
Abstract
Bisphosphonates are commonly used as first-line agents in the treatment of postmenopausal bone fragility. Recently, concern has been raised regarding the risk of atypical fracture with long-term therapy. A potential solution to obtaining the benefits while minimizing the risks of bisphosphonate therapy is the use of a drug holiday, or temporary cessation of medication. For drug holidays to be an effective approach, patients must maintain fracture protection while off therapy. One way to optimize fracture protection during this time is to prevent falls. Risk of atypical fracture and bisphosphonate drug holiday will be discussed, along with a summary of the most effective fall prevention modalities.
‘A potential solution to obtaining the benefits while minimizing the risks of bisphosphonate therapy is the use of a drug holiday, or temporary cessation of medication’
Introduction
Two strong determinants of fracture in postmenopausal women include bone fragility and falls. Each year, approximately one third of community dwelling adults age 65 years and older experience a fall. 1 Women sustain both a greater number of falls and make up a higher proportion of fallers than do men. 1 Following menopause, bone resorption outpaces bone formation, resulting in decreased bone mineral density and increased bone fragility. Independently and in concert, bone fragility and falls increase the risk and contribute to the significant morbidity, mortality, and cost associated with fracture. Treatment of bone fragility and prevention of falls are therefore of upmost importance in reducing the number of fractures in this population.
Bisphosphonates are first-line therapy in the treatment of postmenopausal osteoporosis. 2 This class of medication exerts its therapeutic effect on bone by binding to hydroxyapatite and inhibiting bone resorption. 3 This inhibition shifts the action of bone remodeling from greater resorption to greater formation, thereby increasing bone mineral density and strength and decreasing the risk for fracture. Fracture risk is reduced by 30% to 70% at all skeletal sites with bisphosphonate therapy. 4 Peak suppression of bone resorption occurs after 3 months of use and remains relatively stable throughout therapy. 3 Although bisphosphonates are generally well tolerated, limited clinical data exist on the long-term efficacy and safety of these agents. Of specific concern is the association of bisphosphonate use with atypical femur fractures. A potential solution to obtaining the benefits while minimizing the risks of bisphosphonate therapy is the use of a drug holiday, or temporary cessation of medication.
For drug holidays to be an effective approach, patients must maintain fracture protection while off therapy. While lifestyle behaviors, specifically physical activity, may be of negligible benefit for bone health with regard to its effect on bone mineral density, it is of great benefit in reducing fracture risk through its effect on fall prevention. In addition to physical activity, several other lifestyle modifications have been shown to significantly decrease the risk for falls.
The purpose of this article is to discuss the risk for atypical fracture and the evidence regarding bisphosphonate drug holidays as well as to summarize the most effective lifestyle modifications in the prevention of falls.
Long-Term Bisphosphonate Therapy and Atypical Fracture
Concern regarding skeletal fragility as a result of bisphosphonate therapy was first introduced in 2005 following the publication of a case series in which atypical femur fractures were identified in 9 patients treated with bisphosphonates. 5 The case series raised concerns of oversuppression of bone turnover with long-term bisphosphonate use. Normally, skeletal microdamage that occurs as a result of routine daily activity is repaired by the bone remodeling process. Treatment with bisphosphonates suppresses bone remodeling, which may potentially result in bone fragility through an accumulation of unrepaired microdamage.
To date, 4 retrospective studies have assessed the incidence of this adverse effect.6-9 Black et al 6 found no association between bisphosphonate use and atypical fractures with a treatment durations of up to 10 years. Limitations to this study include an event rate of only 12 fractures, confounding use of alternate osteoporosis pharmacotherapy, lack of radiographic evidence for the majority of fractures reported, and the fact that it was a secondary analysis of 3 completed trials. A larger, national register-based matched cohort study found similar results. 7 There was no difference between atypical femur fractures in the bisphosphonate treated group versus their matched untreated controls. There was, however, a significantly higher risk of hip fracture in the untreated group compared with the bisphosphonate-treated group. In contrast, Schilcher et al 8 found an association between bisphosphonate use and atypical fractures in a cohort analysis and population-based case–control study. The analysis also showed longer duration of bisphosphonate use conferred a higher risk of atypical fracture. The fourth study was a population-based, nested case–control study of postmenopausal women. 9 A total of 716 patients experienced an atypical fracture during bisphosphonate therapy over the 7-year assessment period. The analysis demonstrated an increased risk in atypical fracture in women treated with bisphosphonates for 5 or more years, while shorter duration of treatment did not confer significant increased risk.
Conflicting evidence exists regarding the risk of atypical fractures with bisphosphonate use. An association seems apparent, while a relationship of causation is less clear. The evidence that does show an association, demonstrates a small absolute risk, which does not likely outweigh the benefit of preventing osteoporotic fractures. A drug holiday, however, is a potential solution that allows the patient to realize the benefits of bisphosphonate therapy while minimizing the risks associated with long-term use.
Bisphosphonate Drug Holiday
In response to the evidence regarding long-term bisphosphonate therapy and atypical fracture risk, the American Association of Clinical Endocrinologists updated their practice guidelines to suggest a drug holiday for select patients receiving long-term therapy. 2 Drug holidays should be considered after 10 years of treatment for patients at high risk for fracture and after 5 years in patients with mild osteoporosis.
The effects of bisphosphonates appear to be sustained following treatment cessation. Bisphosphonates are incorporated into the bone structure and may remain incorporated in the bone matrix for many years, lending to long suggested half lives (approximately 10.5 years for alendronate) and plausible residual benefit years after treatment discontinuation. 10 A study by Stock et al 11 found that increases in bone mineral density following 2 years of bisphosphonate treatment were retained for 1 to 2 years after the drug was discontinued. A second analysis, the FLEX study, compared bone mineral density, bone turnover markers, and fracture risk in patients randomized to either continued alendronate therapy or drug holiday (placebo). All patients in the FLEX study received 5 years of alendronate therapy before randomization. The results demonstrated that while bone mineral density gradually decreased and bone turnover markers gradually rose in the drug holiday group, both remained improved over pretreatment levels. 10
The FLEX study also evaluated fracture risk following 5 years of alendronate drug holiday. 10 There were no significant differences in the risk of nonvertebral fractures between patients on drug holiday and those continuing with alendronate therapy. On secondary analysis, this continued fracture protection was only demonstrated in women whose bone mineral density was greater than −2.5 when bisphosphonate treatment was discontinued. Results from the FLEX study suggest that fracture protection may be sustained during a 5-year alendronate drug holiday in women at low risk of fracture, while women at high risk of fracture (T score ≤−2.5) may benefit from therapy continued beyond 5 years.
Initial treatment duration and medication adherence should also be considered when employing drug holidays. A study by Curtis et al 12 evaluated the risk of hip fracture after discontinuing bisphosphonate treatment. The study included women aged 60 to 78 years who had been treated with a bisphosphonate for at least 2 years prior to discontinuation. The results showed that the incidence of hip fracture was lower while the patients were actively treated with bisphosphonates compared with the incidence during the drug holiday. Interestingly, this increased incidence was not observed in patients with high adherence rates. Specifically, those who were 80% to 100% compliant (according to the medication possession ratio) had no significant increased risk of fracture.
Fall Prevention
For drug holidays to be an effective approach, patients must maintain fracture protection while off therapy. One way to optimize fracture protection outside the effects of pharmacotherapy, is to prevent falls. Fall prevention strategies should be considered for every individual at risk for fracture (including those individuals using drug therapy for osteoporosis). Table 1 summarizes the most effective fall prevention modalities. Physical activity, specifically multicomponent exercise programs are 1 of only 2 strategies proven to reduce both the number of individuals that fall as wells as the rate of falls. 13 Both group interventions and individualized exercise programs using more than one exercise component have been shown effective in fall prevention. 13 Tai Chi seems to be the most effective single-training modality reported to reduce the number of falls by 37% to 50%. 14
Evidence-Based Fall Prevention Strategies.
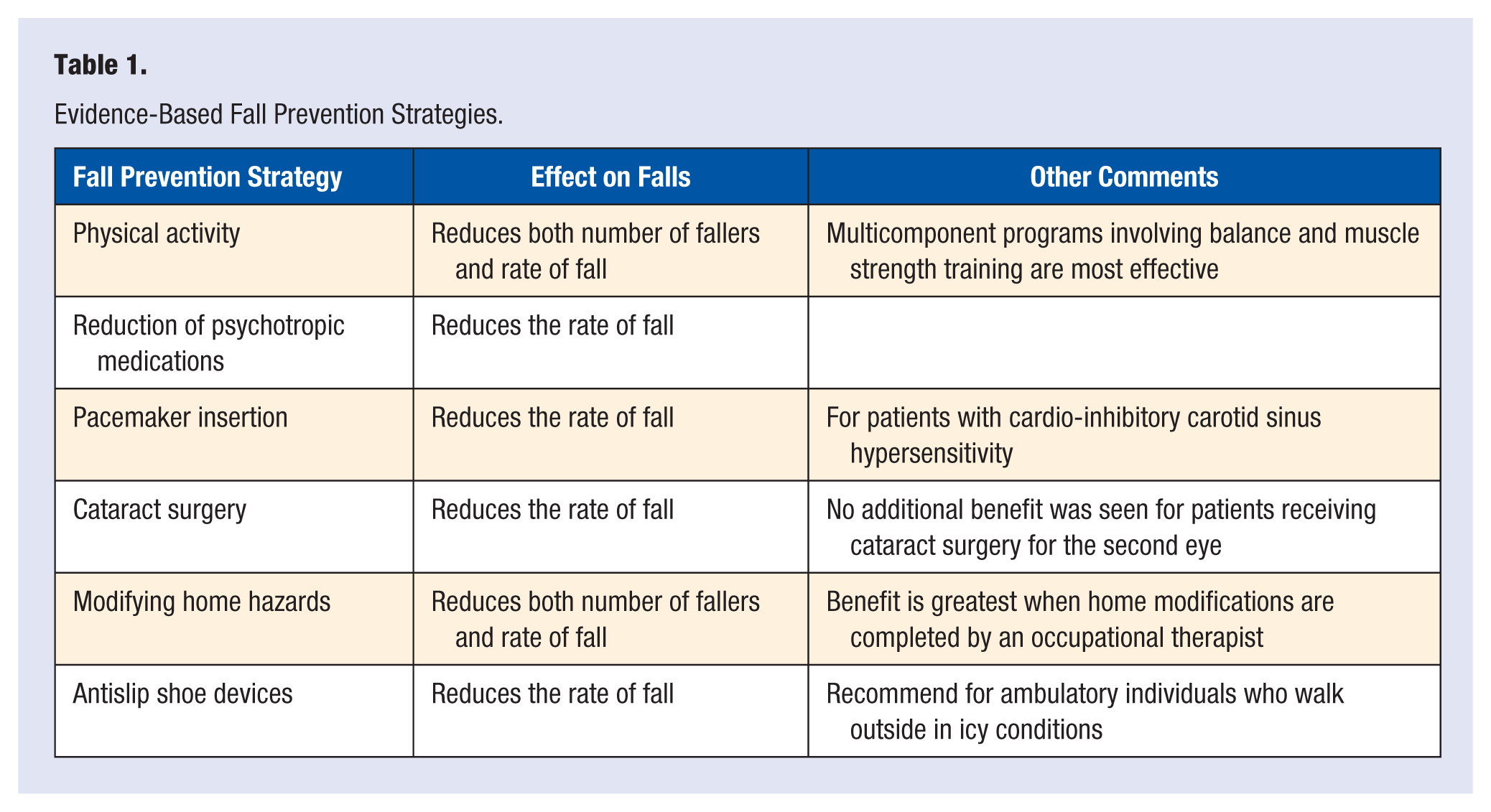
Several medications are known to increase the risk of fall in older patients, most of which are detailed in the American Geriatric Society’s BEERS criteria list. Reducing these medications, especially gradual reduction of psychotropic medications has been shown to reduce the rate of fall by 66% in community-dwelling older adults. 13 Pacemaker insertion and eye cataract surgery, in the appropriate patients, has also been shown to reduce the rate of fall by 58% and 34%, respectively. 13 Modifying home hazards (removing fall-provoking items such as loose rugs and clutter, and installing safety equipment such as grab bars and stair railings, etc) has been shown to reduce falls by 41% and reduce the number of fallers by 24%. This benefit was most obvious when carried out by occupational therapists. 13 Antislip shoe devices have been shown to reduce the rate of fall in ambulatory individuals who walk outside in icy conditions by 58%. Finally, multifaceted interventions, including a combination of the aforementioned strategies have the potential to decrease fall risk and the number of falls.
Conclusion
Postmenopausal fracture is a prevalent health condition associated with significant morbidity and health costs. Two strong determinants in postmenopausal fracture include bone fragility and risk of fall. While bisphosphonate therapy can be used to improve bone mineral density, recent concern has been raised regarding the risk of atypical fracture with long-term use. Bisphosphonate drug holidays are one approach to obtain the benefits of bisphosphonate therapy while minimizing the risks associated with long-term treatment. Initial treatment duration, medication adherence, and t score should all be considered when selecting appropriate candidates for drug holiday.
Anytime fracture is a risk (especially during a bisphosphonate drug holiday), fall prevention strategies are important to implement. The most effective fall prevention strategies include multicomponent exercise programs, reduction of medications known to increase risk of fall, surgical interventions, including pacemaker insertion and cataract repair, use of antislip shoe devices, and implementing programs to modify home hazards.