
Abstract
As the lifestyle medicine movement continues to gain traction and strength, it is critically important that lifestyle medicine practitioners base their recommendations on the best available evidence. This review outlines ways of accomplishing that goal. The core concepts behind lifestyle medicine reside in many different bodies of information. These include nutrition, exercise physiology, behavioral medicine, psychology, and many more. Lifestyle medicine practitioners will need to be knowledgeable in all of these areas. A good place to start is with the evidence-based recommendations put out by major national bodies. The Dietary Guidelines for Americans and Physical Activity Guidelines for Americans also provide comprehensive, evidence-based information regarding these 2 critically important modalities. This review also discusses ways that scientific information is often distorted and how conjecture may sometimes be confused with proof. The review concludes with some recommendations for how lifestyle medicine practitioners can ground their recommendations on sound scientific evidence.
‘It is important for lifestyle medicine practitioners to remain conscientious in their pursuit of the best available evidence in a wide variety of areas including physical activity, nutrition, weight management, . . .’
As the lifestyle medicine movement continues to gain traction, it will be critically important for physicians and other health care professionals who are interested in this discipline to have a firm grasp of the evidence supporting how daily lifestyle habits and actions affect both short-term and long-term health and quality of life. The evidence in the areas that constitute lifestyle medicine is now overwhelming. Unfortunately, the evidence that supports the core concepts of lifestyle medicine is spread over a wide variety of disciplines, journals, books, and evidence-based guidelines. It is important for lifestyle medicine practitioners to remain conscientious in their pursuit of the best available evidence in a wide variety of areas including physical activity, nutrition, weight management, smoking cessation, behavioral medicine, men’s health, women’s health, counseling strategies, coaching, and many other disciplines that constitute the core areas of concern for lifestyle medicine.
The purpose of this article is to review the evidence supporting the multiple impacts of lifestyle practices and habits on health. Levels of evidence will also be discussed with a significant emphasis on the difference between conjecture and proof. Several case studies will also be presented where widely accepted beliefs are not supported by scientific evidence and conclude with a discussion of the unique challenges and opportunities for applying solid scientific evidence to lifestyle medicine.
Background
This review starts with the fundamental premise that an overwhelming body of scientific evidence exists supporting the linkages between lifestyle habits and practices on both short-term and long-term health and quality of life. This evidence is incorporated as a central tenant of the major authoritative guidelines involving both the prevention and treatment of chronic disease in virtually every area of metabolic conditions including coronary heart disease (CHD), diabetes, obesity, hypertension, nutrition, and many others both for adults and children. Some of the core, evidence-based guidelines that emphasize lifestyle medicine practices are listed in Table 1.1-12
A Sample of Evidence-Based Guidelines That Emphasize the Importance of Lifestyle Habits and Practices to Prevent or Treat Chronic Disease.
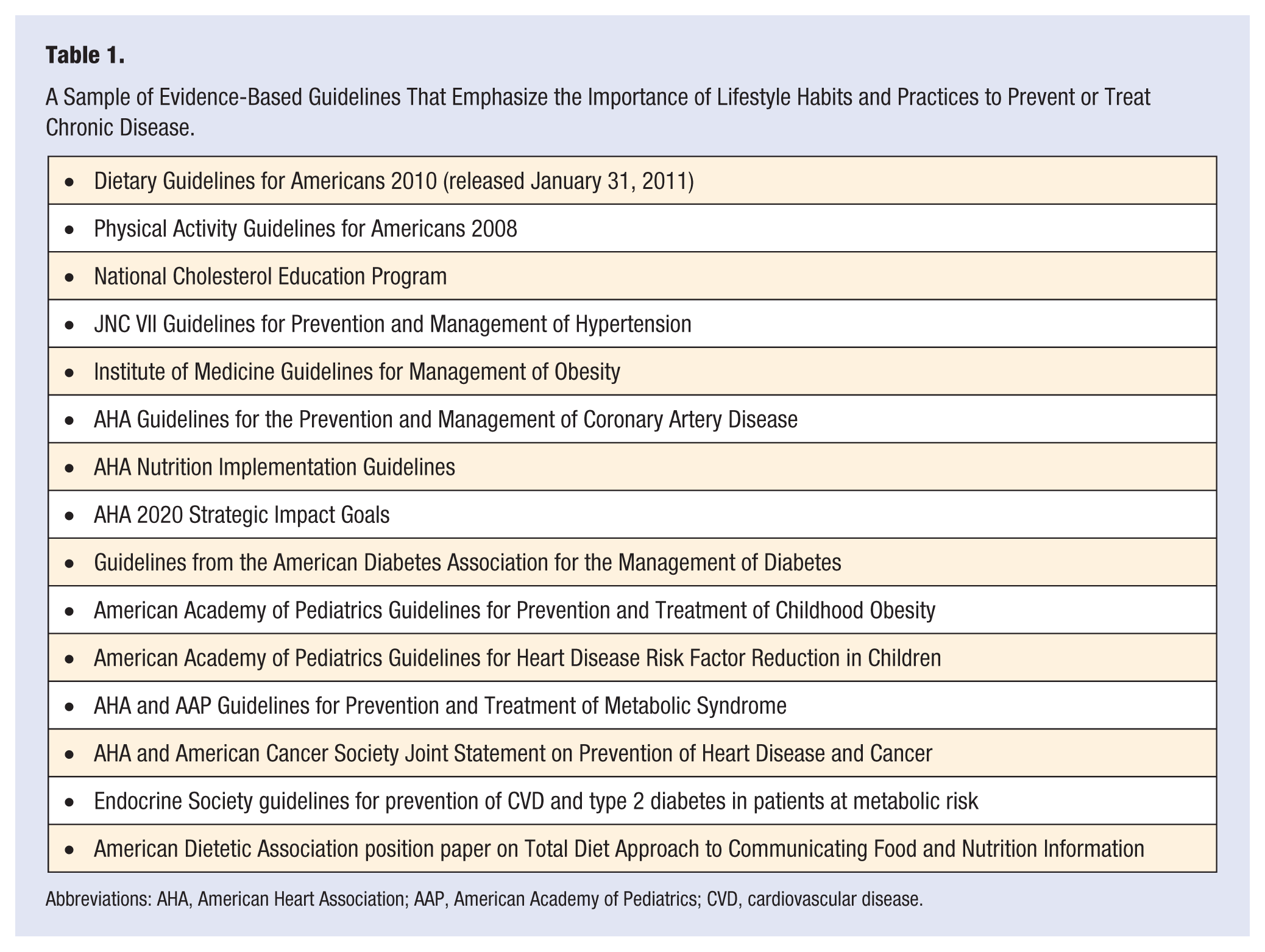
Abbreviations: AHA, American Heart Association; AAP, American Academy of Pediatrics; CVD, cardiovascular disease.
While this review will focus largely on evidence supporting positive lifestyle habits and practices and their relationship to good health, it is important to emphasize that medicine is both an art and a science. A firm knowledge of evidence is only the beginning. It must be coupled with the thoughtful and compassionate practice of medicine to help people make positive changes in their lives.
Behavior changes are multifaceted and difficult, and while there is very significant evidence in how behavior change can be brought about, it is important to remember that the quality of the doctor–patient interaction is now emerging as a significant component of whether or not patients will take our advice to change behaviors that may be harming their health.
My research organization, Rippe Lifestyle Institute (RLI), has been devoted for many years to providing research in the interface between lifestyle habits and practices and health. We have also sought to engage other investigators and health care professionals to provide evidence-based literature in this area. These efforts have resulted in a number of comprehensive publications over the past few years. For example, in 2012, we edited the Encyclopedia of Lifestyle Medicine and Health 13 (SAGE Publications; http://www.sagepub.com/refbooks/Book230684).
This 2-volume encyclopedia brought together the vast experience and wisdom of more than 255 contributors who wrote more than 350 essays on every conceivable topic related to lifestyle habits and practices and their impact on health. It may be found in many large public and university libraries. The intent of the encyclopedia was to provide evidence-based literature to the educated public seeking real answers to issues of how to incorporate positive lifestyle practices into their lives to promote good health.
In 2013, the second edition of our Lifestyle Medicine textbook was published. 14 This textbook brought together the skill of more than 200 distinguished health care professionals and researchers who provided state-of-the-art, scientific evidence in the major areas that constitute the discipline of lifestyle medicine. The intent of this textbook was to provide lifestyle medicine practitioners with one comprehensive source of evidence-based information to establish firm grounding for their daily practice and to advance the field of lifestyle medicine.
In addition, in 2013, my Research Director, Ted Angelopoulos, and I edited an academic textbook titled Obesity: Prevention and Treatment. 15 In many ways, obesity represents the quintessential lifestyle disease incorporating issues related to physical activity, sound nutrition, and behavioral management.
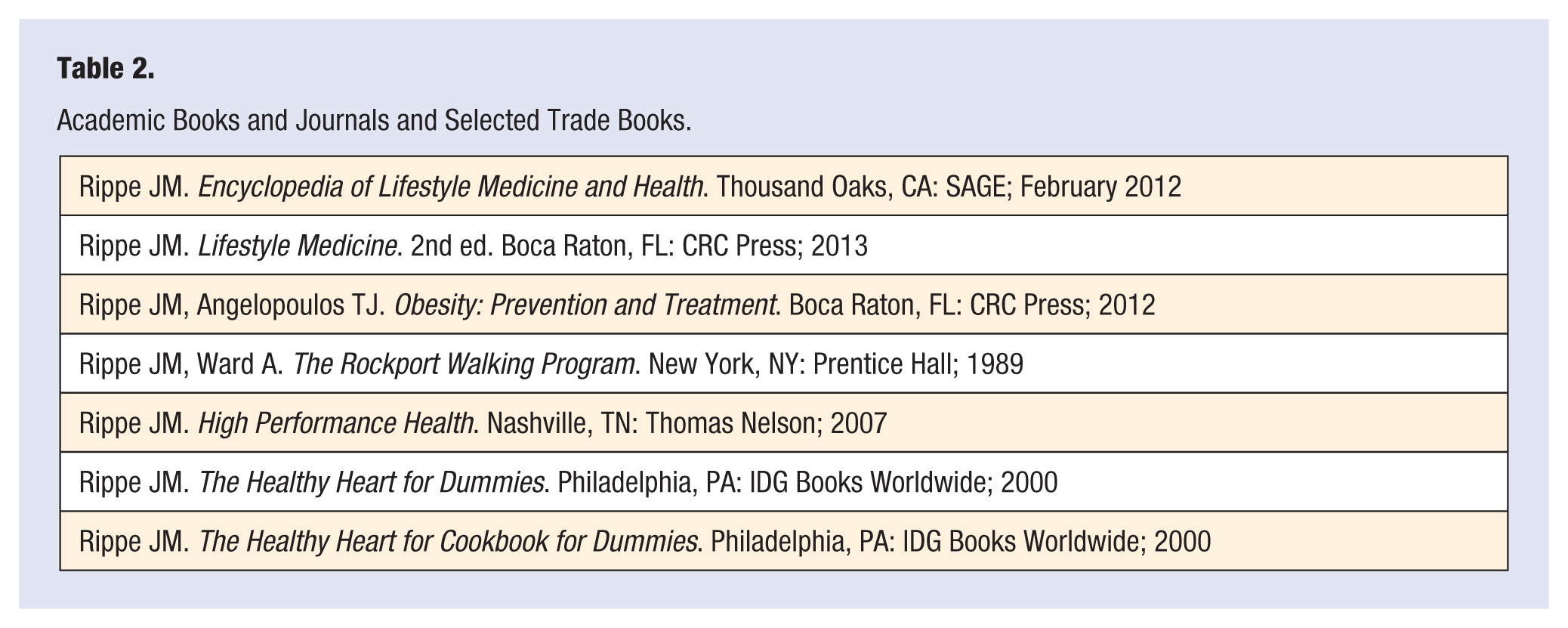
In addition to these academic textbooks, I have been honored to serve for the past 8 years as the Editor in Chief of the American Journal of Lifestyle Medicine, whose mission it is to provide a forum for lifestyle medicine professionals to exchange ideas and evidence. Finally, my organization has attempted to bring the message home to the public with a series of books for the lay person based on research performed in our laboratory and in many others. A selective sampling of some of the books that we have generated may be found in Table 2.16-19 Of course, these books represent only one organization’s contributions to lifestyle medicine. The field has been greatly enhanced and expanded by the contributions of many other researchers and investigators, all of whom focus on the ever-expanding knowledge of how lifestyle affects health.
Academic Books and Journals and Selected Trade Books.
What Constitutes Strong Science?
Practitioners of lifestyle medicine must always evaluate evidence through the lens of what constitutes strong science. In this area, it is crucial that evidence from studies be based on well-designed trials encompassing diverse and large sample sizes. Human studies are preferred to animal studies because of the significant differences of physiology between human beings and most animal models, which are often used to initiate research and raise hypotheses in various areas. A hierarchy of evidence also exists, and it is crucial to understand that the highest level of evidence comes from randomized controlled trials. Often epidemiologic studies and other forms of observational data are misinterpreted to suggest cause and effect when they are only capable of raising questions and establishing associations. The longer the duration of research studies, the more likely they are to generate strong evidence.
Case Studies
In this section, I will offer several case studies to illustrate the importance of evaluating evidence before leaping to conclusions in areas related to lifestyle medicine.
Case Study 1: Does Sugar Cause Obesity?
The issue of whether or not sugar causes obesity recently became prominent both in the scientific community and the public at large when 2 well-known obesity experts reported a temporal association between rise in prevalence in obesity in the United States and consumption of high fructose corn syrup (HFCS). 20 These investigators noted that in the same timeframe that HFCS became more commonly used in the United States, obesity levels also rose (see Figure 1).
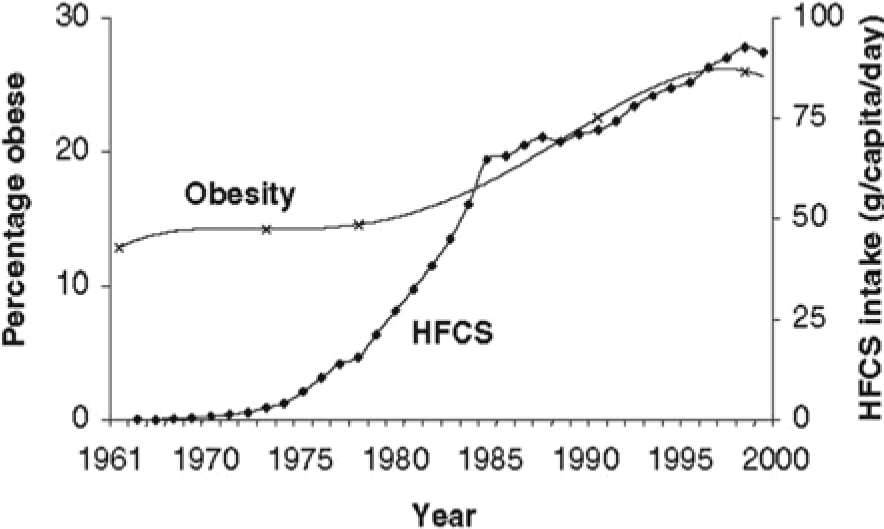
Temporal association between increase in prevalence of obesity and high fructose corn syrup consumption in the United States, 1970-2004.
This article led to a virtual explosion of comments on the Internet with many well-intentioned physicians and others jumping in to offer opinions that this relationship was true. It even caused some manufacturers to eliminate HFCS from their products.
There were multiple problems, however, with this concept. First, a temporal relationship does not establish cause and effect. For example, during the same timeframe, bottled water consumption also exploded in the United States (see Figure 2). Moreover, consumption of asparagus and use of cell phones also increased substantially during this period of time. The point is, of course, that temporal relationships do not establish cause and effect. Furthermore, there has been a dramatic decrease of sugar consumption (both sucrose and HFCS) in the United States over the past 12 years, and these data are not included in the original article that postulated this relationship. 21
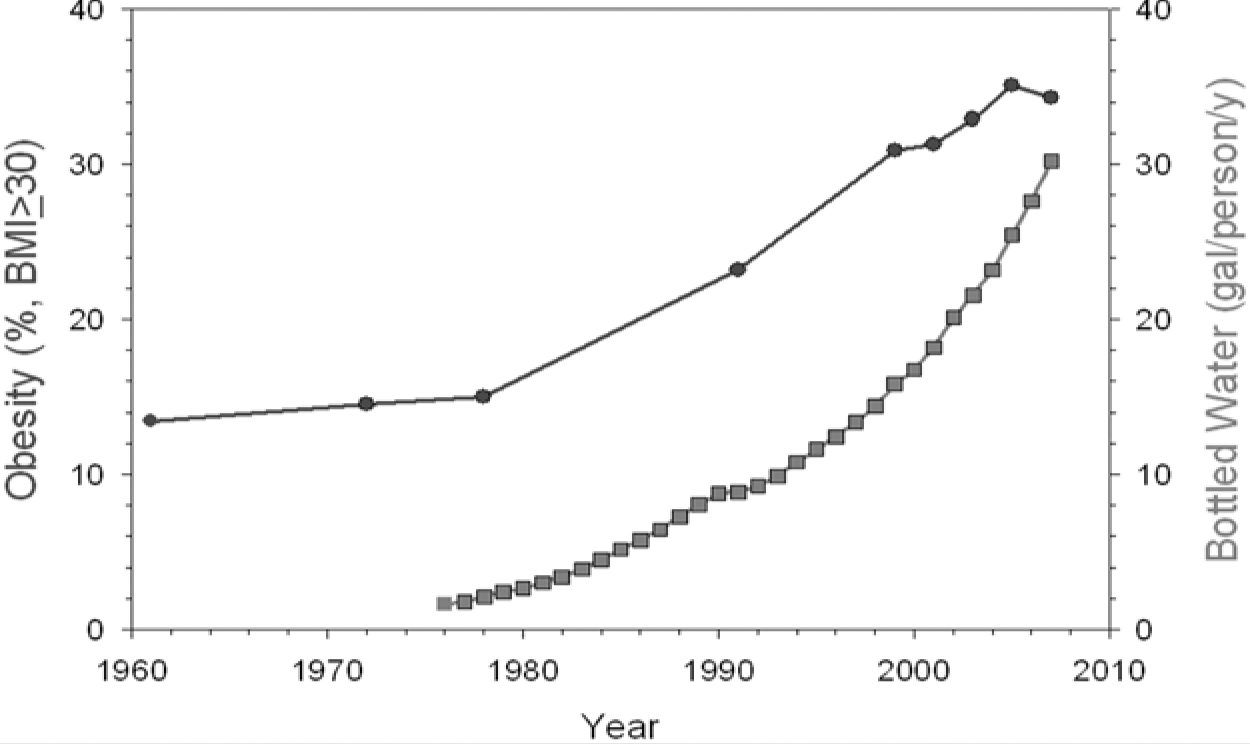
Temporal association between prevalence of obesity and bottled water consumption in the United States, 1970-2004.
The debate was further complicated by some investigators studying large quantities of pure fructose and comparing them to pure glucose.22-24 These studies demonstrated that the 2 sugars had different effects on energy regulating hormones such as insulin, leptin, and ghrelin, with glucose stimulating greater spikes of insulin, a greater leptin response, and more suppression of ghrelin than did fructose. The major problem with these studies was that human beings essentially never consume fructose or glucose alone. When these experiments were repeated with real-world conditions, using either sucrose or HFCS, both of which contained approximately 50% fructose and 50% glucose, all differences disappeared. 25
It should also be noted that during the period of time between 1970 and 2010, the average adult in the United States increased their caloric consumption by 458 calories according to data from the US Department of Agriculture Economic Research Service, and HFCS was responsible for less than 3% of that increase. 26 All these considerations point to the complexity of obesity and the danger of blaming one particular component of the diet as a major cause of this very complex condition that involves calorie consumption from all sources, genetic influences, other environmental influences, and level of physical activity. 27
Case Study 2: Are Certain Foods Addictive?
Some investigators have argued that certain foods may be “addictive,” leading to overconsumption of energy-dense foods (eg, high fat or high sugar) or foods that may be particularly pleasurable (eg, chocolate, ice cream, potato chips, etc), which are often high fat and/or sugar. 28 Some investigators have advocated the use of the Yale Food Addiction Scale (YFAS) to determine whether or not individuals are addicted to certain foods. 29 An academic textbook was even published in this area titled Food and Addiction: A Comprehensive Handbook. 30
Much of the argument related to food and addiction is based on either animal data or highly artificial experiments. This model also adopts a drug abuse model that may be poorly mimicked in human beings when it comes to food consumption. Nonetheless, this argument resonates strongly with the media and the public and has been perpetuated rather uncritically.
The science, however, does not support a food addiction model. Based on DSM-V Criteria for Substance Abuse Disorders, there is very little evidence for food addiction. Moreover, most obese people do not meet YFAS criteria. 29 A substantial portion of underweight and normal weight subjects do however. Thus, the YFAS criteria may not be appropriate for diagnosing food “addiction.” In addition, brain imaging studies (such as functional magnetic resonance imaging) do not support an addiction model. Finally, and perhaps most important, much of the food-related pathology that is seen clinically can be explained and treated without invoking addiction, and in some cases using an addiction model may lead to further food-related pathology. These considerations have been outlined in 3 recent reviews disputing the applicability of the addiction model to obesity and food consumption.29,31,32
Case Study 3: Do Certain Foods Cause Cancer?
Numerous studies from the field of nutritional epidemiology have been undertaken seeking to identify factors that affect major health outcomes including cancer risk. These studies often influence dietary guidelines and public policy and receive wide attention in the news media. The use of large databases may amplify statistically significant, but clinically irrelevant, findings. Moreover, the interpretation of these studies may be extremely difficult.
Several investigators recently adopted a novel approach to putting some of the nutritional epidemiology studies in perspective. These investigators conducted a systematic cookbook review where they selected 50 common ingredients from random recipes in a well-known cookbook. 33 They reported that 80% of these ingredients had articles published in the nutritional epidemiology literature reporting cancer risk. Moreover, when investigators reviewed the actual studies, the association was either weak or had minimal statistical significance. These investigators conducted a meta-analysis by combining all these studies, which did not support increased risk of cancer from these ingredients. Thus, it is very important to look closely at the evidence when it involves areas where there is great anxiety such as in the case of cancer risk.33,34
Case Study 4: Does Exercise Lead to Weight Loss?
A number of studies have been published suggesting that regular exercise is not effective for weight loss. In this area, it is important to make a clear distinction between initial weight loss and maintenance of weight loss. The National Weight Control Registry 35 and the Weight Watchers Group Leaders Program 36 have both shown that individuals who pay attention to what they eat on a daily basis, as well as performing exercise on a regular basis, are more likely to lose weight and keep it off when compared with individuals who do not follow these practices. Here the important distinction is between short-term weight loss and maintenance of weight loss. While exercise by itself may not be a particularly effective modality for short-term weight loss, it is critically important for the long-term maintenance of weight loss. It has been argued that the ultimate recommendation for losing weight and maintaining the weight loss may ultimately be to eat more rather than less (Dr Russell Pate, personal communication).
Case Study 5: Do Sugars Cause Diabetes?
Several recent ecologic studies have suggested an association between sugar consumption and diabetes.37,38 Unfortunately, these studies have been misinterpreted to suggest that there is a causal link between sugar consumption and diabetes. In reality, ecological research studies represent a low form of evidence and are subject to multiple potential confounding errors. Indeed, other ecologic studies have found the reverse—that sugar consumption has declined in countries such as the United States and Australia where obesity has continued to rise or at least stay the same. 39
These conflicting data highlight the important limitation of drawing conclusions about sugar consumption and diabetes from ecologic studies. It is very difficult to disentangle whether associations seen in the ecologic studies is caused by sugar consumption, excess energy, their interaction, or the collinearity of sugar consumption with other dietary and lifestyle factors associated with diabetes, obesity, and overall cardiometabolic risk. Furthermore, in the situation of the United States, added sugar consumption has been accompanied by even larger increases in consumption of protein, fat, and other carbohydrates, further complicating ecological analyses. 40 The inability of such studies to account for all changes opened all ecological analyses to what has been called the “ecological fallacy” and reinforces the need for applying higher level evidence such as that obtained from randomized controlled trials and prospective cohort studies, which have not suggested a direct link between sugar consumption and risk of developing diabetes.
Common Ways That Scientific Evidence Is Distorted
Dr David Allison and colleagues have offered a framework for exploring common ways that scientific evidence may be misinterpreted. They list the following 7 ways that scientific evidence may be distorted:
Investigators describing studies demonstrating associations as having demonstrated causation
Press releases that markedly distort the evidence in studies
Statements in abstracts that do not accord with the results in the same papers
Incorrect citations of past studies in ways that exaggerate their findings
Publication bias in which studies with supportive results may seem more likely to be published than are those with negative results
A disconnect between scientific study and public health media advertisements
Revision of the primary outcomes reported in a study when a significant result in not obtained related to the original primary outcome
(Source: Simple Steps That Could Improve the Use, Reporting and Interpretation of Epidemiologic Research from Experimental Biology Meeting 2013. Used with permission of Dr David Allison)
Potential Reasons for Confusing Conjuncture With Proof
Allison and colleagues also have produced an interesting model for why conjuncture may be confused with proof. 41 They argue that the following factors may be in play that can perpetuate myths or misinterpretations:
Cognitive dissonance where the actual reality may be different from what investigators think it should be
Repeated exposure to erroneous claims where either investigators themselves or other individuals citing their work continue to promulgate claims that are conjecture and not proven
Confirmation bias where investigators start out with a point of view and then establish experiments to try to confirm their initial point of view even if it is biased
White Hat Syndrome—the desire to fix a perceived problem (a common mindset that motivates people to choose the health care professions)
A Modest Proposal for Evaluating Evidence in Lifestyle Medicine
I would suggest that a good start for grounding the future of lifestyle medicine in the strongest available evidence would use the following steps:
Start from the peer reviewed, evidence-based national guidelines including documents such as the Dietary Guidelines for Americans 6 and the Physical Activity Guidelines for Americans 42
Use peer reviewed, evidence-based guidelines such as those I have outlined in this article (Table 1) from major medical organizations
Critically evaluate the levels of evidence to sort out the hierarchy of evidence ranging from randomized controlled trials (highest) to less robust forms of evidence such as epidemiologic studies
While these steps will, in my opinion, help ground practitioners of lifestyle medicine more firmly in the evidence, it is important to never forget that medicine is both an art and a science. Lifestyle medicine practitioners must also learn and adopt research proven behavioral change techniques. It is also important to “walk the walk” since we know that practitioners who pay attention to such issues as proper nutrition and weight maintenance in their own lives are much more likely to effectively counsel their patients in these areas and carry more credibility. We also need to focus on active listening and recognize that change is hard, but not impossible.
The future of lifestyle medicine is indeed bright and the world seems to be rushing toward us. For example, the American Heart Association Council on Nutrition, Physical Activity and Metabolism recently changed its name to the Council on Lifestyle and Cardiometabolic Health. 43 Furthermore, the goals of the Affordable Care Act and Accountable Care Organizations it established can only be achieved through the application of lifestyle medicine techniques and practices.
The evidence supporting the efficacy of positive lifestyle habits and practices to promote good health is real and overwhelming. It is incumbent on all of us who care about and practice lifestyle medicine to know and employ this evidence.
Footnotes
Author’s Note
This article is based on a talk delivered at the American College of Lifestyle Medicine 2013 Annual Meeting on October 28, 2013. This speech was sponsored in part by an unrestricted grant from the ConAgra Foods Science Institute.