39 Table 2 provides a Web site link to NATA for additional information on treating cold injuries.
Lightning
An estimated 70% of all lightning-related injuries and fatalities occur in the afternoon and during the late spring to early fall.42,43 Many outdoor collegiate sport practices occur during this time frame. Consequently, although the risk of being hit by lightning is relatively low in the general public, athletes may be at increased risk.
Lightning most likely occurs at either the beginning or the end of a storm, 44 with lightning threat persisting up to 30 minutes after the last sound of thunder. Often, athletes leave the playing field too late on a storm’s commencement or return to play too soon after a storm’s demise. Golf, in particular, has the highest number of lightning-related deaths. Golf courses may also lack on-site shelters. 45 Golfers also have long periods of outdoor exposure and often have an overwhelming desire to complete a game despite weather conditions. Thus, a lack of knowledge exacerbates the risk of lightning-related injury.
Prevention
Coaches, parents, and officials need to be aware of the risk of storms and consult meteorologists prior to competition and practice to ensure the safety of their athletes. A safe place to seek shelter should also be made available.44,46,47 In golf, it has been recommended that courses install lightning detection systems and warning sirens. 45 Other sports facilities may also help protect their athletes with installation of similar lightning detection systems.
Management
A “30/30” policy has been proposed to protect athletes in outdoor venues: (1) postpone play when there is a flash-to-bang count of 30 seconds or less, which signifies that lightning is only 6 miles away, with the possibility of the next strike being closer and (2) wait 30 minutes after the last lightning strike or sound of thunder before recommencing play. 48 In the case of an unexpected thunderstorm, school buses can potentially serve as nearby safe shelters. 48 Spectators should also be evacuated, as the presence of significant quantities of water and large metal lighting towers and bleacher stands increase risk. Swimming pools are also vulnerable areas because of the transmission of electrical energy through water. Individuals should also avoid locations that increase risk (eg, high terrain, solitary trees, bodies of water, power lines) and know the weather patterns of the surrounding area.44,46,47 Table 2 provides a Web site link to NATA for guidelines and precautions regarding lightning.
Poor Air Quality
Poor air quality is an overlooked environmental risk factor. Although only inconvenient to average daily life, bad air quality can be debilitating to an athlete. Oxygen is required for cells to convert fuel to energy. This energy is used to create movement and power, as well as recover from activity by restoring fuel stores and metabolizing the by-products of cellular activity. Physiology dictates that vigorous physical activity requires more oxygen than less vigorous tasks. Thus, poor air quality’s interference with the transfer of oxygen from the blood may lead to respiratory symptoms that may affect athlete performance, increase athletic fatigue, and consequently, increase injury risk. Thus, although environmental factors such as poor air quality may not be directly related to injury incidence, they are nevertheless possible factors that exacerbate injury risk.
Wildfires affect the air quality of outdoor sports activities by creating smoke, ash, and a variety of combustion by-product gases, some of which are noxious. By-product gases interfering on the cellular level can impede oxygenation. For these reasons, athletic competitions may need to be cancelled in areas near wildfire. Pollution may also be of concern for reasons similar to that of wildfires. At the 2008 Olympic Games in Beijing, China, world record–holding marathoner Haile Gebrselassie chose not to compete because of concerns about air quality affecting his asthma. 49
Poor air quality can also occur indoors, particularly in indoor ice skating rinks that use propane- or gasoline-powered ice resurfacers and edgers. 50 Such machinery produces exhaust gases such as carbon monoxide (CO) and nitrogen dioxide (NO2). If indoor arenas have improper ventilation, air pollutants may collect, mostly at the ice level. Those at greatest risk include athletes who spend long durations on ice; children, who use oxygen faster than an adult; and individuals whose preexisting pathogenic conditions (eg, asthma) are exacerbated by poor air quality.
Prevention
Sports medicine professionals working with sports teams should acquire adequate knowledge regarding the air quality of the locations where competitions and practices occur. The US Environmental Protection Agency’s (EPA) Air Quality Index (AQI) provides daily air quality information, based on major pollutants such as ground level ozone, particle pollution, carbon monoxide, and sulfur dioxide. Sports medicine professionals should refer to their area’s AQI to recommend modifications for athletic events when air quality is poor. Table 2 provides Web site links to the EPA for additional information on the AQI.
It is essential that indoor sports facilities routinely check air quality levels. Prior to the 2000 Olympic Games in Sydney, the Australian Olympic Committee created guidelines 51 mandating that indoor facilities
do not emit harmful levels of pollutants, respirable particles, dust, or unpleasant odors at any point after construction
have low adsorption characteristics
are resistant to microorganisms such as bacteria, mold, and dust mites
can be effectively cleaned using benign cleansers and processes
do not emit harmful levels of radiation
are as safe as possible during installation and under extreme conditions
remain nonsmoking
complete construction early enough to allow for dissipation of pollution
use indoor plants to help metabolize pollutants.
We recommend that indoor facilities implement similar guidelines to help protect athletes and spectators, particularly those most at risk. Table 2 provides a Web site link to the EPA for information on air quality in ice arenas.
Management
Sports medicine professionals should also refer to updates to their area’s AQI to recommend modifications for athletic events as air quality decreases. In addition, although there may not be any realistic way to control poor air quality at outdoor events, it is important to be able to cancel, postpone, or move events when necessary. Sports medicine professionals in areas where outdoor air quality is an issue should encourage their sports organizations to create policies to assist in determining when and how to cancel, postpone, or move events. Last, sports medicine professionals should be educated on the signs and symptoms resulting from poor air quality (eg, haziness, foul odor, excess dust or ash on flat surfaces, burning sensation when breathing, wheezing, coughing, eye irritation). These same principles should be applied to indoor events as well.
Exposure to Various Playing Surface Conditions and Ground Hardness Levels
Athletes have extensive physical contact with the playing surface during practice and competition. Research suggests that harder playing surfaces present less shock absorption and consequently increases risk of musculoskeletal injury. 52 In volleyball, injuries during practice are more common on hard court surfaces than on sand. 53 In tennis, injuries are more common on hard courts and grass courts, compared with clay courts, although results between hard courts and grass courts vary.54,55 Uneven ground surfaces have also contributed to injury.56,57
Ground hardness softens with rainfall,52,58 reduced evapotranspiration (ie, the transporting of water into the atmosphere from surfaces),52,58 and high humidity. 52 In studies of rugby players, less rainfall,52,59 higher ground evaporation, 59 and higher temperature60,61 were associated with a greater incidence of injuries. 52 Two studies found that the injury incidence in rugby players was higher during the summer season than in the winter season.57,62 In another study, the highest injury rate was found in autumn, compared with early winter, late winter, and spring. 60
Varying shoe-surface tractions may also affect injury risk. A harder surface provides more shoe-surface traction and more force is transferred to the body.59,61 Higher traction (and thus, speed) equates to greater injury risk.52,63 However, diminished traction may also result in a loss of balance, which may contribute to injury. Playing surfaces that hold too much moisture may cause cleats to get caught in muddy ground more often.
Changes in turf characteristics over a season can affect playing surface quality. Many schools have opted for artificial turf fields, which can withstand more usage over a season, are easier to maintain, and have lower maintenance costs than a natural grass field. 64 There is also the recent development of third-generation artificial turf (3GAT), which features long grass-like fibers filled with sand and rubber particles to match the qualities of natural grass. There is concern that artificial turf holds more heat than natural grass fields, gets slippery as it gets warmer, 65 and poses higher injury risk for athletes.63,66 However, studies examining injury rates by playing surface have yielded mixed results, with higher injury rates on artificial turf, 67 higher injury rates on natural grass, 68 and no significant differences between both playing surfaces.69,71 Rates pertaining to particular injuries also vary.66,72,73 More attention to the study of the association between playing surface and injury is warranted.
Teams that invest in artificial turf may still be exposed to grass fields at away games. How the ball in play moves on the field (eg, bounce, roll) may differ between artificial turf and natural grass fields, 63 causing athletes to have to adapt their playing behavior. The changes in playing behavior caused by frequently playing on different surfaces may increase overuse injury. 74 In addition, the changes in the dynamics of game play may displeasure many athletes. 75
Prevention
Sports medicine professionals can encourage athletes to undergo training of basic movements (eg, acceleration, deceleration, pivoting) on different surfaces to help the body get accustomed to various playing conditions. Furthermore, being in peak physical fitness will allow for a faster learning curve of new skills and increase lower extremity strength and balance, which will help when accelerating and decelerating. 76
Management
Sports medicine professionals should work with their sports organization to ensure that playing fields are adequate for practice and competition. First, ground crews should maintain fields with proper irrigation, 52 and extra watering and covering of grounds when high water evaporation occurs, particularly during dry, sunny, and windy weather. 59 Before competitions, particularly during or following adverse weather conditions, it may be beneficial to walk the surface to look for debris and dangerous uneven patches of ground such as divots or overly worn areas. Maintenance of sports playing surfaces needs to also account for adequate shoe-surface traction that equally considers optimized player performance and decreased injury risk. 63 Few guidelines that define the ideal surface hardness currently exist. More research is warranted. In the case where the playing surface is soft or slushy due to weather, sports medicine professionals may advocate for a change in time or venue, or at the least, ensure that athletes are wearing proper footwear, if available.
The Social Environment
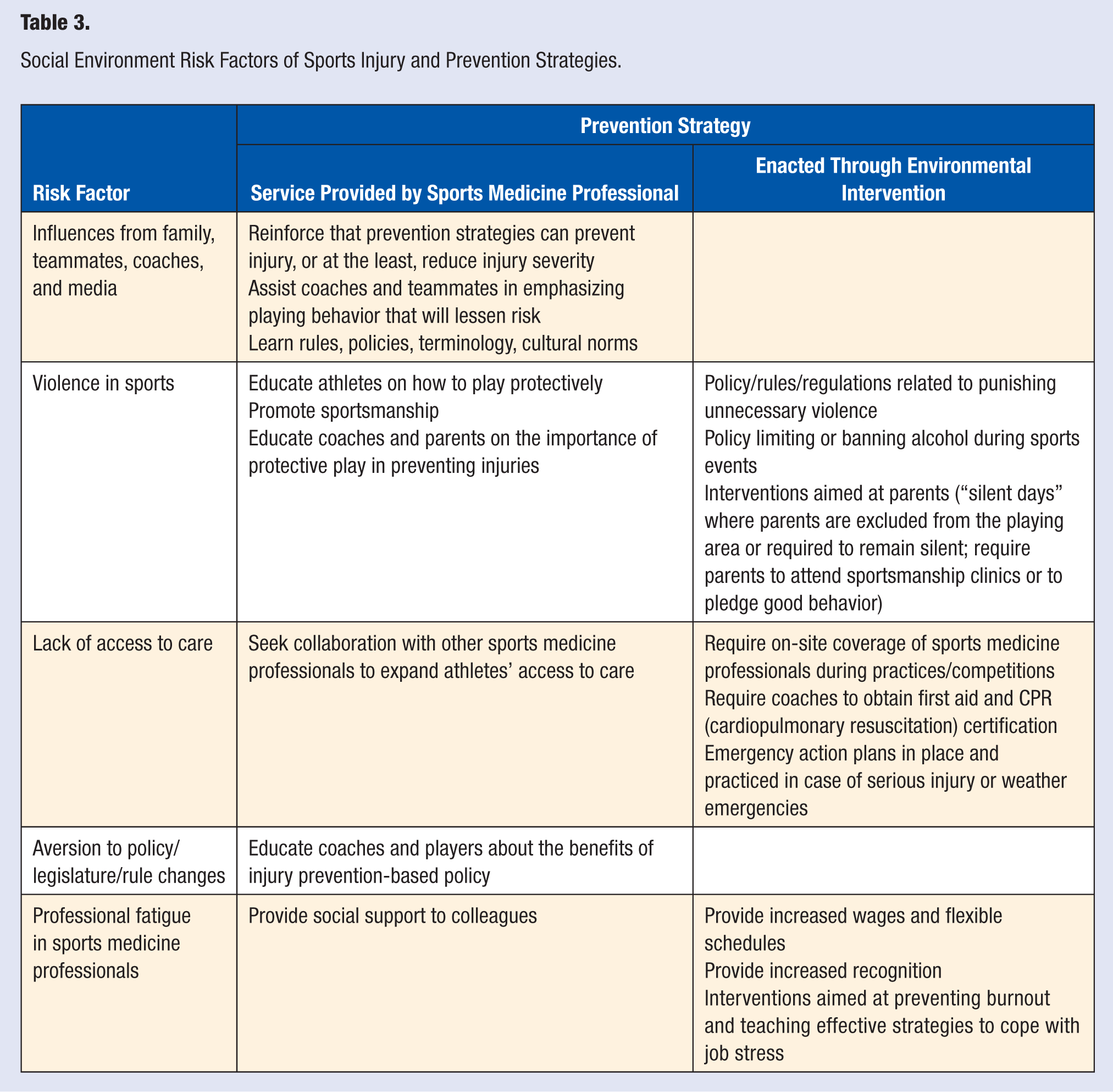
Athletes are thought to be at the pinnacle of physical health given the amount of training they perform to be prepared for competition. Research has found that compared with nonathletes, youth athletes engage in more regular vigorous activity and are also less likely to smoke cigarettes or use any illicit drugs.77,78 However, findings comparing alcohol use in athletes and nonathletes are inconsistent. 79 Although such characteristics may be related to an overall lower risk of morbidity and mortality, athletes are nevertheless influenced by the observation of others via social contexts, media, and other modes of communication. 80 As a result, the social environment, or “the totality of the behavioral, personality, attitudinal, and cultural characteristics of a group of people,” 81 can potentially contribute as much injury risk as the physical environment and is crucial for sports injury prevention.13,82 Table 3 outlines the various social environment risk factors and prevention strategies that can be implemented by sports medicine professionals or through environmental intervention.
Social Environment Risk Factors of Sports Injury and Prevention Strategies.
Influences From Family, Teammates, Coaches, and the Media
Athletes are influenced by outside sources such as family, teammates, and coaches. Parents, with aspirations of their children receiving future gains through sports, such as college scholarships, may place undue pressure on the student- athlete to play under adverse circumstances. Parents may also attempt to fulfill their own need for accomplishment and success 83 by expecting their child to have adult- and professional athlete–like performances. 84 On the other hand, parental involvement can take an overprotective stance, which can be as equally detrimental to a child.
Social forces can prevent an athlete from receiving the care that they need. Athletes may be reluctant to seek care because of a perception that they are letting their team down. There may also be subtle social pressures that discourage care-seeking, such as the so-called “Badge of Honor” mentality in which some athletes choose to celebrate the pain and injury they endured for their sport. Sometimes athletes and teams simply lack knowledge of the actual severity of the injury. For example, a study of youth football coaches found that more than a quarter reported that they would have allowed a concussed athlete exhibiting symptoms to return to play, 85 despite the fact that clinical guidelines state that concussed athlete exhibiting symptoms should be removed from play. 86
Social and news media also normalize the concept of pain and injury as a “normal” aspect of sports participation. A content analysis 87 of Sports Illustrated articles that detailed reports of pain, injury, and disability found themes related to athlete and coach attitudes that (1) pain/injury should not get in the way of the game and (2) athletes should push their bodies and accept injury risk, and if needed, play hurt to further the success of the team. A recent Gentlemen’s Quarterly article 88 on NFL players’ perceptions about concussions noted that athletes felt that the love of the game and salary outweighed the risk of injury and that those wanting to entirely avoid the risk of injury should not play.
Media also creates portrayals of masculine identities in male sports. Duncan and Messner 89 argued that media contributes to how masculine identities were socially constructed through descriptions of male athletes that emphasized strength (eg, “confident,” “powerful,” “gutsy”). Meanwhile, descriptions of athletes that emphasized weakness (eg, “weary,” “panicked,” “dejected”) suggested that athletes were not living up to their masculine identity. For example, in 2009, when Pittsburgh Steelers quarterback Ben Roethlisberger was not cleared by a neurologist to play in an important game because of a recent concussion, the media reported that teammates labeled him as “soft,” inferring that he should have withheld information about his injury from his health care providers.90-94
Prevention
Athletes exposed to media that normalizes pain and injury as a part of sports play may require prevention education from their healthcare providers. Young athletes in particular may ignore injury prevention information because they believe that they are already knowledgeable and understand risk. 95 Consequently, sports medicine professionals need to reinforce that although athletes are inherently at risk for injury in any sports participation, prevention strategies, particularly those with buy-in from coaches, teammates, and parents, can reduce the burden of injury. For example, the Centers for Disease Control and Prevention’s “Heads Up: Concussion in High School Sports” concussion prevention toolkit focuses on providing specialized messages to parents and coaches alongside players in order to better prevent, recognize, and respond to concussions.96,97 Better understanding of the mind-sets of parents, coaches, and athletes will help tailor future intervention and education programming appropriately.
Management
Sports medicine professionals must emphasize to injured athletes the need to adhere to rehabilitation regimes in order to help athletes attain their full athletic potential. 98 Alongside tailored interventions, sports medicine professionals also need to educate coaches, teammates, and parents about the importance of allowing full recovery from injury. Associations that help parents in being positive role models during sports plays also exist. Table 2 provides a link to additional information.
Violence in Sports
Sports-related violence, in general, has resulted in both physical and emotional injury to participants, parents, referees, and fans. 99 Recent data suggest that the incidence of foul play–related injury is high. 100 Even though reports of sport-related violence are abundant, and earnest efforts have been taken to control it, few studies have examined the prevalence of sports-related violence or measures of the resultant morbidity and mortality. A review by Fields et al 99 found that a large number of youth athletes reported that “cheap shots” against opposing players were common in youth sports. 101 In addition, athletes found aggression to be acceptable in sports 102 : to protect themselves against uncalled fouls 103 or in retaliation for poor officiating. 104
Spectator violence is also an issue of considerable importance. In a recent study, Rees and Schnepel 105 found that at Clemson University, the campus area saw larger than expected numbers of documented aggressive behavior (eg, vandalism, arrests related to disorderly conduct arrests, and alcohol-related offenses) when home football games occurred. Larger deviances from the expected number occurred when a game ended in an upset. Violence may also occur as a result of perceiving officiating to favor the opposing team. 106 Although spectator violence may be directed toward fans of opposing teams or officials, athletes may also be at risk. Unfortunately, in some cases, such as the 2004 NBA Pistons/Pacers brawl, the athletes may be the perpetrators of violence on spectators.
Given its heavy coverage, media may exacerbate the dilemma of sports violence involving incidents related to hazing, foul play, and brawling. 107 Messner et al 108 noted that sports broadcasters commended athletes for exhibiting aggressive behavior, particularly when directed toward an injured player (eg, a football defense blitzing an injured quarterback). Rhetoric regarding sports violence may contribute to aggressive playing behavior in athletes. It has been suggested that sports broadcasters need to refrain from excessive coverage of sports violence. 109
Prevention
Sports medicine professionals must take a lead role in educating athletes on how to play protectively. The more that an athlete understands the biology and damage due to inflicted injury, the more likely the athlete is to be compliant with campaigns discouraging violence in sports. Furthermore, sports medicine professionals can also promote sportsmanship in the athletes with which they work. Sports medicine professionals can also educate coaches and parents on the importance of protective play in preventing injuries.
In addition, sports organizations can promote interventions for spectators. For example, a number of youth sports leagues enforce “silent game” days where parents must remain silent during game play or are not allowed to attend. 99 However, “silent game” days also inhibit positive spectator behavior, which has been found to be associated with positive player behavior. 110 In addition, there has been discussion for eliminating alcohol consumption at sporting events, although some organizations have found no decreases in violent behavior with the implementation. 105 Future research is needed to better understand the effects of individual and environmental interventions that aim to provide safe and respectful playing venues among all athletes and fans.
Management
It may not be possible for a single sports medicine professional to convince an entire team to play fairly and less violently. However, if injured athletes are educated during recovery, they can be an influential source of information to teammates. In addition, sports medicine professionals should advocate for zero-tolerance policies that suspend players that purposely inflict harm toward players on opposing teams. Table 2 provides a link to information regarding the NCAA’s RESPECT initiative that aims to decrease sports play violence.
Lack of Access to Care
The availability of sports medicine professionals at practice and competition facilities can lessen the severity of chronic injury and the resulting time loss from play. In professional and Division I collegiate sports, there is typically at least one certified athletic trainer on-site, for both practice and competition. Coverage in lower division collegiate sports and high school athletics is limited, and worse in club sports. It is estimated that only 42% of US high schools have access to a certified athletic trainer. 111 Studies examining high schools from North Carolina (private schools), 112 Wisconsin, 113 Southern California, 114 and Illinois 115 all reported high schools with inadequate coverage, including no access to certified athletic trainers, no physician coverage at practice and competitions, no ambulance coverage at games, and coaches with limited first aid and cardiopulmonary resuscitation knowledge. One study 115 found that high schools that were rurally located and had smaller student populations (<500) had less access to certified athletic trainers.
In addition, there may be differences in the quality and availability of pre-participation screening to detect chronic or underlying health issues that may place athletes more at risk for injury. If done appropriately, screening can be a valuable tool. However, when athletes are from communities with lower socioeconomic status, access to medical care for preparticipation screening may be an issue in itself. Furthermore, there is limited standardization of preparticipation screenings.
Prevention
Sports medicine professionals and athletic administrators need to advocate for increased on-site coverage at practices and competitions in order to reduce injury severity in athletes. Appropriate preparticipation screenings of musculoskeletal, cardiorespiratory, and neurological systems can also help identify student-athletes who may be at risk for sudden or severe injury. This is especially important in the absence of daily coverage by sports medicine professionals, where immediate care is not available. Sports medicine professionals working with communities with lower socioeconomic status should also seek collaboration with other sports medicine professionals to provide athletes with additional access to care.
Management
Since it may not be realistic to expect medical coverage in all scenarios, it would be beneficial to recommend that coaches are trained and certified in first aid and cardiopulmonary resuscitation. Emergency action plans should be implemented and practiced for a wide range of scenarios, including serious injury events or weather emergencies. The plans should ensure all personnel (coaches, athletes, and school supervisors) know how to react when an emergency occurs. Such mandates could be implemented at the school, state, or national level. Table 2 provides a Web site link to NATA for guidelines on emergency planning.
Aversion to Policy/Legislation of Sports
In a recent analysis of approximately 12 000 sports injury prevention publications, only 66 (0.1%) examined how changes in rules and regulations increased safety and/or reduced injuries. 116 The lack of research is surprising, given that many policies exist to protect athletes. Colleges, schools, communities, and sporting organizations have enacted policies to limit sport-related violence (eg, anti-hazing laws, parents signing contracts, “silent game days”). States and state high school associations have or are in the process of enacting legislature and policy related to concussions 117 and heat injury. 27
Policy changes may lack buy-in from athletes. Eight NFL players interviewed for a Gentlemen’s Quarterly article found the NFL’s attempts to prevent concussions through fining players who committed helmet-to-helmet hits to be insincere and hypocritical. 88 Players noted that it is difficult to change a sports play culture that emphasizes hard hits, and they questioned the NFL’s sincerity, as it does not offer insurance for life to retired players. In addition, players noted that the NFL’s video, which intended to teach players the difference between proper and improper hits, was vague.
Although policy changes aim to modify barriers to injury prevention, they can backfire. A policy that mandates that athletes cannot return to play the same day after sustaining a concussion may inadvertently cause an athlete to withhold reporting the injury for fear of being taken out of a critical game. A reduced number of injuries could reflect not an actual reduction in injuries, but rather a reduced number of injuries reported. Furthermore, policy that helps increase education and accurate identification of injury should cause the reported number of injuries to actually increase. Without careful interpretation, opponents of policy may incorrectly conclude that such policy consequently had a detrimental effect.
Prevention
Sports medicine professionals can assist in the dissemination and implementation of new policy/legislation by helping coaches and athletes understand how new policy benefits player safety. Previous success stories of policy/legislation can be highlighted to reflect the positive changes created through their implementation.
Management
With new policy/legislation in place, sports medicine professionals should emphasize positive changes that are seen through its implementation. However, they must proceed with caution as to not misinterpret data and thus, generate incorrect conclusions. Given the call for more implementation- and dissemination-based research,116,118 sports medicine professionals could turn to academia to help understand the effects of new policy/legislation.
Professional Fatigue in Sports Medicine Professionals
Although most sports injury research related to the social environment focuses on the athlete, it is essential to also focus on the social environment of those sports medicine professionals providing care to injured athletes. Sports medicine professionals experiencing high levels of stress may provide lesser quality of care to injured athletes. Research regarding “professional fatigue” in sports medicine professionals is limited but has cited high work volumes, low administrative support, and difficult policy and procedures as contributors to job stress.119,120
Prevention
Burnout is of particular concern. It is important for sports organizations to support certified athletic trainers, both occupationally (increased wages, flexible schedules) and emotionally (administrative support, increased recognition). 119 In addition, students and fellows training to become sports medicine professionals need to receive support from their mentors and colleagues.121,122
Management
The concern for burnout warrants the exploration of interventions that will help sports medicine professionals exhibiting the symptoms of burnout. Both current sports medicine professionals and those in training need to be taught effective strategies to cope with job stress.121,122 Future research on effective interventions, particularly those that use elements from previous successful interventions in other fields,123,124 is warranted. Table 2 provides a link to general information on preventing job burnout.
Conclusion
Sports medicine professionals have an integral role in a sports organization and should be proactive in recommending better prevention and care strategies for the athletes they serve. This article has discussed numerous environmental risk factors and prevention strategies related to sports. We recommend that sports medicine professionals consult Table 2 for a list of resources that would provide additional information related to themes discussed in this article. Given our search strategy, there are many other themes that are not discussed in detail in this article, such as snow blizzards, avalanche risk, and lighting conditions, that warrant exploration. As a result, we also recommend that sports medicine professionals use the vast resources available not only through US organizations but also those on an international scale. The “general” info section of Table 2 includes organizations and Web sites where additional sports safety resources can be obtained. A better understanding of environmental risk factors, as well as prevention and management strategies, will help athletes to reduce their burden of injury, and optimize athletic performance.
Footnotes
Acknowledgements
The authors thank the staff at The Matthew A. Gfeller Sport-Related Traumatic Brain Injury Research and The Center for the Study of Retired Athletes for their input. The authors also thank the reviewers for their valuable feedback during the review process. There have been no involvements that might raise the question of bias in the work reported in the conclusions, implications, or opinions stated.