
Abstract
This article explores and reviews the available evidence pertaining to lifestyle, disease, and economic losses in the workplace. The literature shows clearly that higher levels of health risks and behaviors lead to the development of disease and moving to a high-cost status. The data suggest that those individuals with lower health risks and those individuals who achieve a reduction in health risks and unhealthy behaviors result in lower probability of disease and high health care costs. The business case for wellness and prevention is also discussed, as is the concept of investing in health as opposed to a strict focus on health care cost reduction. Furthermore, additional determinants of health such as the social–emotional states and positive characteristics of the individual and of the environment and culture are described. Since health is much more than simply the absence of disease, the members of the College of Lifestyle Medicine are encouraged to expand their interests and research inquiry and efforts in evaluating, supporting, and treating these areas. Physicians play a special role in helping individuals improve their healthy behaviors and knowledge of these lifestyle factors will add significantly to their capacity to serve patients. It is very clear that there are growing research, prevention, and treatment opportunities for members of the College of Lifestyle Medicine. It was demonstrated that there is sufficient evidence that justifies the College of Lifestyle Medicine, as observed by the content and quality of the information shared at the conference in Arlington, Virginia in October 2013.
‘What is needed is a transformational system if organizations desire to create a healthy workplace and workforce.’
Introduction: Shared Values Shared Results
When most individuals think about health and economics they almost immediately associate health with the cost of health care and the absence of illness. Some of the discussions in this article are presented to separate health from health care, costs from investments, and health from the absence of disease. In the case of illness and the precursors to illness, costs track with health care. In the case of health, we separate costs of health care from investments in health. After reading this article, we believe you will agree with these definitions.
Many organizations have offered wellness and prevention programs as tactics to influence health and economic outcomes but with fair to good results. To move to an optimal level of performance, more system-level initiatives should be implemented consistent with other enterprise initiatives. What is needed is a transformational system if organizations desire to create a healthy workplace and workforce. 1 The Zero Trends System described in the referenced book builds on a 5-pillar framework and was designed as a model for organizations desiring to achieve outcome measures relevant to a thriving, healthy, high-performing, and sustainable workplace and workforce.
The following statements are characteristics of a thriving, healthy, high-performing, and sustainable workplace and workforce.
Shared values and shared results, including shared pride and successes
Cultivate an energized workplace environment and culture
Support healthy, engaged, and thriving workforces
Retain and attract talented employees
Promote healthy families and communities
Natural Flow of Employed Persons: Health Risks and Behaviors
Physicians and other health professionals most often look at preventive services as the first step in a health initiative in their patients, employees of an organization, or citizens of the community. The second step is to use the typical medical methods to treat high risks, symptoms, and illness. This is how physicians were trained and it is a useful view from the lens of the medical model. However, there is another perspective that the College of Lifestyle Medicine has adopted, that is, the use of lifestyle as a medicine to maintain or regain the health of individuals in the population.
The typical prevalence of high health risks and behaviors of employees is shown in Table 1. The percentages represent the approximate levels of risks in all organizations. The data have changed ever so slightly over the past 20-year period. Most organizations have an employee profile with a high percentage of individuals with high body mass index, high stress levels, and low levels of physical activity and low safety belt use in vehicles. The natural target of physicians and wellness practitioners is the high-risk individual and those with chronic conditions (the typical medical/wellness model).
Prevalence of Risks and Behaviors in a Working Population.
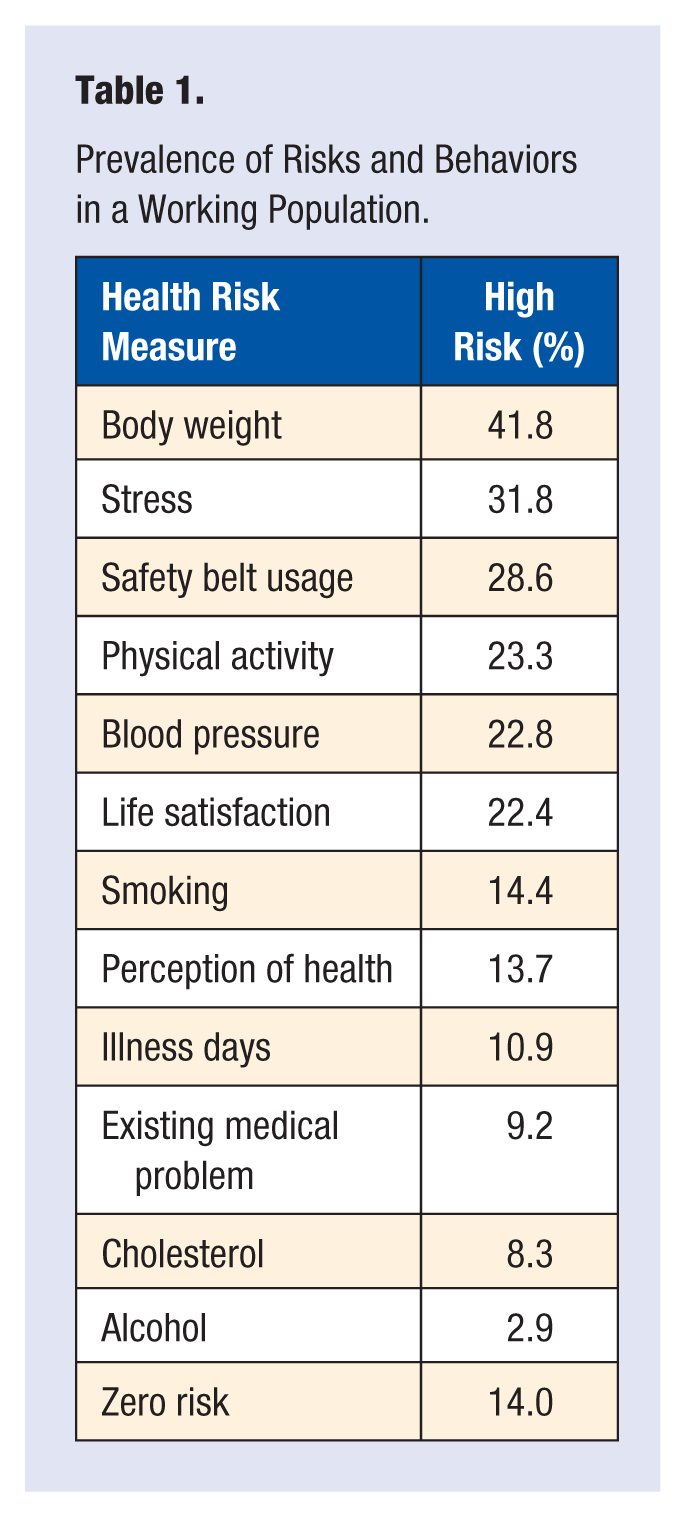
Figure 1 indicates that the percentage of individuals with at least 1 of the 5 diseases (diabetes, heart problems, cancer, past stroke, or bronchitis/emphysema) increases with age and risk status. It should be noted that the percentage of the population of low-risk individuals older than 65 years is less than the percentage of high-risk individuals younger than 45 years. This is consistent with the concept that low risk status is associated with a lower percentage of one or more of the 5 diseases.
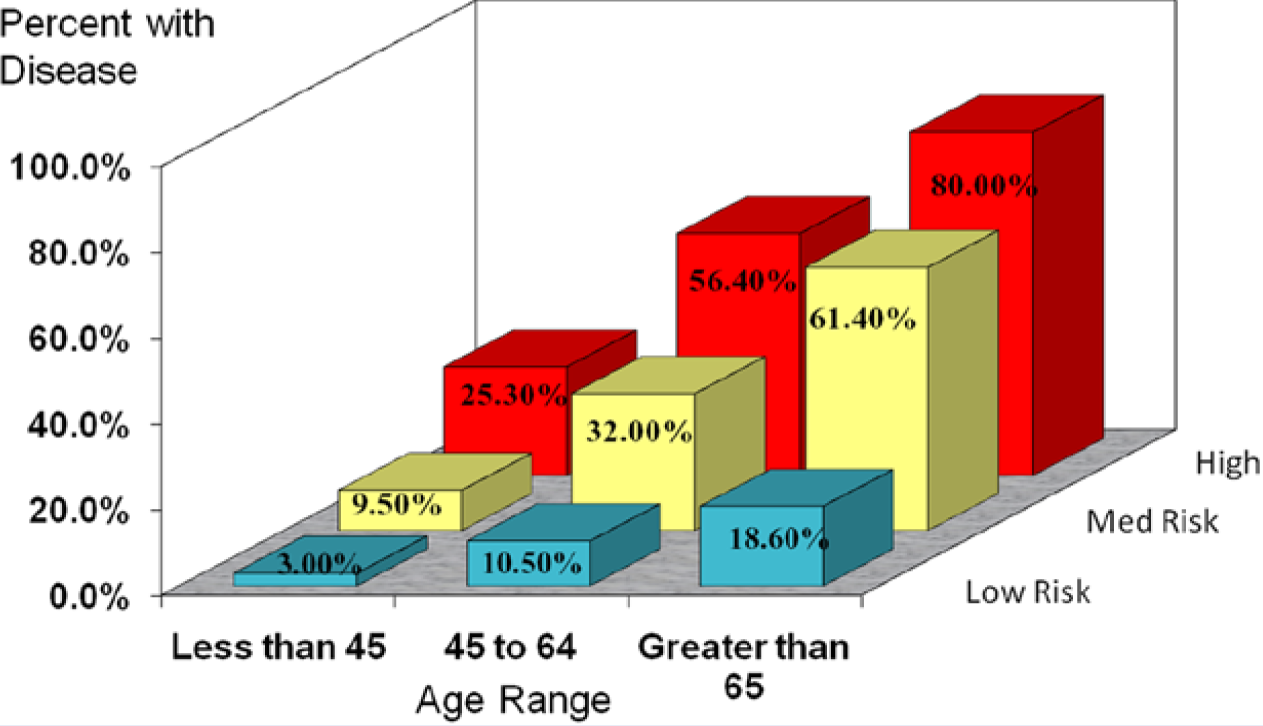
Disease (heart, diabetes, cancer, past stroke, bronchitis/emphysema) associated with risks.
The data in Figure 2 give us a longitudinal picture of the same population over a 3-year period (natural flow of the population). Individuals are grouped into the 3 overall risk-status levels (low, medium, and high). Within each of the 3 risk-status levels, the top rectangle shows the number of individuals in that risk status at year 1. The bottom rectangle is the number of individual in that risk status at year 3. The arrows indicate where the year 1 individuals migrated by year 3. Notice that low-risk status individuals decreased over the 3-year period while the number of high-risk status individuals increased. The overall natural flow of a population is to high risk as people age. That is, if we do nothing to intervene in a population, the flow of individuals will be to high risk.
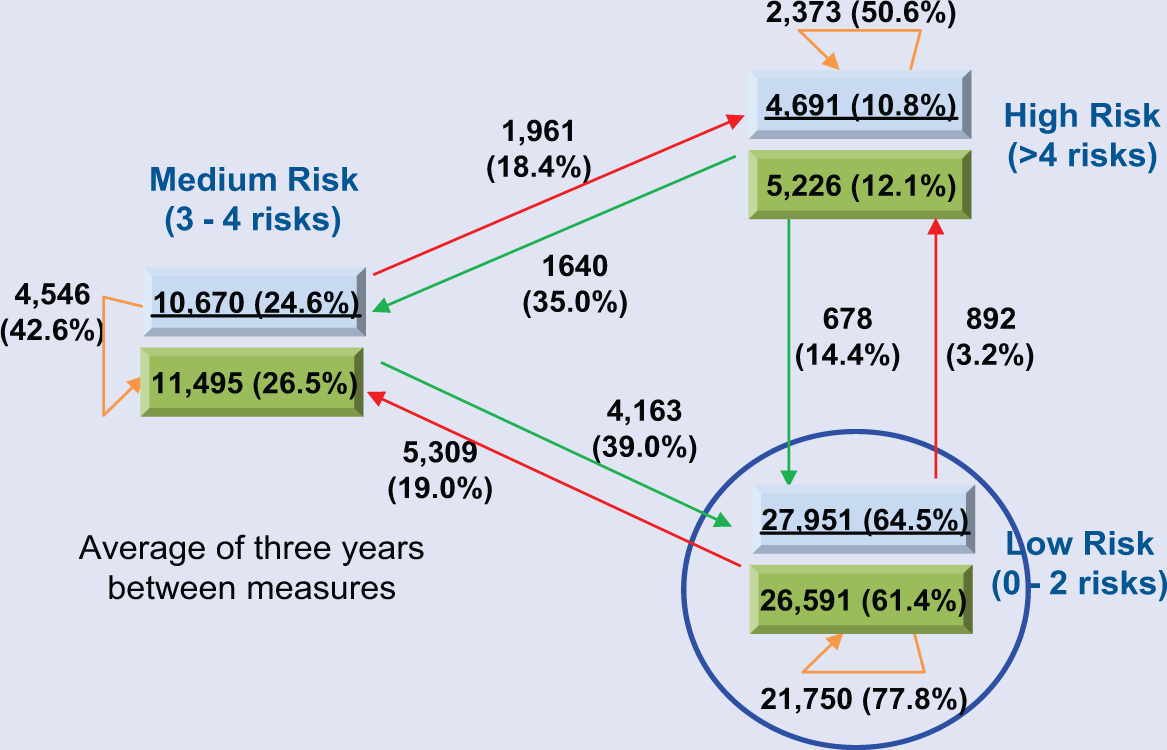
Natural flow of a population by levels of risks. The data for Year 1 are in the top boxes and Year 3 data are in the bottom boxes in Year 1.
Business Case for a Wellness and Prevention Approach
The data in Figure 3 show the relationship of the overall risk categories with age and medical plus pharmaceutical costs. It is clear that costs and risks are strongly associated. Using this definition of risk status, the data show the interaction of age, risk level, and medical/pharmaceutical costs. Costs are higher with age and with high risk levels. The line in the graph indicates the natural flow of a population with age and risk levels.
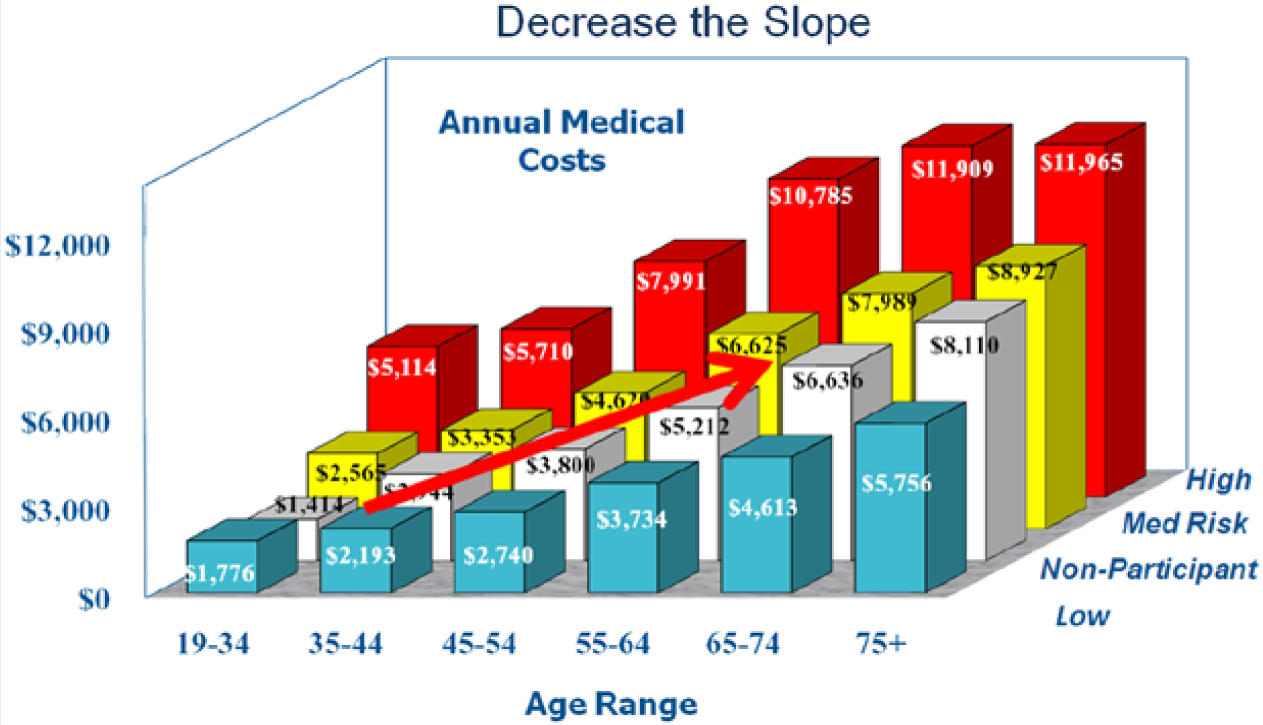
Natural flow of a population by risks–costs–age.
Also in Figure 3, it is evident that in every age group as the risk status increases from low to high the costs also increase. As in Figure 1 with disease, we see the same results in Figure 3 with costs: The population in the 65- to 74-year-old low-risk status is less expensive than the high-risk 19- to 34-year-old population.
Dilemma or Paradox: Reduce Health Care Costs or Invest in Health?
The natural trend for medicine and wellness is to focus on reducing health care costs by treating or intervening with the high-risk and chronic disease individuals, which is natural given their respective training in disease and behavior change. An alternative approach would be to invest in healthful living and pay attention to those already in a low-risk or healthy state. Obviously, an overall strategy has to include both approaches.
Only recently has any attention been given to the low-risk status population. One of the learnings from Figure 2 is that the way to maintain and even increase the number of individuals in the low-risk category is to stop the upward risk flow by investing in helping individuals not get worse.
Thus, our answer to the question for this section is that it is a paradox: If an organization invests in the low-risk individuals, the ultimate result is a healthier and higher performing population and perhaps eventually lower health care costs.
The Special Role of Physicians
Physicians are trained to treat disease while only a small fraction of their training is spent learning how to prevent disease. Most of the diseases they are trained to treat have a relatively well-defined etiology. We now have learned that a significant amount of ill health arises from stress, anxiety, environment, cultural, interpersonal, and other social–emotional factors.
As the American College of Lifestyle Medicine moves forward it is natural that heart disease, diabetes, cancer, and other chronic diseases would be the first targets. The major difference between the more traditional medical approach and the lifestyle medicine approach is the adoption of many of the current wellness initiatives into your strategy. Currently, there are many occupational physicians, nurses, and other members of this academy already in this space and they have been using the lifestyle approach for many years.
Positive Health: On the Healthy Side of Low-Risk and Prevention—Determinants of Health
During the past 30 years we have found that not all low-risk individuals are equal. That is, individuals with the corresponding risk-level status do not universally have the same disease and cost outcomes. At one time we considered low-risk individuals to be at the wellness end of the health spectrum. There is now increasing evidence that positive emotional and psychosocial factors (eg, optimism, life satisfaction, happiness, social support, etc) can affect a physically healthy life. We use the term positive health to represent outliers on a health spectrum with a positive endpoint that goes far beyond health as the absence of risk or illness. Positive health includes thriving on physical, emotional, and social levels.
As we think about the definition of health and positive health in particular, it may be helpful to take a brief look at history. In ancient societies, people most often thought of health as a divine gift and it may not have been until Hippocrates’ time (~400
It is still difficult to operationalize the World Health Organization’s definition of health in a practical way, however. Illness and injury rates are relatively easy to measure and quantify whereas “physical, mental, and social well-being” are comparatively difficult to quantify. Researchers have done much in the past few decades to identify the constructs that comprise health and well-being, as well as developing tools to measure them. McDowell 3 lists dozens of rating scales and questionnaires used in measuring different aspects of health. Subject areas covered by McDowell 3 include physical disability and handicap, social health, psychological well-being, anxiety, depression, mental status testing, pain measurements, and general health status and quality of life.
Occupational medicine and health promotion practitioners recognize that each individual exists on a health continuum that ranges from extreme morbidity on one end to optimal functioning on the other end. People at the optimal functioning position on the spectrum will not have zero health care costs (traditionally touted as the best outcome of a wellness program) but an appropriate level of health care spending as well as vitality and excitement about their life and work responsibilities.
A large component of positive health is emotional health. The World Health Organization Global Burden of Disease Survey estimates that depression and anxiety disorders, including stress-related health conditions, will be second only to ischemic heart disease in the scope of disability experienced by sufferers by the year 2020. 4 According to one estimate, stress-related disorders in the United States cost $300 billion per year in absenteeism, turnover, diminished productivity, and medical, legal, and insurance costs. 5
There is much evidence to suggest that American working adults are struggling under unprecedented levels of stress. For example, one third of US employees report being chronically overworked. 6 The National Institute for Occupational Safety and Health reports that 40% of workers view their job as very or extremely stressful; 25% believe their job is the number one stressor in their life; 26% of workers said they were often or very often burned out or stressed by their work. 7
Determinants of Health
There is a confluence of evidence from many disciplines about the health benefits of positive attitudes and outlook, supportive environment, and culture. Insights from social and cognitive and positive psychology, neuroscience, behavioral economics, organizational studies, and many more, all provide collective evidence with important implications for the practice of lifestyle medicine. Factors such as resilience, optimism, gratitude, and mindfulness help us flourish and live creative, satisfying, and meaningful lives. There is evidence that people who embody these positive characteristics have enhanced motivation to act and be productive,8-11 have less stress and anxiety, 12 are less likely to become ill and bounce back more quickly from disease,13,14 and as a result should ultimately cost employers less in health care spending and decreased lost productivity.15-18
Among the most important findings is that while some of these positive characteristics have a genetic component, with effort and attention we can develop stronger positive attitudes and disposition.19,20 Simple practices such as recalling 3 good things that happened during your day, or taking the time to express gratitude to someone in your life can lead to increases in happiness and optimism.20,21 (Seligmanet al 21 have suggested that there are at least 100 strategies for increasing happiness, a class of Positive Psychology students identified more than 1000 happiness-increasing strategies, and an Amazon.com search for books about happiness yields more than 4000 hits.) In one randomized trial experiment, people who reflected on the things they were grateful for reported fewer physical symptoms, and more time exercising and improved well-being and optimal functioning than individuals who reflected on daily hassles. 22
New discoveries about the brain have led to some of the most revolutionary and important ideas in science. Modern brain research has discovered that the brain is much more malleable or “plastic” throughout life than was once thought. While the brain is indeed more plastic in our early years, research on neuroplasticity is shedding some light on how we can effectively shape our brains and rewire old unhealthy habits.
There are 2 basic rules governing neuroplasticity changes in the brain. The first rule, “use it or lose it,” refers to the “competitive nature of brain plasticity.” 23 If we do not regularly use a skill or perform a behavior, the area of the brain responsible for that activity will be taken over by brain activity for other skills that we do practice. The second rule is that “neurons that fire together wire together.” This refers to the tendency of brain cells that are active at the same time to chemically “wire” together resulting in a greater tendency for one cell to fire when the other is active.
Practitioners of lifestyle medicine can help their patients understand how to use these principles of brain plasticity to replace their unhealthy habits. Instead of working to “break bad habits” patients can work to replace them with better ones. This takes awareness of the habit and/or its triggers, and a concerted effort to actively focus attention on something pleasurable other than the old habit. This will strengthen the brain circuitry and trigger dopamine release which rewards the new activity. Over time and with repeated effort, our old bad habits can be replaced with new more healthy ones.
These rules of brain plasticity can also work to help us build more positive dispositions. As one prominent neuropsychologist puts it, “If you point your attention toward the good in life, the better your brain will get at fostering goodness, and the healthier it will become.” 24 There is an increasing body of evidence that supports the idea that practicing gratitude, mindfulness meditation, and reframing negative thoughts into positive affirmations, all work to physically change your brain, and strengthen positive states of mind. This has important implications for any practitioner working to improve health and well-being.
A Thriving, Healthy, High-Performing, and Sustainable Workplace and Workforce
In our experience, an organizational health assessment could be as important as an individual health assessment. Following the above logic we used for the individual it is unlikely that all healthy and high-performing organizations are equally healthy and high performing.
Wellness and possibly population health strategies have focused on risk reduction toward evidence-based prescriptive levels or risks. However, an individual meeting all the predetermined risk status standards but working or living in an unhealthy organizational or family environment or culture will likely not maintain that risk status and definitely not achieve or maintain a positive health status or even a low-risk status. Organizational health has to be measured on a different but interactive scale than solely on a health risk–behavior metric.
Achieving a positive organizational health is a continuing journey as is positive health for the individual. The primary drivers of positive organizational health include the elements of a healthy environment and healthy culture in addition to positive health of the individuals. In Zero Trends, we outlined the 5 basic pillars on which to build a healthy organization:
Senior leadership. What is the responsibility of the senior leaders?
Operations leadership. How are all policies and procedures aligned?
Self-leadership. How can the organization help people become self-leaders?
Recognition of positive actions. Are positive actions recognized or rewarded?
Quality assurance. How to get the right information to support decision making.
In our forthcoming book, Beyond Zero Trends (spring/summer, 2014) we present a system to get to positive organizational health. The system is flexible so it can be adjusted to the various types of organizations and those at different stages of organizational health. Briefly, the system starts with a landscape assessment and vision, an organizational environment and culture assessment, an identification of the strengths and gaps, an approach to developing self-leaders, and a real-time and comprehensive organizational assessment system.
Measurement, Evaluation, and Decision Support to Provide Real-Time Feedback
The financial outcome measures used by the wellness community over the past 40 years have been shown to be somewhat controversial. The assumptions were that to prove the business case it was necessary to show business leaders that they could get a return on investment from their wellness (risk reduction via behavior change) program. The history of this work indicates that the results are too dependent on participation, industry sector, age, gender, engagement, wellness program, incentives, insurance coverage, areas of the country, and other factors, including unknown determinates of health to get to consistent outcomes. Even the most rigorous study designs and statistical methods were not consistently showing positive results.
There is no lack of intuitive belief that those with the most healthy behaviors and lowest risk factors are the more healthy and low-cost individuals. However, the evidence that moving to that wellness end state will result in lower health care costs is where the inconsistency in the evidence arises.
Summary
The first half of this article is devoted to behavioral economics. It is clear that sufficient data are available to indicate that poor lifestyle factors lead to disease and lead to economic losses. Higher levels of health risks and behaviors are in the natural flow of Americans to develop disease and moving to a high-cost status. The data suggest that reduction in risk and unhealthy behaviors result in lower probability of disease and health care costs.
The second half of the article is a discussion of additional lifestyle determinants of health beyond risk factors and poor health behaviors. The additional areas include social–emotional states and positive characteristics of the individual and the environment and culture of the organization. Recent research findings from the study of the brain and impact on attitudes and health are additional areas of future research and have implications for prevention and treatment.
It is very clear that there are growing opportunities for members of the College of Lifestyle Medicine. Sufficient evidence exists to justify further research and advanced lifestyle treatment practices. The members of the college are encouraged to expand their interests and research inquiry in evaluating and treating these areas.