
Abstract
Background. Chronic pain is a major health condition that has significant financial and lifestyle implications. Due to the complex etiologies of pain, it is difficult to find treatment modalities that would be universally applicable to the general population presenting for care. Mindfulness meditation is a complimentary treatment modality that has some preliminary, inconclusive evidence in support of its benefit on patients with chronic pain. Objectives. The purpose of this article is to systematically review the current literature for randomized controlled trials that assess the outcomes of mindfulness as an intervention for individuals with chronic pain. Methods. An electronic database search was performed for studies investigating the efficacy of mindfulness in treatment for chronic pain. The studies included were randomized controlled trials, published in English, from a peer-reviewed journal that identified mindfulness as the primary treatment focus for chronic pain in at least one group, and included participants with at least a 12-week history of symptoms. Results. The database search revealed 283 articles, of which 6 met the inclusion criteria. Conclusion. Mindfulness meditation appears to have minimal or statistically insignificant effects on chronic pain according to the current data. However, the effects of mindfulness on mental health scores are significant and may be an area for future trials to target. Well-conducted research is necessary before the effects of mindfulness on chronic pain can be definitively determined.
‘Meditation is a treatment modality that has been investigated for its effects on managing chronic pain.’
Chronic pain is a common health ailment that affects nearly 100 million adults in the United States. 1 Individuals with chronic pain may also suffer from depression, 2 fatigue, 3 difficulty sleeping, 4 and decreased quality of life. 5 Gaskin and Richard 1 reported that chronic pain in the United States costs up to $635 billion per year in expenses, losses, and decreased employee productivity. This study also suggested that the annual cost of pain in the United States is higher than that of cancer, heart disease, and diabetes, the nation’s principal diseases. 1 A study performed by Engel et al 6 found that “a minority of primary-care back pain patients accounted for a majority of health-care costs.” Additionally, they reported that targeting factors such as dysfunction, pain persistence, and depression may help reduce health care utilization and costs. 6
The etiology of chronic pain is multifactorial and can be caused by diseases of many organ systems. Moreover, chronic pain may be primary or secondary in nature. Disorders of the neuromuscular system such as neuralgia, radiculopathy, disc herniation, and trauma can lead to chronic pain. Epidural fibrosis can lead to Failed Back Surgery Syndrome, another etiology of chronic pain. 7 Autoimmune diseases are often associated with chronic pain as well, with 7.6% to 9.4% of the total population suffering from at least one autoimmune disease. 8 Fibromyalgia, a condition characterized by chronic widespread pain, is present in at least 2% of adults. 9 Endocrine disorders such as Addison’s disease, diabetes, and hypothyroidism can cause chronic pain symptoms or lead to other conditions that cause chronic pain, such as diabetic peripheral neuropathy. Diabetic peripheral neuropathy has an estimated presence between 28% and 50% of all diabetic patients,10-13 with related pain present in 14% of all diabetic patients. 11
Due to the various etiologies, many treatment options exist for treating chronic pain, ranging from conventional to alternative, adjuvant, and invasive options. Nearly 400 000 spine surgeries are performed each year to treat chronic low back pain, with a failure rate between 10% and 40%.14,15 Alternative treatment modalities such as acupuncture, 16 self-hypnosis, 17 and yoga 18 have been shown to have an effect on chronic pain. Fatty acid, 19 willow bark extract, 20 and ginger extract 21 supplementation have been shown to reduce pain related to chronic diseases. Medications such as anticonvulsants, 22 serotonin-norepinephrine reuptake inhibitors,23-25 and COX-2 inhibitors 26 have been shown to be effective in treating chronic pain despite the widespread and well-known side effects. Oral opioids are effective for treating chronic pain, with higher doses leading to greater side effects 27 such as endocrinopathy,28-30 sudden death, 31 and hyperalgesia. 32 Transforaminal steroid injections33-35 and radiofrequency nerve ablation36-39 have been shown to be effective in managing neurological and mechanical pain.
Meditation is a treatment modality that has been investigated for its effects on managing chronic pain. Carson et al 40 analyzed the effects of loving-kindness meditation, a technique that attempts to transfer anger into love and compassion. Forty-three participants who experienced chronic low back pain for a minimum of 6 months participated in this randomized controlled trial. Loving-kindness meditation was successful in reducing the intensity of chronic low back pain (P = .03) as measured by the McGill Pain Questionnaire. Additionally, loving-kindness meditation significantly reduced usual pain (P = .04) as measured by the Brief Pain Inventory. Meditation is a common practice in various religions and cultures and has received attention in the scientific community. Meditation has been defined as “a family of complex emotional and attentional regulatory training regimes developed for various ends, including the cultivation of well-being and emotional balance.” 41 Various meditation techniques have been studied, including transcendental meditation,42,43 Qigong,44-46 and breathing awareness meditation.47,48 Meditation is an attractive modality due to the ease of access and low cost.
Mindfulness meditation is a meditation technique that has been used in clinical trials with mixed outcomes. Mindfulness originated in ancient Buddhism, but was introduced as a therapeutic intervention in the scientific community by Jon Kabat-Zinn in an article published in 1981. 49 Jon Kabat-Zinn began teaching mindfulness meditation in 1979 at the University of Massachusetts Medical School Stress Reduction Clinic. 50 Mindfulness focuses on openness and acceptance of the present moment 51 and has been defined as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally to the unfolding of experience moment by moment.” 50 Mindfulness alters brain activity and functional connectivity 52 and decreases anticipatory anxiety and pain unpleasantness. 53 Mindfulness has been studied on various conditions related to stress such as asthma, 54 HIV, 55 and insomnia. 56 Mindfulness has been used in meditation and stress reduction formats. Mindfulness meditation uses mental techniques traditional to meditation. Mindfulness-based stress reduction (MBSR) can use mindfulness meditation in conjunction with yoga. They are often associated with each other because both techniques primarily use mindfulness to elicit the beneficial response.
Various studies have analyzed the effect of mindfulness on chronic pain, with mixed outcomes. Schmidt et al 57 performed a 3-arm trial on the effectiveness of MBSR on individuals diagnosed with fibromyalgia. Their results showed improvement in sensory and affective measures of the Pain Perception Scale, with P values of .06 and <.001, respectively. Although there was improvement in the MBSR group, there was also statistically significant improvement in the waitlist and active control groups. The 2 significant effects in the MBSR group were reductions in anxiety and increased self-rated mindfulness. Fox et al 58 examined the effects of mindfulness meditation in 22 women with chronic pelvic pain and found a significant improvement in daily maximum pain scores (P = .02). However, this study was uncontrolled and had a 45% dropout rate. Currently, there is no conclusive review on the literature surrounding the effects of mindfulness on chronic pain. The contradicting evidence that is present in the literature prompts the question of whether mindfulness is a useful practice for patients with chronic pain. Therefore, a systematic review of the literature may provide a global assessment of the efficacy of mindfulness on chronic pain.
Methods
A computerized electronic search was conducted on Ovid (1946 to October 1, 2013) and Medline/Pubmed (1950 to October 1, 2013). The following key words were used independently and in combination: chronic pain, meditation, meditates, meditating, and mindfulness. One reviewer (PLR) examined all abstracts of identified studies to determine eligibility. Full-text articles were reviewed if eligibility was not clear in the abstract and to evaluate specific inclusion criteria. If eligibility was not clear, 2 other authors (WJH and MJK) reviewed. A majority consensus was necessary for inclusion into the study. A cross-reference of the reference lists was also performed.
Studies included in the review must have been a randomized controlled trial, appeared in a peer-reviewed journal, been published in the English language, identified chronic pain as the/a primary treatment focus, clearly identified mindfulness as the primary treatment in at least one group, and included participants who had chronic pain for a 3-month period prior to enrolling into the study. Also, selected studies must have used a validated pain outcome measure. Outcome measures were considered validated if previously published studies reported adequate criterion or construct validity. Studies were excluded if the type of meditation was not specified, the duration of pain prior to enrollment into the study was not clearly described, or the study design was not a randomized controlled trial. Quality of the selected trials was assessed using the PEDro scale and when available scores were extracted from the PEDro database, otherwise scores were calculated by the authors.
Study Selection
The initial electronic database search revealed a total of 283 articles. Of those, 20 were selected as potentially eligible based on the title and abstract. Examination of the full-text articles revealed 6 that met the aforementioned inclusion criteria (Figure 1).
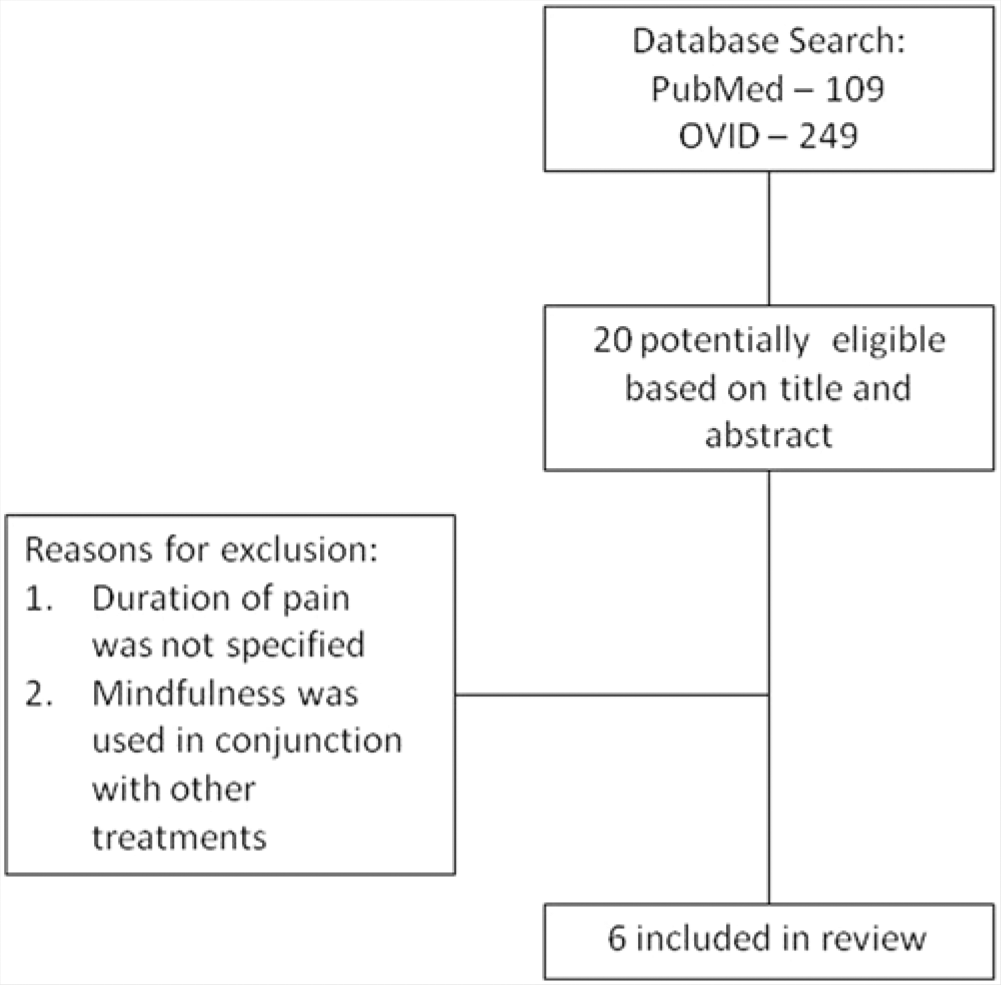
Search Strategy.
Methodological Quality
The methodological quality assessment using the PEDro scale revealed a median score of 5, with a range of 4 to 7. Subject and instructor blinding was not possible for any of the randomized controlled trials due to the nature of the meditation intervention, allowing for a maximum possible score of 8 out of 10. Each of the selected studies used random assignment. All studies reported baseline comparability with no significant difference except the study by Teixeira, 59 which reported differences in pain intensity between groups at baseline. One point of variation was whether adequate follow-up was conducted. The PEDro scale requires 85% follow-up for point allocation. The studies by Wong, 60 Wong et al, 61 Morone et al, 62 and Plews-Ogan et al 63 did not report adequate follow-up. Between-group comparisons, point estimates, and variability were used for all selected trials. The clinical trials identified in this systematic review were also rated based on levels of evidence, which have been included in Table 1.
Study Characteristics, Interventions, and Primary Outcome Measures.
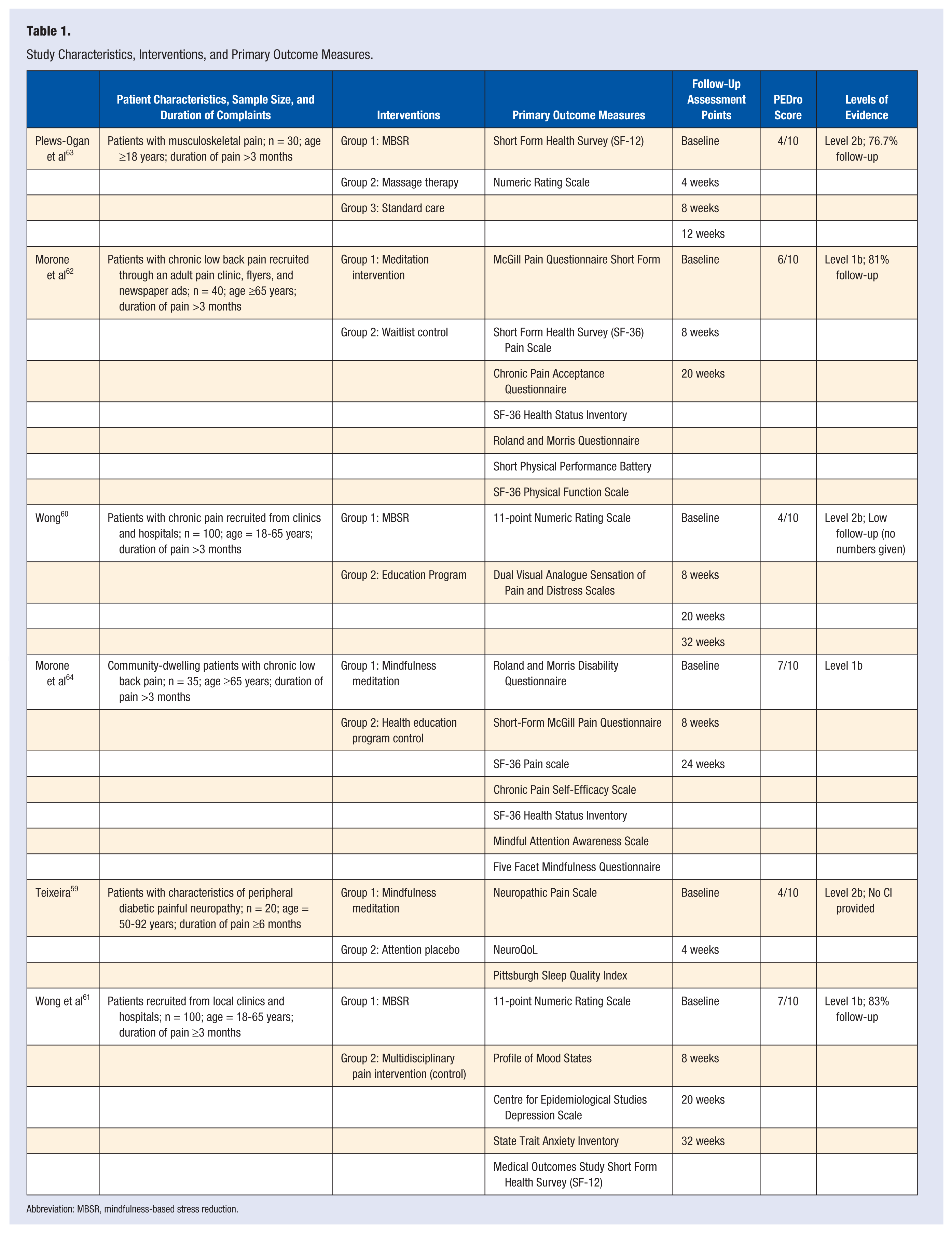
Abbreviation: MBSR, mindfulness-based stress reduction.
Study Characteristics
Mindfulness Meditation
Morone et al 62 compared a mindfulness meditation group with a waitlist control group. They did not find statistically significant improvements in pain intensity but did find significant improvements in pain acceptance in the meditation group. After 8 weeks, the control group crossed over to receive mindfulness meditation instruction, and there were statistically significant improvements in pain intensity (P = .03). Teixeira 59 analyzed the effects of mindfulness meditation in participants with peripheral diabetic neuropathy and found no statistically significant difference between the meditation and control groups for postintervention pain intensity (P = .16) and unpleasantness (P = .96). Morone et al 64 compared a mindfulness meditation group with an active control group. There was a reduction in pain intensity; however, the difference between the meditation and control groups did not reach statistical significance.
The control and intervention groups had baseline comparability similar in both of Morone and colleagues’ studies.62,64 Teixeira’s 59 meditation group had a higher mean pain intensity score than the control group, with an effect size of 0.16. Morone et al62,64 used the same frequency and intervention length with 8 weekly, 90-minute sessions in the meditation group. Teixeira 59 used one, 60-minute session to train the participants in mindfulness meditation prior to the intervention. Morone et al 64 used an active control group and a waitlist control group, whereas Teixeiera used a health education control group. The evidence of the 3 analyzed studies indicates weak evidence for the potential of mindfulness meditation to slightly improve pain intensity in patients suffering from chronic pain.
Mindfulness-Based Stress Reduction
Wong et al 60 did not find a statistically significant difference between the control and MBSR treatment groups for pain intensity, but there was a statistically significant improvement in both groups. There was a statistically significant difference between the 2 groups in pain-related distress, with the control group showing more improvement than the MBSR group. In another study, 60 Wong et al 61 found that both the MBSR and control groups experienced significant improvements in pain intensity until 6 months postintervention.
Plews-Ogan 63 compared MBSR, massage, and control groups, and did not find significant differences in pain outcomes in the MBSR group. Eight weekly, 150-minute sessions were conducted with the MBSR group, and the control group used standard care treatment. Wong et al 61 used 8 weekly, 150-minute sessions and a 7-hour retreat session in the MBSR group. The control group was an active intervention that met for 8 weekly, 150-minute sessions. The results from the 3 analyzed studies indicates weak evidence for the superiority of MBSR potential for reducing pain in patients with chronic pain. In all 3 studies, the evidence indicates weak to no support for the superiority of MBSR for decreasing pain intensity to control groups.
Discussion
MBSR entails the inclusion of therapeutic yoga exercises along with mindfulness meditation techniques, which may lead to different effects compared to interventions using mindfulness meditation exclusively. The extent of the difference between the 2 modalities is unknown. Yoga seems to have a positive effect on chronic low back pain, which may affect the results obtained from an MBSR and mindfulness meditation intervention. 65
While we used mindfulness meditation as key words in our search, meditation as performed may have been different in the various studies. This can be due to multiple factors such as experience and training of instructors, individual participant preference, and intervention organization. If participants are not trained in the same manner, the results of the study may be affected. The goal of mindfulness is common to all approaches, but the thought processes and exercises used may vary due to differences in training. Similarly, various forms of meditation have been used in treatment of disease, and each may have varying effects on different health markers. For example, there is some evidence showing that loving-kindness meditation may be effective in treating chronic low back pain. 40 The effects of mindfulness meditation in the studies analyzed in this systematic review suggest a potential for treatment of psychological diseases.
Exclusively examining articles published in the English language was one of the inclusion criteria. Mindfulness meditation may be more widely practiced and studied in other countries where publications are not always in the English language, and this inclusion criterion may have limited the total number of eligible articles that we examined in our systematic review.
Many factors may influence the successfulness of a mindfulness intervention such as length, frequency, and number of sessions. Plews-Ogan et al 63 suggested that the effects of mindfulness may take time to become evident, which may affect the results obtained from shorter trials involving mindfulness. Similarly, Wong 60 measured improvements in the physical component of the SF-12 in the MBSR group at 6 months postintervention and not at any other, earlier time. In the mindfulness meditation interventions, Morone used 8 weekly, 90-minute sessions in both of her studies trials.62,64 The study performed by Teixeira 59 lasted for 4 weeks, which may not be long enough for the effects of mindfulness to manifest. All of the MBSR trials that were analyzed lasted for 8 weeks, which may be a minimum for effective evaluation of the effects of mindfulness interventions. In a shorter trial, perhaps the study length could be compensated for by increasing the mindfulness session frequency, but it is unknown if the effects of mindfulness are time-dependent or dependent on the number of total sessions.
The effects of mindfulness may also be partially attributable to the group interaction and guidance by health care professionals. 66 All of the studies that we analyzed had weekly meetings with the participants and health care professionals except for those by Teixeira 59 and Wong. 60 Additionally, some of the improvements in pain in control groups may be due to the active, health education model of control groups used instead of waitlist control groups. Active control groups were used in studies performed by Wong, 60 Wong et al, 61 Morone et al, 64 and Teixeira. 59 Also, guidance by instructors in mindfulness techniques may have affected the practice of participants. Teixeira 59 did not have weekly interaction between participants and instructors, which may be a cause of the lack of results in the study.
Confounding variables such as medication use, number of participants, and prior meditation experience may alter the results of a mindfulness meditation intervention. Some studies60-62,64 used prior experience with meditation as an exclusion criterion. In the study performed by Teixeira, 59 9% (2/22) of participants used meditation (not necessarily mindfulness meditation) as a complementary therapy for managing painful diabetic peripheral neuropathy. Previous experience with mindfulness meditation could have led to alterations in intrinsic brain connectivity, as discussed by Kilpatrick et al. 52
Medication use among participants in the reviewed trials may have been a potential source of bias. Among the 6 evaluated trials, baseline use of various analgesics varied. In 2 trials,59,61 acetaminophen was reported to be the most commonly used analgesic medication. Nearly all trials reported participants using opiate analgesic medications, with a range from 1% 61 to 60% 63 of participants. Such a wide range of opiate analgesic use may have lead to significant differences in treatment effectiveness. Patients using stronger analgesic mediations such as opiates/narcotics may have a higher level of pain or specific pain etiologies that may benefit less from mindfulness meditation. It is currently unclear what pain etiologies are most improved by mindfulness meditation, if any.
Changing of medication dose, frequency, or other factors during the duration of the trial may potentially lead to errors. Two of the 6 reviewed trials did not allow participants to receive new treatments for their chronic pain during the interventions, minimizing the effects of altered medication regimes on the interventions.60,61 Other trials did not include this information in their inclusion and exclusion criteria, but it may be a beneficial criterion for future trials investigating the use of mindfulness meditation in populations of patients with chronic pain. Side effects from varied medication use may lead to varied results not necessarily attributable to the mindfulness interventions. Few participants in the evaluated trials reported taking no analgesics for their chronic pain. Participants who did not use any analgesic medications to control their chronic pain represent an ideal situation for investigating the effect of mindfulness meditation on chronic pain, but results may not be applicable to clinical patient populations who may be taking analgesic medications.
Many of the currently available studies on the subject of mindfulness and meditation use small sample sizes and are pilot studies. As measured by the PEDro scale, some studies appear to be of lower quality with multiple scores as low as 4 out of 10. The highest score possible in these trials is 8 out of 10, due to the inability to blind the instructors and participants. Indicative of the low quality of some of these studies, some had small sample sizes and high dropout rates, which may have altered the results. Plews-Ogan et al 63 and Wong 60 reported high dropout rate by participants. In certain studies, the dropout rate in the mindfulness group was higher than that of the control or other groups, perhaps due to the time required by the mindfulness intervention.
The continued practice of mindfulness meditation indicates that there must have some effect. Morone et al 64 reported that after completion, 14/16 (88%) participants continued to practice formal meditation, and 15/16 (94%) practiced informal meditation. The effects of mindfulness are not limited to physical health and have been shown to improve various measures of psychological health such as depression 67 and others. 68
Compliance is a potential problem with consideration in assessing the validity of results of mindfulness interventions. Some studies require significant, consistent time investments by the participants. Morone et al62,64 instructed participants in the MBSR group to practice 6 days per week for 45 minutes each day, in addition to the weekly sessions. In one trial, Morone et al 64 reported an average compliance of 5 days per week with 31 minutes per day among participants in the mindfulness meditation intervention group. In another trial, Morone et al 62 reported an average compliance of 4.3 days per week for 31.6 minutes per day among participants in the mindfulness meditation intervention group. The compliance was self-reported by study participants, which introduces validity concerns. If all participants were fully compliant with the requirement of 6 days per week with 45 minutes per day of mindfulness meditation, the results may be unequal to those of a trial that required 20 minutes per day for 5 days per week. The results of trials may be skewed based on the amount of time spent on mindfulness, which should be standardized in future trials on mindfulness.
Currently, the evidence in support of mindfulness interventions for treatment of chronic pain is weak. The current data show evidence that there may be a potential for mindfulness to slightly improve the intensity of chronic pain, but the main effects of mindfulness are psychological. More high-quality studies need to be performed to reasonably draw a conclusion on the effects of mindfulness on chronic pain. The potential for mindfulness meditation has been established, and more high-quality studies with larger sample sizes are needed at this point. The magnitude of effect on pain by mindfulness appears to be minimal, not even reaching statistical significance in some interventions. Morone et al 62 reported an improvement in the crossed-over control group of 4.3 units on the McGill Pain Questionnaire Short Form (P = .03).
Conclusion
The aim of this systematic review was to assess the possibility of using mindfulness as a therapeutic intervention for treating chronic pain. Six randomized controlled trials were analyzed, all with minimal or statistically insignificant improvements in chronic pain measures. In summary, the current evidence supporting improvement of chronic pain due to mindfulness interventions is weak. Further higher quality studies are required before the effects of mindfulness on chronic pain can be accurately determined.