
Abstract
Physical fitness is tightly linked to our ability to be physically active, and poor fitness is tied to increased risk of lifestyle diseases such as diabetes and cardiovascular disease in adulthood. In 2011, the Institute of Medicine appointed an expert committee to review the evidence between physical fitness and health outcomes in youth. Specifically, experimental and longitudinal studies published between 2000 and 2010 were reviewed in the areas of body composition, cardiorespiratory fitness, musculoskeletal fitness, and flexibility. Specific fitness tests that were linked to health risk factors or health outcomes in each of these areas were identified. Recommendations for the best fitness test items for use in schools and also for a national survey were given. In addition, guidance was provided for interpretation of fitness test scores along with recommendations for areas of needed future research. Key findings from the final report “Fitness Measures and Health Outcomes in Youth” will be reviewed.
Keywords
‘Physical fitness has been defined as “a set of attributes that people have or achieve that relates to the ability to perform physical activity.”’
The lack of adequate physical activity that is affecting our nation’s youth has received considerable attention over the past few decades, and only again more recently have we seen a resurgence in the promotion of physical fitness and the study of its impact on health outcomes. Physical fitness has been defined as “a set of attributes that people have or achieve that relates to the ability to perform physical activity.” 1 It is through several of these attributes that fitness is associated with our ability to be physically active and in turn acquire additional health benefits such as decreased risk of diabetes and cardiovascular disease.
Over a half of a century ago, physical fitness testing among American’s youth focused on performance-related fitness, such as measures related to sports or military performance. Today, fitness testing has evolved to focus on health-related fitness, which has been categorized to include 4 general areas/components: body composition, cardiorespiratory endurance, musculoskeletal fitness, and flexibility. In adults, each of these has been related to specific health outcomes; however, research supporting similar relationships for each of these in children and adolescents is less well-established, especially in identifying specific fitness tests that correspond to health risk factors and/or health outcomes.
In 2011, the Institute of Medicine (IOM) appointed an expert committee to assess the research evidence for the relationship between each of the fitness components and related health outcomes. Within this context, the committee was asked to identify physical fitness test items for youth that are valid, reliable, and related to health as well as suitable to include in a national survey to measure health-related fitness. Finally, the committee was tasked with identifying areas for future research. This review will serve to outline these practical recommendations from the final report titled “Fitness Measures and Health Outcomes in Youth” that was released in the fall of 2012. 2 Readers may wish to use this information for enhanced interpretation of field-based and clinical research studies and to better understand needed areas of future research in the context of youth fitness and health outcomes.
Methodology
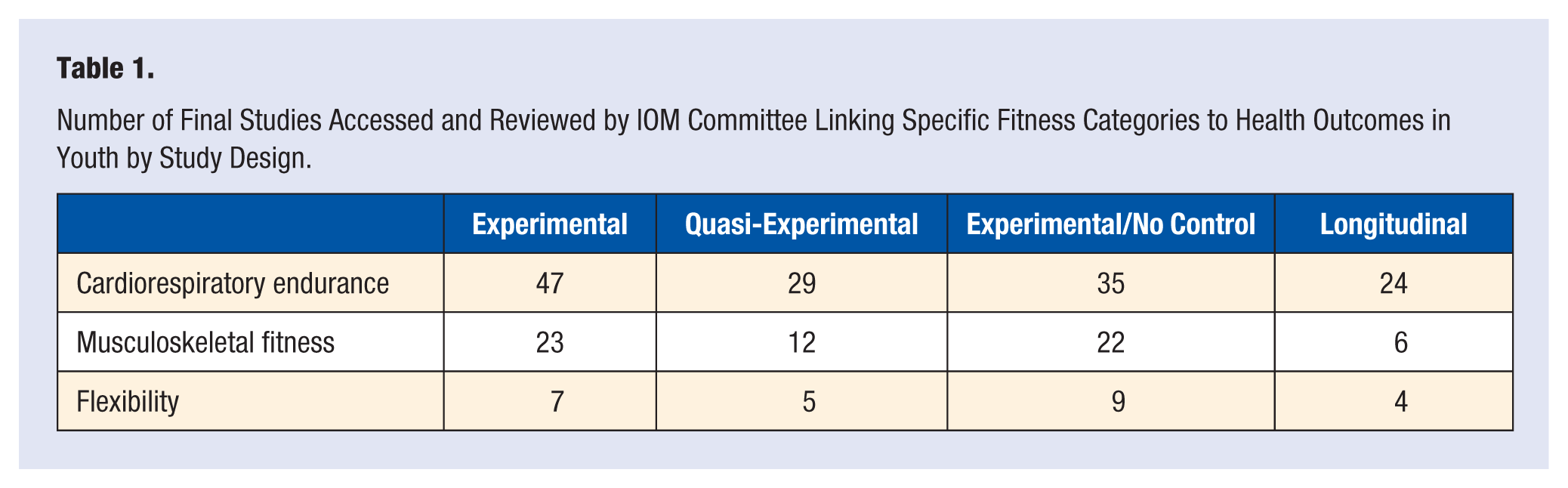
The primary evidence base that the IOM committee used was a systematic review. This was performed and compiled by the Centers for Disease Control and Prevention (CDC) and included literature on physical fitness and health outcomes published from 2000 to 2010 encompassing 3 major areas: cardiorespiratory endurance, musculoskeletal fitness, and flexibility. Over 32, 000 abstracts from 4 literature searches retrieved by CDC Reference Librarian were initially screened, more than 20, 000 screened for inclusion after removal for duplicates, 462 papers were fully reviewed, and from these 179 were extracted for the working database (cross-sectional studies were not included). The reviewed studies were grouped into longitudinal studies, experimental studies, and quasi-experimental studies. Table 1 refers to the number of studies examined in each group by fitness category. Body composition was not independently compiled by the CDC due to the relationship between body composition and health outcomes being well-established. However, the committee developed their conceptual framework (Figure 1) and determined that body composition should be assessed as both a fitness measure and health outcome. Body composition studies were therefore gathered from the CDC literature search when examined as a fitness component with independent health outcomes. In addition, IOM committee members supplemented the systematic search with select publications based on their knowledge of the scientific literature.
Number of Final Studies Accessed and Reviewed by IOM Committee Linking Specific Fitness Categories to Health Outcomes in Youth by Study Design.
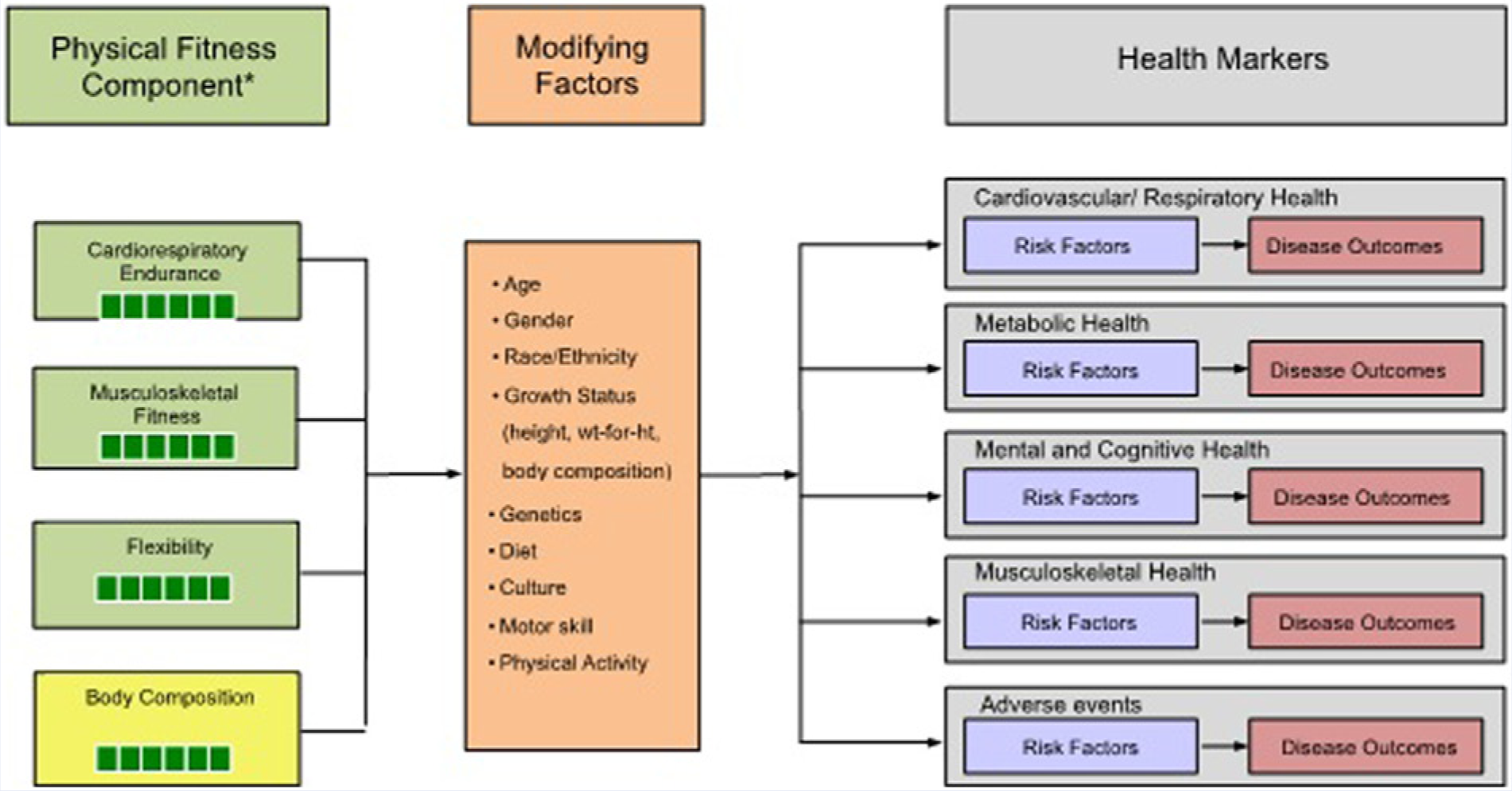
Conceptual framework for physical fitness measures, modifying factors, and health markers/outcomes in youth.
The conceptual framework (Figure 1) guided the systematic review. First, the committee established a link between individual fitness components and health risk factors and/or outcomes. Health risk factors are included as many health outcomes are not yet detectable in youth. Once the link between a fitness component and health risk factors/outcomes was established, studies were reviewed for the most reliable, valid, and practical measures of fitness for each component and their link with health outcomes. A standard rubric was used to evaluate each study for strength and quality of research design and findings. Links between test items and health outcomes were categorized as direct or associational based on the strength of the study design and the rigor of the statistical analysis. The strength of the evidence was categorized as sufficient or insufficient based on the number of studies with direct or indirect evidence, the study designs, appropriate populations, assessment of known confounders, and the statistical significance of the association.
Finally, modifying factors (e.g. age, sex, maturity, socioeconomic status, race/ethnicity, weight status, motor coordination, etc.) affecting fitness tests and health outcomes were assessed. A more thorough explanation of the detailed methodologies undertaken for the review is outlined in the final IOM report. 2 Below we outline the findings and practical recommendations for each fitness component.
Findings From Individual Fitness Components
Body Composition
Body weight and body fat are elements of body composition, which the committee defined as a component of fitness, a modifier of fitness, and a health marker/outcome (Figure 1). Body composition can vary widely due to age, sex, maturation status, and race/ethnicity. Sex differences in body mass index (BMI) are small during childhood but increase during adolescence. 3 In childhood, girls experience faster increases in fat mass than do boys, and fat mass plateaus near boys’ adolescent growth spurt. 4 For both sexes, BMI reaches its lowest point around 5 to 6 years of age and then continues to increase linearly with age through early adulthood. Males accumulate relatively more subcutaneous fat on the trunk, while females have a more equal distribution between the trunk and the extremities.5,6 In addition, youth who are more advanced in maturity status have more body fat and more subcutaneous fat on the trunk.3,6
Body Composition as a Fitness Component
There is a well-established link between excessive body fat and risk factors for chronic disease. The Bogalusa Heart Study found that 60% of children who were overweight by the age of 10 had at least one biomarker or risk factor for cardiovascular disease. 7 NHANES data also revealed a dose–response relationship between increasing body weight and 2 or more cardiovascular disease risk factors. 8 This association between elevated weight status and increased risk of cardiovascular disease is particularly evident in children with low cardiorespiratory fitness.9,10 Higher childhood weight was also associated with markers of metabolic syndrome 11 and prediabetes. 12 The location of adipose may also play an important role in disease risk. In the Bogalusa Heart Study, an increase in waist circumference was associated with a decrease in high-density lipoprotein (HDL) cholesterol and an increase in triglycerides and insulin among African American girls. 13 Another study in children found that fat distribution was a better predictor of cardiovascular disease risk factors than BMI. 14
These relationships also track into adulthood. Research from the Fels Longitudinal Study shows a relationship between childhood and adult obesity, 15 and more data from the Bogalusa study demonstrate that skinfolds and BMI z-score in childhood were the main contributors to C-reactive protein (CRP; another cardiovascular disease risk factor) in adults. 16
Body Composition as a Modifier of Fitness
Body composition is also a major factor/modifier of physical fitness and performance on physical fitness tests. Studies in youth found negative correlations between BMI and the sum of skinfolds and various fitness tests in both sexes.17-19 Also, low levels of cardiorespiratory endurance were correlated with percent body fat in African American and white adolescents 20 and with BMI and skinfolds in obese children aged 6 to 13. 21 Children and adolescents aged 5-14 who were classified as “underfit” had a higher risk of obesity. 22
Measures of Body Composition
Though there is no body composition method that is universally accepted as the gold standard, 23 laboratory measures (ie, underwater weight, body potassium, total body water, and dual-energy X-ray absorptiometry [DEXA]) are recognized as the most accurate. However, these methods require specific training, expensive equipment, and often a clinical setting and are therefore are unlikely to be feasible for measuring body composition of large samples of youth.
Field-based measures include measurement of BMI, skinfolds, bioelectrical impedance, and waist circumference. BMI, calculated from height and weight, is most useful for classification of weight status. Though there is no prediction of body fat, 24 BMI is adequately well-correlated with fat mass and percent body fat in youth.25,26 Skinfold thickness is a double fold of skin along with underlying fat tissue taken at specific body sites—the most often used are triceps and subscapular (under the shoulder blade). Skinfold measurements performed by trained individuals are valid and reliable estimates of subcutaneous fat distribution and predictors of body fat.27-29 Waist circumference is useful as an indicator of abdominal fat. 30 Though it is not a particularly reliable indicator of percent body fat, it provides information about abdominal fat, a useful dimension of body composition linked to health risks.
National Youth Survey
For large national surveys, field-based measures of body composition—BMI (estimate of body weight relative to height), skinfold thickness (at the triceps and under the shoulder blade as indicator of subcutaneous body fat), and waist circumference (indicate of abdominal adiposity)—are recommended. Each of these measurements of body composition has limitations, including reduced accuracy and high variability, with variable validity. However, due to each assessing a different aspect of body composition, along with their minimal subject burden, adequate reliability, and associations with markers of health risk, their inclusion in a national youth fitness survey is justified.
School-Based Survey
For school-based fitness tests, the committee recommends measuring BMI, which is a practical measurement that can be performed rather quickly through measurement of standing height (linear growth) and weight (body mass). Due to measurement in a school environment, potential privacy issues may be encountered and care should be taken to ensure privacy.
Future Studies
To date, many studies examining fitness and health outcomes in youth have not adequately controlled for or measured body composition. Future studies involving body composition should explore the relationship between specific body composition measures and physical fitness tests with particular attention to the potential interactions among body composition, fitness, and health in youth.
Cardiorespiratory Fitness
Cardiorespiratory endurance, the ability to perform whole-body exercise at moderate to high intensities for long periods of time, 31 is an important component of physical fitness. Producing energy at high rates through aerobic metabolism depends on transport of oxygen through with cardiovascular system, consumption of oxygen in the aerobic metabolic process, and removal of waste products. Those with high levels of cardiorespiratory endurance have well-adapted skeletal muscles and highly functional cardiorespiratory systems. In adults, clear relationships have been found between cardiorespiratory endurance and health outcomes such as lower risk of cardiovascular disease,32-34 type 2 diabetes, 35 hypertension, 36 certain cancers, 37 and premature mortality.33,38,39
Fitness Tests
The usual laboratory test for assessing cardiovascular endurance is maximal aerobic power (VO2max), the gold standard. This is measured by a participant exercising at a maximal level on a treadmill or cycle ergometer, typically via a graded exercise test, and is a key physiologic determinant of cardiorespiratory endurance.40-42 Distance or timed runs such as the 1 mile run and shuttle runs, in which participants run between 2 set points 20 meters apart, are also reliable and valid field tests used for assessing cardiorespiratory endurance.43,44 Distance run tests greater than 1 mile have acceptable validity versus VO2max28,45 and have also been found to be reliable. 45
Studies in Youth
Among studies assessing cardiorespiratory endurance through treadmill and cycle ergometer tests, one found that an increase in VO2max through adolescence corresponded to a healthy cardiovascular risk profile in adulthood, 46 and another demonstrated a relationship between changes in cardiorespiratory endurance and health markers over 5 years. 47 Other longitudinal studies also found associations between improvements in cardiorespiratory endurance and improvements in BMI, along with a lower risk of becoming overweight.48-51
Considering the high correlation between cardiorespiratory endurance and body fatness, it can be difficult to assess their individual effects since both are risk factors for cardiovascular disease. Walther and colleagues revealed increases in VO2max in youth without corresponding decreases in adiposity. 52 Several studies also examined the relationship between changes in cardiorespiratory fitness and changes in adiposity and cardiometabolic risk factors but were not always able to tease out the independent effects of changes in fitness and adiposity on the health markers.53-58 One cycle ergometry study found improvements in cardiorespiratory endurance and corresponding improvements in HDL cholesterol in overweight youth after exercise training independent of changes in adiposity. 59 Overall, cardiorespiratory endurance as measured by either treadmill or cycle ergometry tests demonstrate the strong relationships with changes in adiposity and cardiometabolic risk factors.
For studies involving distance/timed run and shuttle run tests, of which the shuttle run studies were the most common, most were school based. Two school-based experimental studies found a relationship between increases in physical fitness and decreases in adiposity, improvements in cardiometabolic risk factors, 60 and blood pressure. 61 Others demonstrated relationships between improved performance on the shuttle run and improvements in cardiometabolic risk factors,61,62 while two other longitudinal studies found inverse relationships between baseline cardiorespiratory endurance and increasing BMI and incidence of overweight.22,63 Two studies demonstrated fitness improvements and corresponding improvements in bone health 64 and blood pressure. 61 Overall, the strongest relationships identified in these studies used the shuttle run as the fitness test and indicated a strong relationship with changes in BMI as the health outcome.
National Youth Survey
The three tests that demonstrate the strongest evidence for a relationship to health—shuttle run, treadmill, and cycle ergometer—are all generally feasible. The treadmill and cycle ergometer, while requiring much less space, necessitate expensive equipment and extensive training for the administrator. Therefore, the shuttle run is recommended for a national survey of cardiorespiratory fitness. If space is limited, the cycle ergometer and treadmill tests are valid and reliable alternatives.
School-Based Survey
For school-based surveys of cardiorespiratory fitness, the progressive shuttle run is recommended. Additional tests, such as the distance or timed runs, although not yet shown to be related to health, may be considered as supplemental educational tools.
Future Studies
Studies should continue to examine the relationship between changes in cardiorespiratory endurance as measured by field tests and subsequent changes in health risk factors in youth beyond weight status and cardiometabolic risk factors (eg, bone health and neurocognitive function and behavior). Additionally, many studies to date have not appropriately examined the effects of various modifiers such as demographics, body composition, and nutrition on the relationship between cardiorespiratory endurance and health.
Musculoskeletal Fitness
Musculoskeletal fitness by definition encompasses muscular strength (ability of skeletal muscle to produce force), endurance (ability of skeletal muscle to perform repeated contractions over time), and power (the rate at which muscle work is performed).65,66 In adults, a review of fitness test items and health outcomes found a valid link between abdominal/core strength and back health with musculoskeletal fitness. 67 Over time, research has moved beyond back health and associations have been uncovered connecting muscle strength with personal independence, quality of life, lower cardiometabolic risk factors, and the declining frequency of cardiovascular disease events.68-72 Muscle endurance has been associated with overall quality of life and negatively associated with falling and the associated injuries, 71 while the loss of muscle power has been associated with decreases in functional ability and decreased mobility and premature mortality.71,73
Fitness Tests
Over the years, musculoskeletal fitness has been assessed in youth using a variety of different fitness test items. There has been an increased focus on these test items in youth since the 1970s due to health data from the adult population.74-77 In fact, more than 11 different classes of fitness test items have been used to evaluate musculoskeletal fitness in children, though many of those items do not satisfy the physiological definitions of the aforementioned three dimensions (muscular strength, endurance, and power) and many are site-specific (eg, upper vs lower body). Examples include hand-grip strength test (static strength), standing long jump (strength, power), pull-ups and flexed arm hang (strength, endurance), sit-ups (strength, endurance), and throwing (explosive strength).
Studies in Youth
Though far less evidence exists to support the relationship between musculoskeletal fitness and health in youth, it has been studied recently in relation to the development of the Fitnessgram/Activitygram 78 and a new test battery for European youth.79-81 A recent review 80 reported inverse associations between lower-limb muscular power and lower-abdominal obesity in youth, 82 a composite muscle fitness index score and a composite measure of cardiovascular risk in adolescent girls, 83 and cardiovascular inflammatory markers and muscular strength normal-weight and overweight adolescents. 84 Another recent review found strong associations between changes in muscular strength and changes in overall adiposity. 81 There are still questions regarding the possible association between improved musculoskeletal fitness and bone health. There is indirect evidence of associations between upper-body, trunk, and lower-body strength with various skeletal measures, mainly in girls.85-87 Few have studied this relationship in boys, and only two studies found direct evidence linking musculoskeletal health and bone health.88,89
Studies examining the relationship between musculoskeletal fitness and markers of metabolic health exclusively studied overweight/obese youth. One found associational evidence between muscle strength (upper-body, trunk, and lower-body) and hepatic insulin sensitivity and glucose production, 90 while another provided direct evidence of an association between bench press and leg press and improved insulin sensitivity in boys. 91 As for cardiorespiratory health, among normal-weight boys and girls there was an association between increases in handgrip strength and reductions in systolic blood pressure. 47 Another revealed that gains in bench press and leg press strength were linked to systolic blood pressure improvements and markers of heart function in obese boys and girls. 92
National Youth Survey
Although several relationships have been determined in adults between musculoskeletal fitness and health, a lack of studies has resulted in fewer relationships between musculoskeletal fitness and health outcomes in children. Due to a lack of high-quality studies studying these relationships in children, the committee does not recommend specific musculoskeletal fitness test items (to be measured in a health context) for inclusion in a national fitness survey. However, due to evidence found in adult populations, both the handgrip strength and standing long jump tests may be included due to their adequate validity, reliability, and feasibility.79,82,93-96 These tests should not be interpreted in a health context until more research confirms their relationships with health outcomes.
School-Based Survey
Schools should also incorporate the handgrip strength and standing long jump tests in their fitness surveys. The modified pull-up or push-up can also be measured for assessment of upper body musculoskeletal strength and the curl-up for measuring core strength—these are valid and reliable tests although at this time they have not been conclusively related to health in youth.
Future Studies
Studies should continue to address the relationship between specific musculoskeletal fitness items and health markers in youth. Many were not designed to appropriately determine the relationship between musculoskeletal fitness tests and health outcomes (either the intervention was not specific enough or the dosage and duration was inadequate) and others were statistically underpowered. Priority should be given to test items for which there is growing evidence, such as the handgrip or the standing long jump, or others that are promising. Since musculoskeletal fitness is a multivariate construct, the studies should be designed so that a variety of tests are conducted.
Flexibility
Flexibility is the intrinsic property of body tissues, including muscle and connective tissue, which determines the range of motion achievable without injury at a joint or group of joints. Flexibility is also specific; one can have good range of motion at the hips but be limited in his or her shoulders. In adults, studies demonstrating associations between flexibility and health are mixed. Flexibility may enhance postural stability and balance among adults, 70 yet the association between flexibility and low-back pain is less conclusive. 77 Due to its role in sports performance, flexibility has also been studied in its relation to muscle cramps, 97 injury, 98 performance,99,100 postural stability, 101 and delayed muscle soreness.102,103 However, data linking flexibility to more general health outcomes is scarce. Activities that involve stretching have been linked to health outcomes, such as yoga’s association with treating low-back pain,104-106 but these activities also involve other components of fitness (eg, strength, muscular endurance) and therefore it is difficult to tease out the effect of flexibility.
Fitness Tests
Flexibility can be determined through laboratory tests, which measure the angle of joints or their range of motion with goniometers, or field tests. In the United States, the most popular of the field tests are the shoulder stretch, the trunk lift, and sit-and-reach. The reliability of these tests is high, though the validity ranges from low to moderate depending on the test.28,45,77,79,107
Studies in Youth
In youth studies, physical activity programs often result in improved flexibility among youth.108,109 However, there are differences based on age and sex. Girls were shown to be more flexible than boys, across all age groups. 110 Welk and colleagues also found improvements in flexibility through the years for boys, though girls had lower sit-and-reach scores in high school when compared to lower grade levels. 111 The most recent California fitness test also found that more girls than boys meet the sit-and-reach standards and more youth overall meet the standard at upper grades. 112
Though flexibility tests have been present in many youth fitness tests, it has proven difficult to link them to health outcomes due to joint specificity of the tests. One study found that back pain scores in teens improved as flexibility increased. 108 And in a small study of teens with back pain, those exposed to 8 weeks of rehabilitation increased performance with side bends, sit-and-reach, and sit-ups, and lessened their pain intensity. 109 Good flexibility, as measured through the sit-and-reach, was associated with decreased neck tension in boys, but not back pain. 113 Burton et al found that flexibility was not predictive of back pain when tracking adolescents over 4 years. 114 Finally, two studies showed an association between decreases in flexibility and higher skinfold measurements 115 and BMI, 22 but others found no association among these measures.116,117
In youth, the main health outcomes that may be correlated with flexibility include prevention of low-back pain, prevention of musculoskeletal injury, and improved posture. At this time, however, there is little solid data to support a strong link between flexibility and health outcomes in children due to a lack of large-scale studies, an effect of the combination with other musculoskeletal variables, and a high degree of variability among studies.
National and School-Based Surveys
Due to the high specificity of flexibility, it is difficult to correlate a single flexibility test to a health outcome. There is the added difficulty of field tests and their possible inability to isolate the flexibility of particular joints. Due to these restrictions, the committee recommends further research on this fitness component and the use of flexibility tests only for educational purposes. A flexibility fitness test in a national survey of youth is not currently recommended; however, the inclusion of a measure of flexibility, such as the sit-and-reach test, in a school survey may be considered for educational purposes.
Future Studies
Studies in youth should investigate the relationship between specific flexibility items (eg, sit-and-reach and its modifications), either by themselves or in combination with musculoskeletal items, and potential health markers (eg, back pain, posture, injury prevention). Such studies should include stretching interventions specifically designed to produce changes in joint specific flexibility. Since flexibility is a multivariate construct, the studies should be designed so that a variety of tests are conducted. Researchers should investigate the development and validation of a general marker of musculoskeletal systemic flexibility and its relationship to health markers and risk factors.
Interpretation of Results
Developers of fitness test batteries should use age- and sex-specific cutoff scores to determine which individuals are at risk of poor fitness-related health outcomes. Two evaluation approaches have been often used in fitness evaluation: norm-referenced and criterion-referenced standards. 118 In the norm-referenced evaluation approach, a test taker’s performance is compared with his/her peers, often by gender and age. For example, students’ scores might be categorized depending on whether they score below or equal or higher than the 85th percentile of their peers. When the interest is in performance, then the norm-referenced evaluation is appropriate. However, limitations of norm-referenced standards include time dependence, population dependence, discouragement of unfit youth, and favoring genetically gifted and/or punishing disadvantaged youth.
Many of these limitations are overcome with the use of a criterion-referenced evaluation approach, when a test taker’s performance is compared with an absolute criterion (eg, low HDL threshold) related to whether a child meets a minimal needed physical fitness level. Because the criterion is defined independently, it is not affected by changes in a population that occur over time or in level of fitness of the specific population. Cutoff scores should therefore be based on criterion values if available. In their absence, interim values may be used until necessary data are available to establish health-related cut-points. For example, population-based (percentile) values can be extrapolated from the adult population or from standards for other health-related fitness measures. The reader is referred to the final report for further details regarding the derivation and use of cut-points for each fitness category.
Summary and Future Research Needs
Collecting fitness data at both the national level and school/educational level should remain a public health priority. Well-designed research studies aimed at advancing understanding of the associations between fitness components and health in youth should continue to be undertaken. Researchers should ensure that the interventions studied are both specific and sufficient (ie, appropriate dosage and duration) to induce a change in fitness. In addition, studies should be designed so that the effect of potential confounders (eg, nutrition, physical activity, demographic variables, maturity status, etc) can be analyzed. Longitudinal studies should also be conducted to provide empirical evidence concerning how health markers related to fitness track from youth into adulthood. Collecting these data not only helps with setting and achieving fitness goals in our nation’s youth but also promotes it further as a priority for public health.
During 2012, the NHANES National Youth Fitness Survey measured fitness physical fitness in a nationally representative sample of youth for the first time in over 25 years, but unfortunately, biological and health markers such as these were not assessed in the same sample of children. 119 The collection of fitness and health data in the same individuals would have enabled investigators to further confirm whether relationships between specific test items and health markers and risk factors exist. Considerable limitations thus remain in the available research to link specific fitness components and tests to health in youth. As additional research is needed and performed, we will advance our understanding of the health impact of physical fitness, answer remaining questions about fitness test items, and advance the national conversation about fitness in youth.
Footnotes
Acknowledgements
We would like to acknowledge the Centers for Disease Control and Prevention for compiling the extensive literature review, the Institute of Medicine of the National Academies for convening the report committee, and to all the Institute of Medicine committee members for their work on the Fitness Measures and Health Outcomes in Youth report.