
Abstract
Physical fitness is simply defined as the capacity to perform physical work. Energy is necessary to perform work and sustain life and is extracted aerobically and anaerobically. Evaluation of aerobic fitness is based on the assessment of maximal oxygen consumption (V
‘Accurate assessment of the level of physical activity in large populations becomes important when investigating associations between health benefits and a physically active lifestyle.’
Introduction
Work is defined as the energy transfer or force required to move an object at a certain distance. For humans, the energy necessary for locomotion or the displacement of an object (work) requires muscular involvement. Thus, the capacity to perform such physical tasks is defined as physical fitness.
Unlike machines, energy transfer (work) in humans is difficult to assess precisely. Energy for work is derived mainly from 2 systems (aerobic and anaerobic) working synergistically to perform a given task that is usually more complex than moving an object from point A to point B. For example, the complex movements involved in sports such as change in direction requires more energy than moving linearly. Isometric contractions such as those involving certain stances in gymnastics (iron cross, parallel bars) demand tremendous amounts of energy. However, movement in such tasks is absent and therefore (theoretically) work is not performed. Accordingly, the precise assessment of work and physical fitness is subject to these limitations.
Definition of Physical Activity, Exercise, and Fitness
Physical Activity and Exercise
Physical activity and exercise both describe a physiologic state that requires a degree of muscular effort beyond resting conditions. Although the terms can be used interchangeably in some instances, there are differences. Physical activity is defined as movement that requires any form of skeletal muscle contraction and results in energy expenditure beyond resting levels.1,2 This work can be performed as part of the daily requirements of the job or around the house (yard work), or leisure time activities also known as recreational activities. Accurate assessment of the level of physical activity in large populations becomes important when investigating associations between health benefits and a physically active lifestyle.
Exercise is best defined as a structured program designed to achieve a state of physical exertion of certain intensity, duration, and frequency. 2 The by-product of exercise intensity and duration yields the volume of work or energy expenditure per unit of time. Exercise programs can be tailored to one individual. Furthermore, the intensity, duration, and frequency can be manipulated to produce the desired goals. For these reasons, exercise programs are implemented in interventional research studies to assess the effects of exercise on a specific physiologic parameter, such as blood pressure, body weight, blood lipid, and so on.
Physical Fitness
Physical fitness is defined as a set of physical attributes that people have or achieve that relates to the ability to perform physical activity.1,2 These attributes have important implications, including one’s ability to perform recreational or occupational activities, the determination of disability, injury prevention, and skeletal muscle, bone, and cardiovascular health. Moreover, higher fitness is strongly associated with better long-term health outcomes.3,4 Engaging in proper physical training leads to an improvement in these physical attributes and physical fitness. The degree of improvement is determined by several factors, including training, diet, rest, psychological factors, and genetics.
Aerobic and Anaerobic Fitness
The energy necessary to sustain life and perform work is generated by the cells in 1 of 2 ways: with the use of oxygen and without oxygen. In general, high-intensity activities derive their energy mainly independent of oxygen, while low-intensity activities use oxygen to meet their energy requirements. Historically, the utilization of oxygen to generate energy has been referred to as aerobic metabolism, and generating energy without using oxygen has been referred to as anaerobic metabolism.
Therefore, aerobic fitness refers to the ability to provide the required energy for a specific task in which the cardiopulmonary system adequately supplies the needed oxygen to the working muscle cells. Aerobic activities consist of repetitive, low-resistance movements (eg, walking or cycling) that last over a relatively extended period of time (generally 5 minutes or more). Most of the energy for such activities is derived from the catabolism of intracellular and adipose tissue–released free fatty acids.
Anaerobic fitness refers to the body’s capacity to provide the required energy for a specific task independent of oxygen. Anaerobic activities are characterized by bursts of intense activity lasting a comparatively short period of time (sprinting, lifting of a heavy weight, jumping, etc). The immediate energy requirements (approximately initial 10 seconds) for such activities are met by intramuscular stores of adenosine triphosphate and phosphocreatine. This system allows time for the glycolytic pathways to generate an increasingly greater percentage of energy and meet the requirements for the activity lasting beyond the initial phase and for the next 2 to 3 minutes. The energy demands for work at maximal or near maximal capacity beyond 2 to 3 minutes exceed the capacity of the anaerobic pathways. Consequently, the intensity of the activity gradually decreases or ceases completely.
It is important to note that muscle cells are never entirely aerobic or anaerobic. Rather, these 2 energy systems (aerobic and anaerobic) are almost always working together in a harmonious way, sharing the responsibility for providing the energy requirements for the working muscles and the entire body. However, one is likely to be the predominant system providing most of the energy for the particular activity at hand.5(pp19-50)
Determining Exercise Capacity: Direct Method Open Circuit Spirometry
The “true” maximum aerobic capacity is the maximum amount of oxygen (referred to as maximal oxygen uptake or V
The individual breathes room air via a mouth piece (nose occluded), connected to an automated system (often termed a metabolic cart) by plastic tubes. The mouth piece is designed in such a way that it allows the measurement of the volume of expired air, while a small sample of the expired air enters the metabolic cart and is analyzed for its oxygen and carbon dioxide content. Oxygen uptake is determined by the product of ventilation and the difference between the O2 content of the ambient and expired air. After resting samples are taken, the individual is subjected to a standardized exercise protocol on a treadmill or stationary bike. The exercise begins at a very low workload and increases progressively until volitional fatigue or until a clinical indication for stopping is reached. The rate of increase in external work depends on the exercise protocol used, but it is typically recommended that the test be individualized to last between 8 and 12 minutes.
Since the relationship between the increase in workload and oxygen consumption is linear, oxygen requirements also increase. At some point the individual reaches a volitional fatigue endpoint, and the test is terminated. This level is referred to as the maximal aerobic capacity of the individual. The oxygen used by the body at the point of fatigue is referred to as the V
The advantage of the direct method is that it allows an accurate assessment of the exercise intensity of an individual based on directly measured rather than estimated aerobic capacity. However, it is an elaborate method that requires expensive equipment and trained personal and is therefore cost-prohibitive for large populations. For this reason, it is mostly used in individuals with specific clinical needs and for research purposes 5 . For someone who simply wishes to know the appropriate exercise intensity during his or her training, exercise intensity can be easily determined by the heart rate that corresponds to the appropriate percentage of oxygen consumption. Since heart rate and oxygen uptake are continuously recorded during the metabolic test, one can easily match a desired percentage of heart rate to the corresponding oxygen consumption.
Determining Aerobic Fitness by Standardized Tests Using Indirect Methods
The need for more practical methods to assess aerobic capacity for large populations led to the development of standardized exercise tests and the common practice of estimating energy requirements from different workloads. An indirect method for estimating the fitness level of an individual is based on the same principle as that for the direct assessment of V
Commonly Used Treadmill and Bicycle Exercise Protocols.
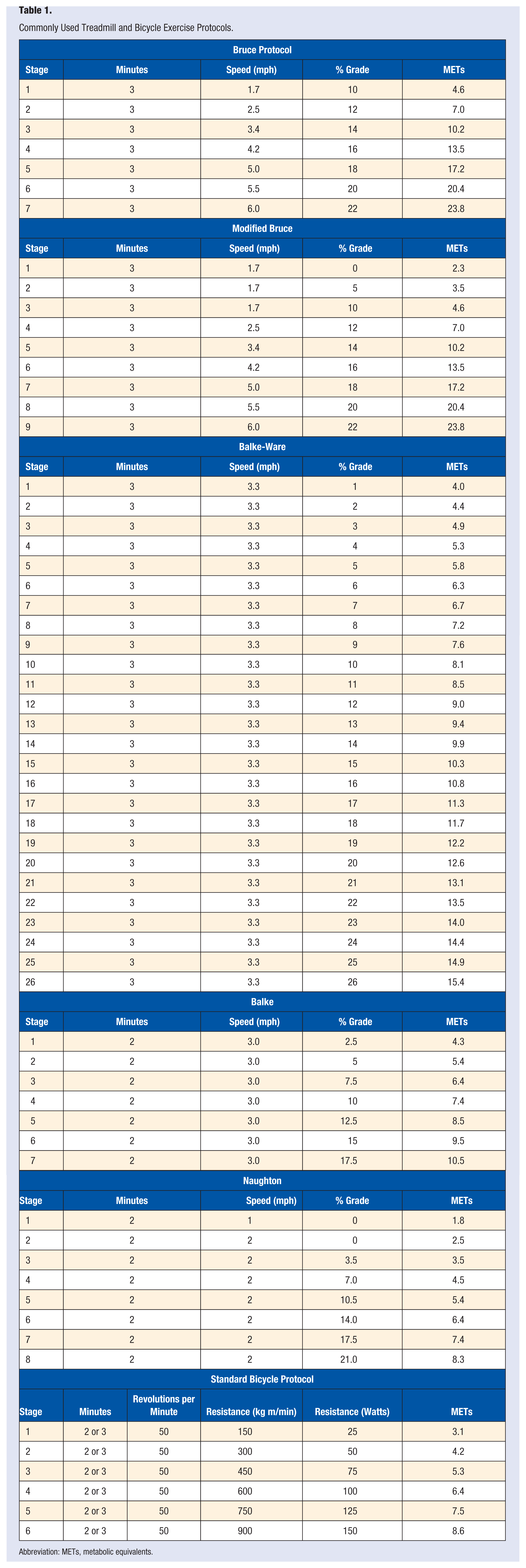
Abbreviation: METs, metabolic equivalents.
The workload is estimated for each exercise stage based on the speed and elevation of the treadmill. This estimation is based on comparison studies in which the energy requirements (oxygen consumption) were measured directly with open circuit spirometry. In general, the amount of oxygen used during resting conditions is approximately 3.5 mL of oxygen per kilogram of body weight per minute (3.5 mL O2/kg/min). This value (the resting metabolic rate) is termed 1 metabolic equivalent or 1 MET. Naturally, any increase beyond the 1-MET level represents higher total body oxygen consumption. Based on this rationale, several standardized exercise protocols have been developed to assess the MET level of individuals for clinical and other reasons. The MET level achieved on termination of the test (the individual reaches volitional fatigue) represents the peak aerobic capacity of the individual. Because each MET is equal to approximately 3.5 mL O2/kg/min, V
Exercise Protocols
The purpose of the test and the person tested are important considerations in selecting the protocol. Exercise testing may be performed for diagnostic purposes, for functional assessment, or for risk stratification. An often ignored but nevertheless consistent recommendation in the recent exercise testing guidelines is that the protocol be individualized for the patient being tested.8,9 For example, a maximal, symptom-limited test on a relatively demanding protocol would not be appropriate (or very informative) for a severely limited patient. Likewise, a very gradual protocol might not be useful for an apparently healthy, active person. Use of submaximal testing, gas exchange techniques, the presence of a physician, and the exercise mode and protocol should be determined by considering the person being tested and the goals of the test.
Commonly used exercise protocols, their stages, and the MET level for each stage are outlined in Table 1. The most suitable protocols for clinical testing should include a low-intensity warm-up phase followed by progressive, continuous exercise in which the demand is elevated to a patient’s maximal level within a total duration of 8 to 12 minutes.8-12 In the absence of gas exchange techniques, it is important to report exercise capacity in METs rather than exercise time, so that exercise capacity can be compared uniformly between protocols. METs can be estimated from any protocol using standardized equations that have been put into tabular form.8,12 In general, 1 MET represents an increment on the treadmill of approximately 1.0 mph or 2.5% grade. On a cycle ergometer, 1 MET represents an increment of approximately 20 W (120 kg m/min) for a 70-kg person. The assumptions necessary for predicting MET levels from treadmill or cycle ergometer work rates (including not holding the handrails, that oxygen uptake is constant [ie, steady-state exercise is performed], that the subject is healthy, and that all people are similar in their walking efficiency) raise uncertainties as to the accuracy of estimating the work performed for an individual patient. For example, the steady-state requirement is rarely met for most patients on most exercise protocols; most clinical testing is performed among patients with varying degrees of cardiovascular or pulmonary disease; and people vary widely in their walking efficiency. 13 It has therefore been recommended that a patient be ascribed a MET level only for stages in which all or most of a given stage duration has been completed. 14
Ramp Testing
An approach to exercise testing that has gained interest in recent years is the ramp protocol, in which work increases constantly and continuously. In 1981, Whipp et al 15 first described cardiopulmonary responses to a ramp test on a cycle ergometer, and many of the gas exchange equipment manufacturers now include ramp software. Treadmills have also been adapted to conduct ramp tests.12,16,17 The ramp protocol uses a constant and continuous increase in metabolic demand that replaces the “staging” used in conventional exercise tests. The increase in workload is tailored for each patient, based on information gathered prior to the test regarding the level of physical activity of the individuals and symptoms. The uniform increase in work allows for a steady increase in cardiopulmonary responses and permits a more accurate estimation of oxygen uptake.12,18 The recent call for “optimizing” exercise testing8,10,12,15 would appear to be facilitated by the ramp approach because large work increments are avoided and increases in work are individualized, permitting test duration to be targeted. Because there are no stages per se, the errors associated with predicting exercise capacity alluded to previously are lessened.2,8,12
Cycle Ergometer Protocols
The most modern, electronically braked cycle ergometers consist of a single wheel and have controllers that permit ramp testing, in which the work rate increments can be individualized in continuous fashion. Cycle ergometers are relatively inexpensive, minimize the risk of falling, can be moved from place to place and can accurately predict energy output.
When assessing maximal aerobic power, it is recommended that the initial workload selected is low and increase gradually. It is recommended that the pedaling frequency should be maintained at 50 to 60 revolutions per minute. Although there are specific bicycle protocols named for early researchers in Europe, such as Astrand, 19 bicycle ergometer protocols tend to be more generalized than for the treadmill. For example, 15- to 25-W increments per 2-minute stage are commonly used for patients with cardiovascular disease, whereas for apparently healthy adults or athletic individuals, appropriate work rate increments might typically be between 40 and 50 W/stage.
Submaximal Testing
In general, maximal, symptom-limited tests are not considered appropriate until 1 month after myocardial infarction or cardiac surgery. Thus, submaximal exercise testing has an important role clinically for predischarge, post–myocardial infarction, or post–bypass surgery evaluations. Submaximal tests have been shown to be important in risk stratification17,20-23 for making appropriate activity recommendations, for recognizing the need for modification of the medical regimen, or for further interventions in patients who have sustained a cardiac event. A submaximal, pre-discharge test appears to be as predictive for future events as a symptom-limited test among patients less than 1 month after myocardial infarction. Submaximal testing is also appropriate for patients with a high probability of serious arrhythmias. The testing endpoints for submaximal testing have traditionally been arbitrary but should always be based on clinical judgment. A heart rate limit of 140 beats/min and a MET level of 7 are often used for patients younger than 40 years, and limits of 130 beats/min and a MET level of 5 are often used for patients older than 40 years. For those using beta-blockers, a Borg perceived exertion level in the range of 7 to 8 (1-10 scale) or 15 to 16 (6-20 scale) are conservative endpoints. The initial onset of symptoms including fatigue, shortness of breath, or angina, is also indications to stop the test. A low-level protocol should be used, that is, one that uses no more than 1-MET increments per stage. The Naughton protocol 23 is commonly used for submaximal testing. Ramp testing is also ideal for this purpose because the ramp rate (such as 5 METs achieved over 10-minute duration) can be individualized depending on the patient tested. 12
Submaximal tests can be used to assess the capacity of apparently healthy individuals to exercise safely or to estimate V
It is important to note that the accuracy of such tests is affected by the assumption of linearity between heart rate and oxygen consumption as exercise intensity increases. Although this assumption generally holds, especially in low-to-moderate workloads, differences in maximal heart rate, variability in maximal heart rate estimation by the formula 200 − age, day-to-day heart rate variability and mechanical efficiency among individuals are not considered. Consequently, the V
Walk Tests for Cardiorespiratory Fitness Assessment
A number of walking tests have also been developed for estimating cardiorespiratory fitness or assessing functional status of healthy individuals, and patients with cardiovascular or pulmonary disease in clinical settings. Advantages of walk tests include the fact that they are easy to perform and are relatively inexpensive, and thus can be applied to large populations. It is important to keep in mind that equations developed to predict V
Walking tests include (a) the 6-minute walk test, (b) the Cooper 12-minute test, (c) the 1.5 mile test, and (d) the Rockport 1-mile fitness walking test. 2
The 6-minute walk test is popular for assessing functional status in clinical settings and is mostly used among diseased populations such as patients with heart failure, stroke, and peripheral vascular disease. The objective of the test is to cover the greatest distance by walking in 6 minutes. Its obvious advantages are that it requires practically no equipment (other than a stopwatch) and little time.
Although the association between 6-minute walk performance and exercise capacity is only modest, peak V
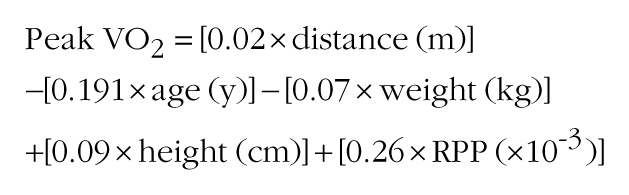
where m = meters, kg = kilogram, cm = centimeters, y = years, and RPP = rate pressure product (systolic blood pressure [mm Hg] × heart rate).
The Cooper 12-minute test is based on a similar concept (covering the greatest distance in 12 minutes), while the objective of the 1.5-mile test is to run the distance (1.5 miles) in the shortest period of time. Unlike the 6-minute walk test, both these tests are more suitable for healthy, younger individuals. They also require little or no additional equipment and can be administered to large populations.
The Rockport 1-mile fitness walking test involves covering a 1-mile distance in the shortest period of time. However, in addition to the time required to cover the 1-mile distance, the test uses peak heart rate achieved during the last minute of the walk, and an estimate of peak V
Step Test
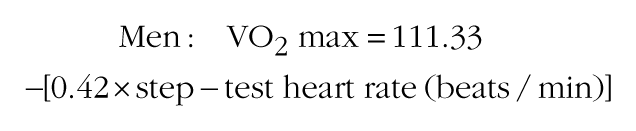
A number of step test have been developed over the years. One common step test that has been used consists of stepping up and down a step of a certain height and fixed rate. The rate of stepping is established with a metronome set at 88 beats/min. The stepping cadence has four counts: up (right foot), up (left foot), down (right foot), down (left foot). The stepping height is approximately 40 cm. Cardiorespiratory fitness is estimated by assessing the post exercise heart rate response. The heart rate is measured for 15 seconds immediately after the cessation of the test and while the participant is standing. The 15-second heart rate is then converted to beats/min (15-second heart rate × 4) and compared with established percentile rankings (Table 2). The relationship between recovery heart rate and V
Predicted Aerobic Capacity Estimated by the 15-Second Recovery Heart Rate (HR) Attained Immediately After Cessation of the Step Test 21 .
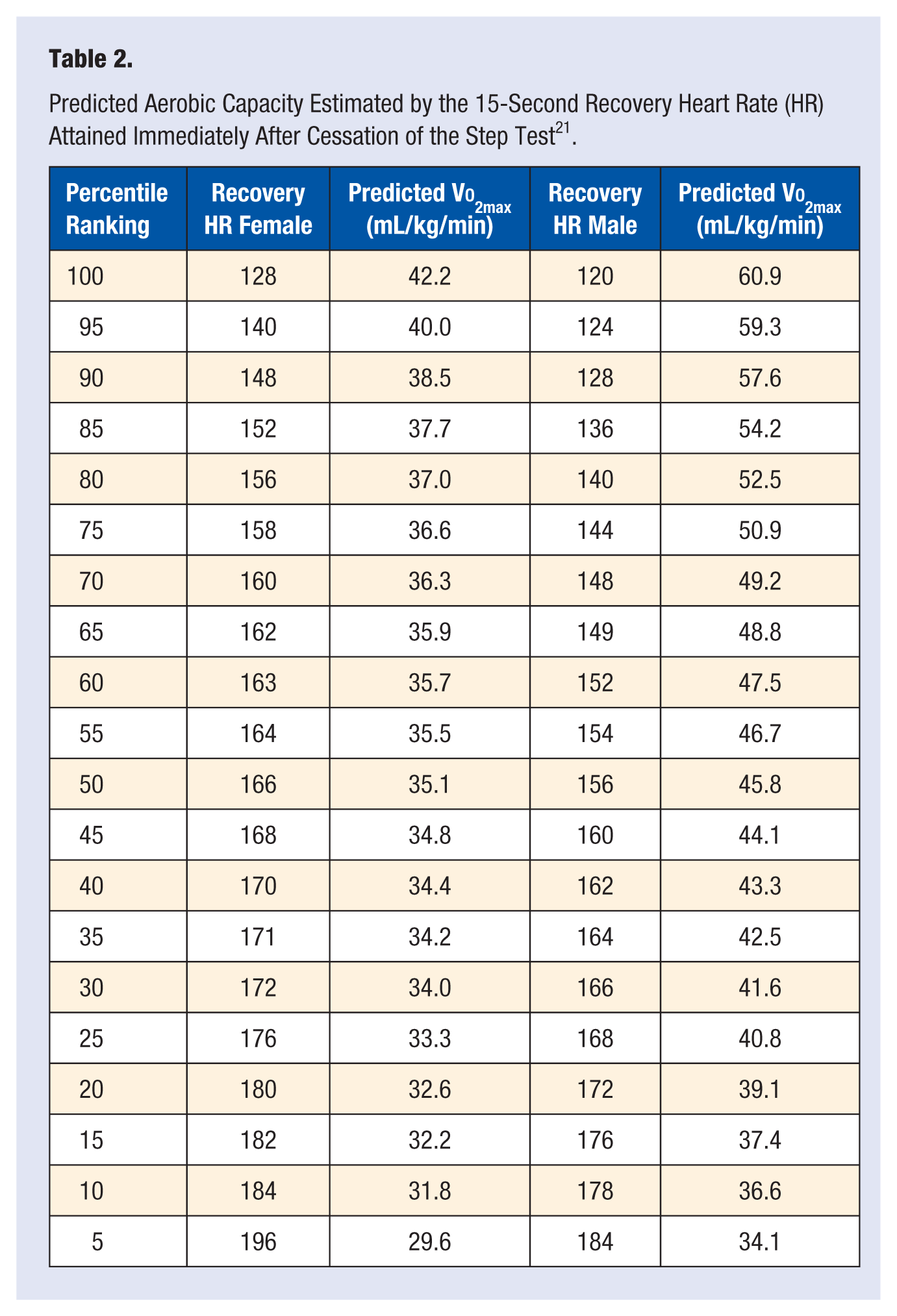
The step test is a realistic alternative to other test in field studies. It requires little or no equipment, little practice or skill and can be implemented to a large cohort. However, it is more difficult to standardize, difficult to monitor heart rate or blood pressure. In addition, the risk of falling at higher stepping paces is relatively high.
Muscular Fitness
The American College of Sports Medicine defines muscular fitness as the ability of the muscle to perform tasks that require muscular strength or muscular endurance. The role of muscular strength in the performance of activities of daily living and exercise, as well as in the prevention of chronic disease, is increasingly being recognized.28,29
Traditionally, resistance exercise training or strength training is the preferred mode for increasing muscular strength. Resistance exercises can be performed by either using free-standing weight or weights housed within an apparatus (weight training machines). Such apparatuses use pulleys to allow the displacement of a preselected weight by the individual. Both free weights and strength training apparatuses are similarly effective in promoting muscular fitness. However, weight training machines offer a greater degree of safety and efficiency, but they are more expensive.
Strength is an important component of fitness assessment since it has implications for an individual’s functional capabilities, disability, bone health, and insulin resistance and has been shown to have a strong association with long-term outcomes.30,31 Muscular strength is inversely and independently associated with death from all causes and cancer in men, even after adjusting for cardiorespiratory fitness and other potential confounders. 31
Muscular Strength
Muscular strength is defined as the ability of the muscle or muscle groups to exert force during a voluntary contraction. 1 The maximal force a muscle or group of muscles can exert is traditionally assessed by tests that require maximum effort against the greatest resistance one can move through the full range of motion once. This is known as the 1-repetition maximum (1-RM). A percentage of the 1-RM is then used to determine the number of repetitions one should perform to enhance the strength for a specific muscle. Generally, 8 to 12 repetitions at 40% to 60% of 1-RM are sufficient to enhance muscular strength. An appropriate resistance training regimen involves performing these 8 to 12 repetitions 1 to 3 times, 2 to 3 times per week. While intensities as much as 80% and relatively low repetitions (such as 3-5) have been shown to be quite effective for rapid strength gains, this approach is generally limited to athletes whose performance requires great amounts of force.
It is important to note that intensity for resistance exercise is not always easy to determine and the 1-RM does not depict a true intensity. The number of repetitions and the percentage of resistance based on 1-RM differ significantly between individuals and muscle groups. Thus, the 1-RM should only be used as a general guideline. 2
Muscular Endurance
Muscular endurance is defined as the ability of the muscle or muscle groups to perform repetitive contractions over a period of time against a submaximal resistance, such as lifting a set amount of weight several times. 2 Muscular endurance is assessed by tests requiring more than 12 repetitions. A simple test of muscular endurance is the maximum number of push-ups or sit-ups one can execute without rest. 2
Anaerobic Power
Because anaerobic power is an important determinant of athletic performance requiring high levels of exertion over short periods, tests have been developed to measure the capacity of the anaerobic energy systems. As mentioned, the immediate energy requirements for such high-intensity (anaerobic) activities are met by intramuscular stores of adenosine triphosphate and phosphocreatine for initial 10 seconds (approximately) and by the glycolytic pathways for activities lasting beyond 10 seconds.
One of the more common tests of this type is the Wingate test, which involves 30 to 120 seconds of high-intensity effort on a cycle ergometer. After adequate warm-up, the subject begins pedaling as fast as possible without resistance. Within just seconds, a fixed resistance is applied to the flywheel, while the subject continues pedaling at an all-out effort. The resistance is based on body mass (originally 0.075 kp per kg body mass, though this may vary) and is applied after initial inertia and unloaded resistance are overcome.
Peak power is considered to represent the highest mechanical power generated during any 3- to 5-second period during the test; average power is the average of the total power generated during the test. An underlying assumption of the Wingate test is that peak power reflects the energy-generating capacity of the oxygen-independent high-energy phosphates, whereas average power is a representation of the individual’s glycolytic capacity, but it is not a precise measure of this capacity.32,33 In studies comparing the Wingate test results with athletic performance and laboratory findings, it has been demonstrated to be a good index of these energy systems, although studies are mixed in terms of its ability to predict success in events requiring high exercise intensity. 33