
Abstract
Over recent decades, abundant scientific evidence has led to authoritative dietary guidelines and recommendations for heart healthy eating and lifestyle behaviors. But most children and adults do not regularly achieve these goals. Consequently, our focus must now be on helping individual patients and our communities implement these guidelines in everyday life. This article reviews current evidence for insights and practical techniques that can help individuals move from ideal goals to real practice of heart healthy nutrition and lifestyle behaviors.
The purpose of this review is to describe the current landscape of dietary recommendations for heart health. We also intend to identify influences on heart healthy eating and lifestyle behaviors. Finally, we will describe counseling strategies and techniques to help individuals implement heart healthy behaviors in their daily lives.
Over the past decade, a dramatically expanded view of prevention has evolved. Leading the way in this regard have been such national organizations as the American Heart Association (AHA), the Preventive Cardiovascular Nurses Association, and the American Dietetic Association to name but a few. What unites all these efforts is the desire to provide an evidence-based approach toward implementing various heart healthy guidelines. Our focus in this review will be specifically on implementing nutrition guidelines for cardiovascular health.
Many health care professionals now concur that we must move from simply developing evidence-based guidelines into a new era where our focus will be on implementing these guidelines.
We have characterized the implementation process as moving from “ideal to real.” Many health care professionals now concur that we must move from simply developing evidence-based guidelines into a new era where our focus will be on implementing these guidelines.
In a sense, this new emphasis reflects the prevailing belief among many health care professionals, which is shared by the authors of this review, that despite promulgating evidence-based guidelines, we have fallen short in developing research-proven strategies for how these guidelines can be implemented in people’s daily lives.
How else can we explain the fact that approximately 21% of the adult population in the United States still smokes 1 or that only 21.9% of the adult population accumulates at least 30 minutes of moderate brisk activity on 5 or more days per week. 2 Furthermore, more than two thirds of the adult population in the United States is either overweight or obese 3 and only 25% to 30% of adults follow the simple nutritional practice of consuming five or more servings of fruits and vegetables daily.4,5
The health-related behaviors cited in the preceding paragraph are not chosen at random. In fact, an analysis of data from the Nurses Health Study showed that 74% of all cardiovascular disease (CVD), 82% of coronary heart disease, and 91% of diabetes in women could be prevented by following 5 simple lifestyle behaviors: not smoking, regular physical activity, maintaining healthy weight, eating healthier food, and moderate alcohol consumption. 6
These benefits are not confined only to women. The Health Professionals Follow-up Study, which was composed of men 40 to 75 years old, showed that study participants having 1, 2, 3, 4, or 5 of the same healthy behaviors had 54%, 63%, 71%, 78%, or 81% lower risk of these same diseases compared with men with no healthy behaviors. 7
Sadly, when all of these behaviors are combined, these studies have shown that only 4% or 5% of the adult population in the United States follows all 5 of these proven strategies for lowering the risk of heart disease and diabetes.6,7 Furthermore, in a scientific statement published in 2010, the AHA estimated that the prevalence of ideal cardiovascular health at only 5% of US adults. 8
The lack of adherence to these simple principles appears to underlie the slower decline in coronary death rate recently experienced in both men and women. Data from the National Vital Statistics System of the National Center for Health Statistics, as analyzed by Ford et al 9 , indicate that after peaking in 1968, the age-adjusted death rates from coronary heart disease began to decline. Between 1980 and 1989, for instance, the coronary death rate declined at 5.4% per year in women (35-55 years old) and at 6.2% per year in men (35-55 years old). However, by 2000-2002, this decline had leveled off: During this period, declines in men (35-55 years old) were only 0.5% per year and in women (35-55 years old) death rates actually increased by 1.5% per year. Researchers attributed this decline in approximately equal measure to reductions in major risk factors and to increased use of evidence-based medical therapies. It is possible that the low percentage of individuals who follow all or most of the major lifestyle practices recommended for the reduction of CVD and comorbid conditions has contributed to this slowing of progress. (This concept will be pursued in more detail later in this review.)
The Landscape of Dietary Recommendations for Heart Health
Dietary guidelines are typically framed as dietary recommendations for the prevention of chronic diseases or the promotion of health, or both. Table 1 lists major dietary guidelines that are familiar to all health care professionals.10-16 The first 5 items in Table 1 name current guidelines that address dietary recommendations related to the prevention of CVD and its major risk factors. The last bullet lists the most recent Dietary Guidelines for Americans (DGA) whose traditional purpose has been to recommend nutrition practices that promote the general good health of all Americans 2 years or older; given the increased prevalence of overweight/obesity and poor diet and physical inactivity, the DGA 2010 has expanded its recommendations to include prevention of chronic disease. 15 The public facing My Plate (formerly MyPyramid) Food Guidance system is based on the DGA and in keeping with the expanded goal of the DGA is intended to make recommendations about energy balance, food group intakes, and portion control more clear (http://www.ChooseMyPlate.gov).
Major Dietary Guidelines
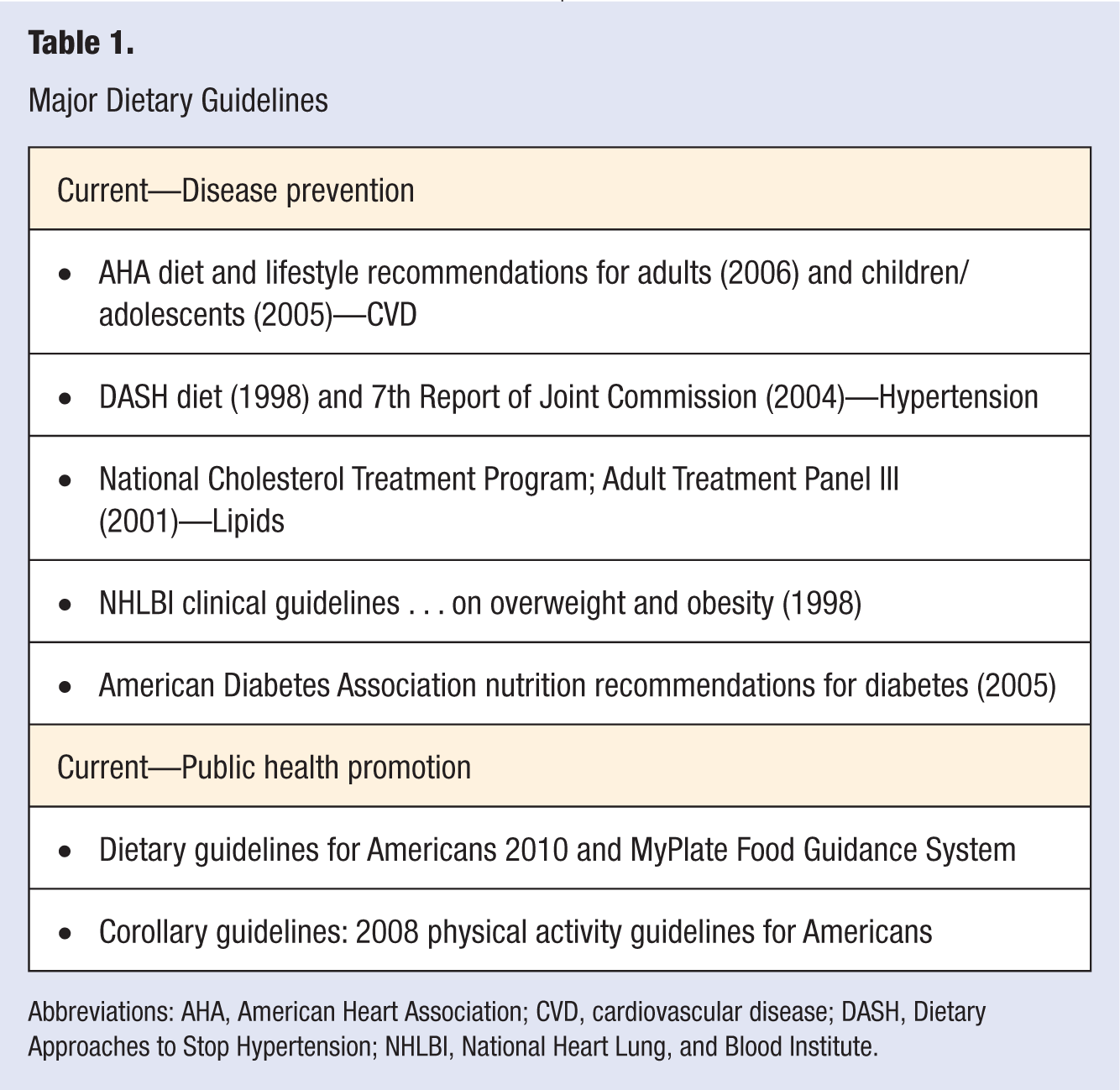
Abbreviations: AHA, American Heart Association; CVD, cardiovascular disease; DASH, Dietary Approaches to Stop Hypertension; NHLBI, National Heart Lung, and Blood Institute.
The final bullet point in Table 1 represents an important set of corollary guidelines that were issued in 2008 recommending physical activity levels for both children and adults.
Such nutrition guidelines have been in wide use for decades as a means to educate patients and the public about what constitutes a healthful or disease preventing diet and to encourage their adoption of the healthy practices. These guidelines also served as the basis for the AHA Strategic Cardiovascular Health Promotion Goals for the Year 2020 as they relate to dietary aspects of cardiovascular health and reduction of risk factors. 8
Although multiple different guidelines have been developed, they are strikingly similar both in both intent and content. Although the DGA 2010 and the AHA Diet and Lifestyle Recommendations tend to be presented first in terms of eating whole foods in the context of healthful eating patterns and the other guidelines tend to first emphasize specific nutrients or food components, there is a striking consistency among the recommendations for nutrient and energy intakes as shown in a review by Krebs-Smith and Kris-Etherton 17 and presented in Table 2. Although the DGA 2010 has increased emphasis on energy balance and weight management and has increased its discussion of specific foods to decrease as well as increase, its overall nutrient and energy intake recommendations are consistent with DGA 2005. A recent analysis by Flock and Kris-Etherton 18 of the implications of the DGA 2010 for CVD concludes that convincing evidence supports the effectiveness for preventing CVD of the DGA recommendation of nutrient dense, food-based eating patterns that emphasize intakes of fruits and vegetables, legumes, whole grains, fiber-rich foods, low-fat dairy, lean proteins, and vegetable oils, and reducing intake of foods high in saturated and trans fatty acids, dietary cholesterol, added sugars, refined grains, and sodium.
Comparison of Recommendations of Authoritative Guidelines
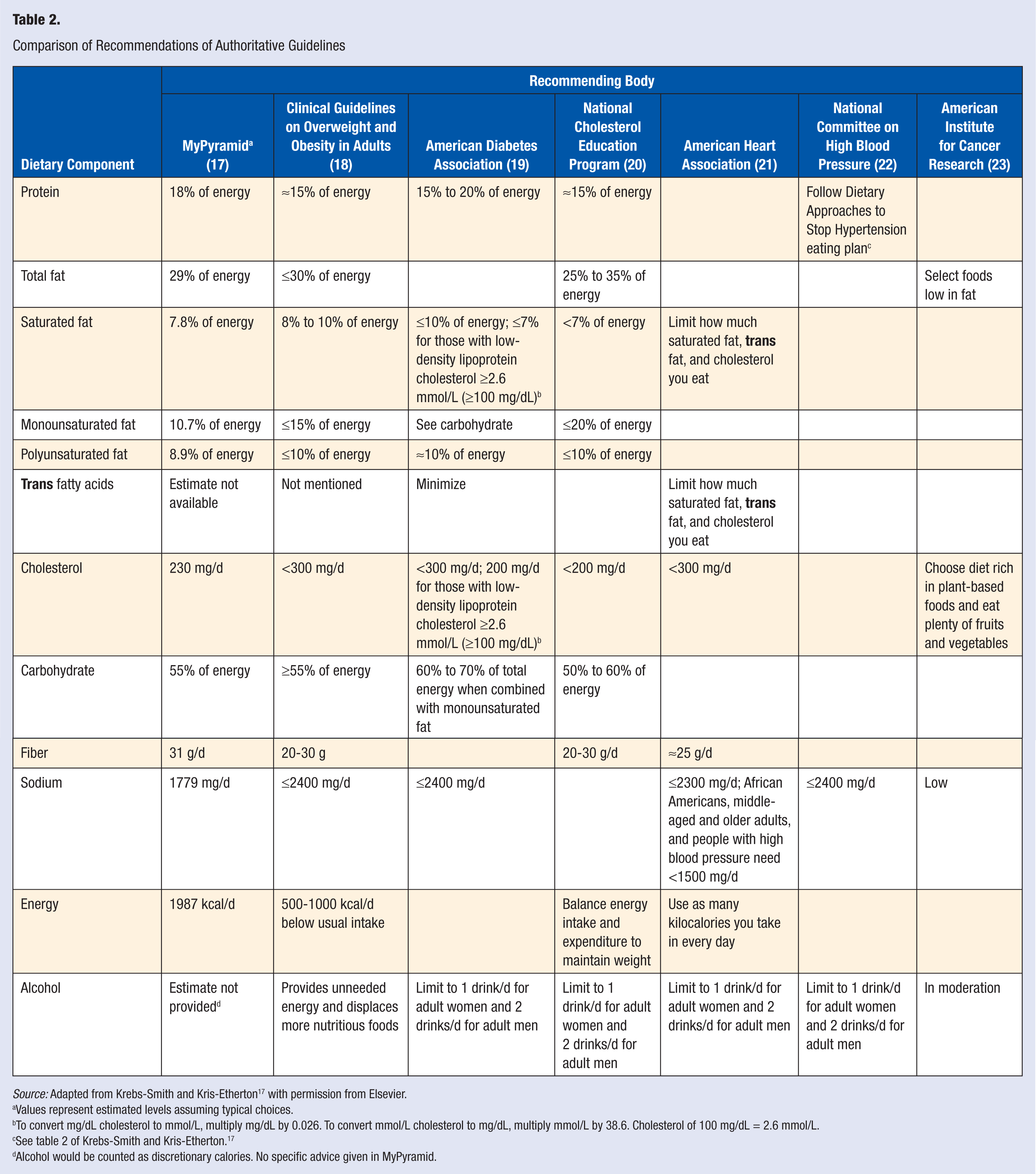
Source: Adapted from Krebs-Smith and Kris-Etherton 17 with permission from Elsevier.
Values represent estimated levels assuming typical choices.
To convert mg/dL cholesterol to mmol/L, multiply mg/dL by 0.026. To convert mmol/L cholesterol to mg/dL, multiply mmol/L by 38.6. Cholesterol of 100 mg/dL = 2.6 mmol/L.
See table 2 of Krebs-Smith and Kris-Etherton. 17
Alcohol would be counted as discretionary calories. No specific advice given in MyPyramid.
Impact on Cardiovascular Disease
Clearly, these guidelines and the degree to which they have been implemented have had a positive impact on CVD in the United States. Deaths from CVD and stroke have declined for the past 4 decades 8 ; however, in the latest preliminary data from 2009, these 2 conditions are still leading causes of morbidity and mortality ranking first and fourth among the leading causes of mortality in the United States. 19
The reduction in the prevalence of risk factors and advances in treatment therapies have both contributed to the decline in deaths from CVD and stroke. 9 Unfortunately, the increased prevalence of diabetes, obesity, and the aging of the population in the United States have created trends in the opposite direction. Efforts to continue to reduce the incidence and burden of CVD and stroke must, therefore, address all these trends.
An analysis by Ford et al 9 exploring a decline in age-adjusted death rates for coronary heart disease from 1980-2000 estimated that there were 341 745 fewer deaths in 2000 as a result of risk factor reduction and advances in treatment. Treatment advances (eg, preventive therapies after myocardial infarction or revascularization, initial treatments for acute myocardial infarction or unstable angina, advances in treatments for heart failure, revascularization for chronic angina, and other therapies) accounted for 47% of the decline according to this analysis whereas risk factor reduction resulted in 44% of the decline. 9
Increases in obesity and diabetes, however, have undercut advances in risk factor reduction. As depicted in Figure 1, increases in obesity and diabetes have undercut some of the advances in cholesterol reduction, blood pressure control, decreased prevalence of smoking, and some decreases in physical inactivity. The estimated decrease in deaths attributed to better cholesterol control were 82 830, decreased systolic blood pressure were 68 800, decreased smoking were 39 925, and decreased inactivity were 17 445. On the opposite side, estimated increases in deaths attributed to increase in body mass index (BMI) were 29 905, whereas increase in deaths attributed to diabetes were 33 465. 9
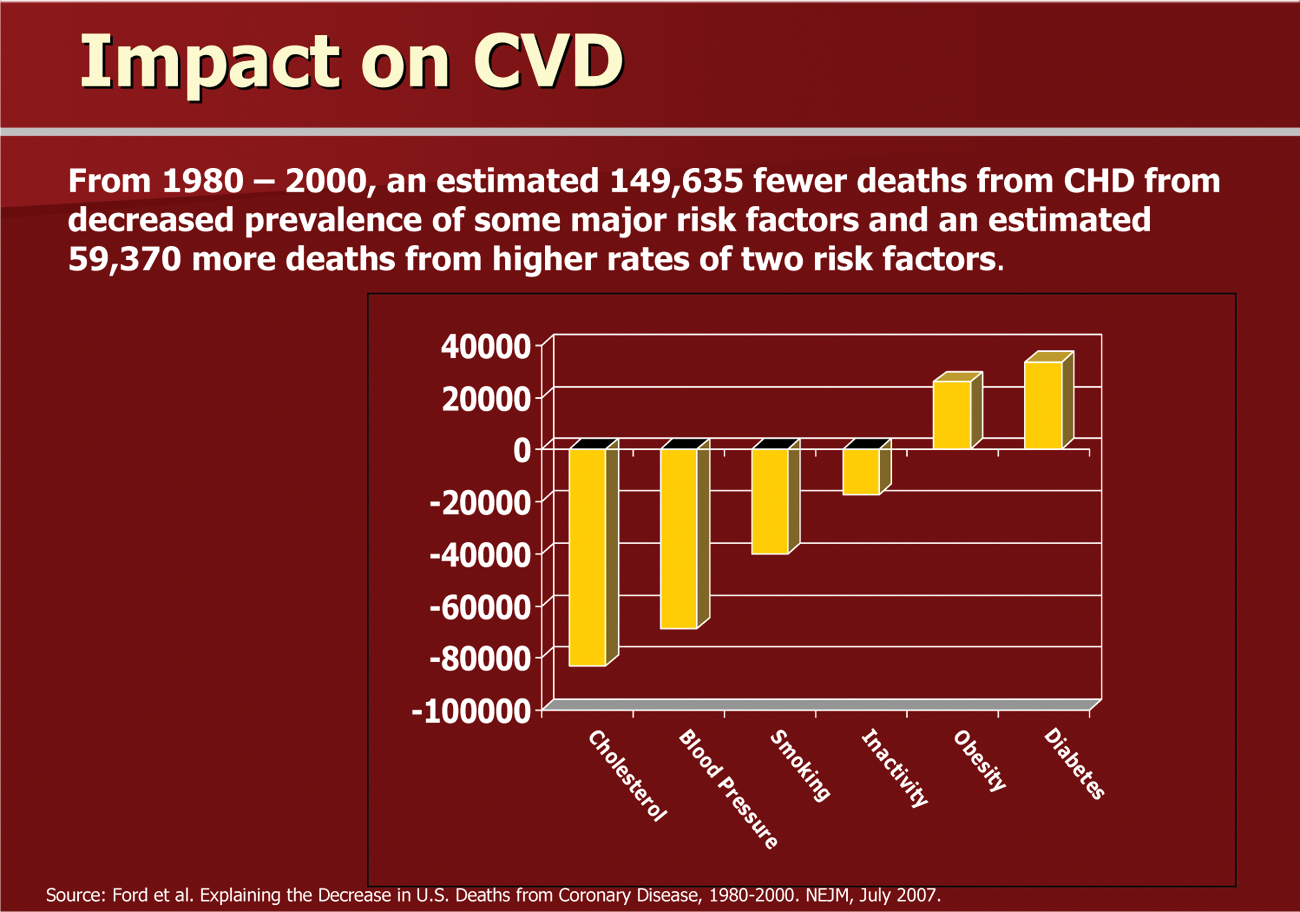
Impact on Estimated Deaths From Chronic Diseases on Overall Deaths From Coronary Heart Disease (CHD).
Beyond increased prevalence of diabetes and obesity, there are other indicators of failure to meet dietary guidelines. In 2005, for example, only 27.2% of adults consumed vegetables 3 or more times daily whereas 32.6% of adults consumed fruit 2 or more times daily. 5 In 2007-2008, the prevalence of obesity was 32.2% among adult men and 35.5% among adult women. 3 Although there was no increase in prevalence of obesity over the last 3 data points measured through the National Health and Nutrition Examination Survey (NHANES), neither was there decline in the prevalence of obesity. 3
Furthermore, despite the research-proven benefits of a Dietary Approaches to Stop Hypertension (DASH)-accordant diet in US hypertensives, only 19% of individuals with high blood pressure follow this diet and adherence to this pattern has declined since introduction of the DASH diet. 20 Another study based on data from the Multi-Ethnic Study of Atherosclerosis (MESA) found that although there was variation among different ethnic groups in attaining various DASH nutrient intake goals, overall less than 30% of MESA participants met any DASH nutrient target. 21 Clearly, we have a long way to go in implementing the knowledge that we currently possess.
Impact of Nutrition on Future Guidelines and the AHA 2020 Strategic Impact Goal
It is clear that issues related to nutrition and dietary patterns will continue to play a major role in the promotion of health and prevention of disease. The difficulty of changing the complex constellation of dietary factors will remain a challenge. Nonetheless, the impact that nutritional factors have on the lives and health of Americans will inevitably mandate shaping new goals, guidelines, and strategies for change. This can already be seen in the recently released 2020 Strategic Impact Goal from the AHA and the DGA 2010.
The 2020 Strategic Impact Goal from the AHA represents a welcome proactive step from this organization. 8 The focus of the 2020 AHA strategic impact goal is “Primordial prevention across all levels of risk factors across the lifespan.” The goal was established that “by 2020 to improve cardiovascular health of all Americans by 20% while reducing deaths from CVD and stroke by 20%.” The AHA Expert Committee went on to recognize that “Health is a broader more positive construct than just the absence of clinical evidence of disease.” It also provided as a rationale for its primordial prevention strategy that “it makes sense that the avoidance of adverse levels of risk factors in the first place may be the most effective means for avoiding clinical events during the remaining lifespan.”
The metrics elucidated by the AHA for “ideal” cardiovascular health include 7 metrics found in Table 3.
American Heart Association (AHA) Ideal Cardiovascular Health Metrics
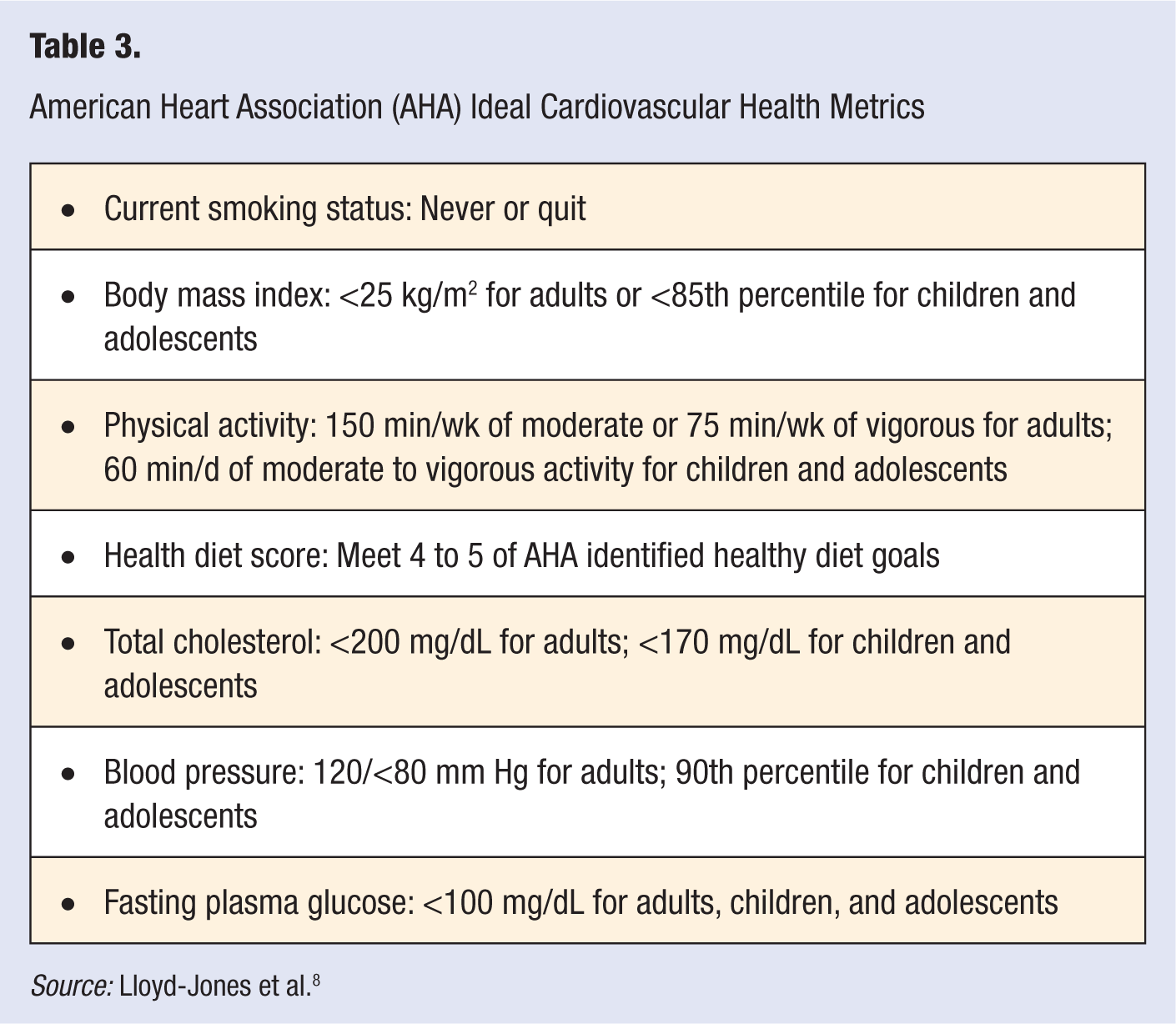
Source: Lloyd-Jones et al. 8
A quick perusal of Table 3 shows that 5 of the 7 metrics included in the AHA definition of “ideal” cardiovascular health have a dietary component. The AHA expert committee went further to define 5 primary dietary goals to serve as the basis for a “Healthy Diet Score” (HDS). The components set forth for the HDS by the AHA are found in Table 4.
American Heart Association (AHA) Healthy Diet Score
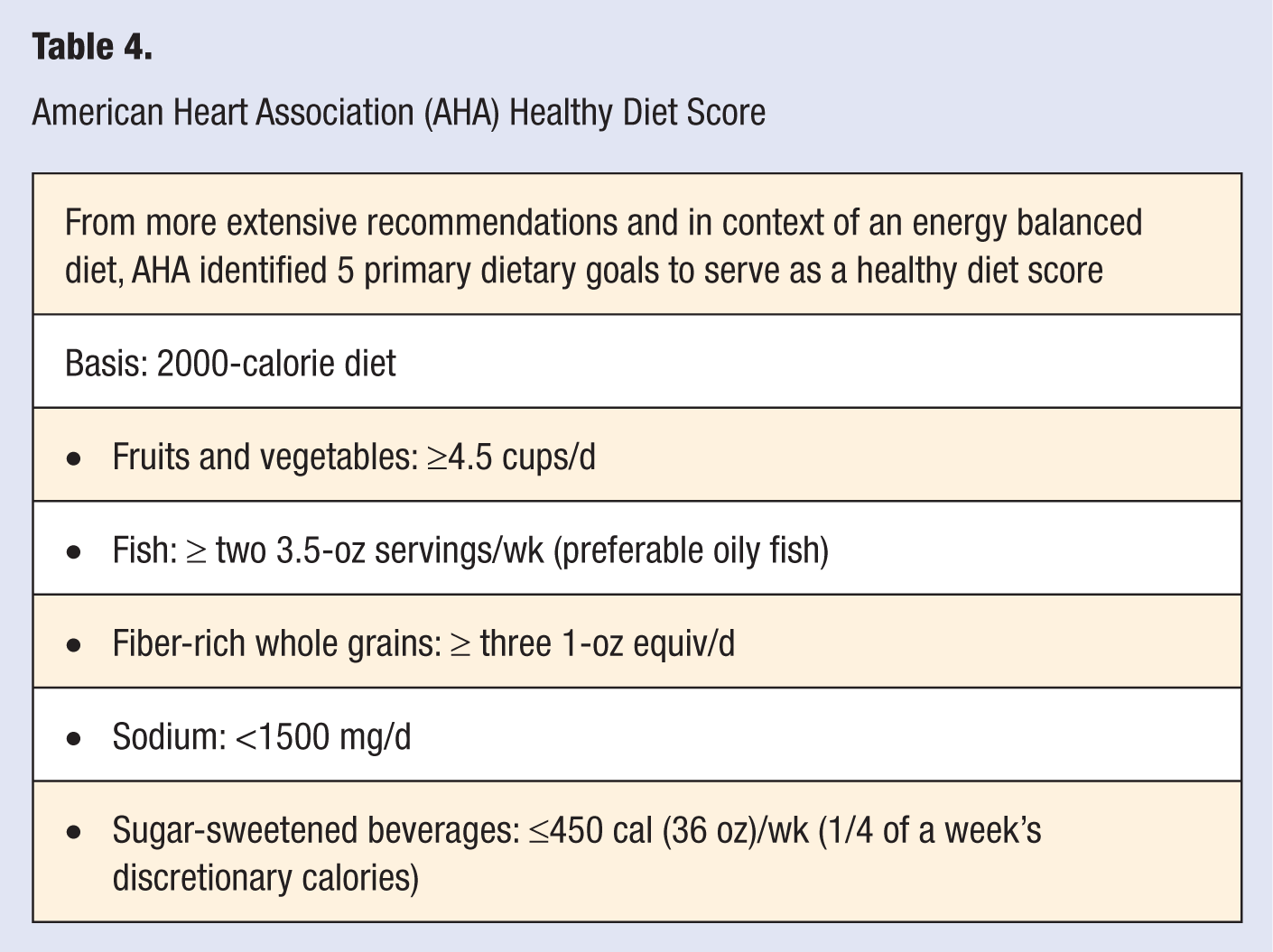
The AHA Committee noted that the overall diet should be consistent with the DASH type eating plan and also cautioned that the HDS had limitations. The score was not intended to be comprehensive but rather provide a practical approach, giving individuals a set of potential concrete actions. Other important factors were not included in the HDS but cited in the strategic plan were recommendations to limit trans fat to none or no more than 2 servings per week and limit saturated fat to less than 7% of total energy, while replacing these fats with nuts, legumes, and seeds.
Major dietary concerns addressed by these recommendations included the following:
Energy balance—calorie intake appropriate to maintain healthy weight
Limit sodium consumption to 1500 mg/day for larger population
Focus on whole foods and eating patterns rather than specific nutrients
A dietary pattern in keeping with DASH, emphasis on fruits, vegetables, fiber-rich whole grains, and fish
These recommendations are based on the 2006 AHA Scientific Statement on Diet and Lifestyle Recommendations 10 and also consistent with principles that guided the DGA 2010. 15
Influences on Heart Healthy Eating and Lifestyle Behaviors
To move toward implementation of nutritional guidelines, it is important to understand both influences on, and barriers to, heart healthy eating. It is only through understanding these influences that effective strategies can be developed to help individuals incorporate recommendations into their daily lives. This is a process that helps us move from “what” to “how.”
What and When Are We Eating Now?
To start the process of moving from what to how it is essential to understand what Americans are currently eating. Data from NHANES 2005-2008 indicate that men are consuming about 200 more calories per day and women 250 calories more per day than they did in the early 1970s. 22 In the areas of calories and sodium, which are 2 of the areas of greatest concern both in the AHA Dietary Recommendations and Healthy Eating Score and the DGA, data from NHANES 2005-2006 show the top sources of both calories and sodium.15,23 These are contained in Table 5.
Major Food Sources of Calories and Sodium in US Diet, National Health and Nutrition Examination Survey 2005-2006
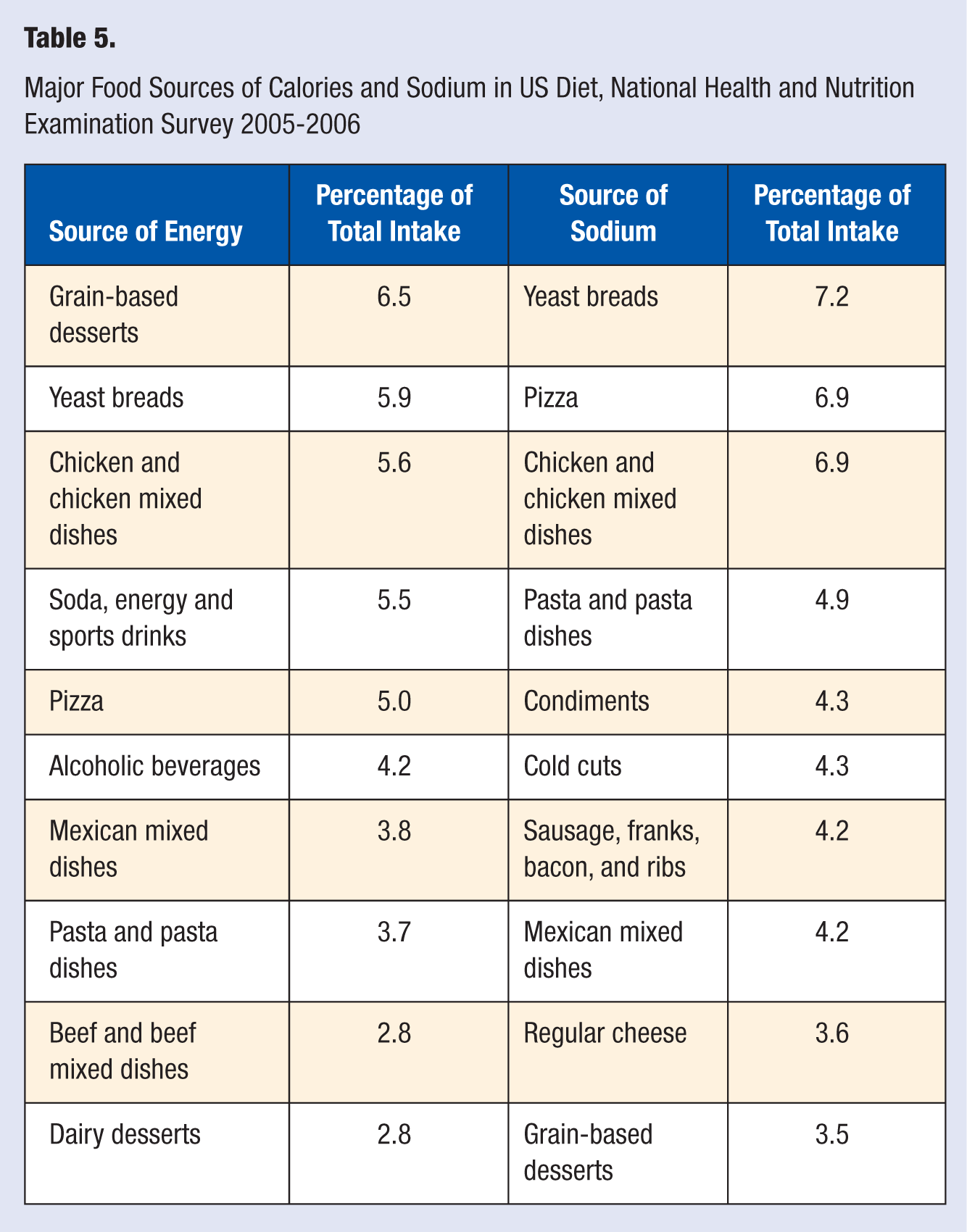
As can be seen in Table 5, calories come from a variety of foods in our diet. These top 10 foods in energy intake supply together 45.8% of the calories in the American diet. Many of them are also major sources of refined grains, added sugars, and solid fats, nutrients that the DGA 2010 recommends consuming less of. The top 10 food sources of sodium provide 50% of total sodium intake in the American diet; many of these foods also are major sources of calories, including those from added sugars and solid fats. Another study using NHANES data from 2003-2004 and 2005-2006 found that children and adolescents (2-18 years old) consumed nearly 40% of daily energy (798 of 2027 kcal/d) from solid fats (433 kcal) and added sugars (365 kcal). 24
Also contributing to higher energy intakes are the larger portions of food inside and outside the home that children and adults are consuming compared with 20 or 30 years ago.25-29 An analysis comparing national survey data from 1977-1978 with that of 1996, for example, found in children the largest increases for Mexican food (133 kcal), hamburgers (97 kcal), salty snacks (93 kcal), French fries (68 kcal), and soft drinks (49 kcal) and in fast food restaurants. 29
The issue of what we are eating is further complicated by “when” we are eating. For example, a comparison of data from NHANES 1971-1975 with that from NHANES 1999-2002 found that snacking events for adults increased by one snacking event a day. 30 The contribution of energy intake from snacks rose from 18% to approximately 25%. A separate analysis by the same researchers found that snacking episodes and calorie intake from snacking also increased in children. 31
Basics of Human Food Behaviors
Another issue that must be considered in attempting to implement nutrition guidance is the factors that drive human behavior whether it be eating or other behaviors. Research as synthesized by Brian Wansink suggests that there are 3 principles of human behavior that cannot be changed.32(pp86-87),33 These principles relate to food choices and other choices. As individuals and consumers we seek
Convenience: Removing the effort required to move, learn, or communicate. Examples include the wheel, printing press, telephone. It is a fundamental that humans desire to follow the path of least effort.
Variety and choice: This trait drives extensive varieties of the same food product. (Of course, this principle is also true in other areas such as the multiple choices in automobiles or of colors of automobiles, etc.) In addition, taste probably plays a big part in which foods out of the variety available we choose along with convenience and value.
(The option of) Value: With a large variety available, people usually choose “quantity over quality.” People look for the most quantity and quality that constitute “value” for their dollar—but quantity can edge quality (eg, health or nutrition), particularly if the food tastes good.
It can easily be theorized how these fundamentals of human behavior influence what Americans are currently eating. For example, major sources of energy (calories) include desserts/sweets, yeast bread, chicken/chicken dishes, soda, energy and sports drinks, and pizza. All these are convenient, offer great variety and choice, and provide a large quantity of calories (value) at relatively low price.
Environmental Influences on Food Choices
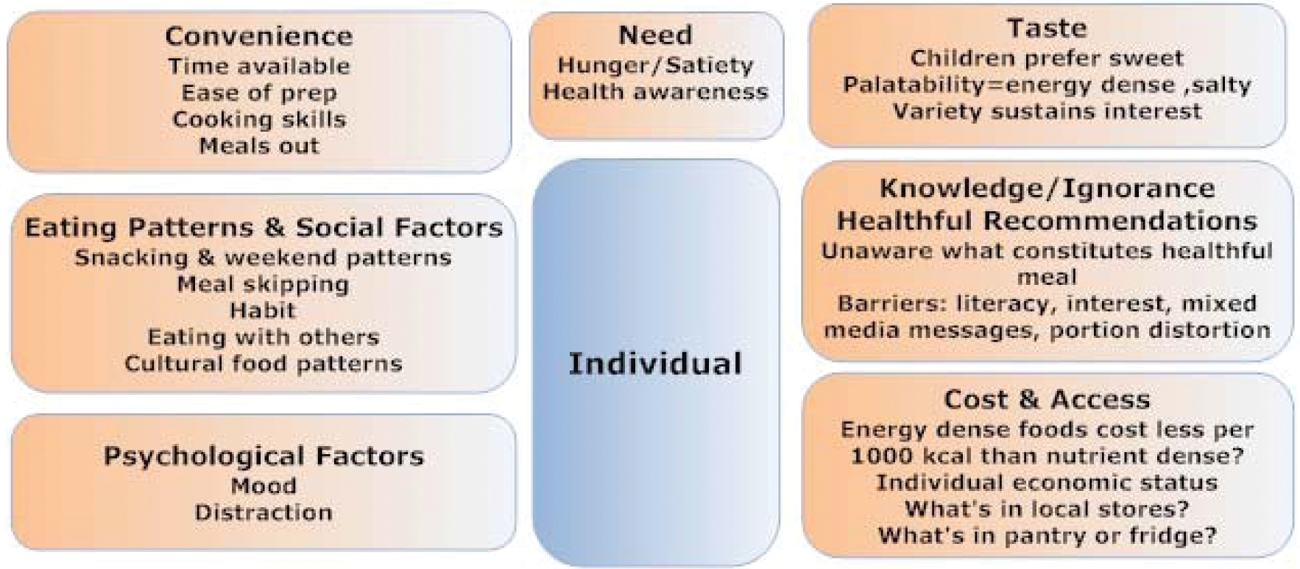
Beyond the internal principles of human behavior when it comes to food and other choices, a growing body of research suggests that a complex mix of environmental factors influence individual food choices.8,34,35 A better understanding of these factors may help us answer why nutritional guidelines have not had as great an impact on individual food choices and public health as intended or hoped. This, in turn, can help us develop more effective strategies of how to promote individual and population change and adherence to healthful food choices and eating patterns. A graphic depiction of factors influencing food choices is found in Figure 2.
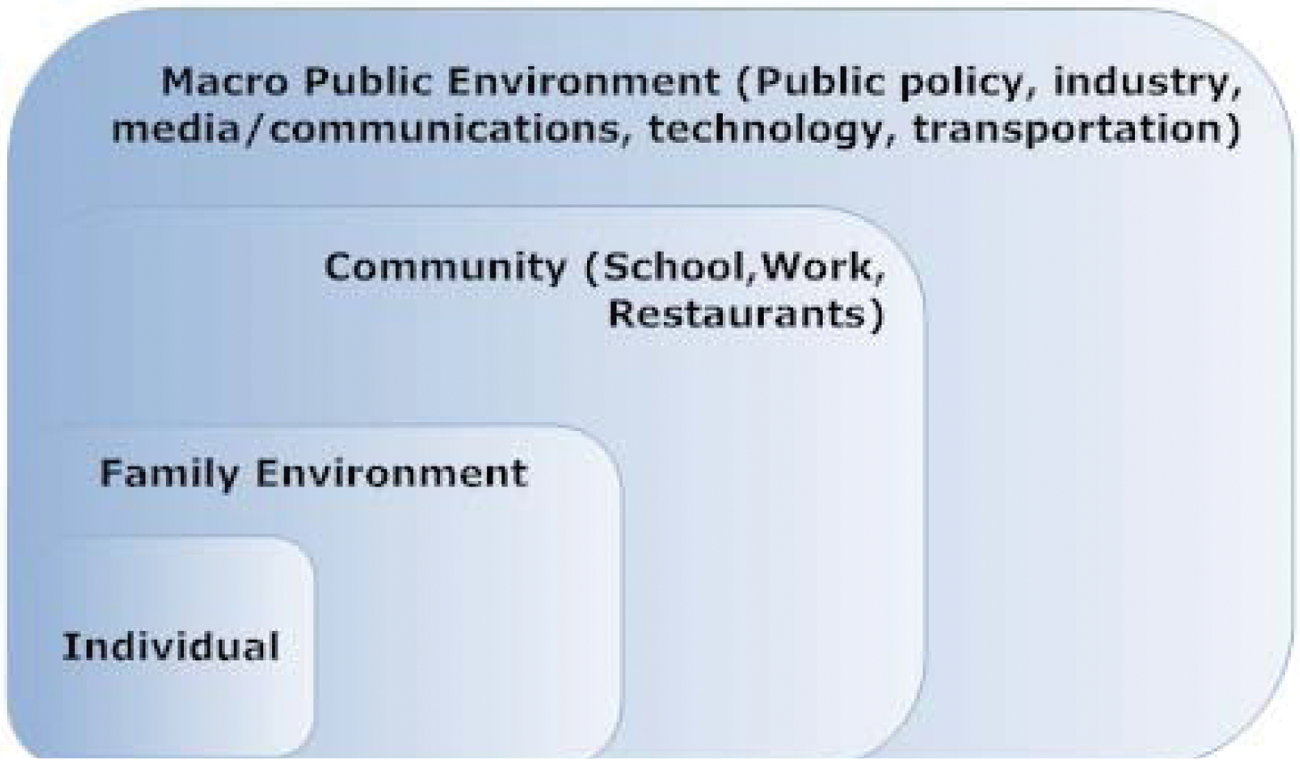
Environmental Influences on Food Choices.
This figure, which is adapted from the AHA Scientific Statement on implementing their nutritional guidelines 34 and a review by Larsen and Story, 35 gives a good visual image of the many domains of factors that influence individual and family food behaviors and choices. Although the domains are presented separately, it is important to remember that for every individual and family they exist simultaneously and are interrelated in a complex web. The key influencers that are most likely to be affected by health care professionals include those influences on the individual, family environment, and community. We have depicted these influences in Figures 3, 4, and 5, respectively. Although most of us as individual practitioners may have little direct influence on the fourth domain, the macro-public influences (Figure 6), it is important to be aware of them because they do affect individual behaviors.
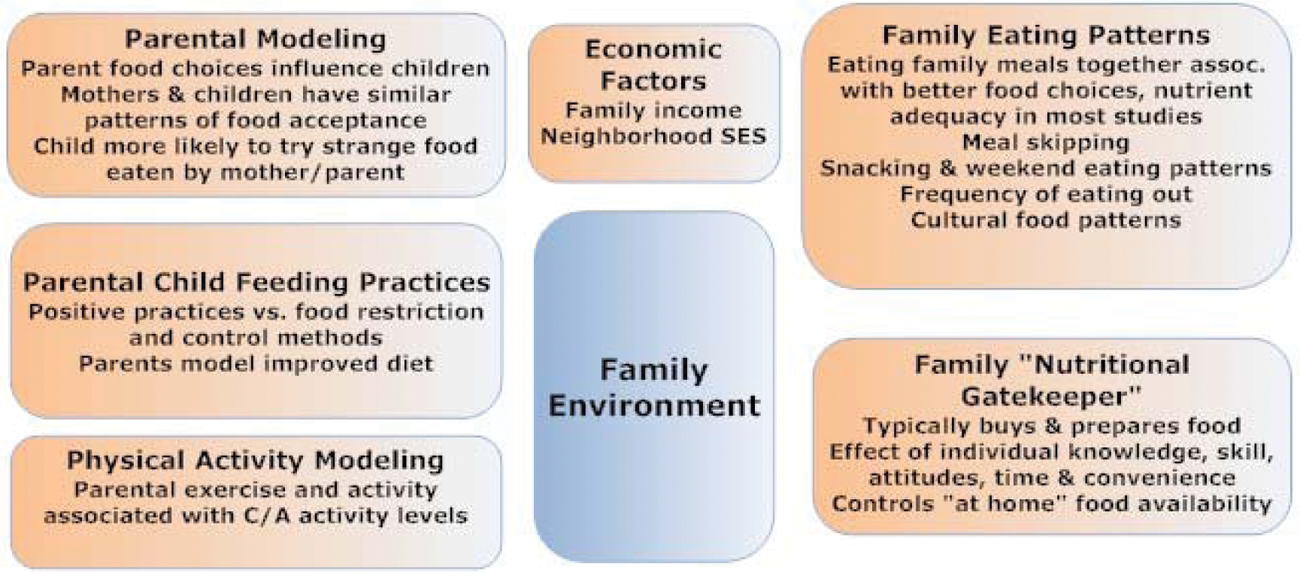
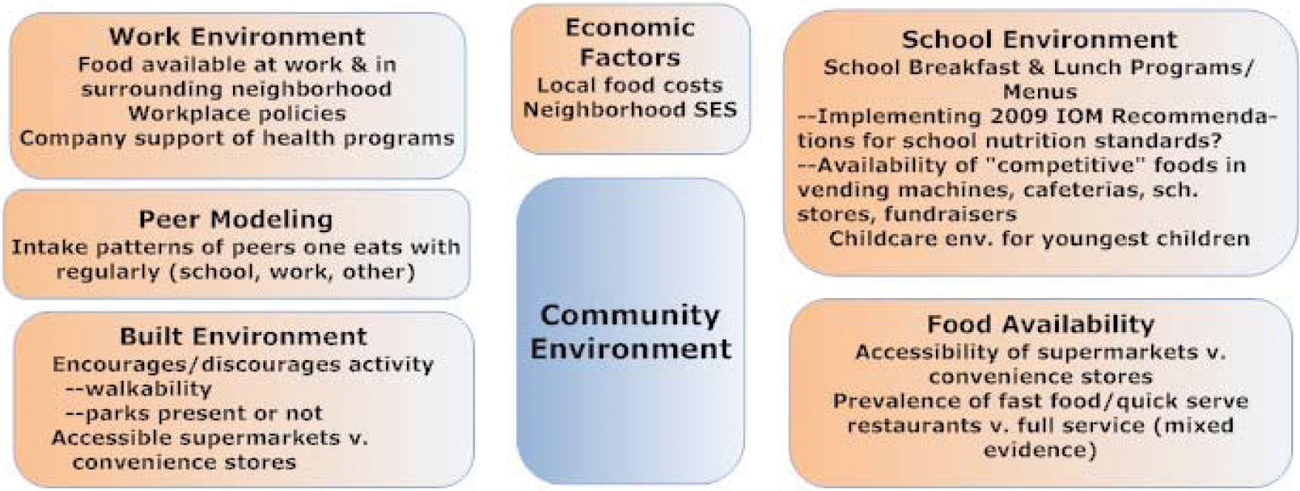
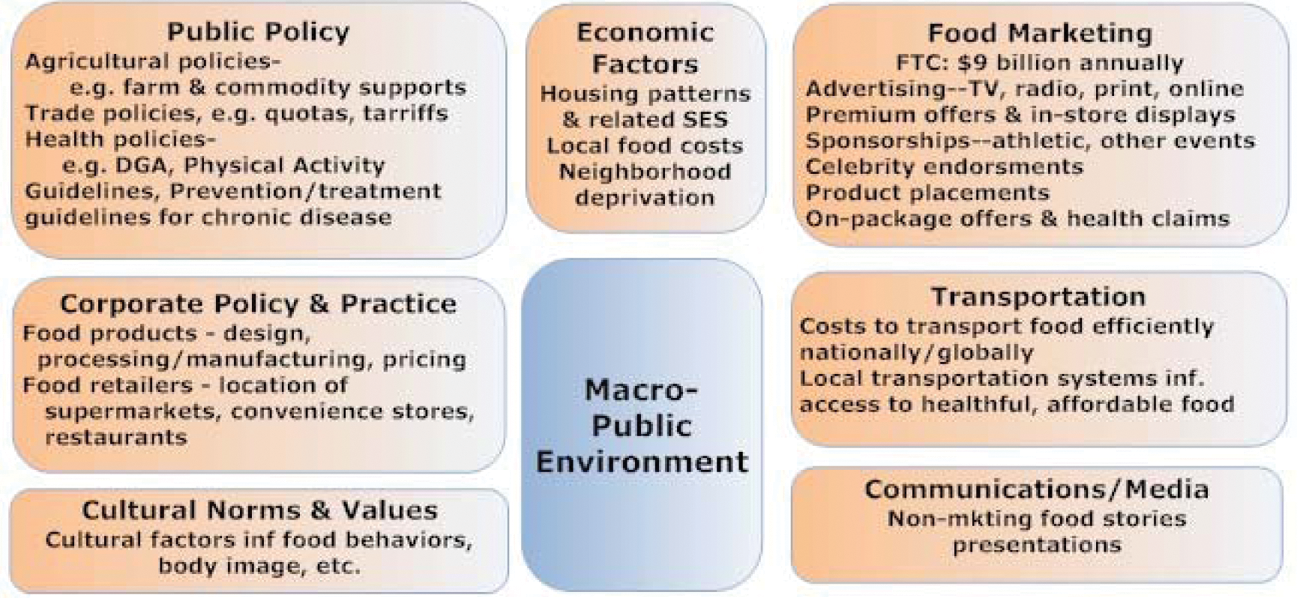
Although a detailed explanation of these figures is beyond the scope of the current review, the reader is referred to 3 resources that together provide an excellent introduction to this important area of research. The scientific statement “Implementing American Heart Association Pediatric and Adult Nutrition Guidelines” 34 and a comprehensive review by Larsen and Story 35 describe in detail how each of these factors affects the ability to implement nutritional guidelines and interventions for both children and adults. Chapter 6 “Helping Americans Make Healthy Choices” of the DGA 2010 presents an accessible summary of a social ecological framework for nutritional and physical activity choices. 15
Although the web of influences on individuals and their food choices is important, research into this area is in its infancy. Most studies that are available are cross-sectional and many have methodological limitations. More longitudinal and experimental studies are needed to explore causality and interlinkage of factors. The promise and importance of deepening this research is to help us develop ever more effective ways to encourage healthful eating behaviors.
Strategies and Techniques to Help Individuals Implement Heart Healthy Behaviors
As we move toward developing effective strategies for helping individuals implement heart healthy nutrition patterns and other practices in their daily lives we will have to meet a variety of challenges.32-34,36,61,75,76 For example, we need to reach real people where and how they live and translate guidelines into practical, simple actions that fit within the realities of their lives. We also have to tap into motivations for health, and change and encourage self-efficacy and self-management. We will also have to provide support and follow-through and keep messages fresh and effective. Messages should be framed in a positive fashion, whenever possible—emphasizing what to “do” rather than what “not to do.” In addition, we will have to develop more effective strategies to segment our messages to a variety of audiences.
Different messages may be appropriate for audiences of different ages, gender, economic and education status, cultural or ethnic group, and risk status for CVD, diabetes, or other chronic diseases as well as interest and commitment to healthy eating/willingness to try new behaviors. In this latter area, a graphic depiction of audience segmentation provided by Wansink provides useful framework.32,33 This is found in Figure 7.
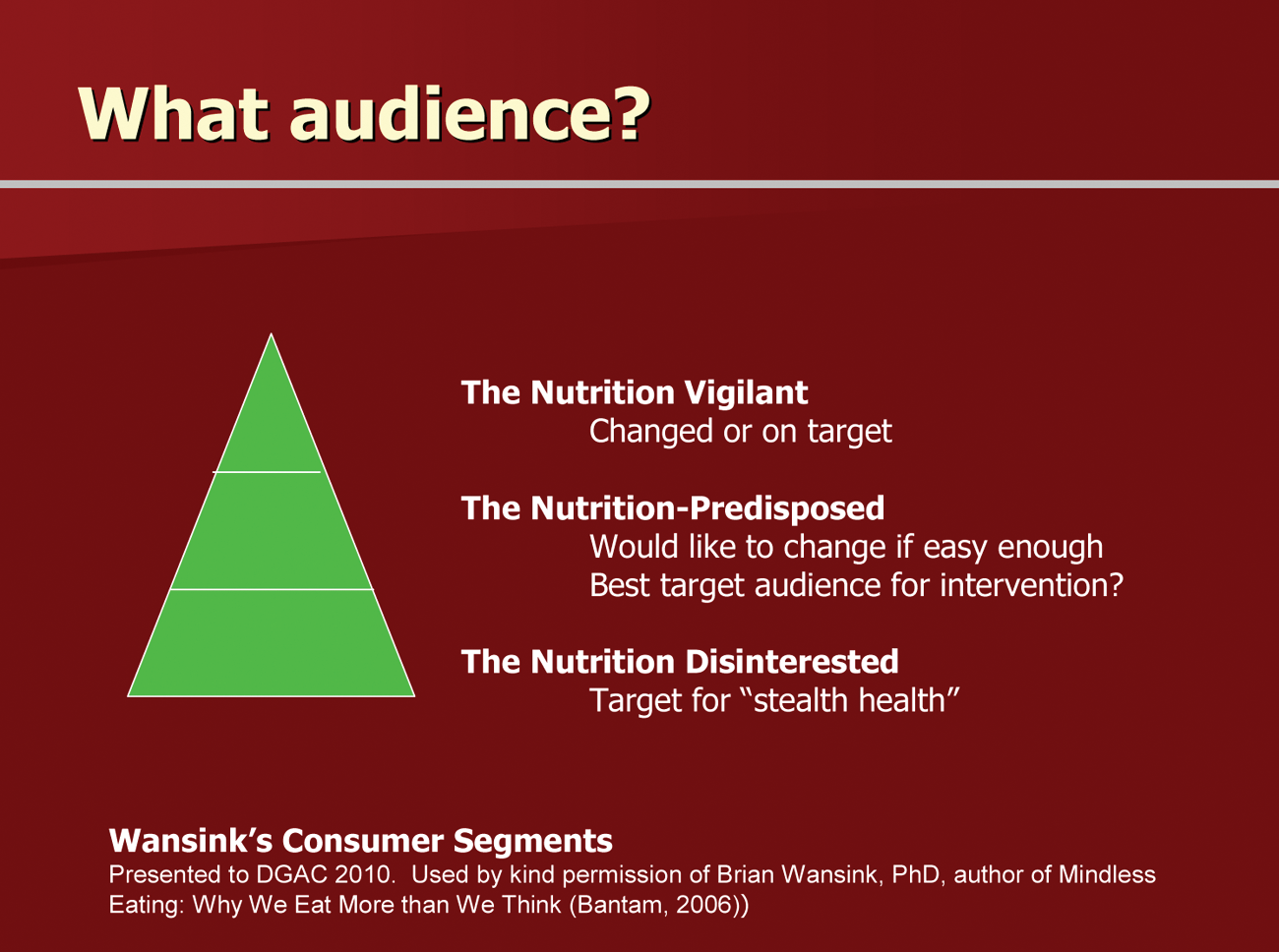
Audiences for Nutritional Messages and Interventions.
As shown in this figure, Wansink suggests that the “Nutrition Vigilant” are those who are most receptive to educational nutritional messages and information. They are the ones who already read and use food labels, for instance. They are part of the audience for interventions but not the ones who need most to change. Continued information and support for them (including counseling) is appropriate.
The group that might constitute the most effective audience for efforts from health care professionals is the “nutrition-predisposed.” Individuals who might be “predisposed” can have a variety of motivations. For example, they might include parents or persons at risk of CVD or other chronic disease. An appropriate approach for them would be to provide counseling and tools.
The “Nutrition Disinterested” might be best addressed, as suggested by Wansink, with “stealth health” such as portion-controlled packages, reformulation of food products, and other passive efforts.
Strategies for Change
A growing body of research, both observational and experimental, has examined various strategies for change in nutritional and related health behaviors and provides evidence of which strategies can be employed successfully. The most thorough, recent review of this body of evidence may be found in the AHA Scientific Statement on Interventions to Promote Physical Activity and Dietary Lifestyle Changes for Cardiovascular Risk Factor Reduction in Adults. 80 Since the 2007 publication cutoff for this review, a number of other pertinent studies have been published.75,77,81-93 Although it is beyond the scope of our discussion to examine each of these reviews and studies, we have observed that the following foundational concepts or principles appear to inform the most successful strategies:
Start with the individual client (or focus group)
Assess client readiness to change
Assess barriers that may block success
Use counseling techniques that foster clients making their own decisions and choosing steps for change (such as motivational interviewing and the use of the “Five As”: Assess, Advise, Agree, Assist, Arrange)
Provide tools for change
Provide support
The overall goal for all of these strategies is to empower the individual to achieve higher levels of self-efficacy.
Counseling for Change
Recent research has provided more insight into which counseling tools are most effective in encouraging individuals to change. Although nutrition education is an important part of helping individuals adopt new dietary behaviors for better heart health, stopping there (as has been common in the past) has been shown to be inadequate for most people. 80 More extensive and individualized counseling is recommended. In 2009, a review of 24 studies of motivational interviewing techniques as part of interventions to modify diet and/or exercise demonstrated overall support of effectiveness. 75 The US Preventive Services Task Force reviewed counseling for change81,94 and concluded the following:
For the general population there is fair evidence for brief, low- to medium-intensity behavioral dietary counseling producing small to medium changes (particularly in the area of reducing fat, and increasing fruits and vegetables).
In an at-risk population for CVD and other chronic disease, there is good evidence for medium- to high-intensity counseling producing medium-to-large changes.
Some examples of counseling for change supported by this growing literature include the following:
Use of brief, validated dietary assessment instruments (print, online, PDA) for assessment and monitoring.95-100
Telephone or online interventions and/or follow-up: instead of or in conjunction with. face-to-face counseling.94,101-109
Motivational print or online newsletters, tailored to individual or group barriers, preferences, and culture.91,110-114
Tools Targeting Simple Steps
Simple tools that support individual or group counseling may also be effective in helping people make changes. Here are 2 brief examples of simple tools that support two positive messages about nutritional choices for better heart health:
Message 1: Eat more fruits and vegetables. Tested strategies include (a) using a “market basket” visual with checklists of affordable, nutrient-dense fruits and vegetables, 115 tailored to the availability and cost of foods for targeted groups 115 ; (b) providing suggestions and simple recipes for preparing specific vegetables (seasonal, new to consumer, etc)116,117; (c) providing additional Web-based resources with more information and feedback103,118-122; and (d) offering a one-time cooking class or a short series of classes focused on preparing vegetables or other skills.123-128
Message 2: Size your portions “right” for good nutrition and weight control.129,130 Use of the “Portion Distortion Quiz” from the National Heart Lung, and Blood Institute or visual depictions of correct portion sizes as well as tips on using controlled-portion foods129,131-135 may all be effective.
More Extensive Interventions
It is important to note that longer term supportive interventions that involve counseling or simple tools have generally been shown to be more effective than shorter term interventions. 94 With the use of tailored technology including phone, print, and computerized support, such interventions may be incorporated into existing clinical or hospital practices efficiently with the additional possibility of partnering with other community organizations.136-140
Some Practical Suggestions for Engaging Patients in Change
As health care professionals, it is important for all of us to remember that our words and behavior can exert a significant impact on our patients. As the saying goes, you can’t expect what you don’t inspect. In this regard, what we do not examine may send as powerful a message as what we do. With this in mind, we would offer the following modest suggestions of ways to incorporate more heart healthy nutritional messages into our daily practices.
Use the Vital Signs of Heart Health
All of us are familiar with the concept of “vital signs” such as heart rate, blood pressure, temperature, and so on. We would suggest that these “vital signs” be expanded into the area of heart health. We would further subdivide this into the following vital signs:
Vital signs of heart healthy diet
Vital signs of obesity
Vital signs of physical activity
Vital signs of heart healthy diet
A quick and structured way of obtaining the vital signs of a heart healthy diet is simply to ask each client how they do on each factor of the AHA HDS presented earlier in this review. 8 This can lead to a more extensive discussion about the key components of a heart healthy diet.
Vital signs of obesity.
We would suggest that every clinician obtain the following pieces of information, which ample evidence supports as the “vital signs of obesity”141-145
Weight
Body mass index
Waist circumference
Vital signs of physical activity
Inquiring about the “vital signs of physical activity” can initiate a discussion on the heart healthy benefits of regular physical activity. Fortunately, a proven tool is available to assist in this process. 146 The Stanford Brief Activity Survey is a validated checklist that asks patients to check the statement that best describes their activity.147,148 The Stanford Brief Activity Survey is found in Table 6. This instrument divides on-the-job activity into 3 levels and leisure-time activity into 5 levels. This simple score may help individuals see how they are doing and help motivate them to increase their level of physical activity.
Stanford Brief Activity Survey
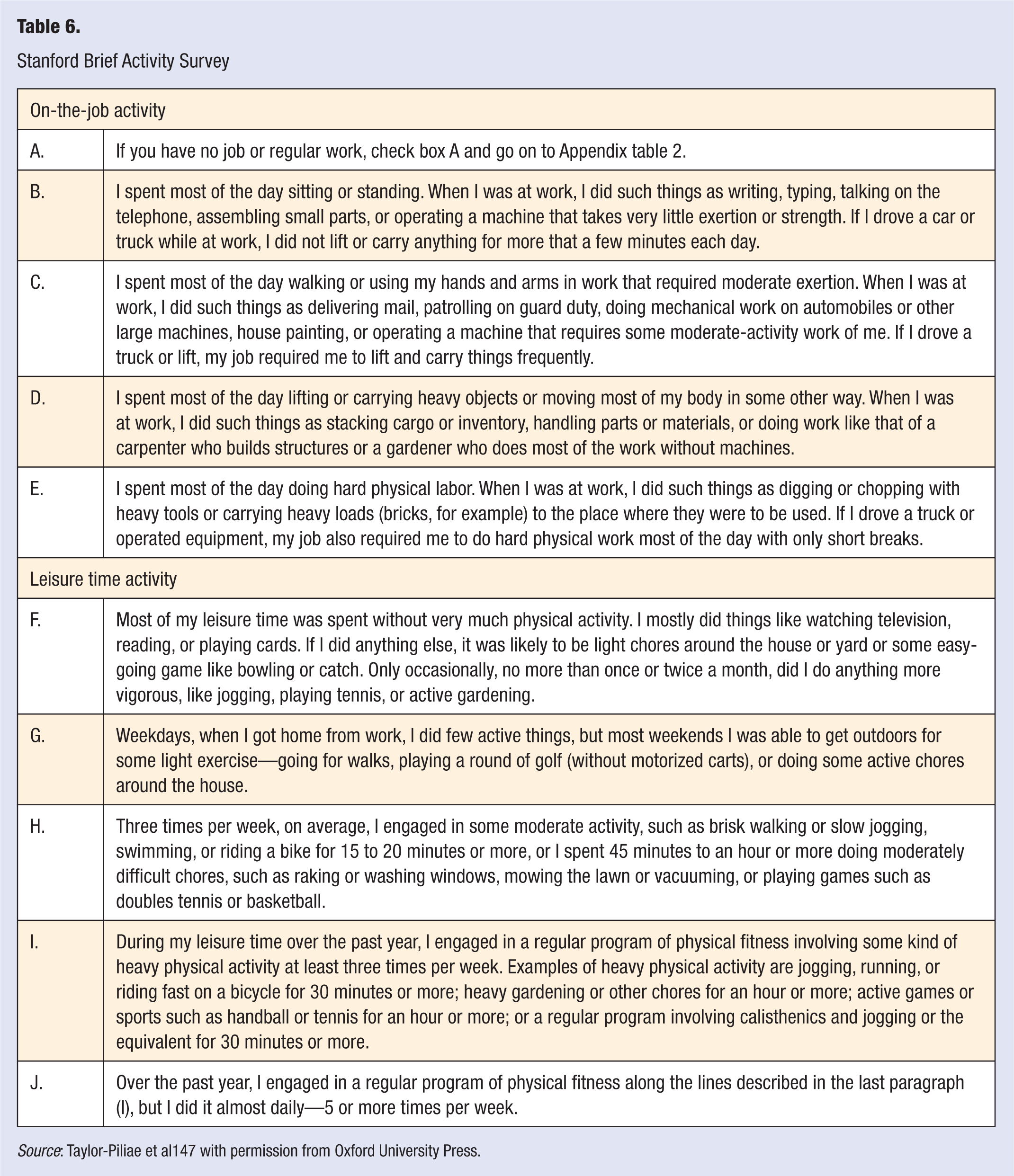
Source: Taylor-Piliae et al147 with permission from Oxford University Press.
Summary/Conclusion
For the past 4 decades, an impressive body of information has been developed about the relationship between daily habits and actions and cardiovascular health. This is particularly true in the area of nutrition. The future challenge will be how to take this information and help individuals implement it into their daily lives. With this in mind we would conclude the following thoughts:
Individualize interventions to overcome barriers
Take vital signs of cardiovascular health to open doors to counseling and educational tools to motivate client change
Target the individuals and groups most receptive to dietary changes for heart health
With this structure, we can begin to take the next important steps in helping individuals to improve their cardiovascular health by truly implementing cardiovascular and nutrition guidelines in a practical and motivational way in the lives of our patients. This is a vital first step in what we view as the next critical step of improving cardiovascular health by moving from “what” to “how.”