Abstract
The study of obesity lends itself to difficulties not only due to our imprecise ability to measure body composition, food consumption, and physical activity but also, even more important, due to complexities involved in defining and conceptualizing obesity. For centuries, obesity has been considered a disease, although researchers and clinicians cannot agree on definitions of “disease” or, if it is one, whether obesity is a disease of metabolism, inflammation, brown fat, chronobiology, the blood-brain barrier, the right brain, or even of infectious origin. The concept of “obesity” as a disease remains controversial to some because not everyone who has excess adipose tissue has any evidence of disease. Obesity, though, has also been considered a sin, a crime against society, an aesthetic crime, a self-inflicted disability, an example of body diversity, a failure in the regulation of energy balance, an appropriate or even inappropriate adaptation to our increasingly obesogenic environment, a genetic disorder, and a psychological/behavioral disorder of overeating involving self-regulation or even addiction. Five major paradigms—medical, sociocultural, evolutionary, environmental, and psychological/behavioral, all with their own subcategorical models—have been identified. All 5 paradigms are required because we are dealing not with “obesity” but with a plurality, the “obesities.”
‘Although studied extensively throughout the years, obesity continues to remain enigmatic, particularly due to the extraordinarily diverse ways it has been conceptualized.’
In their new book, anthropologists McCullough and Hardin 1 (p. 7) write, “When obesity is studied . . . fat [is seen] as a global category of the body that universally means the body is troubled. What if we instead tried to imagine a new relationship . . . by thinking of obesities rather than obesity?” Although there have been literally thousands of publications on all aspects of obesity, we are still far from an understanding of its nature and complexities, perhaps because most researchers and clinicians remain stuck on their own singular concept of obesity. This article expands on McCullough and Hardin’s suggestion and provides a framework for a plurality concept of the “obesities.”
It was almost 50 years ago that Straus 2 called attention to the “many conflicting conceptual models, each of limited dimension,” that have impeded our understanding of obesity. This remains as true today. Throughout the years, researchers, often focusing on one viewpoint, have presented models that have dealt with causation, correlation, and even obesity as metaphor.3-6 Barry et al, 6 for example, explored the role of metaphor, from high individual blame to low individual blame, in public opinion about obesity and found that many of those surveyed accepted the “multi-causal nature of obesity.”
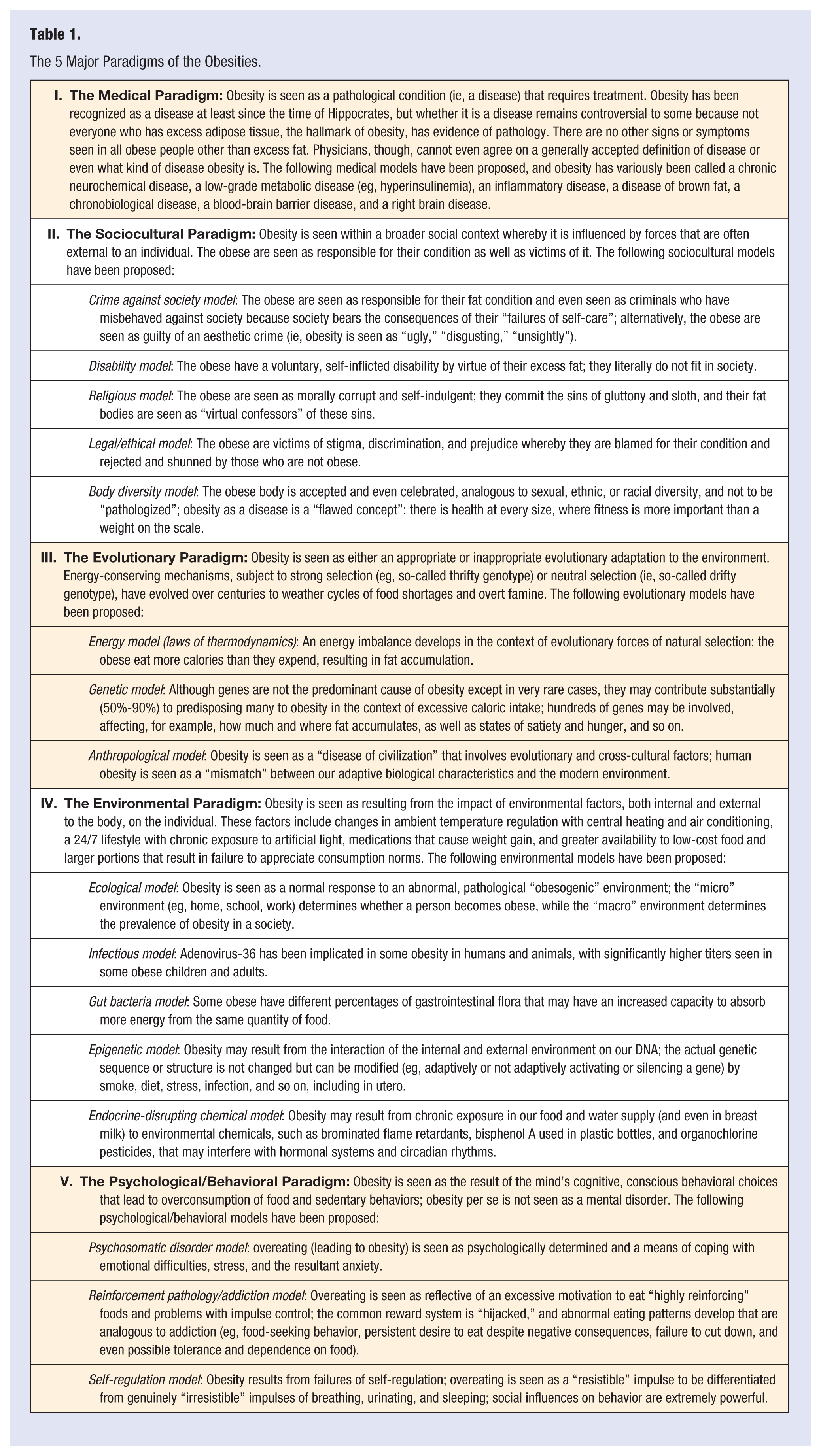
The study of obesity lends itself to extraordinary difficulties due to the imprecise and flawed measurement of food consumption, physical activity, and body composition, including adipose tissue itself.7,8 For a comprehensive discussion of the complexities involved in all aspects of measurement as it relates to obesity, see an earlier article by Karasu 8 in this Journal. Even more important, though, for the purposes of this article, the study of obesity has been hampered by how obesity has been defined and conceptualized.7,8 Five major paradigms of obesity—medical, sociocultural, evolutionary, environmental, and psychological/behavioral, each with its own subcategories—have been identified from a comprehensive review of the literature (see Table 1). A paradigm is a generally accepted pattern or conceptual model that underlies theory and practice at a particular time. In a sense, though, these 5 paradigms are a “museum of past and present” conceptualizations. 9 For heuristic purposes, though, they are presented separately but are not necessarily mutually exclusive, and they frequently overlap. Furthermore, they not only converge and diverge but are even overtly contradictory. All 5 paradigms are needed because we are dealing with “the obesities,” and there is no need to presume a common etiology “for all the failures of such a complex mechanism.” 10 Despite a “virtual shopping list” 11 (p. 137) of “putative contributors” 12 to explain the burgeoning rates of obesity that have occurred worldwide over the past 30 years, obesity remains enigmatic.
The 5 Major Paradigms of the Obesities.
Rittel and Webber, 13 in their classic study on social planning, wrote of the difficulty of defining certain problems and identifying the actions that were required “to effectively narrow the gap between what is and what ought to be.” They described some of the distinguishing properties of what they called these wicked (ie, malignant) problems, including no definitive formulation; no immediate or even ultimate test of a solution; explaining discrepancies in numerous ways, with the choice of explanation determining the nature of the problem’s resolution; no rule or procedure to determine the “correct” explanation; and the analyst’s “worldview” as the strongest determining factor in resolving a wicked problem. Obesity has been considered one such “wicked problem.”14,15 For example, there was a “substantial disconnect” and “limited” frame of reference among different respondents in whether they believed obesity required “individually-oriented interventions” rather than policy-oriented interventions. 16
I. The Medical Paradigm
The medical paradigm focuses on obesity as a pathological state (ie, a disease to be treated). Obesity has been recognized since prehistoric times, but its interpretation over the years has depended on both the culture and science of the time.17,18 Despite more recent (and widely held) thinking to the contrary, the medicalization of obesity is not a new concept.19,20 Although fifth-century Greek physician Hippocrates focused his medical theory on the balance among 4 humors (black bile, yellow bile, blood, and phlegm), he understood that obesity led to a decreased life span.21,119 (p19) Much later, in the 16th and 17th centuries, physicians considered obesity a potentially deadly medical condition.17,20 This view was carried into the 19th century by surgeon William Wadd, who wrote in his Cursory Remarks on Corpulence, or, Obesity Considered as a Disease, “Corpulency . . . is not only a disease itself, but the harbinger of others.”22(p. 53) In the 20th century, Chang and Christakis 23 traced the history of the medicalization of obesity through an analysis of different editions, from the 1920s to 2000, of a classic medical textbook. Although all editions accepted that obesity resulted from an energy imbalance, each edition differed in emphasis, and a model of obesity could change “quite independently of definitive experimental evidence.” Over time, the obese person is cast initially from a “societal parasite” whose obesity results from his or her own aberrant behavior to a “societal victim” whose obesity results more from involuntary genetic factors, environmental influences, and physiological disturbances, with less individual blame or accountability. 23
One of the difficulties about considering obesity a disease is that there is no widely accepted and authoritative definition of disease.18,24-26 Labeling a condition a “disease” has potentially serious implications, for both the patient and even society. The act of diagnosis can link a person to the social system, and disease categories can be used to enforce social norms and define deviance, 27 release a patient from certain obligations, 24 or even confer certain benefits and legal privileges. 28 How a clinician manages a patient depends on whether he or she regards the patient’s condition a “disease” and may lead to unnecessary treatment or possibly no treatment 29 or even whether a patient complies with treatment recommendations because of “increased perceptions of seriousness.” 30
The medicalization process involves both the crusaders who call attention to the problem and mobilize resources and the experts who are the authorities on it.31(p79) It may involve many other interest groups, including the many types of “obesity epidemic entrepreneurs,” 32 such as the “creators, amplifiers/moralizers, legitimators, supporters, and enforces/administrators.” 32 The question, then, maintain David B. Allison and his colleagues, 26 should not be “is obesity a disease” but rather “should obesity be considered a disease” because of the social, political, ethical, and moral aspects involved.
Another problem in considering obesity a disease, according to Heshka and Allison, 25 is that there are no signs or symptoms seen in all obese people other than excess fat—the very definition of obesity—and there is not even a way of predicting who will develop obesity-related problems. 25 Some obese people, for example, have metabolically benign obesity and may not develop any morbidities or earlier mortality typically associated with obesity. “We are therefore placed in the conceptually awkward position of declaring a disease, which, for some of its victims, entails no affliction,” say Heshka and Allison. 25 Furthermore, obesity is defined as the condition of excess body fat, but there is, however, no precise definition of excess and no clear demarcation of normal from abnormal. 33 Just removing fat from a person by liposuction does not improve health. 34
The incidence of obesity is “rooted in its very definition,” and because obesity is defined as a “threshold,” a “relatively small increase in average weight has had a disproportionate effect on the incidence of obesity.” 35 For example, “a minor change in the government’s standard . . . made an extra 30 million Americans ‘overweight’ overnight.” 36 There are conflicting reports, though, on the prevalence of obesity in the United States, particularly related to differences in data collection methods. 37 Although there has been a high prevalence of overweight for years, it has been more recently considered an epidemic,38-40 particularly with its high prevalence in our population and its rapid (and unexpected) increase over the past several decades. 39 Rosenberg makes the point, in his classic delineation of the course of medical epidemics, that epidemics “have always provided occasion for retrospective moral judgment”41(p287) where “susceptibility was not seen as a random accident or as the result of constitutional idiosyncrasy alone,”41(p283) but rather implying that the victim is to blame.
The Council of the Obesity Society 42 and, more recently, the American Medical Association (AMA) have both recognized obesity as a disease, and in the case of the AMA, obesity is seen as a “multi-metabolic and hormonal disease state.” 18 The Report of the Council on Science and Public Health says, “The suggestion that obesity is not a disease but rather a consequence of a chosen lifestyle exemplified by overeating and/or inactivity is equivalent to suggesting that lung cancer is not a disease because it was brought about by individual choice to smoke cigarettes.” 18 The decision remains controversial, and the AMA’s own Council on Science and Public Health, though, argued that it was “premature” to classify obesity as a disease, particularly because body mass index (BMI) is such a “limited tool” for diagnosis. 18
Furthermore, even given that obesity is a disease, researchers cannot even agree on the nature of the “disease” of obesity. From a clinical perspective, it has been called a “chronic neurochemical disease” 43 with a specific etiology; a pathogenesis involving neurochemicals in the brain; a pathology involving enlarged, abnormal fat cells; and a pathophysiology involving changes in the secretory products of these enlarged fat cells. 43 It has also been considered a disease involving increased insulin (hyperinsulinemia)44,45; a chronic, low-grade inflammatory disease46,47; a brown fat disease 48 ; a chronobiological disease49,50; a blood-brain barrier disease 51 ; and a right brain disease 52 involving dysfunction of the prefrontal cortex that leads to more reflexive rather than reflective eating. The concept, though, of the obese as “brain damaged” is controversial. 53 In her classic discussion of illness as metaphor, Sontag wrote, “The notion that a disease can be explained only by a variety of causes is precisely characteristic of thinking about diseases whose causation is not understood . . . it is diseases thought to be multi-determined that have the widest possibilities as metaphors for what is felt to be socially or morally wrong.”54(p61)
II. The Sociocultural Paradigm
This paradigm places individual behavior within a broader social context as it considers economic, cultural, and political determinants and asserts that obesity is a societal disease. Here obesity is seen as somewhat influenced by “forces external to the individual” 55 and may even been seen as a mechanism for “signaling and maintaining social difference.” 56 Furthermore, since society tends, until perhaps very recently, to ignore the needs of the obese, they are made to feel that they do not “really fit” when seats in theaters, planes, and buses are too narrow. 2
Crime Against Society Model
This model holds that the obese are responsible for their fat condition and are seen as criminals. They are seen as committing, at the very least, a “misdemeanor” or even a “felony,” depending on the degree of obesity (p. 93). 57 In other words, they are committing a “crime against society” 58 “because society has to pay for their consequences” 58 of “misbehavior” 58 (ie, “failures of self-care” 58 ). Apparently, though, it is “less criminal to be overweight if one shows others that one is attempting to diet by being an ascetic martyr at a dinner party than if one gorges” and is caught in the act of an eating crime.”57(p92)
Although obesity has been viewed differently throughout the years in different cultures and even coveted in some as a sign of “beauty and desirability,”57(p95) it has also been seen that the obese are committing an aesthetic crime, that is, a crime of “ugliness.”57(pp95,97) Obesity is seen as “unsightly” 59 as well as “disgusting” 60 and “unaesthetic” and “ugly,” even among physicians surveyed. 61
Disability Model
This model maintains that those overweight or obese are completely responsible for the condition and “lacking in an ability to exercise personal control.” 61 In other words, obesity is a “voluntary, self-inflicted disability”57,62 or even a “social disability.” 61 The classic studies of Goodman et al 63 included overweight as not only a type of disability but the worst of those considered, including being in a wheelchair. In their discussion of the Goodman et al research, Maddox and his colleagues 62 noted that they were originally attracted to that study because of “the frank identification of overweight as a type of disability.” Of note is that the AMA, despite voting to make obesity a disease, opposed the effort to make obesity a disability. 18
Religious Model (Obesity as Sin)
Even though the medical model has existed for centuries, over time, obesity has also taken on moral and religious tones. It is seen as evidence of self-indulgence, hence “at least faintly immoral and inviting retribution.”
64
In other words, the obese are “morally weak,”
61
and a fat body is seen as a “virtual confessor” of sins of the flesh.65(p80) Not much is said about gluttony, though, in either the Old or New Testaments.66(p251) The classic definition of gluttony is found in Paul’s letter to the Philippians, and over the years, gluttony became one (along with sloth) of the Seven Deadly Sins of Christian theology, as Augustine (fifth century
Over the years, this model has persisted. For example, the “major themes of the confessional, the testimonial, and redemption for one’s sins of cheating” are seen in a discussion of group dieting.57(pp85-86) “In their redemption, group dieters seek to be saved from their eating sins and to have their guilt atoned for by the group leader and the scale.”57(p86) Even the weekly fee may be seen as some sort of penance and “acknowledges their state of sin.”57(p86) More recently, with people considered responsible for their own health, those who are obese have “moral failings,” 4 and there is a “moral responsibility” to choose an appropriate diet and make “correct” choices when it comes to lifestyle choices, with “foods and behaviors considered good or bad.” 68
Legal-Ethical Model
This model focuses on the victimization of obese people, who are subject to prejudice and even overt discrimination, and on the role of stigma, which is a “cultural phenomenon” (ie, it needs a “cultural script”). 69 Stigma becomes a “potent form of social control.” 69 There is no widely accepted definition of stigma, 69 but it is characterized by “exclusion, rejection, blame, or devaluation that results from experience, perception, or reasonable anticipation of an adverse social judgment about a person or group.” 70 The individual response to stigma is usually “concealment,” but that cannot be done with the obese. 69 Researchers have questioned whether it is ever morally acceptable to foster stigmatization (ie, “good stigma”) in efforts to control behavior for public health, 71 as, for example, when it was used in the public health campaign against smoking. 69 The Supreme Court, in Robinson v California, ruled on stigma in a case involving alcoholism: “The notion of stigmatizing a person because of a disease or addiction is offensive at the outset . . . if we allowed sickness to be made a crime and permitted sick people to be punished for being sick. This age of enlightenment cannot tolerate such barbarous action.” 72
Body Diversity Model
This model asserts that “as a disease, obesity is a flawed construct,” 73 and even though there are obviously medical risks associated with obesity, these risks have been “blown out of proportion.”5(p17) They are the “skeptics” rather than “alarmists” 74 and believe that even the Centers for Disease Control and Prevention’s (CDC’s) red “obesity maps” convey a notion of a “spreading infection” and give the “impression of danger from an epidemic ‘hot zone.’” 73 Furthermore, using the word obesity “implies that fat bodies are pathological.”5(p5) Fat activists have “reclaimed the word fat, much like the civil rights movement re-appropriated the word black and the gay movement reclaimed queer” 4 and assert that fatness is a form of diversity, akin to race, sex, or ethnicity. 4 They object to the notion of overweight as a “pre-disease state” 75 or a “proto-disease” “occupying a position somewhere between warning signal and pathology,” 27 and “now a legitimate point of intervention as it is a precursor for the unhealthy disease state of obesity.” 75 Timmermans and Buchbinder, 76 in their discussion of incidental findings in the genomic literature, have described the concept of “patients in waiting” who “live between sickness and health.” Whether those who are overweight or even those who have metabolically benign obesity (at least when observed cross-sectionally) are in fact “patients in waiting” often remains to be seen.
Some in the body diversity camp believe there is “disease mongering’” about obesity where there is “widening the boundaries of treatable illness in order to expand markets for those who sell and deliver treatments.” 77 In other words, “the social construction of illness is being replaced by the corporate construction of disease.” 77 One contributing factor has been the development of household scales to measure weight so that people can make their own diagnosis.78(p70) Jutel considers “overweight-as-disease” a “marketer’s ploy made in heaven:” “Here we have a self-diagnosable condition that engenders a population-wide-preoccupation with self-surveillance, treatment, prevention, and cure.”78(p74) Those who subscribe to the body diversity model contend that fitness is more important than weight on a scale 34 and there can be “health at every size.” 4 The problem, though, is “weight per se was never what mattered . . . what makes shape and size problematic is they are often harbingers of ill health. . . . What matters here is health. Everything else is fashion.” 79
III. The Evolutionary Paradigm
This paradigm focuses on the importance of either appropriate or inappropriate evolutionary adaptation to the environment. Over the years, energy-conserving mechanisms, consistent with the laws of thermodynamics, have evolved genetically to regulate weight in the context of food shortages.
Energy Model (Laws of Thermodynamics)
This model emphasizes that obesity results from a failure in the regulation of energy balance,55,80-82 based on the laws of thermodynamics. The analogy of edema (ie, the consequence of positive fluid balance or fluid retention) can be applied to the consequence of positive energy balance or calorie “retention.” Just as the assessment of edema requires an evaluation of fluid balance, obesity “requires a comprehensive evaluation of factors potentially affecting energy intake, metabolism, and expenditure.” 83
The first law of thermodynamics (ie, the law of the conservation of energy), when applied to weight control, would hold that the amount of food eaten (ie, calories ingested) does not match the number of calories expended: when we take in more calories than we use, those excess calories are converted to fat.43,83 The problem, though, is that the human body is “not a perfect engine and thus the thermodynamics may not be so pure” (ie, we are never in energy balance). 80 In other words, for some, a calorie is not always a calorie, such that 2 diets with the same number of calories may, in fact, lead to differences in weight loss. 84 And there may be a “misunderstanding” of the laws of thermodynamics to expect a calorie is always a calorie. 85
That obesity results from an energy imbalance is generally accepted, but that still does not tell us about how we regulate food intake or why weight loss stops and weight regain often occurs or why some drugs cause weight gain and others cause weight loss, and so forth. 80 Clearly, genetic, sex, perinatal, developmental, dietary, environmental, neural, and psychosocial factors are also involved. 86
Genetic Model
To say that obesity involves genetics does not say much because any disease can be considered genetic. In other words, any disease “directly or indirectly” involves our genes, but genes are not the “predominant cause” of obesity, except in very rare cases. 84 After all, people do not become obese if they are starved; genetics may predispose someone to obesity but only in the context of excessive calories, 87 and “one should keep an open mind regarding the possibility that the heritability values (from 50 to 90% by some estimates) are highly inflated.” 88 It is highly likely that many genes with “small effect sizes” are involved, 88 perhaps hundreds according to human genome obesity studies. 89 For example, more than 40 genes affect body weight and body mass index, 13 genes for body composition and fat distribution, and 4 genes for energy expenditure. 90 Evidence suggests that genes are also involved with hunger, satiety, and food intake, and genetic variation increases the risk of becoming severely obese. 91
Evolution, though, favors genes that give advantages rather than disadvantages, 92 and so researchers have wondered why, “in the space of 50 years, we have become an obese species.” 92 In fact, “For the first time in human history there are more obese and overweight people on the planet than people suffering from malnutrition.” 92
More than 50 years ago, James Neel speculated about a “thrifty genotype” 93 that developed during the hunter-gathering existence of man (ie, for the first 99% or more of human life), when there was often feast or famine. When food was scarce, and food shortages were an “inevitable fact of life throughout most of human history,” 94 we developed an “important energy conserving mechanism” to weather famines. 93 Neel later came to disavow this original genotype hypothesis as “a grossly overly simplistic view of the physiological adjustments involved in the transition from the lifestyle of our ancestors to life in the high-tech fast lane.” 95 He and his colleagues labeled diseases such as obesity as “syndromes of impaired genetic homeostasis” or, more colloquially, the “civilization syndromes” or the “altered life style syndromes.” 95
Anthropological Model
A subset of the evolutionary paradigm is the anthropological model, which involves “both an evolutionary and a cross-cultural dimension,” 94 and it accepts the allocation rule, which recognizes that organisms must allocate finite time and energy to a range of competing functions, such as growth, maintenance, reproduction, or energy storage. 96 Both a genetic and a cultural predisposition to develop obesity may result from the same evolutionary factors: “first, traits that cause fatness were selected because they improved chances of survival in the face of food scarcities, particularly for pregnant and nursing women; second, fatness may have been directly selected because it is a cultural symbol of social prestige and an index of general health.” 94 Obesity is seen not just as a “disease of civilization” but seen only in certain civilizations where even poor people have enough food to develop obesity. 94 Furthermore, civilized societies overcome seasonal variation in food availability by developing methods to store foods, as well as develop economic diversification, and cultivate social relationships among groups in other areas. 94
With the development of civilization, though, came infectious diseases, such as tuberculosis and malaria, that were life-threatening. 97 Fat, with its hormones such as leptin and adiponectin, is seen as an “auxiliary innate immune system,” and the metabolic syndrome evolved as an extension of that system to protect humans from these devastating infections that kill far more (and much more rapidly) than starvation. The hypothesis is that “the link between fat and inflammation is an evolutionary anachronism” that loses its value with the advent of much of civilization’s ability to fend off these life-threatening infections such as tuberculosis. 97
An alternative theory is that civilization’s genetic predisposition to obesity has not been subject to strong selection but rather has arisen by “neutral evolutionary processes” such as “genetic drift” and hence the “drifty hypothesis.” 98 This theory maintains that there are different evolutionary pressures involved for weight, with the lower limit related to risks of starvation and an upper limit set by a risk of predation. 98 In fact, humans evolved the social behavior of banding together as a means of detecting and protecting each other from predators, and likewise, humans’ “discovery of fire and their use of tools as weapons seriously reduced any predation pressure.” 98 But mutations in genes occur at random, and some are “unfortunate” in this “genetic lottery.” 99
In general, human obesity developed from a “mismatch between adaptive biological characteristics of our species and the modern environment, which has changed dramatically from the one under which we evolved.”100(p5) In other words, “human obesity is an inappropriate adaptive response to modern living conditions” and has led to “significant disadvantages” in our current environment.100(p11) Obesity, then, is not seen as “pathology” but rather as “inappropriate adaptation,” 100(p11) and the human “biological propensity” for weight gain is related to humans’ large, metabolically “expensive” brains, as well as “selective pressure on fetal and maternal metabolism to favor fat babies.”100(p307)
IV. The Environmental Paradigm
This paradigm emphasizes the importance of environmental influences, both internal as well as external, to the human body.
Ecological Model
The ecological model proposes that obesity, rather than an abnormal response, is actually a “normal response to an abnormal, pathological, i.e. obesogenic, environment,” and this response is responsible for the “obesity pandemic.” 101 This “obesogenic” environment can be divided into the macro-environment, involving technology, social norms, and policy, as well as the micro-environment of work, home, school. 101 According to Egger and Swinburn, 101 it is the macro-environment that determines obesity’s actual prevalence in a population, whereas the micro-environment, in conjunction with both a person’s biology and behavior, determines whether a particular individual will become obese. One of the major “drivers” of the obesity pandemic in the past 30 or 40 years is change in the delivery of food worldwide, although sociocultural, economic, and even transportation differences throughout the world “produce wide variation in obesity prevalence recorded across populations.” 102 Weight gain has also been seen as “collateral damage” in the “physiological struggle against modernity.” 103 As such, it should be seen as an “adaptation that ultimately facilitates body energy storage in order to reestablish a new homeostatic state.” 103 Obesity, then, is the result of “chronic exposure to an obesogenic lifestyle” 104 and a “disease ‘outside’ the body, deriving from an inappropriate food supply and marketing system, producing a niche to which individuals then vary in their susceptibility.” 104 Furthermore, obesity can be viewed in the context of a “life-history theory” 104 —namely, that the body’s finite energy must go toward “competing functions” (eg, growth, reproduction, maintenance, and even immune function), and excess adipose tissue “buffers such trade-offs.” 104 The food industry, though, focuses on the “irresponsibility of individuals” rather than “corporate behavior or weak or counterproductive government policies” in its attempt to avoid employing government action as a means to combat obesity. 105
The environment, though, has changed considerably over recent years. Allison and his colleagues 12 describe many other contributors to the global burgeoning rates of obesity, including changes in our ambient temperatures with air conditioning and central heating, a 24-7 lifestyle with considerably greater exposure to ambient (artificial) light, use of medications that affect weight, and smoking cessation.
On a more individual level, Wansink106,107 has found that food consumption can be considerably and unknowingly affected by cues in our environment, including the variety and how food is presented, the size of the plate, the portion served, or even its packaging and the effort involved to obtain it. Even the food environment, such as background music, lighting, or the presence of other people, 106 may affect how much people eat. Furthermore, people do not appreciate these cues “perceptually suggest to us that it is more appropriate, typical, reasonable, and normal to serve and eat more food.” 107 In other words, people eat more with their eyes than with their stomachs, and this influences “consumption norms.” When portion size increases, Wansink has found that people become considerably less accurate in appreciating how much they are actually eating—that is, they have decreased “consumption monitoring.” 107
Infectious (Viral) Model
Some researchers, in efforts to explain the doubling and in some cases tripling rates of obesity, particularly in the past 30 years, have hypothesized that a true infectious epidemic may be involved—“this rapid spread is compatible with an infectious origin.” 108 For years, there have been anecdotal reports of viruses that have caused obesity in animals (eg, chickens, mice, primates), including the canine distemper virus, Borna virus, and several adenoviruses.108-111 To date, one human virus, the adenovirus 36, has also been implicated in human obesity, with significantly higher titers (3-fold higher) found in some obese children and adults (including discordant twin pairs) compared with nonobese individuals. 109 (For a literature review of animal and human studies, see Mitra and Clarke. 110 ) The work, to date, does not prove causation, and it is difficult to ascertain how much of a role viruses play in causing some forms of obesity in humans, but years ago it was preposterous to suggest that peptic ulcer was caused by bacteria (Helicobacter pylori). 111
Gut Bacteria Model
Another intriguing environmental model involves gut flora from the human intestinal tract. The science is still in its infancy and was actually first reported only in 2006. 112 There is speculation that obese people may have a genetically based “increased capacity to absorb energy from their diet” due to the percentages of certain bacteria in their gastrointestinal tracts. In other words, the same food yielded more calories in the obese than in those of normal weight. Factors related to host genotype may be important in determining their bacterial composition, with changes in the diet affecting bacterial cultures. 112 For example, culture methods used to analyze fecal bacteria in both obese and normal-weight participants found that obese participants had fewer Bacteroides than those of normal weight. 113 Furthermore, there is speculation that altering the amount of these gastrointestinal bacteria may lead to weight control in certain obese people. 113 More recently, work has been done with fecal transplants from lean to obese mice, in coordination with changes in diet, to influence gut flora. 114
Epigenetic Model
This model involves the interaction of the environment—both internal and external, including in utero—on our genetic makeup. While not changing a gene’s sequence or structure, epigenetics involves modifications, such as either activating or silencing a gene, and may be inherited from one generation to another. These modifications can be adaptive or maladaptive. 115 Choudhuri 115 describes epigenetics as “an editorial hand that edits and modifies the language of DNA” and has “provided a molecular basis for explaining the ‘nurture’ element of the ‘Nature (genetics) versus Nurture’ (environment) debate.” Although the person’s genome is set at conception, his or her internal environment may be constantly changing and interacting with the genome, 116 and chemicals, smoke, diet, inflammation, stress, and infection may affect the DNA. A metabolic “obesogenic environment” in utero may contribute to increased susceptibility to later obesity: both overnutrition and undernutrition (eg, seen in the natural experiment of the European famine during World War II) may lead to metabolic disturbances and the risk for later diabetes and obesity. 92
Endocrine-Disrupting Chemical Model
Another model that has surfaced in recent years is the relationship of exposure to environmental organic pollutants, such as dioxins, bisphenol A (used in the manufacture of plastic bottles), brominated flame retardants, phthalates (used in shampoos, cosmetics, and nail polish), polychlorinated biphenyls, and organochlorine pesticides, to the obesity epidemic. 117 These environmental pollutants have permeated our environment, including our food and water supply and even mothers’ breast milk. These are endocrine-disrupting chemicals that may be interfering with our hormonal and circadian systems. The data are contradictory, with “divergent interpretations of individual studies” leading to different conclusions. 117 Studies are ongoing. 118
V. The Psychological/Behavioral Paradigm
This paradigm focuses on the important role of the human mind in obesity. Back in the 1960s, researcher Ancel Keys 60 called attention to the importance of psychological/behavioral issues in obesity: “Plenty of patients insist they want to reduce, know that calorie imbalance is the problem . . . and still cannot, or at least do not, reduce. Obviously psychological as well as dietetic problems must be solved.” In general, because there are many homeostatic systems in place to regulate weight under most conditions, researchers have questioned why “some individuals slip the constraints of this highly regulated system and become obese? In fact, we do not have a definitive answer to this question.” 119 Obesity is at “once the prototype model of a complex genetic disease and a product of life-style choice. This apparent paradox has led to the development of two distinct fields of obesity research, one biological and one psychological (i.e. what makes people over-consume and or adopt sedentary behavior).” 120 Even with a highly regulated system, people become obese for reasons that remain unclear.119,121 Whether people exercise less and eat more because of “biological makeup” or “conscious choice 121 is open to question. All of the following models involve the behavior of overeating.
Psychosomatic Disorder Model
One of the earliest models of obesity was proposed by Kaplan and Kaplan in the 1950s 122 that stated “the overwhelming majority of cases of obesity are not caused by any organic disorder of metabolism . . . but simply the result of overeating, which is caused largely by emotional disturbances that abnormally increase the intake of food.” 122 The authors’ conclusion was that the “somatic condition” of obesity was predominantly “psychogenically determined” but “multi-causal in origin” and “may be said to be not only the most omnipresent psychosomatic disorder but also probably the most significant.” 122 Genetic and biochemical regulatory mechanisms that disrupted homeostasis were postulated, but essentially a person’s excessive eating was psychologically determined as a means of coping with emotional difficulties and decreasing anxiety. 122
Reinforcement Pathology/Addiction Model
Some researchers who accept both genetic and energy balance models for obesity appreciate there is a behavioral component: “human obesity appears less a metabolic than a neuro-behavioral disease.” 91 After all, humans, over time, make cognitive, conscious, although perhaps impulsive, decisions to eat more calories than they expend. 123 When, though, there is a combination of excessive motivation to eat “highly reinforcing” foods (eg, foods high in sugar, fat, and salt) and problems with impulse control, there is reinforcement pathology, a term used in the addiction literature. 123 There are similarities between drug addiction and obesity: both involve abnormally enhanced “saliency value” of the reward (either drugs or food) “relative to and at the expense of others,” and both are mediated by the dopamine reward system.124-126 In effect, the common reward circuitry in the brain is “hijacked” to “cause appetitive behaviors to go awry.” 124 There is even speculation that “obesity-associated inflammation” affecting the brain may promote addictive behaviors to drugs and alcohol, as well as to foods. 126 Unlike drugs and alcohol, though, this addiction model is complicated because there cannot be total abstinence from food since obviously it cannot be eliminated. 126 Although researchers can “recognize a behavioral syndrome” (eg, food-seeking behavior), not all accept an addiction model, except perhaps in cases of abnormal eating disorders, such as binge eating. 127 Ziauddeen and colleagues 127 acknowledge, for example, that while features such as a persistent desire, unsuccessful attempts to cut down on use, and continued use despite negative consequences can apply to an addiction model of overeating, tolerance and withdrawal, as seen more consistently with addictive drugs, are not necessarily seen with food.
A study of more than 650 Canadian adults in the general population, though, found that food addiction, including tolerance and withdrawal, was prevalent in 3% of men and 6.7% of women in that sample. 128 Here food addiction was assessed by the 27-item Yale Food Addiction Scale that is based on substance use criteria and was significantly correlated with greater body weight, waist and hip circumference, and percentages of fat as measured by dual-energy x-ray absorptiometry scans. 128 In other words, this study found direct evidence that food addiction is strongly associated with obesity in this general study population. 128
An addiction model that incorporates an abnormal eating pattern, though, for what is considered “nonhomeostatic eating,” whether related to an actual eating disorder (eg, bulimia, binge eating) or disordered eating patterns (eg, skipping meals, eating most calories at night), has its own challenges. 129 For example, quantifying how much weight gain is required, as well as the time period and circumstances involved, is problematic, and terms such as food abuse or food dependence and even user or nonuser (ie, terms used in the language of addiction) are difficult to apply. 129
It was suggested that obesity be included in psychiatry’s recently published fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a mental disorder 130 because some kinds of obesity derive from an “excessive motivational drive for food,” but it was ultimately not included by the DSM-5 task force as a mental disorder, 129 even though obesity is “strongly influenced by behavior.” 129
Although there may be “obesity phenotypes that are caused by a mental disorder,” there was just “insufficient evidence” at this time to include obesity in the DSM-5, and it was ultimately rejected as a psychiatric diagnosis. 131 Rather, obesity is considered a “heterogeneous condition with a complex and incompletely understood etiology.” 131
According to Devlin, 129 “cultural forces” that tend both to increase energy intake and decrease energy expenditure result in a “mismatch between the two,” and hence obesity can be considered a “cultural disorder of sorts,” rather than a psychiatric disorder.
Self-Regulation Model
The focus of this model is that people have more control over their behavior than they may believe, but failures of self-regulation (ie, control over their behavior and emotions) are involved in personal and social problems such as alcoholism, drug addiction, cigarette smoking, and some forms of obesity.”132(p3) This model also holds “social influences on eating are extremely powerful . . . we regulate our intake with reference to the intake of others” and self-regulation “may be tantamount to regulation by others.”133(pp496,497) Self-control enables humans to be flexible and to stop what they are doing in the middle, which generally distinguishes us from most animals.134(p310) Baumeister 135 differentiates “genuinely irresistible impulses” (eg, breathing, urinating, sleeping) from resistible ones (eg, eating, shopping). Say Baumeister, “Claims of irresistible impulses are popular among people whose self-control has failed, but over the years I have become increasingly skeptical of such claims.” 135 In other words, “most claims of irresistible impulses are more a matter of rationalization than of genuinely being helpless against strong desires.” 135
Concluding Remarks
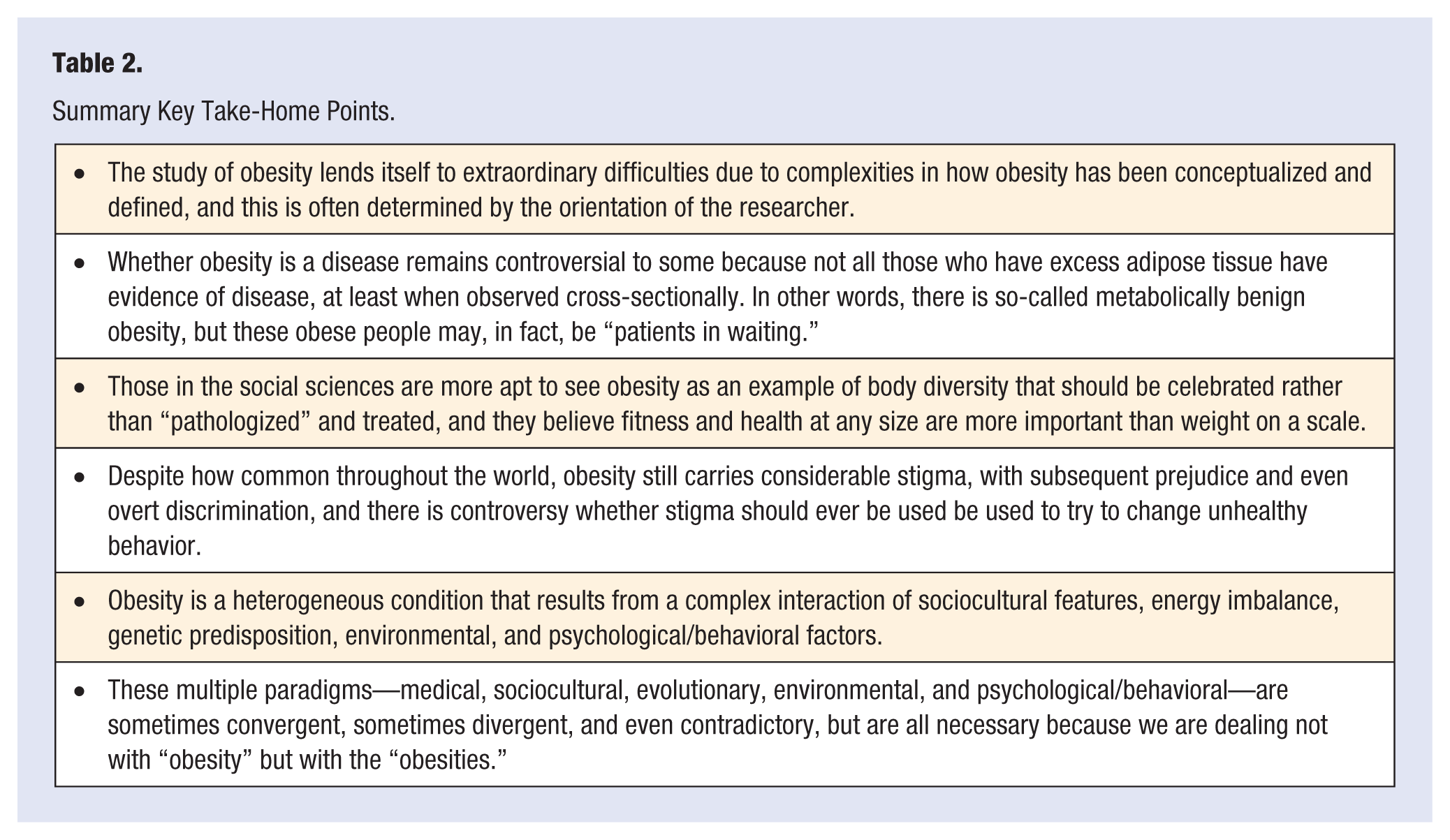
Although studied extensively throughout the years, obesity continues to remain enigmatic, particularly due to the extraordinarily diverse ways it has been conceptualized. These conceptualizations have often varied with the orientation of the researcher (see also Table 1). Most investigators, though, accept that energy balance (ie, calories in, calories expended) is involved as the basic substrate and that underlying genetic predispositions make some people, given the same environment, much more susceptible to weight gain than others. Physicians of all specialties accept a medical model that views obesity as a disease, although they cannot agree on the nature of the disease itself. Those in the social sciences are more apt to see obesity as reflective of body diversity since not all those who are obese or overweight have evidence of disease or dysfunction (ie, there is metabolically benign obesity), and these social scientists focus on fitness and health at every size. Those in the legal profession focus on the victimization of the obese and the notion of stigma, whereas those with a religious orientation may see obesity, with the symptoms of gluttony and sloth, as evidence of moral failings and even sin. Those in the evolutionary field view obesity as inappropriate adaptation to changes in our environments over time. Policy makers see obesity as appropriate adaptation to our increasingly obesogenic environment with contributions from excessive portions of food, medications that lead to weight gain, increased exposure to light, toxic endocrine-disrupting chemicals, or even exposure to viruses, among many others. Those in the mental health profession view obesity as a behavioral disorder involving addiction and abnormal patterns of eating, as well as failures of self-regulation. These 5 paradigms—medical, sociocultural, evolutionary, environmental, and psychological/behavior, all with their own subcategories—may not be reducible to a single integrated paradigm (see also Table 2). They are complementary and convergent, divergent and overtly contradictory, and even seemingly unrelated to each other. They are the “obesities.”
Summary Key Take-Home Points.