
Abstract
There is substantial evidence that lipids are critical in the development and progression of atherosclerotic cardiovascular disease. In November 2013, the American College of Cardiology/American Heart Association in conjunction with the National Cholesterol Education Program IV developed new guidelines for the treatment of blood cholesterol. In this report, we review these new guidelines and emphasize the potential benefits of physical activity and exercise training on plasma lipids.
‘It is important to note that fit patients with hypercholesterolemia had a better survival than did unfit patients with “normal” levels of cholesterol.’
Cardiovascular diseases (CVDs), especially atherosclerotic CVD (ASCVD), are the leading cause of morbidity and mortality in the United States and most of the Westernized World. 1 Although coronary heart disease (CHD) morbidity and mortality, which is mostly a result of ASCVD, has decreased over the past 30 years, CHD still remains a major threat to health across the globe. Therefore, the aggressive primary and secondary prevention of CHD and ASCVD is imperative for our society, and dyslipidemia remains a major modifiable risk factor for many patients. 2 Certainly, most of the evidence supporting the importance of lipid intervention has come from the large clinical trials with HMG CoA-reductase inhibitors (statins) that demonstrate a major reduction in CHD and other ASCVDs, including stroke. 2
The National Cholesterol Education Program (NCEP) has previously developed major guidelines regarding the treatment of blood cholesterol in 2001 (NCEP III), with additional adjustments made in 2004.3,4 However, for several years, specialists in lipids as well as clinicians interested in the prevention and treatment of ASCVDs have awaited the NCEP IV recommendations for the assessment and treatment of patients with dyslipidemia. In November 2013, the American College of Cardiology (ACC)/American Heart Association (AHA) developed an updated set of guidelines along with NCEP IV that have generated considerable attention and controversy. 2
In this report, the major updates in these guidelines are outlined. Additionally, this article reviews the potential for physical activity (PA) and exercise training (ET) to improve plasma lipids, including data on the potential benefits of cardiac rehabilitation and ET (CRET) programs in the secondary prevention of ASCVDs and on plasma lipids.
New Risk Assessment Guidelines
During the past 2 decades, risk of CHD was assessed by the Framingham Risk Score; however, in November 2013, the combined ACC/AHA published new risk assessment guidelines. 5 These updated guidelines use the Race-and Sex-Specific Pooled Cohort equations to predict 10-year risk of ASCVD in non-Hispanic African Americans and Caucasians between the ages of 40 and 79 years. The data were derived from several clinical trials (ARIC, CHS, CARDIA, and Framingham origin and offspring) and used age, gender, total and high-density lipoprotein cholesterol (HDL-C), systolic blood pressure, use of antihypertensive medications, diabetes mellitus (DM), and current smoking status. Additionally, these new guidelines recommended assessment of 30-year or lifetime risk of ASCVD in 20- to 59-year-olds without ASCVD or high short-term risk (defined as <5%-7.5% 10-year risk).
Unfortunately, although this risk assessment may have some improvements over the prior risk assessment, (e.g. including using data from a more diverse population than just Framingham, assessing risk in patients with DM, and allowing risk assessment over longer periods of time), these equations totally neglected the impact of PA and, more so, cardiorespiratory fitness (CRF) levels on the overall risk of major ASCVD and subsequent clinical prognosis and all-cause survival.6-8 Additionally, this assessment does not adequately address risk assessment in Hispanics, Asians, and Indians. The current risk assessment will overestimate risks in Hispanics and Asians, who generally have a relatively low risk of ASCVD and underestimate risk in American Indians, who have a very high risk of ASCVD.
New Cholesterol Guidelines
The emphasis in the new ACC/AHA 2013 Cholesterol Guidelines is on clinical ASCVD, 2 including prior acute coronary syndrome/myocardial infarction, angina (stable or unstable), arterial revascularization (coronary and other), cerebral vascular disease (stroke/transient ischemic attack [TIA]), and peripheral arterial disease, presumably caused by atherosclerosis. The major treatment in the new guidelines is using moderate- and high-dose statins. These guidelines focus on 4 major statin benefit groups, including those with established ASCVD, low-density lipoprotein cholesterol (LDL-C) ≥190 mg/dL, DM (40-75 years old), and a 10-year risk of major ASCVD ≥7.5% (in those 40-75 years of age).
Unfortunately, these guidelines have several major controversial points and potential pitfalls. In fact, there are no specific guidelines for those older than 75 years without ASCVD, 20- to 39-year-olds with DM (who have a very high lifetime risk of ASCVD), and 20- to 39-year-olds without ASCVD and with LDL-C <190 mg/dL. Additionally, the new guidelines call for either moderate- or high-dose statins, but there are no longer any LDL-C or non-HDL-C goals.
Furthermore, there are no goals or guidelines directed at triglycerides (TGs), including severely elevated TGs; also, there are no strong guidelines for nonstatin lipid medications, despite several having significant evidence (Table 1).
New ACC/AHA 2013 Cholesterol Guidelines: No Definitive Guidelines. a
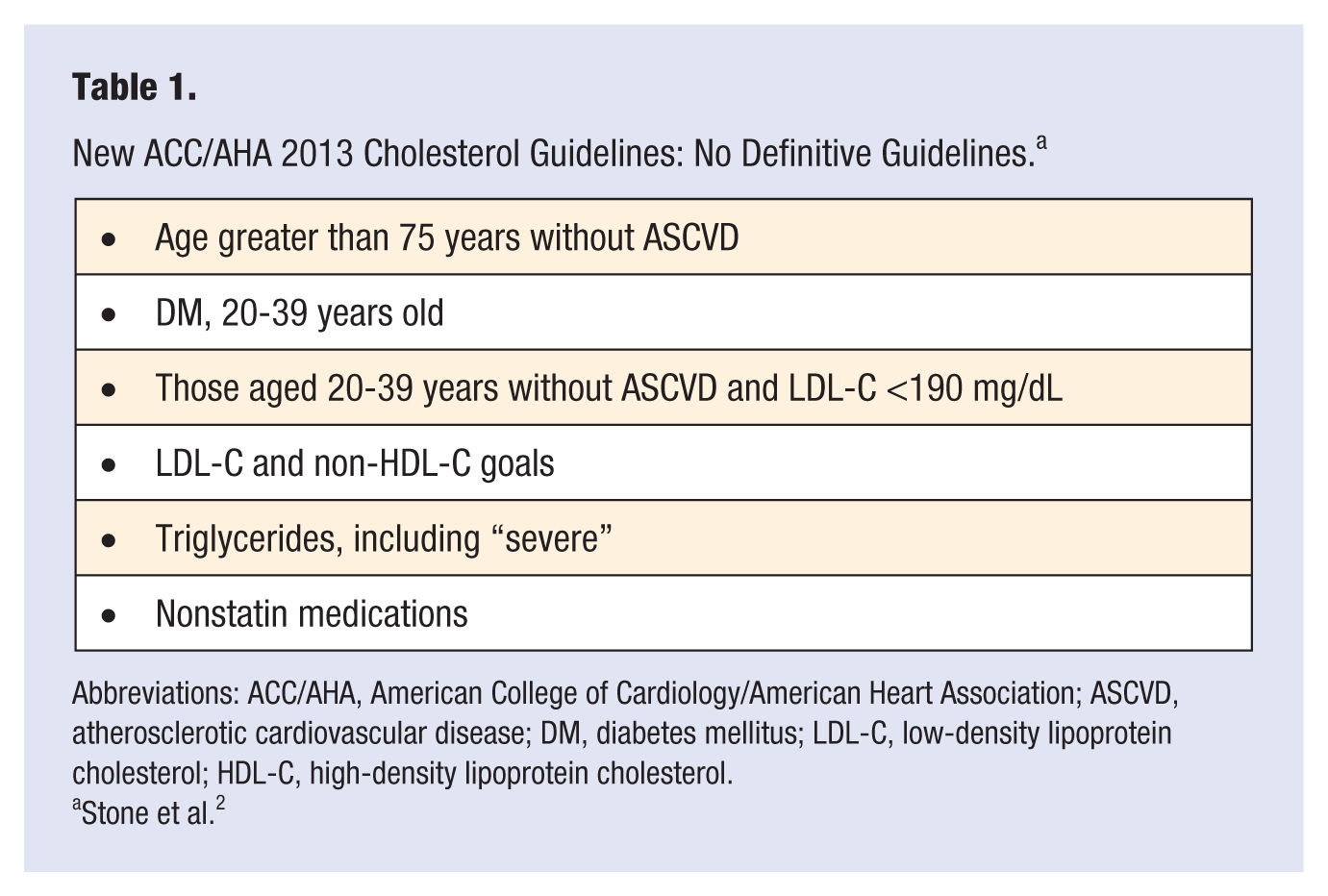
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; ASCVD, atherosclerotic cardiovascular disease; DM, diabetes mellitus; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Stone et al. 2
Specifically in patients >75 years of age, where overall productivity remains high for many and there is very high risk of ASCVD, there are no pharmacological guidelines in those without ASCVD and with LDL-C <190 mg/dL. The guidelines suggest the use of moderate-dose as opposed to high-dose intense statin therapy. These new guidelines, therefore, fail to provide aggressive or maximal therapy to adequately treat many high-risk older patients (Table 2).
New ACC/AHA 2013 Cholesterol Guidelines: Specific Issues in Those >75 Years Old. a
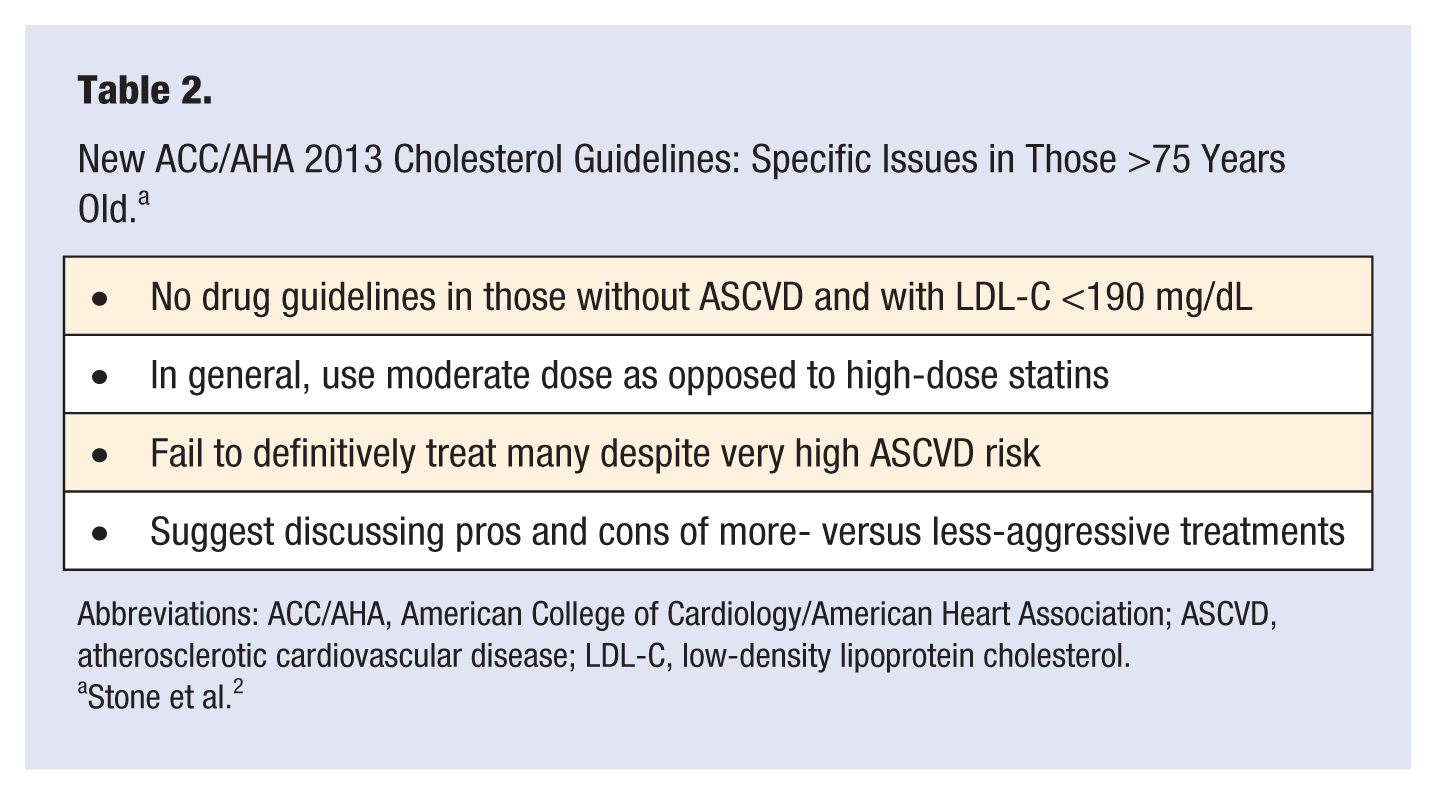
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; ASCVD, atherosclerotic cardiovascular disease; LDL-C, low-density lipoprotein cholesterol.
Stone et al. 2
Nonpharmacological Lipid Treatment: PA and Exercise
The new 2013 ACC/AHA also has guidelines on lifestyle management to reduce CVD risk, which are reviewed in detail elsewhere. 9 Although PA and ET are not emphasized in the assessment equations, they are emphasized in the lifestyle management suggestions.
Despite the fact that there has been an abundance of evidence demonstrating the benefits of PA, ET, and improvements in CRF in CHD and ASCVD morbidity and mortality, the benefits of this therapy on plasma lipids are much more modest. In fact, the majority of studies do not support significant impact of ET on total cholesterol (TC) or LDL-C. However, studies have demonstrated that PA and ET, and high CRF, have beneficial impacts on LDL particles, reducing the level of small, dense LDL particles (pattern B LDL, which is more easily oxidized and more atherogenic) and increasing the level of large LDL particles (pattern A LDL, which is less easily oxidized and less atherogenic).10,11
On the other hand, since the pioneering work of Haskel and Wood in the 1980s, the impact of PA and ET on HDL-C and TGs is much more notable.12-14 A recent meta-analysis by Kodama et al 15 observed that aerobic ET resulted in modest increases in HDL-C (2.5 mg/dL), with greater ET duration and caloric expenditure associated with more marked improvements in HDL-C. In general, the improvements in TGs are larger and more consistent than those of HDL-C, but the improvements in HDL-C seem to be considerably greater in those with elevated TGs. 16
Although the impact of PA and ET on lipids may seem only modest, this therapy is known to have a significant impact on levels of CRF, which is a powerful predictor of prognosis in patients with dyslipidemia. In fact, Blair et al 17 almost 20 years ago assessed the impact of CRF on survival in many groups of patients with chronic diseases. In a long-term follow-up of 25 341 men and 7080 women with 601 deaths and more than 210 000 man/woman years of follow-up, they demonstrated that CRF was a potent predictor of prognosis in patients with many chronic diseases, including hypercholesterolemia. It is important to note that fit patients with hypercholesterolemia had a better survival than did unfit patients with “normal” levels of cholesterol.
Benefits of CRET
We have published numerous benefits of formal CRET programs in patients with ASCVD, which include major reductions in morbidity and mortality.18,19 Although the improvements with CRET programs may be a result of both ET and other non-ET, nonpharmacological aspects of the program, we have reported modest improvements in lipids with comprehensive CRET (Table 3). Following CRET, we have reported significant improvements in a variety of lipid parameters, including TC (−2%), TGs (−13%), HDL-C (+7%), LDL-C (−2% to −4%), and LDL-C/HDL-C ratio (−10%). 20 In general, we have also reported benefits of CRET on body mass index (−2%), percentage body fat (−5%), and exercise capacity or CRF (+30%). It is important to note that patients were more likely to have more improvements in lipids following CRET if they had more abnormal baseline values. 21
Benefits of Cardiac Rehabilitation and Exercise Training Programs on Plasma Lipids. a
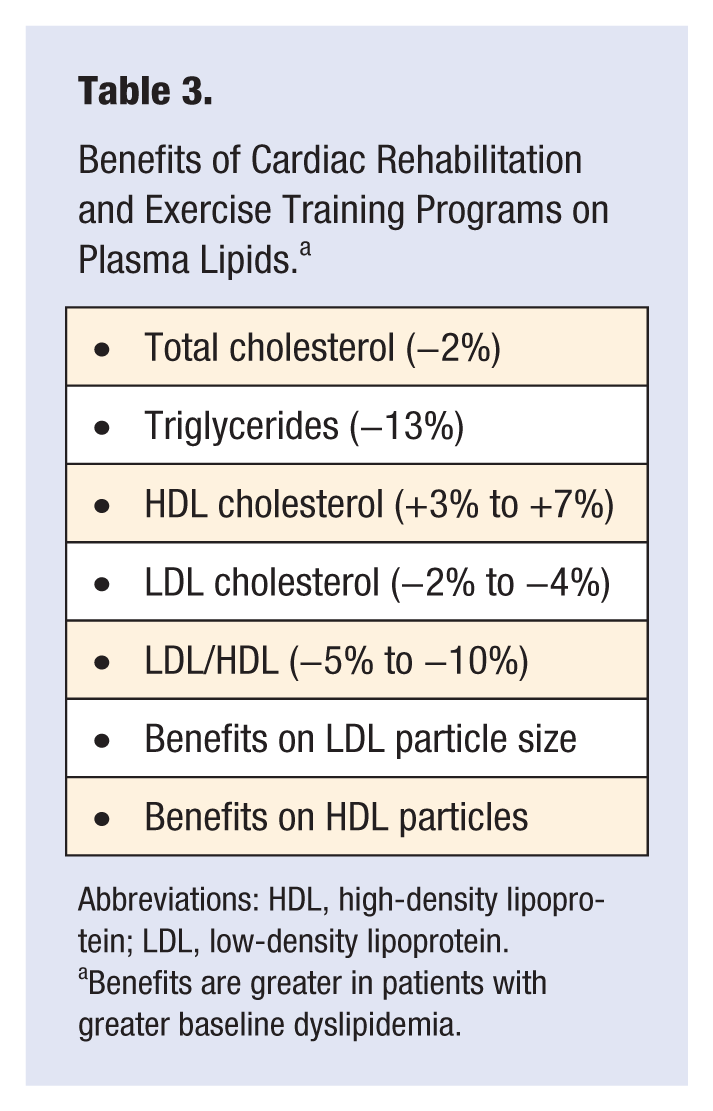
Abbreviations: HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Benefits are greater in patients with greater baseline dyslipidemia.
Potential Mechanisms of PA and ET on Lipids
Although the exact mechanism by which PA and ET improve plasma lipids, especially HDL-C and TGs, are not completely understood, the available evidence suggests that lipoprotein lipase (LPL) and lower very-low-density lipoprotein (VLDL) and chylomicron TG levels are involved, and ET increases LPL activity in tissue and muscle.11,21 Additionally, VLDL TGs are exchanged for cholesterol esters in HDL and LDL, which is then hydrolyzed by lipases, causing reduction in the size of these particles. Besides LPL, hepatic lipase also undergoes beneficial changes with ET, contributing to HDL maturity and enhanced ability in reverse cholesterol transport.
Future Directions
My colleagues and I feel that the current ACC/AHA Risk Assessment Guidelines are considerably lacking, especially because they do not give sufficient weight to the importance of PA, ET, and especially, CRF in reducing overall risk. In fact, my colleagues and I have published substantial data demonstrating that CRF is critical in predicting risk in many groups of patients. 22 Although PA, ET, and CRF have marked benefits on overall risk of CHD and ASCVD, admittedly, the impact on plasma lipids is only modest. Finally, the current ACC/AHA Cholesterol Guidelines may lead to overtreatment with statins in some relatively low-risk patients; but we are more concerned that many high-risk patients, including young patients with DM and elderly patients >75 years old, will be undertreated. Additionally, once patients are treated with moderate- or high-dose statins according to the guidelines, the new guidelines do not provide guidance on how to further improve plasma lipids in those with suboptimal lipid responses to statin therapy alone.
Conclusions
Nonpharmacological treatment of lipids includes increasing PA, ET, and levels of CRF. Although the improvement in lipids with nonpharmacological treatment is only modest, clearly, this therapy is needed in the prevention and treatment of patients with ASCVD as well as in those who are at high risk of ASCVD. The current cholesterol guidelines mostly emphasize moderate- and high-dose statins, but these guidelines have led to considerable controversies, which are introduced and briefly reviewed in this manuscript.